
Associations of Emotional Behavior with Nutritional Status and Lifestyle Habits among Schoolchildren Aged 5–10 Years in Sri Lanka


Abstract
:1. Introduction
2. Material and Methods
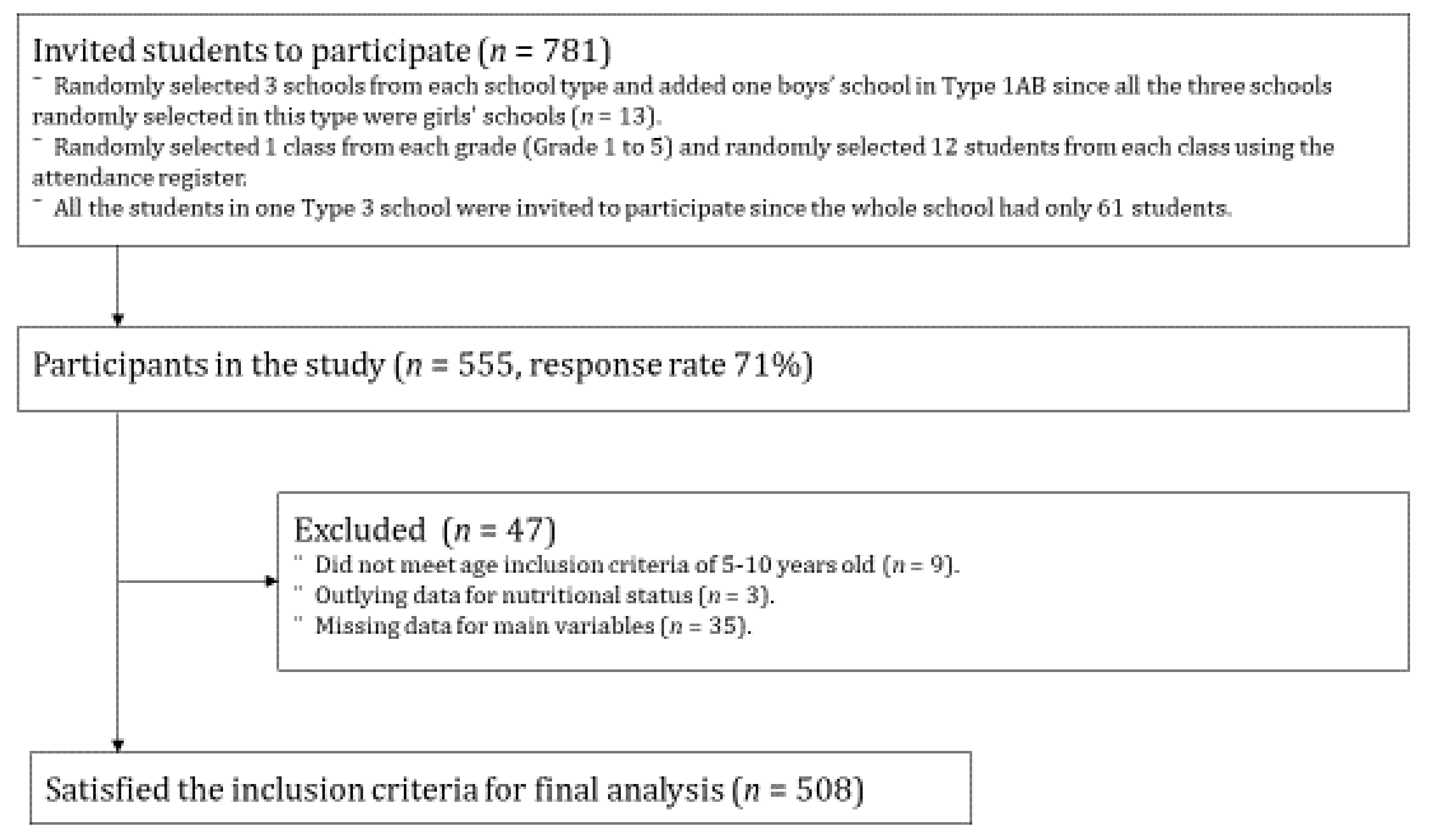
2.1. Study Participants
2.2. Dependent Variables
Psychopathology Data
2.3. Independent Variables
2.3.1. Anthropometric Measurements
2.3.2. Lifestyle Habits
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kieling, C.; Baker-Henningham, H.; Belfer, M.; Conti, G.; Ertem, I.; Omigbodun, O.; Rohde, L.A.; Srinath, S.; Ulkuer, N.; Rahman, A. Child and adolescent mental health worldwide: Evidence for action. Lancet 2011, 378, 1515–1525. [Google Scholar] [CrossRef]
- World Health Organization. Mental Health: Strengthening Our Response. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response (accessed on 9 September 2021).
