1. Introduction
Tuberculosis (TB) is a major global health problem, infecting millions of people annually. TB ranks alongside the human immunodeficiency virus (HIV) as a leading cause of death worldwide, particularly in low- and middle-income countries [
1]. Despite the availability of efficacious treatment for TB, high morbidity, and mortality are observed. In 2017, TB caused about 1.6 million deaths globally. In 2019, there were an estimated 10 million new TB cases worldwide, of which 5.6 million were men, 3.2 million were women, and 1.2 million were children. People living with HIV accounted for 10% of the total. It is estimated that about one-third of the world’s population is infected with the tuberculosis bacillus [
2]. In 2015, the highest number of new TB cases occurred in Asia (61%), followed by Africa with 26% of new cases and usually infects adults in their productive years [
3]. TB has for many years been the leading cause of deaths from a single pathogen, however, it is now the second leading cause of deaths worldwide due to the rise of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [
4].
In 2017, about 72% TB patients were in Africa and two thirds were from the following eight countries: India (27%), China (9%), Indonesia (8%), the Philippines (6%), Pakistan (5%), Nigeria (4%), Bangladesh (4%), and South Africa (3%) [
3]. These eight countries and 22 other countries in the WHO’s list of 30 high TB burden countries accounted for 87% of the world’s cases. Significantly, Europe and the Americas reported only 3% each of the TB global cases. This shows that the severity of national epidemics varies widely among countries. In 2017, there were fewer than 10 new cases per 100,000 population in most high-income countries, 150–400 in most of the 30 high TB burden countries, and above 500 in countries such as Mozambique, the Philippines, and South Africa [
3].
TB continues to be the second leading cause of death after SARS-CoV-2 in South Africa. In 2019, 58,000 people died of TB and of these, about 36,000 were HIV positive [
2]. The burden of TB in South Africa is fueled mostly by the high HIV pandemic. Limpopo is one of the provinces most affected by TB with approximately 55% of TB patients in the province co-infected with HIV. Only 76% of adults know their status compared to 70% of children under 15 years living with HIV [
5]. In some regions of Africa, about 75% of TB patients are co-infected with HIV [
6]. People living with HIV are at a higher risk of developing TB than those who are not HIV-infected. According to Health System Trust, in 2016, the Limpopo Province had the highest number of patients at 96.7% initiated on TB treatment. The province had a treatment cure rate of 76.1% compared to the national target of 85% [
7], and had a TB treatment defaulter rate of 6.1% compared to the national target of 5.4%. While the TB treatment success rate was 80.6%, this was below the national target of 85% and the TB death rate was 11.5% compared to the national average of 5% [
7].
Lack of knowledge about the TB disease causes an underutilization of the health services, delay in seeking diagnosis, and poor treatment adherence amongst TB patients. Improving the roll out of TB public awareness and health promotion is important in increasing knowledge about TB. This, in turn, shapes the community and TB patients’ health-seeking behavior [
8]. Different studies have reported that non-adherence to treatment often results from inadequate knowledge or understanding of the disease and its treatment [
9]. Although people have a general idea of what TB is, there are gaps in knowledge on transmission, treatment, and prevention. This leads to diagnostic and treatment delays for people living with TB [
10]. Another study indicated that patients with low TB knowledge are less likely to seek health care and get diagnosed. Instead, they often turn to self-medication and traditional healers, which lead to delays in diagnosis and appropriate treatment [
8]. In Africa, it has also been reported that community members often have incorrect knowledge about the cause and transmission of TB [
11].
Poor understanding of TB and TB treatment leads to non-adherence to TB treatment [
12]. Non-adherence to the treatment results in uncured TB, spreading of TB in communities, and an increase in TB drug resistance. Patients with drug resistant TB often develop TB that is resistant to at least one first-line anti-TB drug. If the patient continues to be non-adherent to treatment, the patient may develop multidrug-resistant TB (MDR-TB). Drug-resistant TB requires close management and consultation with experts in the disease [
13]. According to the WHO, non-adherence to TB treatment among patients is widespread and results in high mortality rates, the occurrence of drug-resistant TB, and increased treatment cost. The implementation of DOTS by WHO globally was an attempt at reach 100% adherence to treatment by TB patients, which in turn was expected to increase cure rates [
14].
