
Risk Modifying Factors of Anxiety and Depressive Disorders, Using the Example of a Population Study in the Żywiec District

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Limitation
6. Conclusions
6.1. Concerning the Risk of Depressive Disorders
- Being female;
- Age over 60;
- Being unemployed;
- Lower than secondary education;
- Performing mental work;
- Complete lack of physical activity and daily, intensive sports;
- Regular smoking of cigarettes;
- Chronic somatic diseases;
- Abuse of hypnotics and over-the-counter drugs with sedative potential.
- Male gender;
- Age between 40 and 59;
- Higher education;
- Full-time employment or self-employment;
- Performing physical work.
- Marital status;
- Place of residence;
- Use of alcohol, marijuana and stimulants.
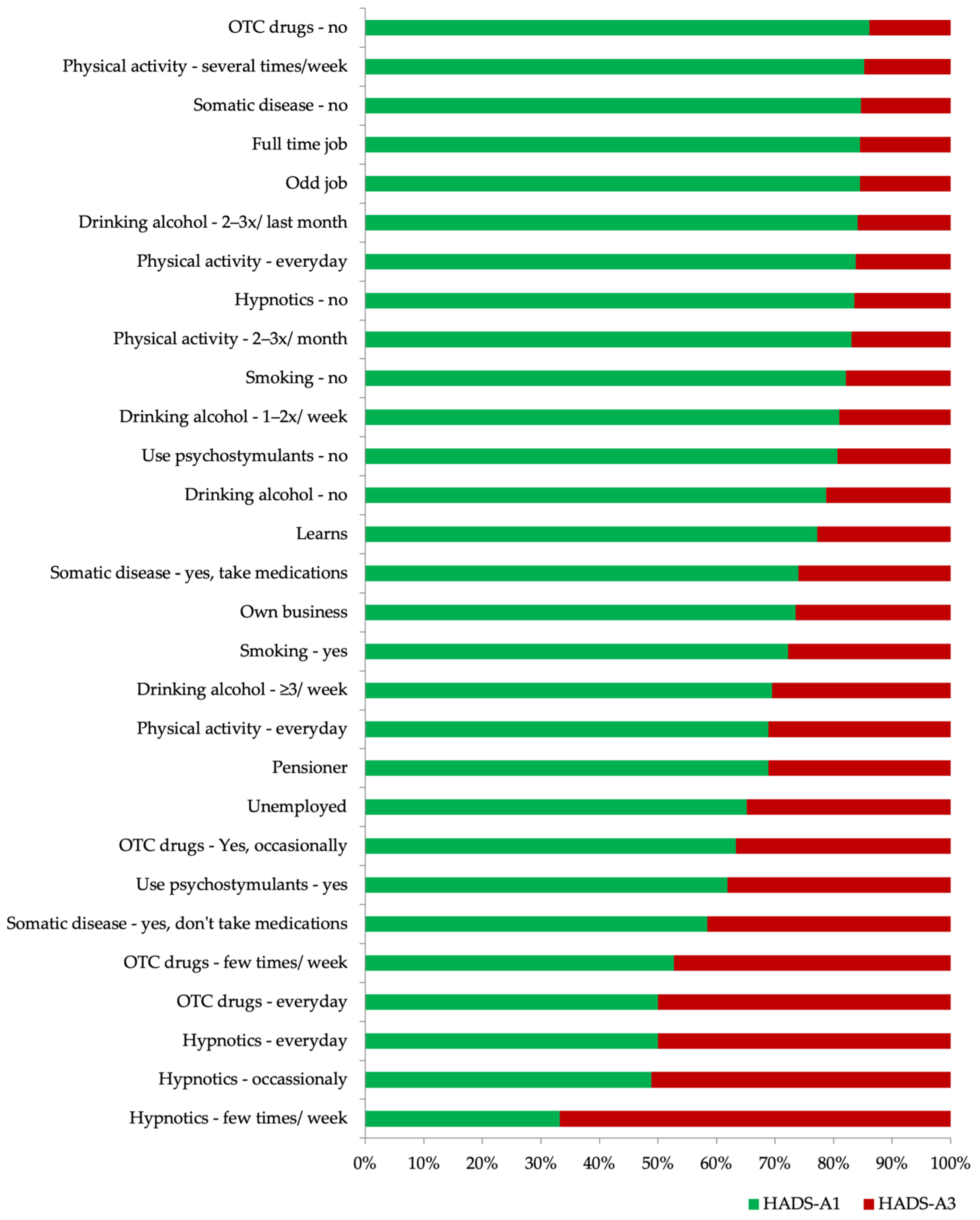
6.2. Concerning the Risk of Anxiety Disorders
- Belonging to the group of the unemployed, self-employed or retired;
- Lack of physical activity;
- Daily use of alcohol or complete abstinence;
- Regular smoking and the use of stimulants;
- The presence of somatic diseases;
- Over-the-counter drugs and drugs prescribed by a doctor to help with sleep.
