
Interventions to Increase Leukocyte Testing during Treatment with Dimethyl Fumarate


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Use of the Dimethyl Fumarate MUET Safety Program
3.2. Interventions and WBC Monitoring
3.3. Adjusted Analyses
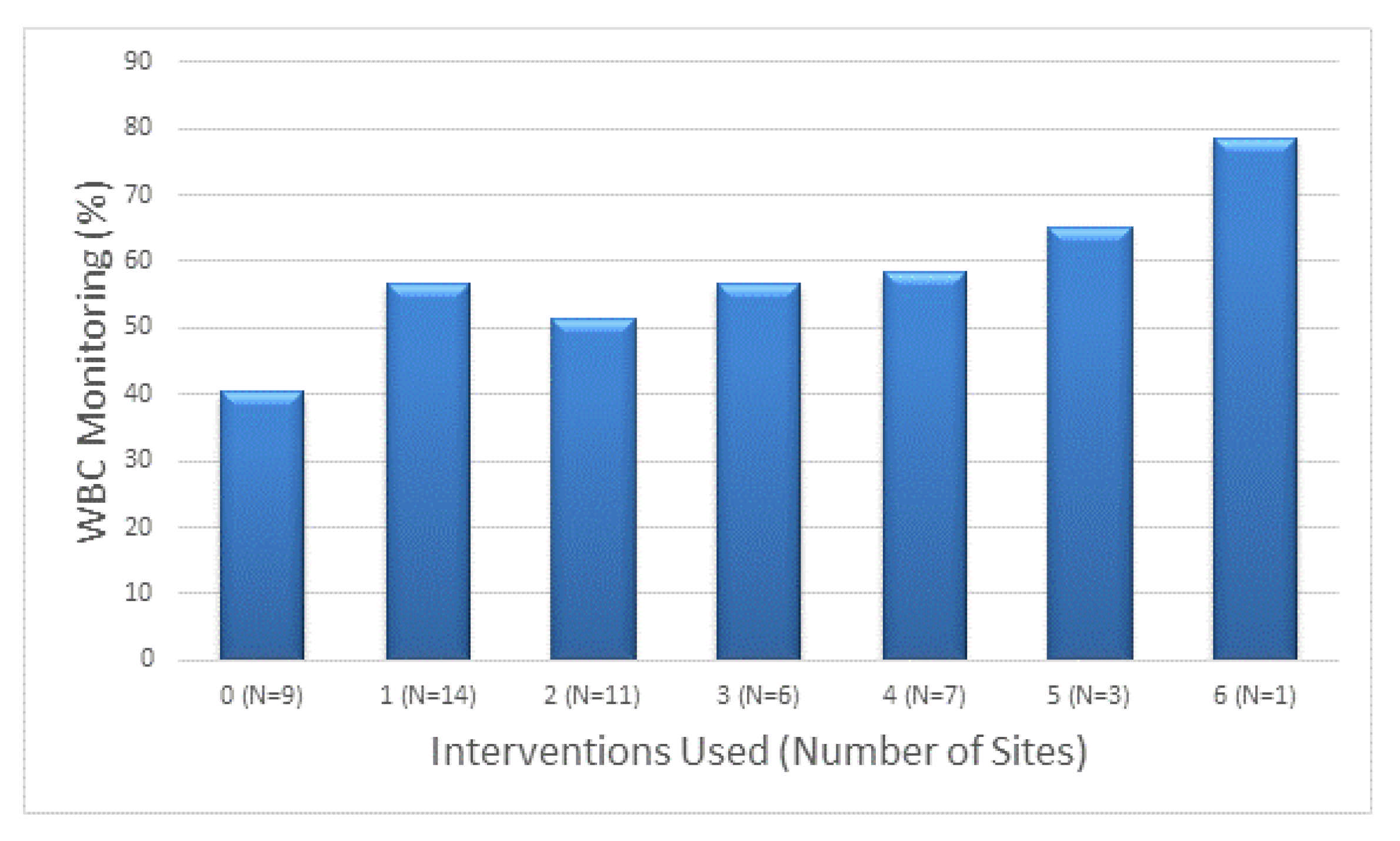
3.4. Number of Interventions
3.5. Barriers to Participation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lee, C.H.; Jiang, B.; Nakhaei-Nejad, M.; Barilla, D.; Blevins, G.; Giuliani, F. Cross-sectional analysis of peripheral blood mononuclear cells in lymphopenic and non-lymphopenic relapsing-remitting multiple sclerosis patients treated with dimethyl fumarate. Mult. Scler. Relat. Disord. 2021, 52, 103003. [Google Scholar] [CrossRef] [PubMed]
- Valencia-Sanchez, C.; Carter, J.L. An evaluation of dimethyl fumarate for the treatment of relapsing remitting multiple sclerosis. Expert Opin. Pharmacother. 2020, 21, 1399–1405. [Google Scholar] [CrossRef] [PubMed]
- Goldman, M.D.; Dwyer, L.; Coleman, R.; Sohn, M.W.; Stuve, O. Patient-specific factors modulate leukocyte response in dimethyl fumarate treated MS patients. PLoS ONE 2020, 15, e0228617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morales, F.S.; Koralnik, I.J.; Gautam, S.; Samaan, S.; Sloane, J.A. Risk factors for lymphopenia in patients with relapsing-remitting multiple sclerosis treated with dimethyl fumarate. J. Neurol. 2020, 267, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Saidu, N.E.B.; Kavian, N.; Leroy, K.; Jacob, C.; Nicco, C.; Batteux, F.; Alexandre, J. Dimethyl fumarate, a two-edged drug: Current status and future directions. Med. Res. Rev. 2019, 39, 1923–1952. [Google Scholar] [CrossRef]
- Mrowietz, U.; Barker, J.; Boehncke, W.H.; Iversen, L.; Kirby, B.; Naldi, L.; Reich, K.; Tanew, A.; van de Kerkhof, P.C.M.; Warren, R.B. Clinical use of dimethyl fumarate in moderate-to-severe plaque-type psoriasis: A European expert consensus. J. Eur. Acad. Dermatol. Venereol. 2018, 32 (Suppl. 3), 3–14. [Google Scholar] [CrossRef] [Green Version]
- Mehta, D.; Miller, C.; Arnold, D.L.; Bame, E.; Bar-Or, A.; Gold, R.; Hanna, J.; Kappos, L.; Liu, S.; Matta, A.; et al. Effect of dimethyl fumarate on lymphocytes in RRMS: Implications for clinical practice. Neurology 2019, 92, e1724–e1738. [Google Scholar] [CrossRef] [Green Version]
- Food and Drug Administration. Tecfidera [Prescribing Information]; Biogen: Cambridge, MA, USA, 2017. [Google Scholar]
- Burk, M.; Moore, V.; Glassman, P.; Good, C.B.; Emmendorfer, T.; Leadholm, T.C.; Cunningham, F. Medication-use evaluation with a Web application. Am. J. Health Syst. Pharm. 2013, 70, 2226–2234. [Google Scholar] [CrossRef]
- Van Hoof, T.J.; Harrison, L.G.; Miller, N.E.; Pappas, M.S.; Fischer, M.A. Characteristics of Academic Detailing: Results of a Literature Review. Am. Health Drug Benefits 2015, 8, 414–422. [Google Scholar]