2. Methods
2.1. Study Design
The study used a quantitative descriptive design to assess the knowledge, beliefs, and perceptions of TB and TB treatment amongst TB patients in Limpopo Province. Quantitative research methods were chosen, and numerical data were collected from a small group of people. The results were then generalized to a larger group to explain the study phenomenon. Quantitative research helped in ensuring that a suitable sample size was used to gain accurate and trustworthy results.
2.2. Study Site
The study was conducted in the Limpopo Province in the three selected districts of Waterberg, Capricorn, and Vhembe. According to the Health System Trust [
7], the province has a population of 5,630,467 divided into 2,649,115 of males and 2,981,352 females. Approximately 80% of the population in Limpopo live in rural areas. The province experiences high numbers of both legal and illegal immigrants. The traditional health system is strong, and communities are influenced by their cultures and beliefs. This has a strong influence on TB treatment non-adherence and hence the reason for conducting this research in the province.
2.3. Study Population
The study population was defined as all TB patients older than 18 years who had completed at least one month of TB treatment and were registered in the selected Community Health Centers (CHCs) in the Limpopo Province during the time of data collection. TB patients who were below the age of 18 were not included in the study.
Inclusion and Exclusion Criteria
All TB patients who were above the age of 18 and had completed at least one month of TB treatment and registered in the selected CHC TB register were included in the study. Respondents who had already completed their TB treatment from the date of data collection were excluded in the study.
2.4. Sampling Procedure
The researcher used systematic random sampling to select samples at a preset interval. The sampling of the respondents was determined through Slovin’s formula and depended on the total number of TB patients registered on the TB register of CHCs. N was the total number of TB patients who were registered in the TB register of the selected CHCs during the time of the study and n was the sample size. The propositional sampling sizes were calculated based on the total population of CHCs. A sample size of 292 was determined. The total number of the TB registered patients (N = 1075) were then divided by the sample size (n = 292) to find the following interval Kth value: Kth value = 1075/292 = 3.68, which was 4. Systematic random sampling technique was then employed to sample TB patients from the CHCs’ TB registers, in order to sample every fourth TB patient for participation in the study. The researcher then randomly chose the starting number to be patient number one (1) who met the criteria as it appeared in the TB register until the total of 292 was reached. The researcher then added about 10% (28) to cover for non-response and the sample became 320 and was proportionally distributed. Subsequently, only 207 respondents participated in the study since others were not available due to COVID-19 lockdown. Most participants responded to the questionnaire from their homes.
2.5. Sample Size Determination
Slovin’s formula, where N is the total number of TB patients registered in the TB register of the selected CHCs during the time of the study,
n is the sample size, and e is the accepted level of error, was used to calculate the sample size. The accepted level of error, e, was 0.05. The estimated overall sample size was 292 of all TB patients drawn from an estimated total population of 1075, with a 95% confident interval.
2.6. Data Collection Instrument
Data were collected using a self-administered questionnaire (
Supplementary Material File) with open and closed-ended questions. The English language written questionnaire was developed by the researcher and reviewed and approved by the study promoters. The questionnaire was divided into four sections. Section A was socio-demographic characteristics that included age, employment status, sex, income, type of income, and level of education; Section B required knowledge about TB and TB treatment; Section C required participants’ information about the cultural, religious, and traditional beliefs regarding TB and TB treatment; and Section D sought to collect information relating to the participants’ perception of TB and its treatment. Section A had eight main questions, Section B had 14 main questions, Section C had eight main questions, and Section D had four main questions. The construct of the questions was open and closed-ended questions, which had two to six answers to choose from. The researcher ensured that all relevant topics were covered. The research participants freely responded to open and closed-ended questions and all unclear questions were explained in more detail to the respondents whenever they required clarity.