- Employed full-time;
- Occasional alcohol users.
- The sex of respondents;
- Marital status;
- Living in a village or city;
- Level of education;
- Type of job;
- Marijuana use.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Mental Health Action Plan 2013–2020. Available online: https://www.who.int/mental_health/publications/action_plan/en/ (accessed on 12 June 2021).
- Jaeschke, R.; Siwek, M.; Grabski, B.; Dudek, D. Comorbidity of depressive and anxiety disorders. Psychiatria 2010, 7, 189–197. [Google Scholar]
- Kiejna, A.; Piotrowski, P.; Adamowski, T.; Moskalewicz, J.; Wciórka, J.; Stokwiszewski, J.; Rabczenko, D.; Kessler, R. The prevalence of common mental disorders in the population of adult Poles by sex and age structure—An EZOP Poland study. Psychiatr. Pol. 2015, 49, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.; Angermeyer, M.C.; Bernert, S.; Bruffaerts, R.; Brugha, T.S.; Bryson, H.; de Girolamo, G.; Graaf, R.; Demyttenaere, K.; Gasquet, I.; et al. Prevalence of mental disorders in Europe: Results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr. Scand Suppl. 2004, 420, 21–27. [Google Scholar]
- Ministry of Health. Depression Prevention Program in Poland for Years 2016–2020. Available online: https://www.gov.pl/web/zdrowie/program-zapobiegania-depresji-w-polsce-na-lata-2016-2020 (accessed on 12 June 2021).
- Modrzejewska, R.; Bomba, J. Prevalence of mental disorders and psychoactive substance use in metropolitan 17-year old youth population. Psychiatr. Pol. 2010, 44, 579–592. [Google Scholar]
- Suwalska, J.; Suwalska, A.; Szczygieł, M.; Łojko, D. Medical students and stigma of depression. Part 2. Self-stigma. Psychiatr. Pol. 2017, 51, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Zagdańska, M.; Kiejna, A. Prevalence and risk factors of depressive episodes among student population in Wroclaw—epidemiological study results. Psychiatr. Pol. 2016, 50, 631–641. [Google Scholar] [CrossRef] [PubMed]
- Schoevers, R.A.; Deeg, D.J.; van Tilburg, W.; Beekman, A.T. Depression and generalized anxiety disorder: Co-occurrence and longitudinal patterns in elderly patients. Am. J. Geriatr. Psychiatry 2005, 13, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Pawlak, A.; Krejca, M.; Janas-Kozik, M.; Krupka-Matuszczyk, I.; Rajewska, J.; Bochenek, A. Evaluation of anxiety and depression in the perioperative period in patients subjected to myocardial revascularization. Psychiatr. Pol. 2012, 46, 63–74. [Google Scholar]
- Duda-Sobczak, A.; Wierusz-Wysocka, B. Diabetes mellitus and psychiatric diseases. Psychiatr. Pol. 2011, 45, 589–598. [Google Scholar]
- Wasilewski, D.; Wojnar, M.; Chatizow, J. Depression and pain: Polish epidemiologic study. Psychiatr. Pol. 2010, 44, 435–445. [Google Scholar]
- Babiarczyk., B.; Schlegel-Zawadzka, M.; Turbiarz, A. Assessment of the prevalence of depressive symptoms in a population of people aged over 65. Med. Og. Nauk. Zdr. 2013, 19, 453–457. [Google Scholar]
- Burzynska, M.; Maniecka-Bryła, I. The Occurance of Depression in Older People Using Social Care—Preliminary Results. Acta Univ. Lodz. Folia Oeconomica 2013, 19, 453–457. [Google Scholar]
- Zigmond, A.; Snaith, R. The Hospital Anxiety And Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Djukanovic, I.; Carlsson, J.; Årestedt, K. Is the Hospital Anxiety and Depression Scale (HADS) a valid measure in a general population 65–80 years old? A psychometric evaluation study. Health Qual. Life Outcomes 2017, 15, 193. [Google Scholar] [CrossRef] [Green Version]
- Parker, G.; Brotchie, H. Gender differences in depression. Int. Rev. Psychiatry 2010, 22, 429–436. [Google Scholar] [CrossRef]
