
Musculoskeletal Disorder Symptoms in Saudi Allied Dental Professionals: Is there an Underestimation of Related Occupational Risk Factors?

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
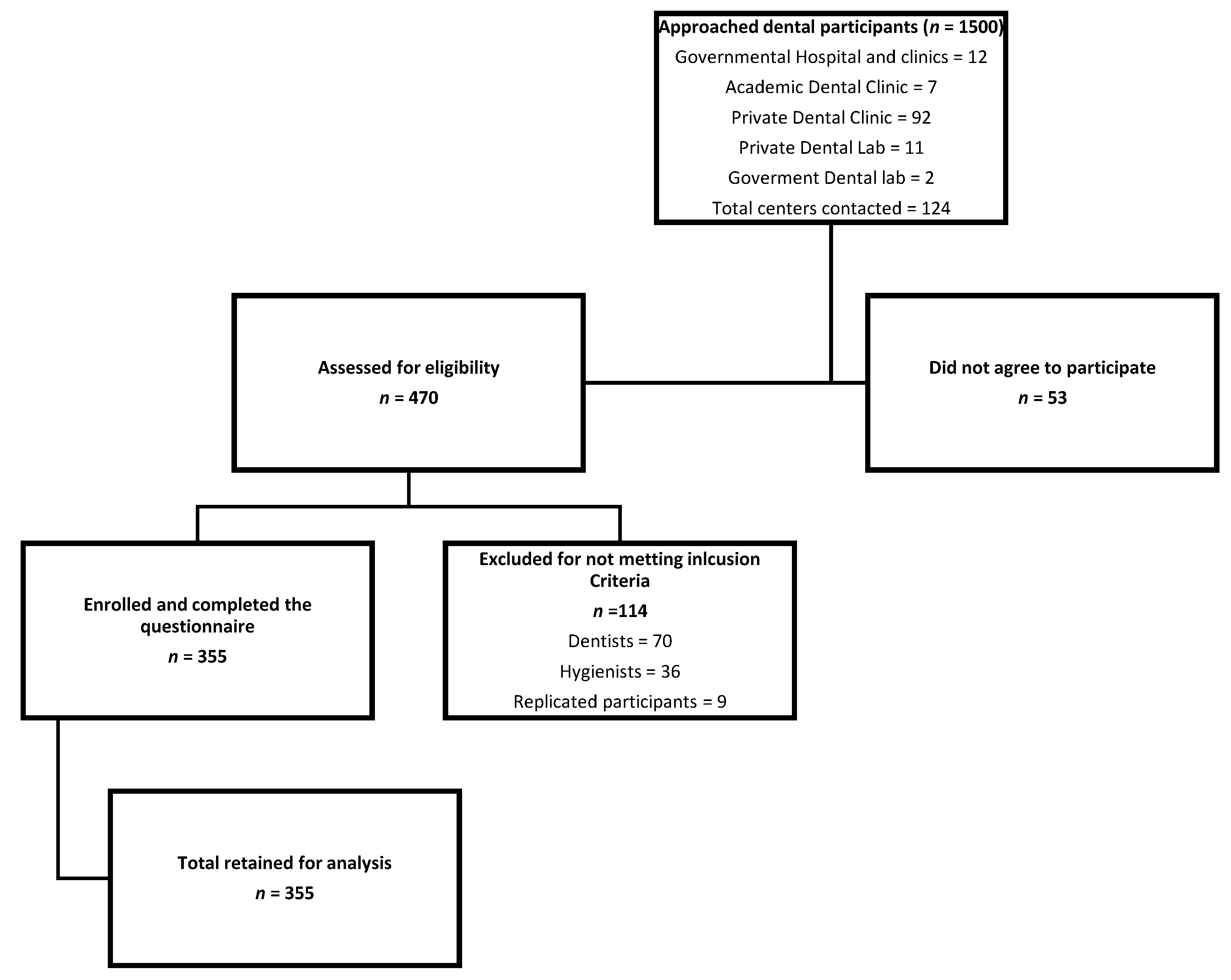
2.1. Study Design and Sample Size
2.2. Participants
2.3. Outcome Measure
2.4. Data Collection Procedure
2.5. Risk Factors
2.6. Statistical Analysis
2.7. Qualitative Analysis
2.8. Quality Assurance
3. Results
3.1. Socio-Demographic Characteristics
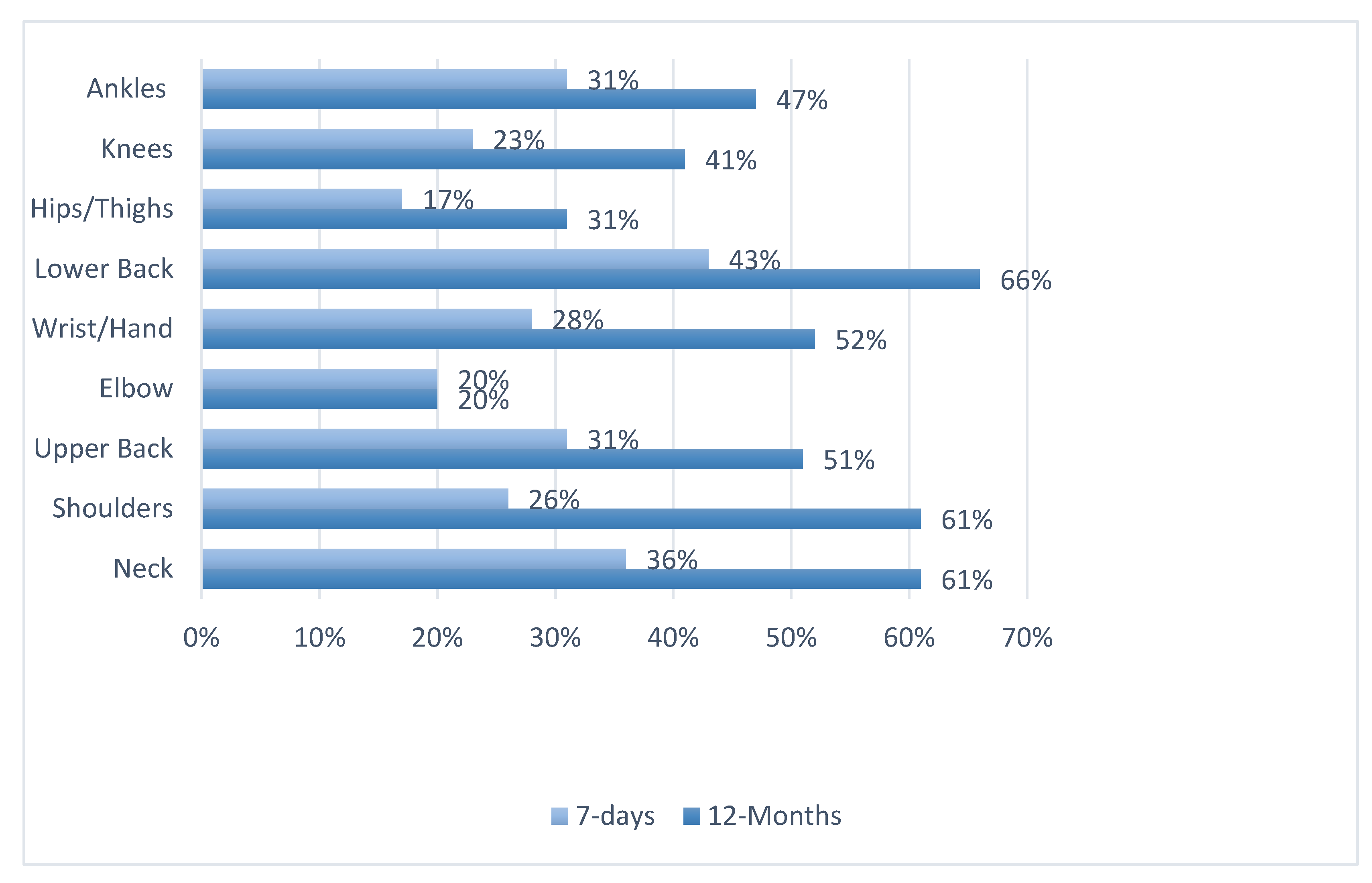
3.2. Prevalence
3.3. Associated Risk Factors
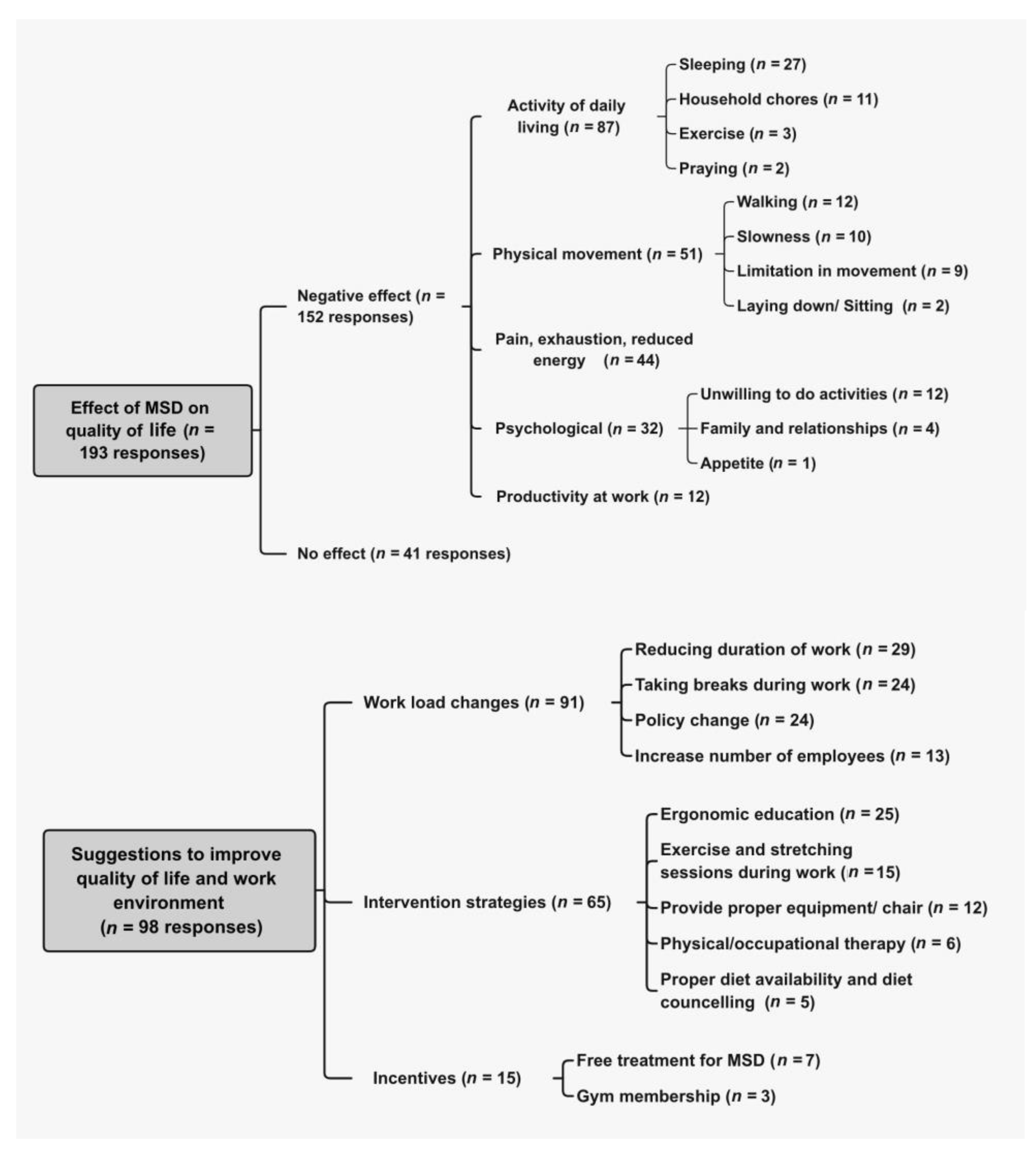
3.4. Participants’ Opinions
4. Discussion
4.1. Prevalence
4.2. Associated Risk Factors
4.2.1. Type of Physical Movement
4.2.2. Age and Years of Experience
4.2.3. Occupation
4.3. Non-Significant Risk Factors
4.4. Participants’ Suggestions for Reducing Burden of MSD Symptoms
4.4.1. Workload Reduction
4.4.2. Ergonomics Education
4.4.3. Exercise
4.5. Strength, Limitations, and Future Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.A.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the global burden of disease study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Briggs, A.M.; Woolf, A.D.; Dreinhöfer, K.; Homb, N.; Hoy, D.G.; Kopansky-Giles, D.; Åkesson, K.; March, L. Reducing the global burden of musculoskeletal conditions. Bull. World Health Org. 2018, 96, 366. [Google Scholar] [CrossRef] [PubMed]
- Aljanakh, M.; Shaikh, S.; Siddiqui, A.A.; Al-Mansour, M.; Hassan, S.S. Prevalence of musculoskeletal disorders among dentists in the Ha’il Region of Saudi Arabia. Ann. Saudi Med. 2015, 35, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Aminian, O.; Alemohammad, Z.B.; Hosseini, M.H. Neck and upper extremity symptoms among male dentists and pharmacists. Work 2015, 51, 863–868. [Google Scholar] [CrossRef]