2.7. Data Collection Procedure
Data collection started after ethical clearance and permission to enter the CHCs were obtained. Data collection took place from June 2020–September 2020. Health care facility managers were engaged, and the details of the study were explained to them. Arrangements to call the selected respondents who met the criteria to come to the facility were made with the facility managers. Appointments were then made with the respondents and the researcher visited the facility on the day of the appointment. Those who could not make it to the facilities were visited at their homes. Respondents were asked to sign consent forms prior to participation. The researcher explained the purpose of the study to each participant before completing the questionnaire. Participants were assured that confidentiality would be maintained. All respondents who agreed to sign a written consent forms were included in the study. About 207 respondents who signed consent forms were given questionnaires to complete. About 3.9% of those who could not read were assisted by the main researcher and health professionals working at the CHCs. About 33% of the participants with primary education were also assisted to clarify any questions that were not clear to them. Questionnaires were collected the same day after the participants completed them. About 207 questionnaires were received from the respondents who were available during the time of data collection. With the help of the clinicians, the response rate was 71% as other patients were not available during the time of the study due to COVID-19 restrictions. Some patients had already been transferred from the facilities and were not from the surrounding villages. Only respondents from the surrounding areas were followed home and invited to participate in the study.
2.8. Data Analysis
Quantitative data analysis was carried out using Statistical Package for Social Sciences (SPSS) version 26.0 (2017). All data from the questionnaire were coded using a code book and was entered into SPSS version 26.0 statistical programs. The researcher used codes rather than the respondents’ names and checked the data by frequency to identify missing or incorrect values. In this respect, the mean, mode, median, and standard deviation variables were used to calculate the various descriptive statistics. Results emanating from the analysis were represented in the form of tables and charts.
2.9. Validity of the Instrument
Validity relates to the degree to which the research measures what it is supposed to measure [
15]. The researcher focused on the content validity and face validity of the instrument.
2.9.1. Face Validity
Face validity of an instrument refers to the judgment that an instrument is measuring what it is supposed to, based primarily on the local link between the questions and study objectives. The questionnaire was presented at the departmental seminars and School of Health Sciences’ Higher Degrees Committee at the University of Venda. The supervisors were consulted for comment and opinion as to whether the instrument would be suitable for collecting adequate data to develop an effective intervention for improving TB medical adherence. The questionnaire was restructured based on the feedback from supervisors.
2.9.2. Content Validity
The researcher reviewed the literature and instruments from similar studies. Supervisors, TB coordinators, and experts in the field were consulted for comments and inputs before finalizing the instrument [
16]. In addition, content validity was addressed by an extensive literature search to identify the domain of the construct before developing the questionnaire.
2.10. Reliability of the Instrument
To ensure reliability of the instrument, the test re-test method was used, re-administering the same instrument to the same set of respondents. Ten percent (
n = 30 respondents) of the sample size was sampled on day one, and the same set of respondents were given the same questionnaire two days later and the two responses were compared using the Cronbach Alpha correlation technique. A correlation co-efficient was used to compare the two instruments and a score was made on both instruments. A correlation co-efficient of 0.9 was found. This was closer to one (1), indicating a strong positive relationship and showed the reliability of the instrument [
17].
2.11. Ethical Consideration
The proposal was submitted and presented to the School of Health Science and the University Higher Degrees Committee (UHDC), and an ethical clearance was granted (SHS/19/PH/28/0411). Permission to conduct the study was obtained from the Limpopo Provincial Department of Health and Vhembe District, Waterberg District, and Capricorn District Department of Health. Furthermore, permission was obtained from the facilities’ operational managers.
All participants were asked to complete consent forms. The nature of the research was described to the respondents, and they were informed of their right to refuse to participate, or to withdraw from participating if they felt that they could not continue. The respondents were also informed and assured that the information within their responses would not be used against them or shared with other people, but would only be reported as study findings.
Anonymity was also ensured as respondents did not write down their names or any personal identification. The researcher respected the choices and agreements made with the respondents. The initial agreement was not changed without the knowledge of the respondents. Individuals were not victimized for refusing to participate.