- Faravelli, C.; Scarpato, A.M.; Castellini, G.; Sauro, C.L. Gender differences in depression and anxiety: The role of age. Psychiatry Res. 2013, 210, 1301–1303. [Google Scholar] [CrossRef]
- Salk, R.H.; Hyde, J.S.; Abramson, L.Y. Gender differences in depression in representative national samples: Meta-analyses of diagnoses and symptoms. Psychol. Bull. 2017, 143, 783–822. [Google Scholar] [CrossRef]
- Kiely, K.M.; Brady, B.; Byles, J. Gender, mental health and ageing. Maturitas 2019, 129, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Riecher-Rössler, A. Sex and gender differences in mental disorders. Lancet Psychiatry 2017, 4, 8–9. [Google Scholar] [CrossRef]
- Stachoń, A.J. Feeling of the selected climacteric symptoms depending on the climacteric phase and type of menopause. Przegląd Menopauzalny 2013, 4, 315–320. [Google Scholar] [CrossRef] [Green Version]
- Nezlek, J.B.; Rusanowska, M.; Holas, P.; Krejtz, I. The factor structure of a Polish language version of the hospital anxiety depression scale (HADS). Curr. Psychol. 2019, 40, 2318–2326. [Google Scholar] [CrossRef] [Green Version]
- Stone, A.A.; Schwartz, J.E.; Broderick, J.E.; Deaton, A. A snapshot of the age distribution of psychological well-being in the United States. Proc. Natl. Acad. Sci. USA 2010, 107, 9985–9990. [Google Scholar] [CrossRef] [Green Version]
- Franczok-Kuczmowska, A.; Kuzian, M. Psychosocial conditions of mental health and functioning in early adulthood. Ann. Univ. Paedagog. Cracoviensis. Studia Psychol. 2018, 11, 115–134. [Google Scholar] [CrossRef]
- Valkanova, V.; Ebmeier, K.P. Vascular risk factors and depression in later life: Systematic review and meta-analysis. Biol. Psychiatry 2013, 73, 406–413. [Google Scholar] [CrossRef]
- Mossakowska, M.; Więcek, A.; Błędowski, P. Medical, Psychological, Sociological and Economic Aspects of Aging People in Poland, 1st ed.; Termedia: Poznań, Poland, 2012; pp. 407–419. [Google Scholar]
- Leray, E.; Camara, A.; Drepier, D.; Riou, F.; Bougeant, N.; Pelissolo, A.; Lloyd, K.R.; Bellamy, V.; Roelandt, J.L.; Millet, B. Prevalence, characteristics and comorbidities of anxiety disorders in France: Results from the “Mental Health in General Population” Survey (MHGP). Eur. Psychiatry 2011, 26, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Wolitzky-Taylor, K.B.; Castriotta, N.; Lenze, R.J.; Stanley, M.A.; Craske, M.G. Anxiety disorders in older adults: A comprehensive review. Depress. Anxiety 2010, 27, 190–211. [Google Scholar] [CrossRef]
- Brown, C.R.; Hambleton, I.R.; Sobers-Grannum, N.; Hercules, S.M.; Unwin, N.; Harris, E.N.; Wilks, R.; MacLeish, M.; Sullivan, L.; Murphy, M.M. Social determinants of depression and suicidal behaviour in the Caribbean: A systematic review. BMC Public Health 2017, 17, 577. [Google Scholar] [CrossRef] [Green Version]
- Frąckowiak-Sochańska, M. Family and sociocultural factors in mental disorders. An analysis from the point of view of the sociocultural gender. Rocz. Socjol. Rodz. 2010, 20, 153–185. [Google Scholar]
- Peen, J.; Schoevers, R.A.; Beekman, A.T.; Dekker, J. The current statusof urban-rural differences in psychiatric disorders. Acta Psychiatr. Scand. 2010, 121, 84–93. [Google Scholar] [CrossRef]
- Ślusarz, R.; Borzyszkowska, A.; Szrajda, J.; Fidecki, W.; Haor, B. Influence of selected socio-demographic factors on incidence of depressive disorders in women. Nurs. Probl. 2011, 19, 21–26. [Google Scholar]
- The Urbanization of the Country and Its Stages. Available online: http://www.irwirpan.waw.pl/dir_upload/site/files/Monografia/02_Czarnecki.pdf (accessed on 12 June 2021).