- Prior, M.; Virasinghe, S.; Smart, D. Behavioural problems in Sri Lankan schoolchildren: Associations with socio-economic status, age, gender, academic progress, ethnicity and religion. Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 654–662. [Google Scholar] [CrossRef]
- Kola, L.; Kohrt, B.A.; Hanlon, C.; Naslund, J.A.; Sikander, S.; Balaji, M.; Benjet, C.; Cheung, E.Y.L.; Eaton, J.; Gonsalves, P.; et al. COVID-19 mental health impact and responses in low-income and middle-income countries: Reimagining global mental health. Lancet Psychiatry 2021, 8, 535–550. [Google Scholar] [CrossRef]
- Ford, T.; John, A.; Gunnell, D. Mental health of children and young people during pandemic. BMJ 2021, 372, n614. [Google Scholar] [CrossRef]
- Lee, G.; Han, K.; Kim, H. Risk of mental health problems in adolescents skipping meals: The Korean National Health and Nutrition Examination Survey 2010 to 2012. Nurs. Outlook 2017, 65, 411–419. [Google Scholar] [CrossRef]
- Wiles, N.J.; Jones, G.T.; Haase, A.M.; Lawlor, D.A.; Macfarlane, G.J.; Lewis, G. Physical activity and emotional problems amongst adolescents: A longitudinal study. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; Gray, C.E.; Poitras, V.J.; Carson, V.; Gruber, R.; Olds, T.; Weiss, S.K.; Connor Gorber, S.; Kho, M.E.; Sampson, M.; et al. Systematic review of the relationships between sleep duration and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S266–S282. [Google Scholar] [CrossRef] [PubMed]
- The World Bank. School Enrollment, Primary (% Net)—Sri Lanka. Available online: https://data.worldbank.org/indicator/SE.PRM.NENR?locations=LK (accessed on 7 December 2020).
- Ministry of Health. Food Based Dietary Guidelines for Sri Lankans. Available online: http://www.fao.org/3/a-as886e.pdf (accessed on 29 November 2019).
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Achenbach, T.M. Manual for the Child Behavior Checklist/4-18 and 1991 Profile; University of Vermont, Department of Psychiatry: Burlington, VT, USA, 1991. [Google Scholar]
- Goodman, R.; Scott, S. Comparing the Strengths and Difficulties Questionnaire and the Child Behavior Checklist: Is small beautiful? J. Abnorm. Child Psychol. 1999, 27, 17–24. [Google Scholar] [CrossRef]
- Wake, M.; Clifford, S.A.; Patton, G.C.; Waters, E.; Williams, J.; Canterford, L.; Carlin, J.B. Morbidity patterns among the underweight, overweight and obese between 2 and 18 years: Population-based cross-sectional analyses. Int. J. Obesity 2013, 37, 86–93. [Google Scholar] [CrossRef] [Green Version]
- Drukker, M.; Wojciechowski, F.; Feron, F.J.; Mengelers, R.; Van Os, J. A community study of psychosocial functioning and weight in young children and adolescents. Int. J. Pediatr. Obes. 2009, 4, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, A.; Foster, C.; Richards, J.; Surenthirakumaran, R. Psychosocial wellbeing and physical health among Tamil schoolchildren in northern Sri Lanka. Confl. Health 2016, 10, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health; Nutrition and Indigenous Medicine. Annual Health Bulletin 2015. Available online: http://www.health.gov.lk/moh_final/english/public/elfinder/files/publications/AHB/2017/AHB%202015.pdf (accessed on 15 May 2019).