4. Discussion
The discussion is arranged under sub-headings based on the objectives of the study, namely demographic profile of the respondents, knowledge about TB and TB treatment, beliefs about TB and TB treatment, and perception of TB and TB treatment. The study data show that about 42% of the TB patients were between 18 and 29 years old, 20.8% were between 30 and 39 years old, and 22.2% were between 40 and 49 years old. Most infected people were between 18 and 49 years. This indicates that young economically productive age groups suffer more from tuberculosis. These results are similar to those from previous studies, in which a rapid rise in TB mortality and morbidity among the young adult population between 15 and 44 years of age has been reported [
18].
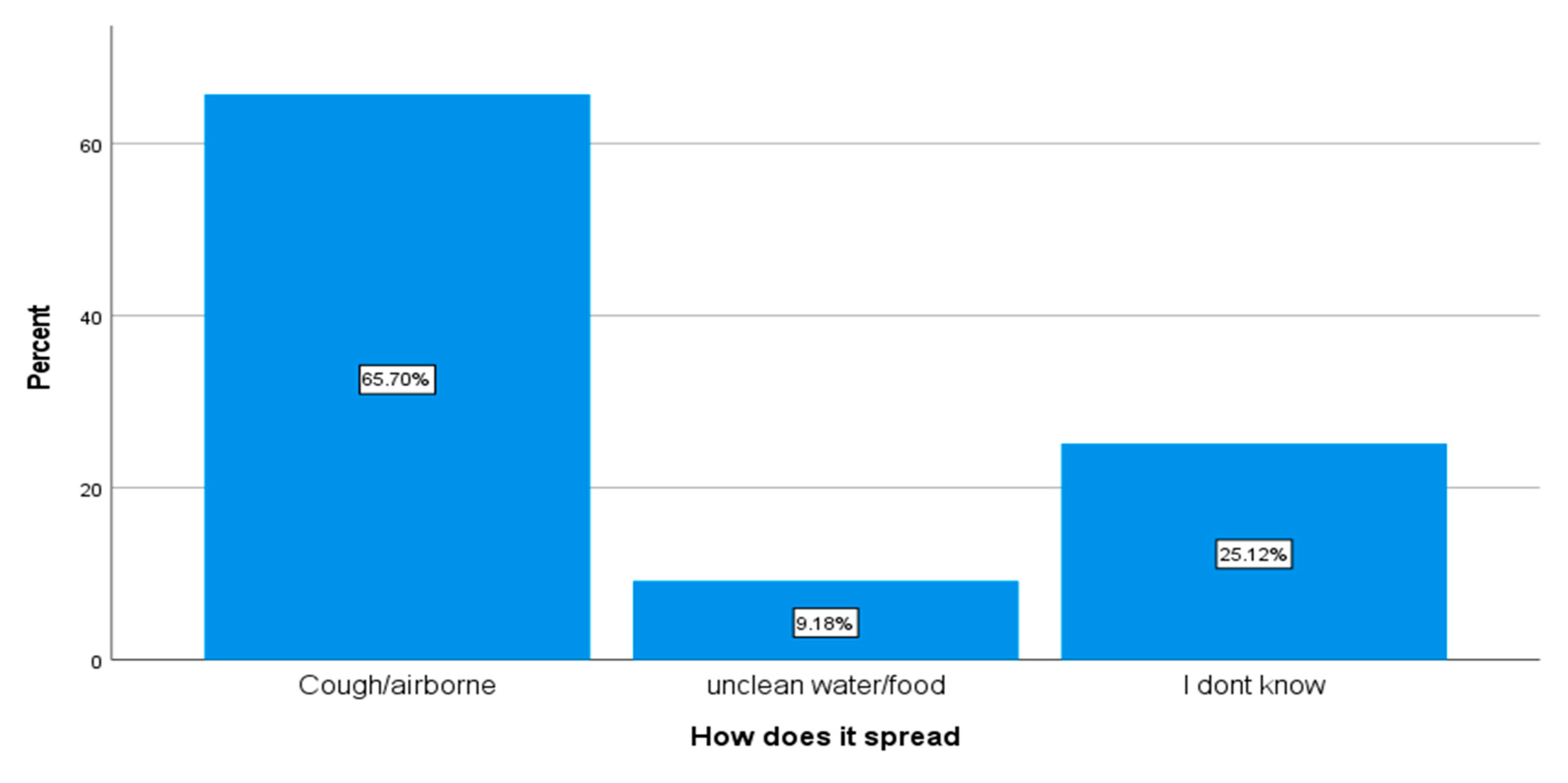
About 93% of the respondents said that they were not aware that they had TB before they consulted the health care facilities and were diagnosed with TB. About 73.9% stated that they only learned about the TB disease after they were diagnosed at the health care facility, and 26% said that they still did not know about TB. Only 65.7% had knowledge on how TB spread from person to person. The study findings revealed that there is still poor TB information in the communities since most respondents only learn about TB when they are already sick. Even after their diagnosis, some respondents still had a poor understanding of TB. Poor knowledge about TB increases misconceptions about the cause and mode of transmission in the community and delays TB diagnosis [
19]. Early diagnosis of TB and prompt initiation of treatment are essential for an effective TB control program. Patients with undiagnosed pulmonary TB predominantly act as reservoirs for transmission, and delay in the diagnosis may worsen the disease, increase the risk of death and chances of transmission of TB in the community [
20].