- Blanc, D.; Farre, P.; Hamel, O. Variability of musculoskeletal strain on dentists: An electromyographic and goniometric study. Int. J. Occup. Saf. Ergon. 2014, 20, 295–307. [Google Scholar] [CrossRef] [PubMed]
- Epstein, S.; Sparer, E.H.; Tran, B.N.; Ruan, Q.Z.; Dennerlein, J.T.; Singhal, D.; Lee, B.T. Prevalence of Work-Related Musculoskeletal Disorders Among Surgeons and Interventionalists: A Systematic Review and Meta-analysis. JAMA Surg. 2018, 153, e174947. [Google Scholar] [CrossRef]
- Anwer, S.; Li, H.; Antwi-Afari, M.F.; Wong, A.Y.L. Associations between physical or psychosocial risk factors and work-related musculoskeletal disorders in construction workers based on literature in the last 20 years: A systematic review. Int. J. Ind. Ergon. 2021, 83, 103113. [Google Scholar] [CrossRef]
- Huisstede, B.M.; Miedema, H.S.; Verhagen, A.P.; Koes, B.W.; Verhaar, J.A. Multidisciplinary consensus on the terminology and classification of complaints of the arm, neck and/or shoulder. Occup. Environ. Med. 2007, 64, 313. [Google Scholar] [CrossRef]
- Huisstede, B.M.; Wijnhoven, H.A.; Bierma-Zeinstra, S.M.; Koes, B.W.; Verhaar, J.A.; Picavet, S. Prevalence and characteristics of complaints of the arm, neck, and/or shoulder (CANS) in the open population. Clin. J. Pain 2008, 24, 253–259. [Google Scholar] [CrossRef]
- Roquelaure, Y.; Ha, C.; Leclerc, A.; Touranchet, A.; Sauteron, M.; Melchior, M.; Imbernon, E.; Goldberg, M. Epidemiologic surveillance of upper-extremity musculoskeletal disorders in the working population. Arthr. Care Res. 2006, 55, 765–778. [Google Scholar] [CrossRef]
- Alnaami, I.; Awadalla, N.J.; Alkhairy, M.; Alburidy, S.; Alqarni, A.; Algarni, A.; Alshehri, R.; Amrah, B.; Alasmari, M.; Mahfouz, A.A. Prevalence and factors associated with low back pain among health care workers in southwestern Saudi Arabia. BMC Musculoskelet. Disord. 2019, 20, 56. [Google Scholar] [CrossRef]