- Saleem, J.J.; Patterson, E.S.; Militello, L.; Render, M.L.; Orshansky, G.; Asch, S.M. Exploring barriers and facilitators to the use of computerized clinical reminders. J. Am. Med. Inform. Assoc. 2005, 12, 438–447. [Google Scholar] [CrossRef] [Green Version]
- Alagoz, E.; Chih, M.Y.; Hitchcock, M.; Brown, R.; Quanbeck, A. The use of external change agents to promote quality improvement and organizational change in healthcare organizations: A systematic review. BMC Health Serv. Res. 2018, 18, 42. [Google Scholar] [CrossRef]
- Fischer, M.A. Academic Detailing in Diabetes: Using Outreach Education to Improve the Quality of Care. Curr. Diabetes Rep. 2016, 16, 98. [Google Scholar] [CrossRef]
- O’Brien, M.A.; Rogers, S.; Jamtvedt, G.; Oxman, A.D.; Odgaard-Jensen, J.; Kristoffersen, D.T.; Forsetlund, L.; Bainbridge, D.; Freemantle, N.; Davis, D.A.; et al. Educational outreach visits: Effects on professional practice and health care outcomes. Cochrane Database Syst. Rev. 2007, 4, CD000409. [Google Scholar] [CrossRef]
- Vandenberg, A.E.; Echt, K.V.; Kemp, L.; McGwin, G.; Perkins, M.M.; Mirk, A.K. Academic Detailing with Provider Audit and Feedback Improve Prescribing Quality for Older Veterans. J. Am. Geriatr. Soc. 2018, 66, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Aspinall, S.L.; Sales, M.M.; Good, C.B.; Calabrese, V.; Glassman, P.A.; Burk, M.; Moore, V.R.; Neuhauser, M.M.; Golterman, L.; Ourth, H.; et al. Pharmacy Benefits Management in the Veterans Health Administration Revisited: A Decade of Advancements, 2004–2014. J. Manag. Care Spec. Pharm. 2016, 22, 1058–1063. [Google Scholar] [PubMed] [Green Version]
- Lin, C.P.; Payne, T.H.; Nichol, W.P.; Hoey, P.J.; Anderson, C.L.; Gennari, J.H. Evaluating clinical decision support systems: Monitoring CPOE order check override rates in the Department of Veterans Affairs’ Computerized Patient Record System. J. Am. Med. Inform. Assoc. 2008, 15, 620–626. [Google Scholar] [CrossRef] [Green Version]
- American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 2012, 60, 616–631. [Google Scholar] [CrossRef] [PubMed]
- Vanderman, A.J.; Moss, J.M.; Bryan, W.E., III; Sloane, R.; Jackson, G.L.; Hastings, S.N. Evaluating the Impact of Medication Safety Alerts on Prescribing of Potentially Inappropriate Medications for Older Veterans in an Ambulatory Care Setting. J. Pharm. Pract. 2017, 30, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Gholami, P.; Sahay, A.; Massie, B.; Goldstein, M.K. Clinical reminders attached to echocardiography reports of patients with reduced left ventricular ejection fraction increase use of beta-blockers: A randomized trial. Circulation 2007, 115, 2829–2834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidenreich, P.A.; Chacko, M.; Goldstein, M.K.; Atwood, J.E. ACE inhibitor reminders attached to echocardiography reports of patients with reduced left ventricular ejection fraction. Am. J. Med. 2005, 118, 1034–1037. [Google Scholar] [CrossRef] [PubMed]