- Orzechowska, A.; Florkowski, A.; Gruszczyński, W.; Zboralski, K.; Wysokiński, A.; Gałecki, P.; Talarowska, M. Socio-economic status, aggressive behaviours and coping with stress. Psychiatr. Pol. 2009, 43, 53–63. [Google Scholar]
- Niemeyer, H.; Bieda, A.; Michalak, J.; Schneider, S.; Margraf, J. Education and mental health: Do psychosocial resources matter? SSM Popul. Health 2019, 7, 100392. [Google Scholar] [CrossRef]
- Public Opinion Research Center. Activities and Experiences od Poles in 2012. Available online: https://www.cbos.pl/SPISKOM.POL/2013/K_013_13.PDF (accessed on 12 June 2021).
- Żołnierczyk-Zreda, D.; Holas, P. Psychosocial Working Conditions and Major Depression or Depressive Disorders: Review of StudiES. Med. Pr. 2018, 69, 573–581. [Google Scholar]
- Cybula-Fujiwara, A.; Merecz-Kot, D.; Walusiak-Skorupa, J.; Marcinkiewicz, A.; Wiszniewska, M. Employees with mental illness—Possibilities and barriers in professional activity. Med. Pr. 2015, 66, 57–69. [Google Scholar] [CrossRef]
- Grzanka-Tykwińska, A.; Kędziora-Kornatowska, K. The significance of selected forms of activity in elderly people’s lives. Gerontol. Pol. 2010, 18, 29–32. [Google Scholar]
- Kostrzewski, S.; Worach-Kardas, H. Effects of unemployment on health and quality of life in older production age group. Hygeia Public Health 2015, 50, 372–382. [Google Scholar]
- Nunan, D.; Mahtani, K.R.; Roberts, N.; Heneghan, C. Physical activity for the prevention and treatment of major chronic disease: An overview of systematic reviews. Syst. Rev. 2013, 10, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kandola, A.; Vancampfort, D.; Herring, M.; Rebar, A.; Hallgren, M.; Firth, J.; Stubbs, B. Moving to Beat Anxiety: Epidemiology and Therapeutic Issues with Physical Activity for Anxiety. Curr. Psychiatry Rep. 2018, 20, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guszkowska, M. Exercise dependence—Symptoms and mechanisms. Psychiatr. Pol. 2012, 46, 845–856. [Google Scholar] [PubMed]
- Dyrla-Mularczyk, K.; Giemza-Urbanowicz, W. The influence of physical activity on the functioning of the nervous system and cognitive processes—Research review. Neuropsychiatry Neuropsychol. 2019, 14, 84–91. [Google Scholar] [CrossRef]
- Klimkiewicz, A.; Klimkiewicz, J.; Jakubczyk, A.; Kieres-Salomoński, I.; Wojnar, M. Comorbidity of alcohol dependence with other psychiatric disorders. Part I. Epidemiology of dual diagnosis. Psychiatr. Pol. 2015, 49, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Mathew, A.R.; Hogarth, L.; Leventhal, A.M.; Cook, J.W.; Hitsman, B. Cigarette smoking and depression co morbidity: Systematic review and proposed theoretical model. Addiction 2016, 112, 401–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fluharty, M.; Taylor, A.E.; Grabski, M.; Munafò, M.R. The Association of Cigarette Smoking With Depression and Anxiety: A Systematic Review. Nicotine Tob. Res. 2016, 19, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Boden, J.M.; Fergusson, D.M.; Horwood, L.J. Cigarette smoking and depression: Tests of causal linkages using a longitudinal birth cohort. Br. J. Psychiatry 2010, 196, 440–446. [Google Scholar] [CrossRef]