- Šćepanović, D.; Klavs, T.; Verdenik, I.; Oblak, Č. The Prevalence of Musculoskeletal Pain of Dental Workers Employed in Slovenia. Workplace Health Saf. 2019, 67, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Ohlendorf, D.; Erbe, C.; Hauck, I.; Nowak, J.; Hermanns, I.; Ditchen, D.; Ellegast, R.; Groneberg, D.A. Kinematic analysis of work-related musculoskeletal loading of trunk among dentists in Germany. BMC Musculoskelet. Disord. 2016, 17, 427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valachi, B.; Valachi, K. Mechanisms leading to musculoskeletal disorders in dentistry. J. Am. Dent. Assoc. 2003, 134, 1344–1350. [Google Scholar] [CrossRef]
- Botha, P.J.; Chikte, U.; Esterhuizen, T.M.; Barrie, R. Self-reported musculoskeletal pain among dentists in South Africa: A 12-month prevalence study: Research. S. Afr. Dent. J. 2014, 69, 208–213. [Google Scholar]
- Nokhostin, M.R.; Zafarmand, A.H. “Musculoskeletal problem”: Its prevalence among Iranian dentists. J. Int. Soc. Prev. Community Dent. 2016, 6, S41. [Google Scholar] [PubMed] [Green Version]
- Morse, T.; Bruneau, H.; Dussetschleger, J. Musculoskeletal disorders of the neck and shoulder in the dental professions. Work 2010, 35, 419–429. [Google Scholar] [CrossRef]
- Hodacova, L.; Sustova, Z.; Cermakova, E.; Kapitan, M.; Smejkalova, J. Self-reported risk factors related to the most frequent musculoskeletal complaints among Czech dentists. Ind. Health 2014, 53, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Al Amer, H.S. Low back pain prevalence and risk factors among health workers in Saudi Arabia: A systematic review and meta-analysis. J. Occup. Health 2020, 62, e12155. [Google Scholar] [CrossRef]
- Jradi, H.; Alanazi, H.; Mohammad, Y. Psychosocial and occupational factors associated with low back pain among nurses in Saudi Arabia. J. Occup. Health 2020, 62, e12126. [Google Scholar] [CrossRef]