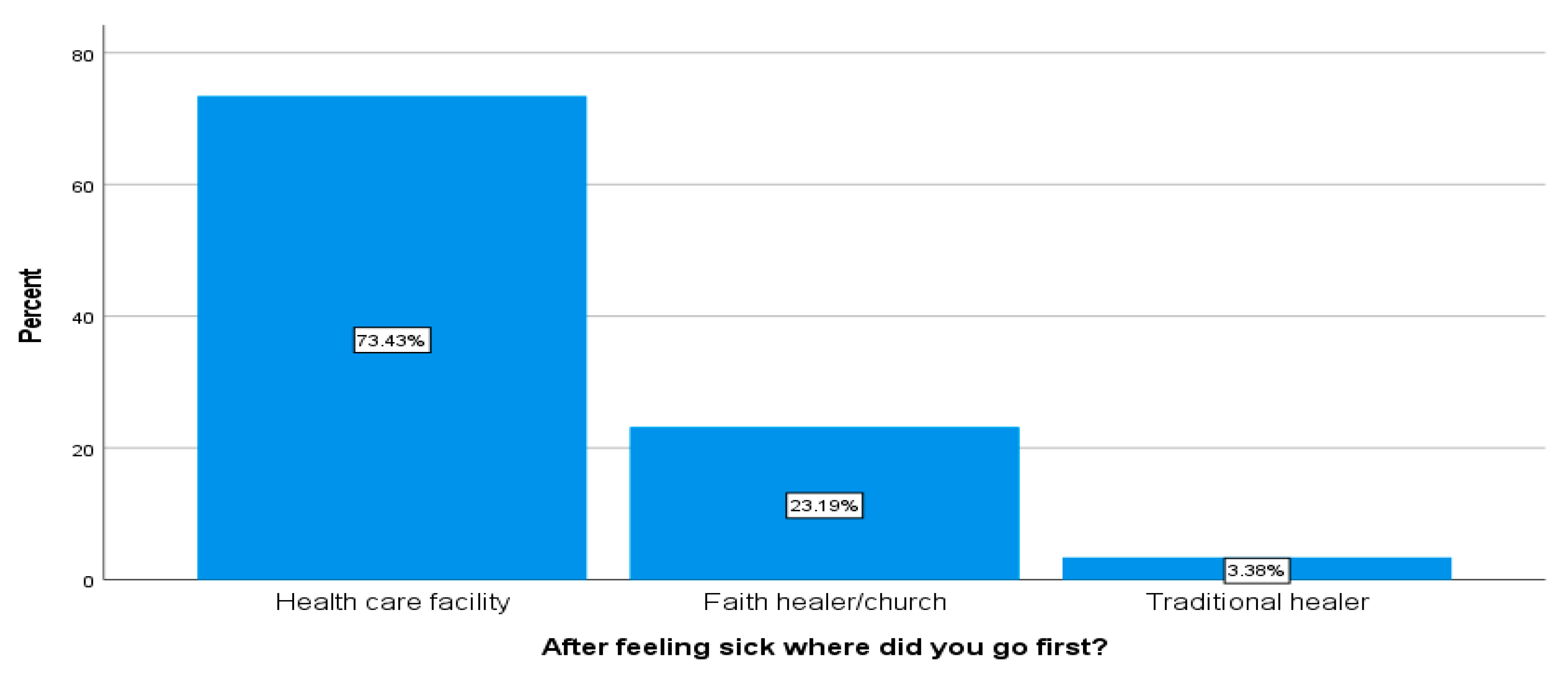
The current study indicated that about 75.3% respondents had visited faith healers for help even after being diagnosed with TB at the health care facility. Only 3.3% acknowledged that they had visited traditional healers first before going to health care facilities, while 2% acknowledged that they had visited traditional healers even after their diagnosis. Most respondents might be reticent to share intimate information about visiting traditional healers or cultural practices with an outsider who is not related to their culture, therefore, the evidence can be treated with caution [
21]. The study further revealed that even though participants acknowledged that TB is caused by a bacteria and that it can be cured if treated correctly, about 76% of respondents indicated that they still had strong beliefs in their culture and religion, and as a result, they acknowledged visiting traditional healers and faith healers for help even after their TB diagnosis as they still linked their disease to a curse or punishment and did not attribute it to a bacteria. This is evident because Limpopo Province has a TB treatment cure rate of 79.9%, which is below the set target of 95%, and a high treatment defaulter rate of 7.4%. This study further revealed that the TB information provided to the TB patients during their health education did not change their perceptions about the TB disease. These findings concur with the findings of a study that was conducted by Gyimah and Dako-Gyeke [
22], which revealed that good knowledge of TB treatment practices amongst TB patients did not spontaneously shape perceptions toward TB treatment. A study that was conducted by Viney et al. [