- Brook, J.S.; Lee, J.Y.; Brown, E.N.; Finch, S.J. Co morbid trajectories of tobacco and marijuana use as related to psychological outcomes. Subst. Abus. 2012, 33, 156–167. [Google Scholar] [CrossRef] [Green Version]
- Flensborg-Madsen, T.; Bay von Scholten, M.; Flachs, E.M.; Mortensen, E.L.; Prescott, E.; Tolstrup, J.S. Tobacco smoking as a risk factor for depression. A 26-year population-based follow-up study. J. Psychiatr. Res. 2011, 45, 143–149. [Google Scholar] [CrossRef]
- Dąbrowska, K.; Miturska, E.; Moskalewicz, J. The consequences of marijuana use and abuse—A review. Alcohol. Drug Addict. 2012, 25, 167–186. [Google Scholar]
- Więckiewicz, G.; Smardz, J.; Wieczorek, T.; Rymaszewska, J.; Grychowska, N.; Danel, D.; Więckiewicz, M. Patterns of synthetic cathinones use and their impact on depressive symptoms and parafunctional oral behaviors. Psychiatr. Pol. 2020, 165, 1–19. [Google Scholar] [CrossRef]
- Harro, J. Neuropsychiatric Adverse Effects of Amphetamine and Methamphetamine. Neuropsychiatr. Complicat. Stimul. Abus. 2015, 120, 179–204. [Google Scholar]
- Hellem, T.L. A Review of Methamphetamine Dependence and Withdrawal Treatment: A Focus on Anxiety Outcomes. J. Subst. Abus. Treat. 2016, 71, 16–22. [Google Scholar] [CrossRef]
- Assari, S.; Burgard, S.; Zivin, K. Long-term reciprocal associations between depressive symptoms and numer of chronic medical conditions: Longitudinal support for Black-White health paradox. J. Racial Ethn. Health Disparies. 2015, 2, 589–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuśmierek, M.; Florkowski, A.; Gałecki, P.; Talarowska, M. Co-occurrence of mental and somatic disorders in patients diagnosed with depression. Curr. Probl. Psychiatry 2011, 12, 285–292. [Google Scholar]
- Gerrits, M.M.; van Oppen, P.; van Marwijk, H.W.; Penninx, B.W.; van der Horst, H.E. Pain and the onset of depressive and anxiety disorders. Pain 2014, 155, 53–59. [Google Scholar] [CrossRef]
- Potoczek, A. Links between duration and severity of anxiety and depressive symptoms with defense mechanisms, coherence and family functioning in patients suffering from severe panic disorder. Psychiatr. Pol. 2010, 44, 101–116. [Google Scholar] [PubMed]
- Polish Patient’s Own Portrait. Report on Adherence to Therapeutic Recommendations by Polish Patients. Foundation for Supporting the Development of Polish Pharmacy and Medicine. Available online: http://docplayer.pl/5801098-Polskiego-pacjenta-portret-wlasny.html (accessed on 12 June 2021).
- Leksowska, A.; Jaworska, I.; Gorczyca, P. Somatic disease as an adaptation challenge for humans. Folia Cardiol. Excerpta 2011, 6, 244–248. [Google Scholar]
- Nowicki, Z.; Grabowski, K.; Cubała, W.J.; Nowicka-Sauer, K.; Zdrojewski, T.; Rutkowski, M. and Bandosz, P. Prevalence of self-reported insomnia in general population of Poland. Psychiatr. Pol. 2016, 50, 165–173. [Google Scholar] [CrossRef]
- Murphy, M.J.; Peterson, M.J. Sleep Disturbances in Depression. Sleep Med. Clin. 2015, 10, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Bao, Y.P.; Han, Y.; Ma, J.; Wang, R.-J.; Shi, L.; Wang, T.-Y.; He, J.; Yue, J.L.; Shi, J.; Tang, X.D.; et al. Cooccurrence and bidirectional prediction of sleep disturbances and depression in older adults: Meta-analysis and systematic review. Neurosci. Biobehav. Rev. 2017, 75, 257–273. [Google Scholar] [CrossRef]