- Awaji, M.A. Epidemiology of low back pain in Saudi Arabia. J. Adv. Med. Pharm. Sci. 2016, 6, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Salam, D.M.; Almuhaisen, A.S.; Alsubiti, R.A.; Aldhuwayhi, N.F.; Almotairi, F.S.; Alzayed, S.M.; Bakri, F.F. Musculoskeletal pain and its correlates among secondary school female teachers in Aljouf region, Saudi Arabia. J. Public Health 2019, 29, 303–310. [Google Scholar] [CrossRef]
- Badawood, M.A.; Obaid, H.; Mohammed, M.E.; Alrogi, A.J. Impact of Low Back Pain on the work performance of male high school Saudi Teachers in Taif City. J. Health Inform. Dev. Ctries. 2017, 11, 1–18. [Google Scholar]
- Aboalshamat, K.T. Nordic assessment of occupational disorders among dental students and dentists in Saudi Arabia. J. Int. Soc. Prev. Community Dent. 2020, 10, 561. [Google Scholar] [CrossRef] [PubMed]
- Al-Gunaid, T.H.; Abdulhai, R.; Flemban, B. Prevalence of musculoskeletal disorders among dentists in Al-Madinah, Kingdom of Saudi Arabia. Int. J. Recent Surg. Med. Sci. 2017, 3, 15–19. [Google Scholar] [CrossRef]
- Al-Mohrej, O.A.; AlShaalan, N.S.; Al-Bani, W.M.; Masuadi, E.M.; Almodaimegh, H.S. Prevalence of musculoskeletal pain of the neck, upper extremities and lower back among dental practitioners working in Riyadh, Saudi Arabia: A cross-sectional study. BMJ Open 2016, 6, e011100. [Google Scholar] [CrossRef] [Green Version]
- Hamasha, A.A.H.; Alturki, A.; Alghofaili, N.; Alhomaied, A.; Alsanee, F.; Aljaghwani, F.; Alhamdan, M.; El-Metwally, A. Predictors and level of job satisfaction among the dental workforce in national guard health affairs. J. Int. Soc. Prev. Community Dent. 2019, 9, 89. [Google Scholar] [CrossRef]
- Samat, R.A.; Shafei, M.N.; Yaacob, N.A.; Yusoff, A. Prevalence and associated factors of back pain among dental personnel in North-Eastern State of Malaysia. Int. J. Collab. Res. Intern. Med. Public. Health 2011, 3, 576–586. [Google Scholar]
- Dajpratham, P.; Ploypetch, T.; Kiattavorncharoen, S.; Boonsiriseth, K. Prevalence and associated factors of musculoskeletal pain among the dental personnel in a dental school. J. Med. Assoc. Thail. 2010, 93, 714–721. [Google Scholar]