23] concluded that most TB patients interviewed in their study did not attribute TB to a bacterial cause.
Even though most respondents (92.3%) indicated that TB could not be treated with traditional medicine, however, some patients still acknowledged visiting traditional healers for help, which is highly influenced by their cultural orientation. When culture and traditional beliefs oppose the existence of HIV, it becomes difficult for patients who are on treatment to adhere to their treatment [
22]. Similarly, Matombo et al. found that cultural practices and beliefs concerning HIV and prevailing faith that traditional healers could treat HIV/AIDS, and the belief that HIV is caused by witchcraft and demons were the factors affecting patients on treatment as patients concurrently visit traditional healers [
24]. Another study indicated that some HIV patients stopped taking their ARVs because of cultural influences and lack of family support. Culture plays an important role in the practices of patients on long-term treatments. Patients do not often adhere to treatment because of cultural convictions. Use of herbal or natural remedies was reported before, during, and after TB treatment [
25].
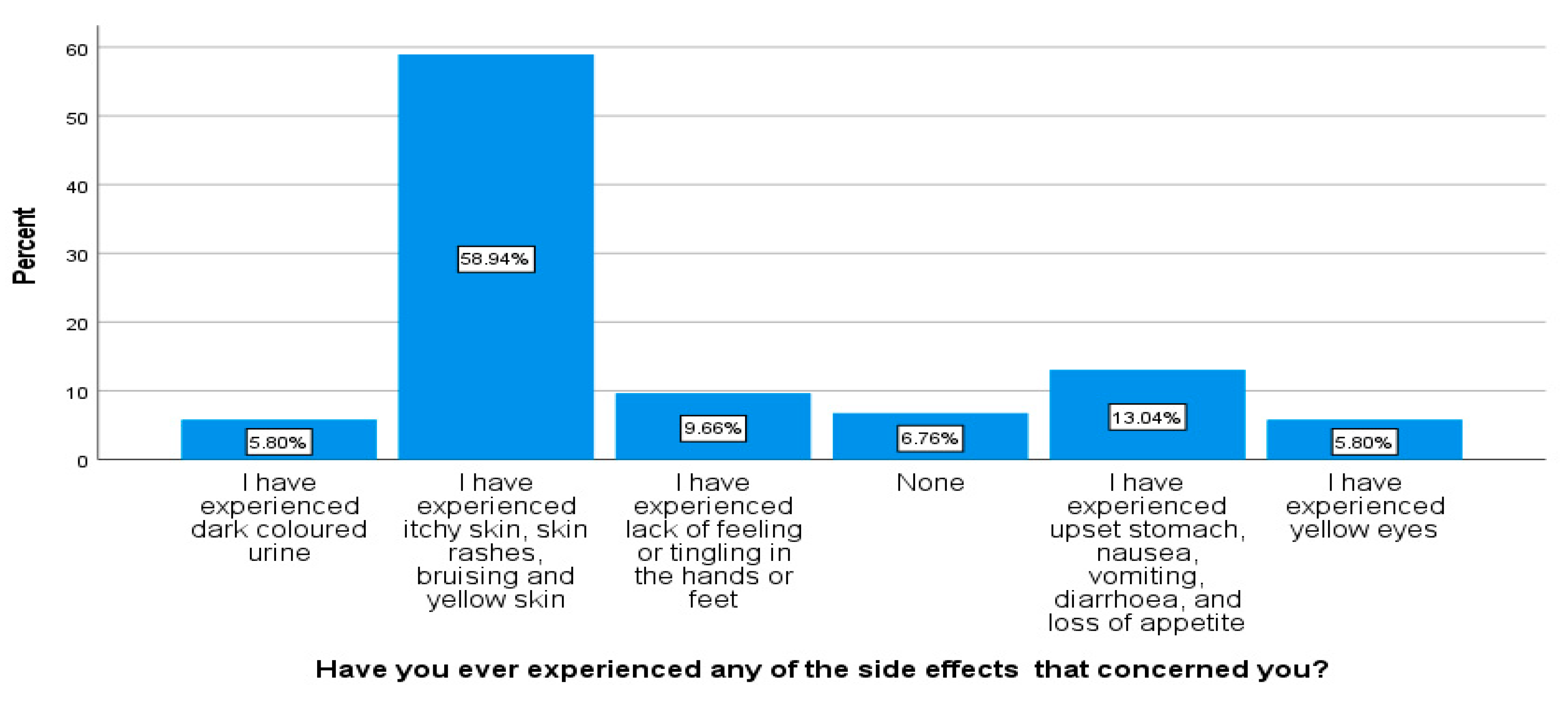
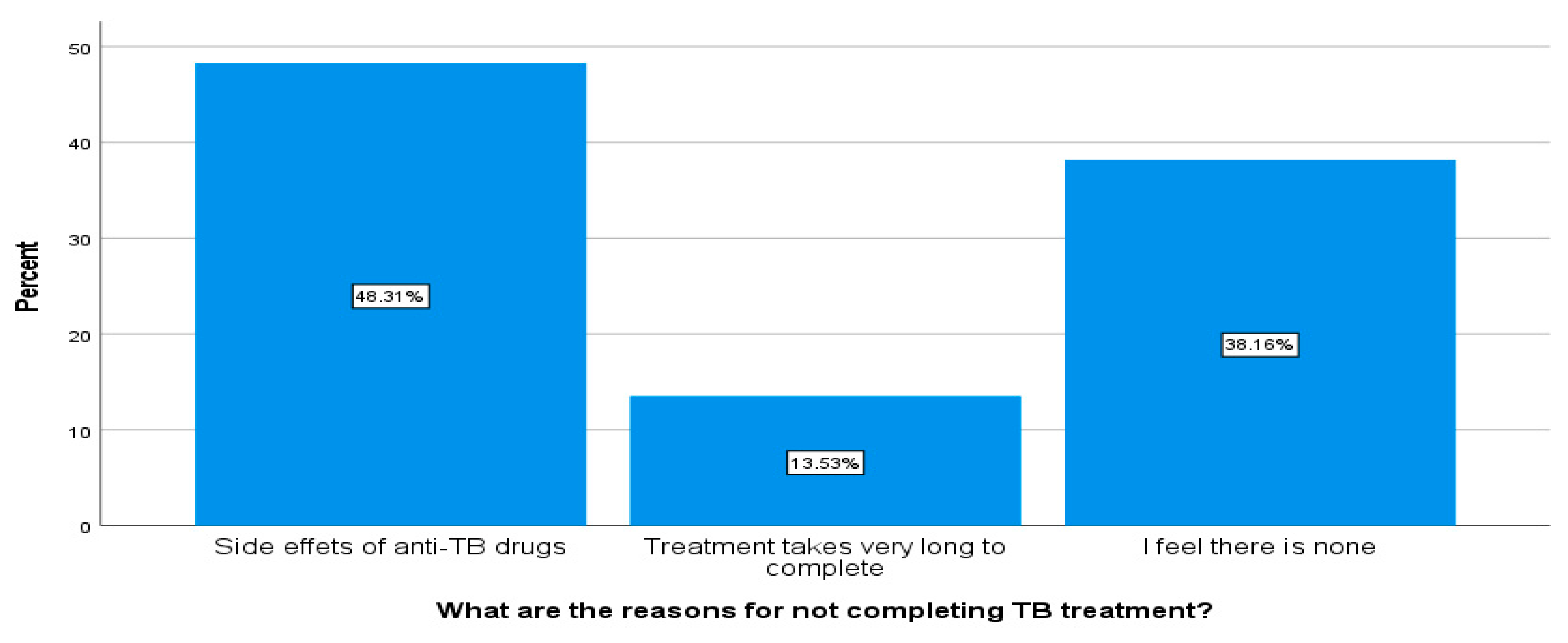
The current study shows that about 48.3% perceived that TB treatment side effects causes patients not to complete their treatment. The results of this study showed that a high proportion (59%) of the respondents indicated that they had experienced itchy skin, skin rashes, bruising, and yellow skin, however, those side effects were mostly mild as patients were still taking their treatment during the time of the study. Previous studies have shown that skin rash is very common during the application of first line anti-tuberculosis drugs [