- Cox, R.C.; Olatunji, B.O. A systematic review of sleep disturbance in anxiety and related disorders. J. Anxiety Disord. 2016, 37, 104–129. [Google Scholar] [CrossRef]
- Bażydło, M.; Żułtak-Bączkowska, K.; Zaremba-Pechmann, L.; Rotter, I.; Ka rakiewicz, B. Analysis of the OTC treatment without consultation in different age groups and evaluation of need for health education. Family Med. Primary Care Rev. 2010, 12, 127–130. [Google Scholar]
- Szafrański, T. Herbal remedies in depression—State of the art. Psychiatr. Pol. 2014, 48, 59–73. [Google Scholar] [CrossRef] [PubMed]
- Sarris, J. Herbal medicines in the treatment of psychiatric disorders: 10-year updated review. Phytother. Res. 2018, 32, 1147–1162. [Google Scholar] [CrossRef]
- Hamann, J.; Linde, K.; Schweiger, H.D.; Kusmakow, O.; Förstl, H. Over-the-Counter-Drugs for the Treatment of Mood and Anxiety Disorders—The Views of German Pharmacists. Pharmacopsychiatry 2014, 47, 84–88. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Risk Modifying Factors | Study Group | |
|---|---|---|
| n | % | |
| Professional activity | ||
| Full time | 1044 | 62.9 |
| Own business | 120 | 7.2 |
| Odd jobs | 73 | 4.4 |
| Studying | 126 | 7.6 |
| Unemployed | 90 | 5.4 |
| Pensioner | 206 | 12.4 |
| Type of job | ||
| Physical work | 707 | 42.6 |
| Mental work | 463 | 27.9 |
| Unemployed | 489 | 29.5 |
| Physical activity | ||
| Never | 414 | 24.9 |
| Occasional (2–3x/month) | 725 | 43.7 |
| Several times/week | 406 | 24.5 |
| Every day (regularly) | 114 | 6.9 |
| Frequency of drinking alcohol | ||
| Not at all/last month | 665 | 40.1 |
| 2–3 times/last month | 588 | 35.4 |
| 1–2 times/week | 285 | 17.2 |
| 3 or more times/week | 121 | 7.3 |
| Smoking | ||
| Yes | 329 | 19.8 |
| No | 1330 | 80.2 |
| The use of cannabinoids | ||
| Yes | 62 | 3.7 |
| No | 1597 | 96.3 |
| The use of psychostimulants | ||
| Yes | 22 | 1.3 |
| No | 1637 | 98.7 |
| Presence and treatment of somatic diseases | ||
| “I get sick, I take medications regularly” | 455 | 27.4 |
| “I get sick, I don’t take medications” | 108 | 6.5 |
| “I’m not sick” | 1096 | 66.1 |
| The use of hypnotics | ||
| No | 1513 | 91.2 |
| Yes, occasionally | 105 | 6.3 |
| A few times a week | 22 | 1.3 |
| Every day | 19 | 1.1 |
| Use of sedative or hypnotic herbal medications or OTC dietary supplements | ||
| No | 1270 | 76.6 |
| Yes, occasionally | 299 | 18 |
| A few times a week | 47 | 2.8 |
| Yes everyday | 43 | 2.6 |
| Risk Modifying Factor | HADS-D1 | HADS-D2 | HADS-D3 | p-Value | HADS-A1 | HADS-A2 | HADS-A3 | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | |||
| Sex | ||||||||||||||
| Female | 578 | 61.9 | 181 | 19.4 | 175 | 18.7 | <0.01 | 736 | 78.8 | 113 | 12.1 | 85 | 9.1 | NS * |
| Male | 566 | 78.1 | 94 | 13.0 | 65 | 8.9 | <0.01 | 539 | 74.3 | 85 | 11.7 | 101 | 13.9 | NS |
| Age range | ||||||||||||||
| 18–39 years | 540 | 84.5 | 78 | 12.2 | 21 | 3.3 | <0.01 | 444 | 69.5 | 99 | 15.5 | 96 | 15 | NS |