- Chrischilles, E.A.; Hourcade, J.P.; Doucette, W.; Eichmann, D.; Gryzlak, B.; Lorentzen, R.; Wright, K.; Letuchy, E.; Mueller, M.; Farris, K.; et al. Personal health records: A randomized trial of effects on elder medication safety. J. Am. Med. Inform. Assoc. 2014, 21, 679–686. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Intervention | Site Use N (%, 95% CI) | Mean Rate of WBC Monitoring (% of Patients) | p-Value | |
|---|---|---|---|---|
| Using Intervention | Not Using Intervention | |||
| Electronic Reminders | 30 (59%, 45%–72%) | 57 ± 16 | 50 ± 16 | 0.13 |
| Provider Education | 27 (53%, 39%–67%) | 59 ± 13 | 47 ± 18 | 0.008 |
| Provider Request for Management Plan | 26 (52%, 37%–65%) | 58 ± 17 | 50 ± 14 | 0.07 |
| Patient Calls | 7 (14%, 4%–23%) | 57 ± 14 | 53 ± 17 | 0.33 |
| Academic Detailing | 6 (12%, 3%–21%) | 73 ± 9 | 52 ± 15 | 0.003 |
| Draft Orders for WBC | 5 (10%, 2%–18%) | 66 ± 11 | 53 ± 16 | 0.09 |
| Patient Mailing | 2 (4%, 0%–9%) | 44 ± 9 | 53 ± 17 | 0.47 |
| Sites Previously Participating (N = 14) | N (%) * |
|---|---|
| Not enough patients to make it worthwhile | 9/14 (64%) |
| Providers adequately educated | 5/14 (36%) |
| Not a high priority safety issue | 1/14 (7%) |
| Any reason provided | 12/14 (86%) |
| Sites that Never Participated (N = 27) | |
| Too time consuming | 8/27 (30%) |
| Not enough patients to make it worthwhile | 6/27 (22%) |
| Not real time data | 4/27 (15%) |
| Need help from other services to implement | 2/27 (7%) |
| Not a high priority safety issue | 2/27 (7%) |
| Not appropriate work for a pharmacist | 1/27 (4%) |
| Information Technology (IT) limitation | 1/27 (4%) |
| Any reason provided | 19/27 (70%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heidenreich, P.A.; Lin, S.; Gholami, P.; Moore, V.R.; Burk, M.L.; Glassman, P.A.; Cunningham, F.E.; Sahay, A. Interventions to Increase Leukocyte Testing during Treatment with Dimethyl Fumarate. Int. J. Environ. Res. Public Health 2021, 18, 10312. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910312
Heidenreich PA, Lin S, Gholami P, Moore VR, Burk ML, Glassman PA, Cunningham FE, Sahay A. Interventions to Increase Leukocyte Testing during Treatment with Dimethyl Fumarate. International Journal of Environmental Research and Public Health. 2021; 18(19):10312. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910312
Chicago/Turabian StyleHeidenreich, Paul A., Shoutzu Lin, Parisa Gholami, Von R. Moore, Muriel L. Burk, Peter A. Glassman, Francesca E. Cunningham, and Anju Sahay. 2021. "Interventions to Increase Leukocyte Testing during Treatment with Dimethyl Fumarate" International Journal of Environmental Research and Public Health 18, no. 19: 10312. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910312