26]. The study further revealed that respondents did not want to disclose their TB status to their family members for fear of discrimination and isolation. Due to the lack of comprehensive knowledge about TB treatment, patients were likely to stop treatment. Treatment interruption is also related to perceptions about TB as a disease [
27]. Patients also fear being discriminated and isolated within the community as there is a misconception about TB in the community. One study indicated that because of fear of stigma and discrimination, patients did not disclose their HIV status to their family members, which in turn influenced non-adherence to TB medication [
28].
6. Conclusions
The results of the study highlighted that there is a lack of knowledge, strong beliefs, and incorrect perceptions about TB and its treatment amongst TB patients in the community. Some patients were unaware about the cause of TB and the key routes of its transmission. Poor knowledge about TB in the communities is one of the main risk factors that increase misconceptions and the wrong perception about the TB disease in the community. The lack of knowledge, wrong TB perception, and beliefs about TB disease can lead to delays in TB diagnosis, which in turn can lead to increased TB transmission in the communities. The wrong perceptions about TB can also lead to increased stigma and discrimination in the community, which might encourage the social isolation of TB patients. These findings highlight the need for health education efforts to be implemented to improve community knowledge and awareness of the TB disease by health care providers as it is vital to reduce incorrect perceptions about TB, its transmission, and further promote early TB diagnosis and infection control in the community.
Recommendations
Based on the above findings and further COVID-19 concerns, the following recommendations are made:
The Department of Health should embark on an intensive community education program aimed at changing any wrong perceptions about TB.
Health care workers should intensify door to door campaigns to improve community TB knowledge.
Policy makers need to develop guidelines and policies that aim at training traditional healers and religious leaders to be DOT supporters.
Develop guidelines that encourage family members who provide support to TB patients to be trained on patient supervision.
Comprehensive COVID-19 and COVID-19 vaccine health education to be provided to TB patients during their visit as people infected with TB may have a weak immune system, may be at a higher risk of contracting COVID-19, and are at a higher risk of suffering more severe COVID-19 symptoms; the risk is even higher if TB patients are co-infected with HIV or diabetes.
Health care workers need to conduct effective TB screening and testing to differentiate between TB and COVID-19 infection.
With large number of TB patients who are not diagnosed or treated, it is important for health care workers to conduct effective point-of-care TB screening and make use of new point-of-care TB diagnostic tools to improve TB case identification.


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}