| 40–59 years | 656 | 84.2 | 79 | 10.1 | 44 | 5.7 | <0.01 | 522 | 67 | 128 | 16.4 | 129 | 16.6 | NS |
| ≥60 years | 107 | 44.3 | 50 | 20.8 | 84 | 34.9 | <0.01 | 152 | 63 | 39 | 16.2 | 50 | 20.8 | NS |
| Marital status | ||||||||||||||
| Single | 394 | 79.6 | 64 | 12.9 | 37 | 7.5 | NS | 335 | 67.7 | 73 | 14.8 | 87 | 17.6 | NS |
| Steady relationship | 909 | 78.1 | 143 | 12.3 | 112 | 9.6 | NS | 783 | 67.3 | 193 | 16.6 | 188 | 16.2 | NS |
| Place of residence | ||||||||||||||
| City | 398 | 81.1 | 59 | 12 | 34 | 6.9 | NS | 337 | 68.6 | 81 | 16.5 | 73 | 14.9 | NS |
| Village | 905 | 77.5 | 148 | 12.7 | 115 | 9.9 | NS | 781 | 66.9 | 185 | 15.8 | 202 | 17.3 | NS |
| Education | ||||||||||||||
| Basic | 100 | 66.2 | 27 | 17.9 | 24 | 15.9 | <0.01 | 93 | 61.6 | 25 | 16.6 | 33 | 21.9 | NS |
| Vocational | 302 | 74.8 | 50 | 12.4 | 52 | 12.8 | <0.01 | 257 | 63.6 | 64 | 15.8 | 83 | 20.5 | NS |
| Medium | 507 | 81.1 | 73 | 11.7 | 45 | 7.2 | <0.01 | 425 | 68 | 110 | 17.6 | 90 | 14.4 | NS |
| Higher (Bachelor’s D.) | 125 | 84.5 | 13 | 8.8 | 10 | 6.8 | <0.01 | 108 | 72.9 | 19 | 12.8 | 21 | 14.2 | NS |
| Higher (Master’s D.) | 269 | 81.3 | 44 | 13.3 | 18 | 5.4 | <0.01 | 235 | 71 | 48 | 14.5 | 48 | 14.5 | NS |
| Professional activity | ||||||||||||||
| Full time | 930 | 89.1 | 85 | 8.1 | 29 | 2.8 | <0.01 | 749 | 71.7 | 158 | 15.1 | 137 | 13.1 | <0.01 |
| Own business | 102 | 85.0 | 15 | 12.5 | 3 | 2.5 | <0.01 | 75 | 62.5 | 18 | 15 | 27 | 22.5 | <0.01 |
| Odd jobs | 69 | 94.5 | 1 | 1.4 | 3 | 4.1 | <0.01 | 49 | 67.1 | 15 | 20.6 | 9 | 12.3 | <0.01 |
| Studying | 93 | 73.8 | 28 | 22.2 | 5 | 4.0 | <0.01 | 81 | 64.3 | 21 | 16.7 | 24 | 19 | <0.01 |
| Unemployed | 63 | 70 | 23 | 25.6 | 4 | 4.4 | <0.01 | 49 | 54.4 | 15 | 16.7 | 26 | 28.9 | <0.01 |
| Pensioner | 46 | 22.3 | 55 | 26.7 | 105 | 51 | <0.01 | 115 | 55.8 | 39 | 18.9 | 52 | 25.2 | <0.01 |
| Type of job | ||||||||||||||
| Physical | 678 | 97.7 | 13 | 1.9 | 3 | 0.4 | <0.01 | 482 | 69.5 | 113 | 16.3 | 99 | 14.3 | NS |
| Mental | 374 | 80.8 | 64 | 13.8 | 25 | 5.4 | <0.01 | 325 | 70.2 | 64 | 13.8 | 64 | 13.8 | NS |
| Not working | 12 | 92.3 | 1 | 7.7 | 0 | 0 | <0.01 | 8 | 61.5 | 0 | 0 | 5 | 38.5 | NS |
| Physical activity | ||||||||||||||
| Never | 294 | 71 | 53 | 12.8 | 67 | 16.2 | <0.01 | 230 | 55.6 | 80 | 19.3 | 104 | 25.1 | <0.01 |
| Occasional (2–3x/month) | 611 | 84.3 | 79 | 10.9 | 35 | 4.8 | <0.01 | 501 | 69.1 | 122 | 16.8 | 102 | 14.1 | <0.01 |
| Several times/week | 314 | 77.3 | 59 | 14.5 | 33 | 8.1 | <0.01 | 299 | 73.7 | 55 | 13.6 | 52 | 12.8 | <0.01 |
| Every day (regularly) | 84 | 73.7 | 16 | 14 | 14 | 12.3 | <0.01 | 88 | 77.2 | 9 | 7.9 | 17 | 14.9 | <0.01 |
| Drinking alcohol | ||||||||||||||
| Not at all/last month | 515 | 77.4 | 83 | 12.5 | 67 | 10.1 | NS | 448 | 67.4 | 96 | 14.4 | 121 | 18.2 | <0.01 |
| 2–3 times/last month | 474 | 80.6 | 70 | 11.9 | 44 | 7.5 | NS | 402 | 68.4 | 110 | 18.7 | 76 | 12.9 | <0.01 |
| 1–2 times/week | 223 | 78.3 | 37 | 12.9 | 25 | 8.8 | NS | 195 | 68.4 | 44 | 15.4 | 46 | 16.1 | <0.01 |
| 3 or more times/week | 91 | 75.2 | 17 | 14.1 | 13 | 10.7 | NS | 73 | 60.3 | 16 | 13.2 | 32 | 26.5 | <0.01 |