- Shinsugi, C.; Gunasekara, D.; Gunawardena, N.K.; Subasinghe, W.; Miyoshi, M.; Kaneko, S.; Takimoto, H. Double burden of maternal and child malnutrition and socioeconomic status in urban Sri Lanka. PLoS ONE 2019, 14, e0224222. [Google Scholar] [CrossRef]
- Youthinmind. Strengths and Difficulties Questionnaire (SDQ) in Sinhalese. Available online: https://www.sdqinfo.org/py/sdqinfo/b3.py?language=Sinhalese (accessed on 18 November 2020).
- Perera, S.; Thalagala, E.; Chandrarathna, S.H.; Agampodi, T.C.; Nugegoda, D.B.; Agampodi, S.B. Factor structure and normative data of the Sinhalese version of self reported Strength and Difficulties Questionnaire (SDQ) for adolescents. Ceylon Med. J. 2013, 58, 66–71. [Google Scholar] [CrossRef] [Green Version]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Global School Health Survey, World Health Organization. Global Physical Activity Surveillance. Available online: https://www.who.int/ncds/surveillance/steps/GPAQ/en/ (accessed on 7 December 2020).
- World Health Organization. Global School-Based Student Health Survey (GSHS). Available online: https://www.who.int/ncds/surveillance/gshs/en/ (accessed on 7 December 2020).
- Moriwaki, A.; Kamio, Y. Normative data and psychometric properties of the strengths and difficulties questionnaire among Japanese school-aged children. Child Adolesc. Psychiatry Ment. Health 2014, 8, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahadi, Z.; Kelishadi, R.; Qorbani, M.; Zahedi, H.; Aram, M.; Motlagh, M.E.; Ardalan, G.; Shafiee, G.; Arzaghi, S.M.; Asayesh, H.; et al. Association of Breakfast Intake with Psychiatric Distress and Violent Behaviors in Iranian Children and Adolescents: The CASPIAN-IV Study. Indian J. Pediatr. 2016, 83, 922–929. [Google Scholar] [CrossRef]
- Eckert, K.F.; Asbridge, M.; Campbell, L.A.; Stewart, S.; Bennett, M.; Loewen, O.K.; Veugelers, P.J.; Cahill, L.E. Meal regularity is associated with self-esteem among grade 5 children. Am. J. Clin. Nutr. 2021, 113, 467–475. [Google Scholar] [CrossRef]
- Sampasa-Kanyinga, H.; Chaput, J.P.; Hamilton, H.A. Associations between the use of social networking sites and unhealthy eating behaviours and excess body weight in adolescents. Br. J. Nutr. 2015, 114, 1941–1947. [Google Scholar] [CrossRef] [Green Version]
- Kurotani, K.; Shinsugi, C. Promotion of Shokuiku (Food and Nutrition Education)—Lessons Learned from Japanese Context. Available online: https://www.nibiohn.go.jp/eiken/programs/shokuiku_report.pdf (accessed on 7 December 2020).