- Haas, Y.; Naser, A.; Haenel, J.; Fraeulin, L.; Holzgreve, F.; Erbe, C.; Betz, W.; Wanke, E.M.; Brueggmann, D.; Nienhaus, A.; et al. Prevalence of self-reported musculoskeletal disorders of the hand and associated conducted therapy approaches among dentists and dental assistants in Germany. PLoS ONE 2020, 15, e0241564. [Google Scholar] [CrossRef]
- Al Wassan, K.A.; Almas, K.; Al Shethri, S.E.; Al Qahtani, M. Back & neck problems among dentists and dental auxiliaries. J. Contemp. Dent. Pract. 2001, 2, 17–30. [Google Scholar]
- Alghadir, A.; Zafar, H.; Iqbal, Z.A. Work-related musculoskeletal disorders among dental professionals in Saudi Arabia. J. Phys. Ther. Sci. 2015, 27, 1107–1112. [Google Scholar] [CrossRef] [Green Version]
- Naing, L.; Winn, T.; Rusli, B. Practical issues in calculating the sample size for prevalence studies. Arch. Orofac. Sci. 2006, 1, 9–14. [Google Scholar]
- Osborn, J.F. Biostatistics: A Foundation of Analysis in the Health Sciences; Wiley Online Library: Hoboken, NJ, USA, 1984. [Google Scholar]
- Ngamjarus, C. n4Studies: Sample size calculation for an epidemiological study on a smart device. Siriraj Med. J. 2016, 68, 160–170. [Google Scholar]
- Al-Hourani, Z.; Nazzal, M.; Khader, Y.; Almhdawi, K.; Bibars, A.R. Work-related musculoskeletal disorders among Jordanian dental technicians: Prevalence and associated factors. Work 2017, 56, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sørensen, F.; Andersson, G.; Jørgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- Hayes, M.; Cockrell, D.; Smith, D. A systematic review of musculoskeletal disorders among dental professionals. Int. J. Dent. Hyg. 2009, 7, 159–165. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Body Mass Index—BMI. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 30 January 2021).