| Smoking | ||||||||||||||
| Yes | 261 | 79.3 | 28 | 8.5 | 40 | 12.2 | <0.01 | 195 | 59.3 | 59 | 17.9 | 75 | 22.8 | <0.01 |
| No | 1042 | 78 | 179 | 13.5 | 109 | 8.2 | <0.01 | 923 | 69.4 | 207 | 15.6 | 200 | 15 | <0.01 |
| The use of cannabinoids | ||||||||||||||
| Yes | 55 | 88.7 | 5 | 8.1 | 2 | 3.2 | NS | 37 | 59.7 | 13 | 21 | 12 | 19.4 | NS |
| No | 1248 | 78 | 202 | 12.7 | 147 | 9.2 | NS | 1081 | 68 | 253 | 15.8 | 263 | 16.5 | NS |
| The use of psychostimulants | ||||||||||||||
| Yes | 20 | 90.9 | 1 | 4.6 | 1 | 4.6 | NS | 13 | 59.1 | 1 | 4.6 | 8 | 36.4 | <0.05 |
| No | 1281 | 78 | 205 | 12.6 | 148 | 9.1 | NS | 1103 | 68 | 265 | 16.2 | 266 | 16.3 | <0.05 |
| Presence and treatment of somatic diseases | ||||||||||||||
| “I get sick, I take medications regularly” | 306 | 67.3 | 68 | 15 | 81 | 17.8 | <0.01 | 268 | 58.9 | 93 | 20.4 | 94 | 20.7 | <0.01 |
| “I get sick, I don’t take medications” | 82 | 75.9 | 14 | 13 | 12 | 11.1 | <0.01 | 52 | 48.2 | 19 | 17.6 | 37 | 34.3 | <0.01 |
| “I’m not sick” | 915 | 83.5 | 125 | 11.4 | 56 | 5.1 | <0.01 | 798 | 72.8 | 154 | 14.1 | 144 | 13.2 | <0.01 |
| The use of drugs with a hypnotic effect | ||||||||||||||
| No | 1203 | 80 | 181 | 12 | 129 | 8.5 | NS | 1059 | 70 | 246 | 16.3 | 208 | 13.8 | <0.01 |
| Yes, occasionally | 75 | 71.4 | 17 | 16.2 | 13 | 12.4 | NS | 44 | 41.9 | 15 | 14.3 | 46 | 43.8 | <0.01 |
| A few times a week | 14 | 63.6 | 5 | 22.7 | 3 | 13.6 | NS | 6 | 27.3 | 4 | 18.2 | 12 | 55 | <0.01 |
| Every day | 11 | 57.9 | 4 | 21.1 | 4 | 21.1 | NS | 9 | 47.4 | 1 | 5.3 | 9 | 47.4 | <0.01 |
| The use of OTC drugs/supplements with a sedative or hypnotic effect | ||||||||||||||
| No | 1023 | 81 | 150 | 11.8 | 97 | 10.7 | <0.01 | 925 | 72.8 | 195 | 15.4 | 150 | 11.8 | <0.01 |
| Yes, occasionally | 225 | 75.3 | 42 | 14.1 | 32 | 10.7 | <0.01 | 157 | 52.5 | 51 | 17.1 | 91 | 30.4 | <0.01 |
| A few times a week | 29 | 61.7 | 8 | 17 | 10 | 21.3 | <0.01 | 19 | 40.4 | 11 | 23.4 | 17 | 36.2 | <0.01 |
| Yes everyday | 26 | 60.5 | 7 | 16.3 | 10 | 23.3 | <0.01 | 17 | 39.5 | 9 | 20.9 | 17 | 39.5 | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lubecka, B.; Lubecki, M.; Kasperczyk, J.; Jośko-Ochojska, J.; Pudlo, R. Risk Modifying Factors of Anxiety and Depressive Disorders, Using the Example of a Population Study in the Żywiec District. Int. J. Environ. Res. Public Health 2021, 18, 10248. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910248
Lubecka B, Lubecki M, Kasperczyk J, Jośko-Ochojska J, Pudlo R. Risk Modifying Factors of Anxiety and Depressive Disorders, Using the Example of a Population Study in the Żywiec District. International Journal of Environmental Research and Public Health. 2021; 18(19):10248. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910248
Chicago/Turabian StyleLubecka, Bogumiła, Marek Lubecki, Janusz Kasperczyk, Jadwiga Jośko-Ochojska, and Robert Pudlo. 2021. "Risk Modifying Factors of Anxiety and Depressive Disorders, Using the Example of a Population Study in the Żywiec District" International Journal of Environmental Research and Public Health 18, no. 19: 10248. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910248