- Wu, X.; Tao, S.; Rutayisire, E.; Chen, Y.; Huang, K.; Tao, F. The relationship between screen time, nighttime sleep duration, and behavioural problems in preschool children in China. Eur. Child Adolesc. Psychiatry 2017, 26, 541–548. [Google Scholar] [CrossRef]
- Biggs, S.N.; Lushington, K.; van den Heuvel, C.J.; Martin, A.J.; Kennedy, J.D. Inconsistent sleep schedules and daytime behavioral difficulties in school-aged children. Sleep Med. 2011, 12, 780–786. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Total | Variable | Total | ||
|---|---|---|---|---|---|
| N or Mean | % or SD | N or Mean | % or SD | ||
| Sex | Emotional behavior (SDQ, mean, SD) | ||||
| Boy | 195 | 38.4 | Total difficulties score (TDS, 0–40) | 12.01 | 5.26 |
| Girl | 313 | 61.6 | Conduct problems (0–10) | 2.53 | 1.81 |
| Age (years) | Hyperactivity–inattention (0–10) | 4.00 | 2.16 | ||
| 5 | 39 | 7.7 | Emotional symptoms (0–10) | 2.24 | 1.90 |
| 6 | 112 | 22.1 | Peer problems (0–10) | 3.23 | 1.47 |
| 7 | 94 | 18.5 | Prosocial behavior (0–10) | 7.39 | 1.94 |
| 8 | 106 | 20.9 | Abnormal (SDQ, N, %) | ||
| 9 | 99 | 19.5 | TDS (19–40) | 57 | 11.2 |
| 10 | 58 | 11.4 | Conduct problems (5–10) | 67 | 13.2 |
| Number of siblings | Hyperactivity–inattention (7–10) | 68 | 13.4 | ||
| 0 | 96 | 18.9 | Emotional symptoms (7–10) | 20 | 3.9 |
| 1 | 242 | 47.6 | Peer problems (5–10) | 89 | 17.5 |
| 2 | 141 | 27.8 | Prosocial behavior (0–5) | 93 | 18.3 |
| 3 | 28 | 5.5 | Nutritional Status | ||
| 4 | 1 | 0.2 | BAZ, (mean, SD) | −0.80 | 1.48 |
| School type | BAZ (%) | ||||
| 1AB | 157 | 30.9 | Thin (<–2) | 99 | 19.5 |
| 1C | 85 | 16.7 | Normal weight (–2 to +1) | 342 | 67.3 |
| 2 | 128 | 25.2 | Overweight or obese (>+1) | 67 | 13.2 |
| 3 | 138 | 27.2 | Lifestyle habits | ||
| Breakfast intake | |||||
| No | 55 | 10.8 | |||
| Yes | 453 | 89.2 | |||
| MVPA (per day) | |||||
| <60 min | 298 | 58.7 | |||
| ≥60 min | 210 | 41.3 | |||
| Wake–up time | |||||
| <6:00 am | 187 | 36.8 | |||
| 6:00 am–6:29 am | 278 | 54.7 | |||
| 6:30 am–8:29 am | 43 | 8.5 | |||
| Bedtime | |||||
| 7:00 pm–8:59 pm | 239 | 47.1 | |||
| 9:00 pm–9:59 pm | 211 | 41.5 | |||
| 10:00 pm–11:59 pm | 58 | 11.4 | |||
| Variables | High TDS (19–40) | Conduct Problems (5–10) | Hyperactivity-Inattention (7–10) | ||||||
| aOR | 95% CI | p | aOR | 95% CI | p | aOR | 95% CI | p | |
| Nutritional status | |||||||||
| Thin (BAZ < −2) | 1.26 | (0.64–2.49) | 1.26 | (0.65–2.44) | 0.90 | (0.46–1.74) | |||
| Normal weight (−2 to +1) | 1.00 | 1.00 | 1.00 | ||||||
| Overweight or obese (BAZ > +1) | 0.60 | (0.22–1.65) | 1.25 | (0.56–2.82) | 0.48 | (0.18–1.28) | |||
| Lifestyle habits | |||||||||
| Breakfast intake—no (1), yes (0) | 1.54 | (0.69–3.42) | 2.95 | (1.50–5.77) | ** | 1.76 | (0.84–3.70) | ||