- Zhang, Z. Variable selection with stepwise and best subset approaches. Ann. Transl. Med. 2016, 4, 136. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, M.Z.I.; Turin, T.C. Variable selection strategies and its importance in clinical prediction modelling. Fam. Med. Community Health 2020, 8, e000262. [Google Scholar] [CrossRef] [Green Version]
- IBM Corp. IBM SPSS Statistics for Windows; IBM Corp.: Armonk, NY, USA, 2019. [Google Scholar]
- Bryman, A. Social Research Methods; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
- QSR International Pty Ltd. NVivo; QSR International Pty Ltd.: Burlington, MA, USA, 2016. [Google Scholar]
- Ohlendorf, D.; Haas, Y.; Naser, A.; Haenel, J.; Maltry, L.; Holzgreve, F.; Erbe, C.; Betz, W.; Wanke, E.M.; Brüggmann, D.; et al. Prevalence of Muscular Skeletal Disorders among Qualified Dental Assistants. Int. J. Environ. Res. Public Health 2020, 17, 3490. [Google Scholar] [CrossRef]
- Osman, E.A. The Prevalence of Work-Related Musculoskeletal Pain among Dentists and Allied Dental Personnel in Private Dental Teaching Hospitals in Khartoum State, in Faculty of Dentistry; University of Science and Technology: Khartoum, Sudan, 2018. [Google Scholar]
- Meisha, D.E.; Alsharqawi, N.S.; Samarah, A.A.; Al-Ghamdi, M.Y. Prevalence of work-related musculoskeletal disorders and ergonomic practice among dentists in Jeddah, Saudi Arabia. Clin. Cosmet. Investig. Dent. 2019, 11, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lietz, J.; Kozak, A.; Nienhaus, A. Prevalence and occupational risk factors of musculoskeletal diseases and pain among dental professionals in Western countries: A systematic literature review and meta-analysis. PLoS ONE 2018, 13, e0208628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bento, T.P.F.; dos Santos Genebra, C.V.; Maciel, N.M.; Cornelio, G.P.; Simeão, S.F.A.P.; de Vitta, A. Low back pain and some associated factors: Is there any difference between genders? Braz. J. Phys. Ther. 2020, 24, 79–87. [Google Scholar] [CrossRef]
- Brady, S.R.; Hussain, S.M.; Brown, W.J.; Heritier, S.; Billah, B.; Wang, Y.; Teede, H.; Urquhart, D.M.; Cicuttini, F.M. Relationships between Weight, Physical Activity and Back Pain in Young Adult Women; BMJ Publishing Group Ltd.: London, UK, 2016. [Google Scholar]
- Wunderlich, M.; Eger, T.; Rüther, T.; Meyer-Falcke, A.; Leyk, D. Analysis of spine loads in dentistry—Impact of an altered sitting position of the dentist. J. Biomed. Eng. 2010, 3, 664. [Google Scholar] [CrossRef] [Green Version]
- Puriene, A.; Aleksejuniene, J.; Petrauskiene, J.; Balciuniene, I.; Janulyte, V. Self-reported occupational health issues among Lithuanian dentists. Ind. Health 2008, 46, 369–374. [Google Scholar] [CrossRef] [Green Version]
- Alexopoulos, E.C.; Stathi, I.-C.; Charizani, F. Prevalence of musculoskeletal disorders in dentists. BMC Musculoskelet. Disord. 2004, 5, 16. [Google Scholar] [CrossRef] [Green Version]
- Leggat, P.A.; Kedjarune, U.; Smith, D.R. Occupational Health Problems in Modern Dentistry: A Review. Ind. Health 2007, 45, 611–621. [Google Scholar] [CrossRef] [Green Version]
- Abduljabbar, T.A. Musculoskeletal disorders among dentists in Saudi Arabia. Pak. Oral Dent. J. 2008, 28, 135–144. [Google Scholar]
- Alrumi, A.; Alsheraimi, A.; Alassaf, S.; Alharbi, A.; Alenezi, A.; Almajed, A.; Alshetan, N.; Alomairiy, K.; Safadi, R.; Aboalela, A. Prevalence and Characterization of Musculoskeletal Disorders among Dental Students, Interns, and Residents in Riyadh, Saudi Arabia. Med. Sci. 2020, 24, 2565–2572. [Google Scholar]
- Šagát, P.; Bartík, P.; Prieto González, P.; Tohănean, D.I.; Knjaz, D. Impact of COVID-19quarantine on low back pain intensity, prevalence, and associated risk factors among adult citizens residing in riyadh (Saudi Arabia): A cross-sectional study. Int. J. Environ. Res. Public Health 2020, 17, 7302. [Google Scholar] [CrossRef] [PubMed]
- Hashim, R.; Salah, A.; Mayahi, F.; Haidary, S. Prevalence of postural musculoskeletal symptoms among dental students in United Arab Emirates. BMC Musculoskelet. Disord. 2021, 22, 30. [Google Scholar] [CrossRef]