| MVPA (per day)—<60 (1), ≥60 (0) | 1.02 | (0.57–1.83) | 0.85 | (0.49–1.48) | 0.79 | (0.46–1.36) | |||
| Wake-up time | |||||||||
| <6:00 am | 1.00 | 1.00 | 1.00 | ||||||
| 6:00 am–6:29 am | 0.91 | (0.50–1.68) | 1.00 | (0.55–1.79) | 0.95 | (0.53–1.69) | |||
| 6:30 am–8:29 am | 0.77 | (0.24–2.47) | 1.50 | (0.57–3.97) | 1.10 | (0.42–2.87) | |||
| Bedtime | |||||||||
| 7:00 pm–8:59 pm | 1.00 | 1.00 | 1.00 | ||||||
| 9:00 pm–9:59 pm | 0.84 | (0.45–1.56) | 0.88 | (0.50–1.57) | 0.81 | (0.45–1.44) | |||
| 10:00 pm–11:59 pm | 1.51 | (0.64–3.54) | 1.20 | (0.50–2.88) | 1.38 | (0.62–3.11) | |||
| Variables | Emotional Symptoms (7–10) | Peer Problems (5–10) | Prosocial Behavior Problems (0–5) | ||||||
| aOR | 95% CI | p | aOR | 95% CI | p | aOR | 95% CI | p | |
| Nutritional status | |||||||||
| Thin (BAZ < −2) | 2.04 | (0.70–5.94) | 0.78 | (0.42–1.43) | 1.06 | (0.59–1.92) | |||
| Normal weight (−2 to +1) | 1.00 | 1.00 | 1.00 | ||||||
| Overweight or obese (BAZ > +1) | 1.50 | (0.37–6.00) | 0.69 | (0.32–1.49) | 0.63 | (0.28–1.41) | |||
| Lifestyle habits | |||||||||
| Breakfast intake—no (1), yes (0) | 0.38 | (0.05–3.00) | 1.69 | (0.86–3.32) | 1.64 | (0.82–3.29) | |||
| MVPA (per day)—<60 (1), ≥60 (0) | 0.81 | (0.31–2.12) | 1.01 | (0.62–1.65) | 1.20 | (0.73–1.97) | |||
| Wake-up time | |||||||||
| <6:00 am | 1.00 | 1.00 | 1.00 | ||||||
| 6:00 am–6:29 am | 0.91 | (0.33–2.50) | 1.46 | (0.88–2.44) | 1.38 | (0.80–2.37) | |||
| 6:30 am–8:29 am | 1.53 | (0.28–8.29) | 0.58 | (0.19–1.79) | 1.75 | (0.75–4.07) | |||
| Bedtime | |||||||||
| 7:00 pm–8:59 pm | 1.00 | 1.00 | 1.00 | ||||||
| 9:00 pm–9:59 pm | 2.07 | (0.72–5.96) | 0.80 | (0.48–1.32) | 1.21 | (0.72–2.04) | |||
| 10:00 pm–11:59 pm | 2.91 | (0.75–11.30) | 1.12 | (0.53–2.38) | 2.43 | (1.17–5.03) | * | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shinsugi, C.; Gunasekara, D.; Takimoto, H. Associations of Emotional Behavior with Nutritional Status and Lifestyle Habits among Schoolchildren Aged 5–10 Years in Sri Lanka. Int. J. Environ. Res. Public Health 2021, 18, 10332. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910332
Shinsugi C, Gunasekara D, Takimoto H. Associations of Emotional Behavior with Nutritional Status and Lifestyle Habits among Schoolchildren Aged 5–10 Years in Sri Lanka. International Journal of Environmental Research and Public Health. 2021; 18(19):10332. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910332
Chicago/Turabian StyleShinsugi, Chisa, Deepa Gunasekara, and Hidemi Takimoto. 2021. "Associations of Emotional Behavior with Nutritional Status and Lifestyle Habits among Schoolchildren Aged 5–10 Years in Sri Lanka" International Journal of Environmental Research and Public Health 18, no. 19: 10332. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910332