- Sakzewski, L.; Naser-ud-Din, S. Work-related musculoskeletal disorders in dentists and orthodontists: A review of the literature. Work 2014, 48, 37–45. [Google Scholar] [CrossRef]
- Proteau, R.-A. Prevention of Work-Related Musculoskeletal Disorders (MSDs) in Dental Clinics; Asstsas: Montreal, QC, Canada, 2009. [Google Scholar]
- Wazzan, K.A.A.; Almas, K.; Qahtani, M.Q.A.; Shethri, S.E.A.; Khan, N. Prevalence of ocular injuries, conjunctivitis and use of eye protection among dental personnel in Riyadh, Saudi Arabia. Int. Dent. J. 2001, 51, 89–94. [Google Scholar] [CrossRef]
- Roll, S.C.; Tung, K.D.; Chang, H.; Sehremelis, T.A.; Fukumura, Y.E.; Randolph, S.; Forrest, J.L. Prevention and rehabilitation of musculoskeletal disorders in oral health care professionals: A systematic review. J. Am. Dent. Assoc. 2019, 150, 489–502. [Google Scholar] [CrossRef]
- Koni, A.; Kufersin, M.; Ronchese, F.; Travan, M.; Cadenaro, M.; Filon, F.L. Approach to prevention of musculoskeletal symptoms in dental students: An interventional study. Med. Lavoro 2018, 109, 276. [Google Scholar] [PubMed]
- Sweeney, K.; Mackey, M.; Spurway, J.; Clarke, J.; Ginn, K. The effectiveness of ergonomics interventions in reducing upper limb work-related musculoskeletal pain and dysfunction in sonographers, surgeons and dentists: A systematic review. Ergonomics 2021, 64, 1–38. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.H.; Lee, J.H.; Lee, Y.S.; Kim, M.K.; Kim, S.G. Changes in the activity of the muscles surrounding the neck according to the angles of movement of the neck in adults in their 20s. J. Phys. Ther. Sci. 2015, 27, 973–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galleano, R.; Carter, F.; Brown, S.; Frank, T.; Cuschieri, A. Can armrests improve comfort and task performance in laparoscopic surgery? Ann. Surg. 2006, 243, 329. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Zamparini, F.; Spinelli, A.; Risi, A.; Prati, C. Musculoskeletal Disorders among Italian Dentists and Dental Hygienists. Int. J. Environ. Res. Public Health 2021, 18, 2705. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Characteristics | n (%) or Mean ± SD |
|---|---|
| Gender, n (%) | |
| Female | 245 (69%) |
| Male | 110 (31%) |
| Age, mean ± SD | 33.6 ± 8.1 |
| Height, mean ± SD | 162.7 ± 9.8 |
| Weight, mean ± SD | 69.8 ± 19.5 |
| BMI, mean ± SD | 26.2 ± 5.9 |
| Underweight (<18.5 kg/m2) | 17 (5%) |
| Normal (18.5–25 kg/m2) | 159 (44%) |
| Overweight (25–29.9 kg/m2) | 105 (29%) |
| Obese (>30 kg/m2) | 75 (21%) |
| Occupational characteristics, n (%) | |
| Occupation | |
| Dental assistant | 249 (70.1%) |
| Dental lab technician | 64 (18%) |
| Dental sterilization technician | 32 (9%) |
| Dental radiology technician | 10 (2.8%) |
| Work setting | |
| Governmental hospital | 106 (29.9%) |
| Governmental dental centre | 76 (21.4%) |
| Academic dental clinic | 45 (12.7%) |
| Private dental clinic | 105 (29.6%) |
| Private dental lab | 17 (4.8%) |
| Other | 6 (1.7%) |
| Years of experience | |
| 0.5–1 year | 38 (10.7%) |
| 1–3 years | 84 (23.7%) |
| 3–5 years | 57 (16%) |
| 5–10 years | 80 (22.5%) |
| 10–15 years | 53 (14.9%) |
| 15–20 years | 24 (6.8%) |
| More Than 20 Years | 19 (5.3%) |
| Working hours | |
| Less than 35 hours | 17 (4.8%) |
| 35–40 hours | 73 (20.6%) |
| 40–45 hours | 144 (40.6%) |
| More than 45 hours | 121 (34%) |
| Physical demands during working hours | |
| Less than 30% | 25 (7%) |
| 30–50% | 49 (14%) |
| 50–75% | 75 (21%) |
| More than 75% | 109 (31%) |
| 100% | 97 (27%) |
| Ergonomic knowledge, n (%) | |
| Awareness of proper work environment and posture | |
| Yes, provided by workplace | 98 (28%) |
| Yes, independently searched | 107 (30%) |
| No | 94 (26%) |
| Not sure | 56 (16%) |
| Follow ergonomic work positions | |
| All the time | 18 (5%) |
| Most of the time | 88 (25%) |
| Sometimes | 158 (45%) |
| Rarely | 53 (15%) |
| Never | 8 (2%) |
| Not sure | 30 (8%) |
| Having proper information about ergonomic work positions | |
| Yes | 139 (39%) |
| No | 70 (20%) |
| Maybe | 146 (41%) |
| Work-related injury, n (%) | |
| Yes | 63 (18%) |
| No | 235 (66%) |
| Not sure | 57 (16%) |
| Occupation | Neck | Shoulders | Upper Back | Elbows | Wrist/Hand | Lower Back | Hips/Thighs | Knees | Ankles/Feet |
|---|---|---|---|---|---|---|---|---|---|
| Dental assistant (n = 249) | 63% | 61.4% | 52.6% | 20.9% | 52.2% | 62.6% | 36.1% | 42.6% | 48.6% |
| Dental lab technician (n = 64) | 57.8% | 57.8% | 43.7% | 15.6% | 46.9% | 71.9% | 10.9% | 37.5% | 31.2% |
| Dental sterilization (n = 32) | 53.1% | 62.5% | 56.2% | 25% | 56.2% | 78.1% | 37.5% | 34.4% | 62.5% |
| Dental radiology technician (n = 10) | 70% | 70% | 30% | 20% | 60% | 80% | 20% | 40% | 70% |
| Occupation | Standing for Long Time | Sitting for Long Time | Lifting Heavy Objects | Pushing Carts or Heavy Objects | Walking Long Distances | Rotation | Bending | Repetitive Hand and Wrist Movement | Working with and/or Operating Large Machines | Working withand/or Operating Machines that Produce Vibration | Keeping an Uncomfortable Posture for Long Periods of Time |
| Dental assistant (n = 249) | 77.5% | 31.3% | 19.3% | 20% | 30.9% | 44.1% | 38.1% | 57.4% | 17.7% | 18.9% | 47.8% |
| Dental lab technician (n = 64) | 62.5% | 51.6% | 21.9% | 17.1% | 31.2% | 50% | 53.1% | 64% | 34.4% | 46.9% | 59.4% |
| Dental sterilization (n = 32) | 84.4% | 21.9% | 43.7% | 46.9% | 28.1% | 43.7% | 56.2% | 68.7% | 46.9% | 15.6% | 50% |
| Dental radiology technician (n = 10) | 80% | 20% | 30% | 20% | 10% | 60% | 50% | 70% | 20% | 0% | 60% |
| Total (All ADP) (n= 355) | 75.2% | 33.8% | 22.2% | 22% | 3.2% | 45.3% | 42.5% | 59.7% | 23.1% | 23.1% | 50.4% |
| Body Area | Dental Assistant (n = 249) | Dental Lab Technician (n = 64) | Dental Sterilization (n = 32) | Dental Radiology Technician (n = 10) | Total (n = 355) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Physician Visits | Pain Medication | Physician Visits | Pain Medication | Physician Visits | Pain Medication | Physician Visits | Pain Medication | Physician Visits | Pain Medication | |
| Neck | 24.1% | 30.1% | 20.3% | 28.3% | 28.1% | 43.7% | 30% | 40% | 23.9% | 31.3% |
| Shoulders | 20% | 30.1% | 26.6% | 28.1% | 21.9% | 34.4% | 40% | 40% | 22% | 30.4% |
| Upper back | 17.7% | 23.3% | 18.7% | 20.3% | 34.4% | 28.1% | 40% | 20% | 20% | 23.1% |
| Elbows | 10.4% | 8% | 9.4% | 4.7% | 12.5% | 6.2% | 10% | 0% | 10.4% | 7% |
| Wrist/Hands | 18.5% | 17.7% | 15.6% | 17.2% | 21.9% | 28.1% | 30% | 20% | 18.6% | 18.6% |
| Lower Back | 27.3% | 36.9% | 21.9% | 31.2% | 43.7% | 50% | 40% | 60% | 28.2% | 37.7% |
| Hips/Thighs | 12.4% | 10.8% | 14% | 9.4% | 9.4% | 15.6% | 10% | 10% | 12.4% | 11% |
| Knees | 18% | 18% | 18.7% | 12.5% | 25% | 18.7% | 10% | 30% | 18.6% | 17.5% |
| Ankles | 19.7% | 20% | 17.2% | 12.5% | 28.1% | 18.7% | 30% | 50% | 20.3% | 19.4% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakhsh, H.R.; Bakhsh, H.H.; Alotaibi, S.M.; Abuzaid, M.A.; Aloumi, L.A.; Alorf, S.F. Musculoskeletal Disorder Symptoms in Saudi Allied Dental Professionals: Is there an Underestimation of Related Occupational Risk Factors? Int. J. Environ. Res. Public Health 2021, 18, 10167. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910167
Bakhsh HR, Bakhsh HH, Alotaibi SM, Abuzaid MA, Aloumi LA, Alorf SF. Musculoskeletal Disorder Symptoms in Saudi Allied Dental Professionals: Is there an Underestimation of Related Occupational Risk Factors? International Journal of Environmental Research and Public Health. 2021; 18(19):10167. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910167
Chicago/Turabian StyleBakhsh, Hadeel R., Heba H. Bakhsh, Seham M. Alotaibi, Maha A. Abuzaid, Latefah A. Aloumi, and Shoug F. Alorf. 2021. "Musculoskeletal Disorder Symptoms in Saudi Allied Dental Professionals: Is there an Underestimation of Related Occupational Risk Factors?" International Journal of Environmental Research and Public Health 18, no. 19: 10167. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910167