
Toward the Integration of Technology-Based Interventions in the Care Pathway for People with Dementia: A Cross-National Study

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Anne, the Embodied Conversational Agent
2.2. Subjects
- Age of 60 years or older
- Living independently
- Mini-Mental Status Examination (MMSE) [20] score between 24 and 30
- Ability to understand and sign the written informed consent
- Lack of written informed consent
- Presence of an unstable chronic condition, with a Mini-Mental Status Examination (MMSE) score <24
- Presence of severe physical illness or disabilities that could be aggravated through the use of Anne
2.3. Recruitment Procedure
2.4. Study Design
- Quality of life in older adults with cognitive impairment (Quality of Life in Alzheimer Disease scale [QOL-AD]) questionnaire [21,22]. It is composed of 13 items covering physical health, energy, mood, living situations, memory, family, marriage, friends, chores, fun, money, self, and life as a whole. The assessment is scored on a 4-point Likert scale ranging from 1 (poor) to 4 (excellent), with total scores ranging from 13 to 52.
- At the end of the period, users also responded to the questionnaires below:
- The System Usability Scale (SUS) [23] provides a quantitative measure of the usability of a system. It is composed of ten statements rated by a 5-point Likert scale scored from 0–100, with 100 indicating perfect usability. This score is usually compared and interpreted considering the acceptable average value of 68 (SD 12.5), which was determined for a variety of products and tools, including websites and technologies, provided by Sauro and Lewis [24] after the analysis of more than 5000 user scores encompassing almost 500 studies.
- The closeness scale [25] assesses the perceived relationship by asking respondents to evaluate their relationship with Anne. Respondents had to select 1 of 7 pairs of increasingly overlapping circles that best described their relationship with Anne. In each pair of circles, one circle referred to the respondent, and the other circle referred to Anne. A larger overlap indicated a closer relationship. For the analysis, visualization was numbered as follows: 1 = no overlap, 2 = little overlap, 3 = some overlap, 4 = equal overlap, 5 = strong overlap, 6 = very strong overlap, and 7 = almost total overlap.
- Some unstructured short questions were asked to users in order to record the role attribute to Anne.
2.5. Statistical Analysis
3. Results
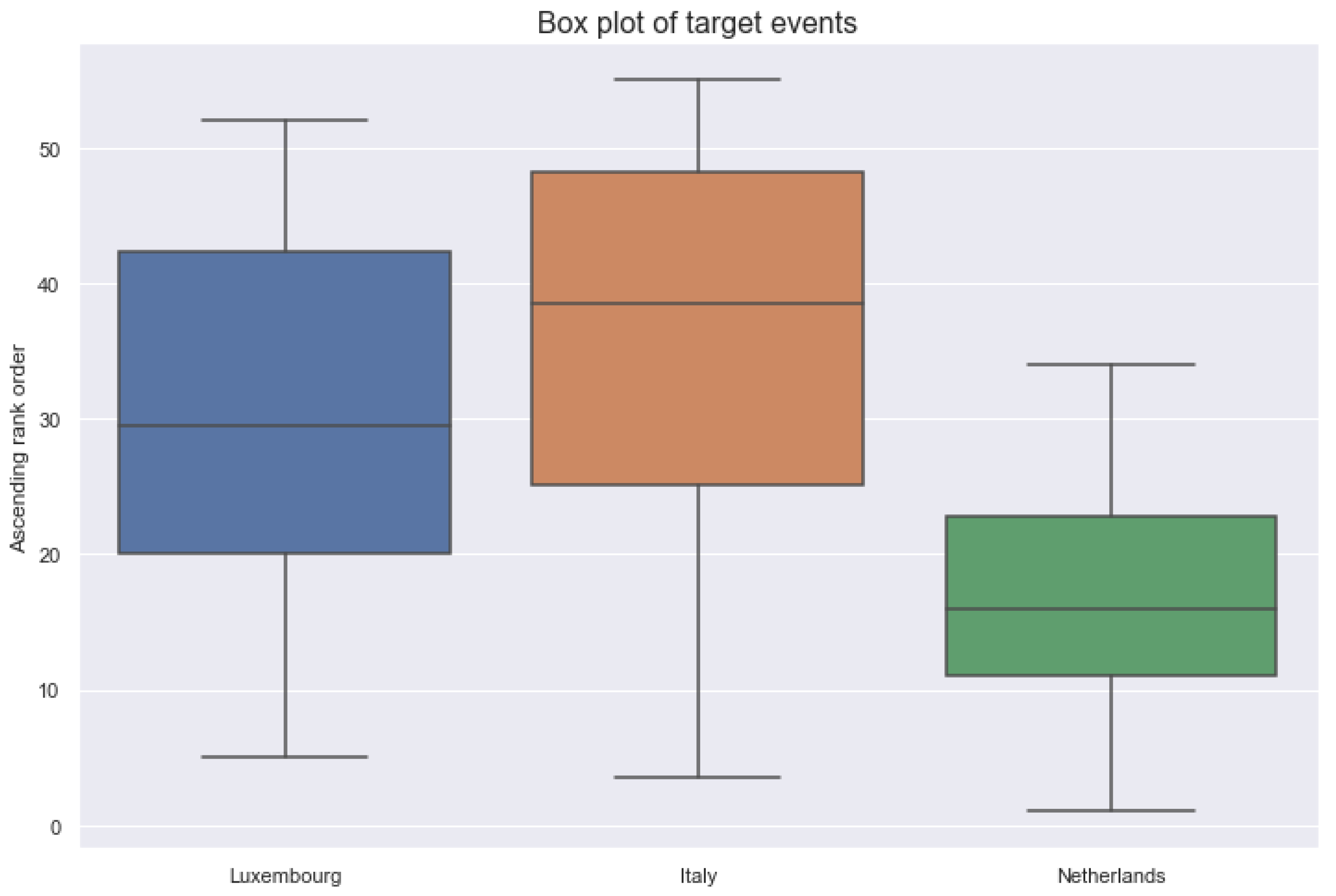
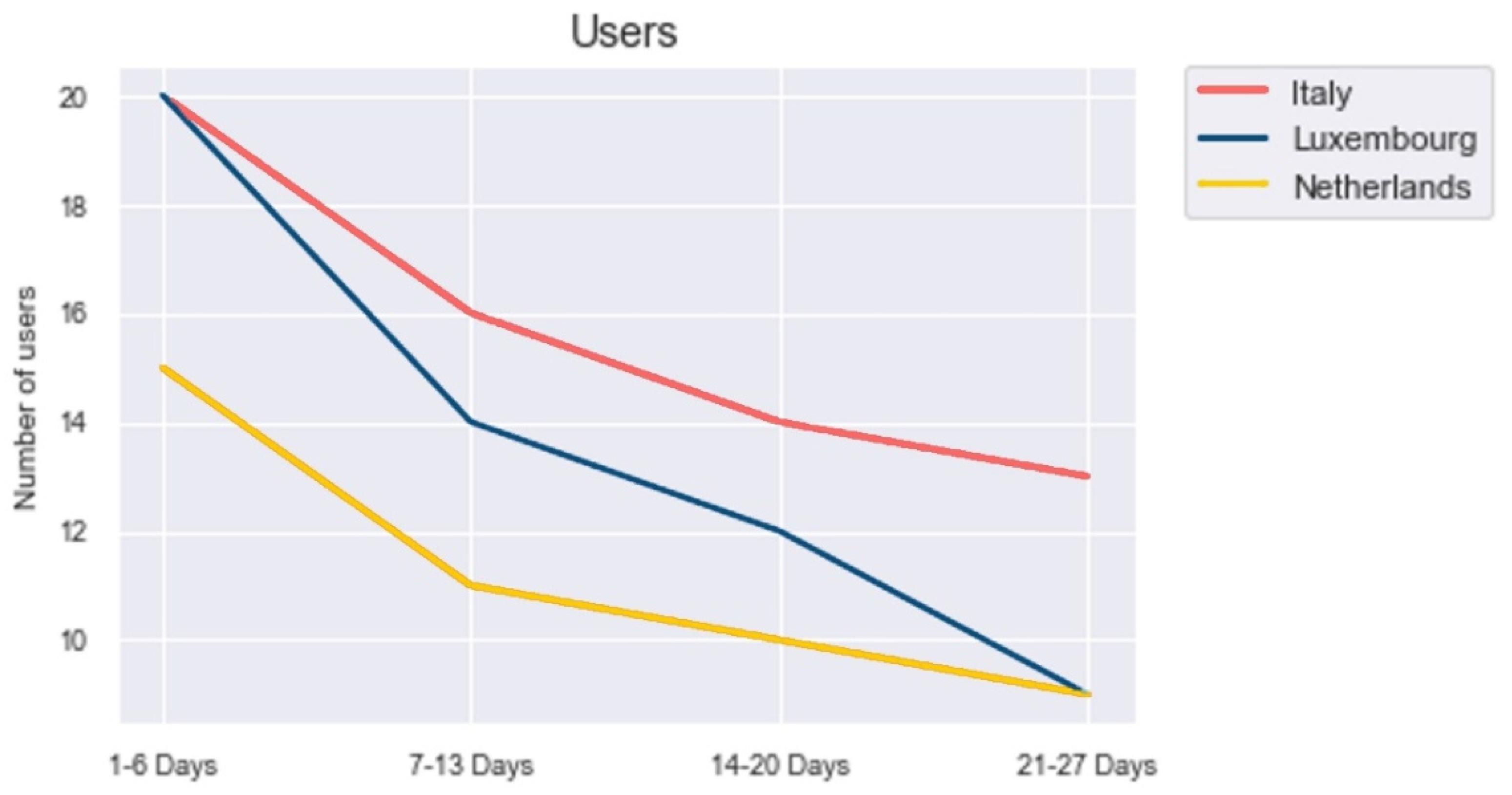
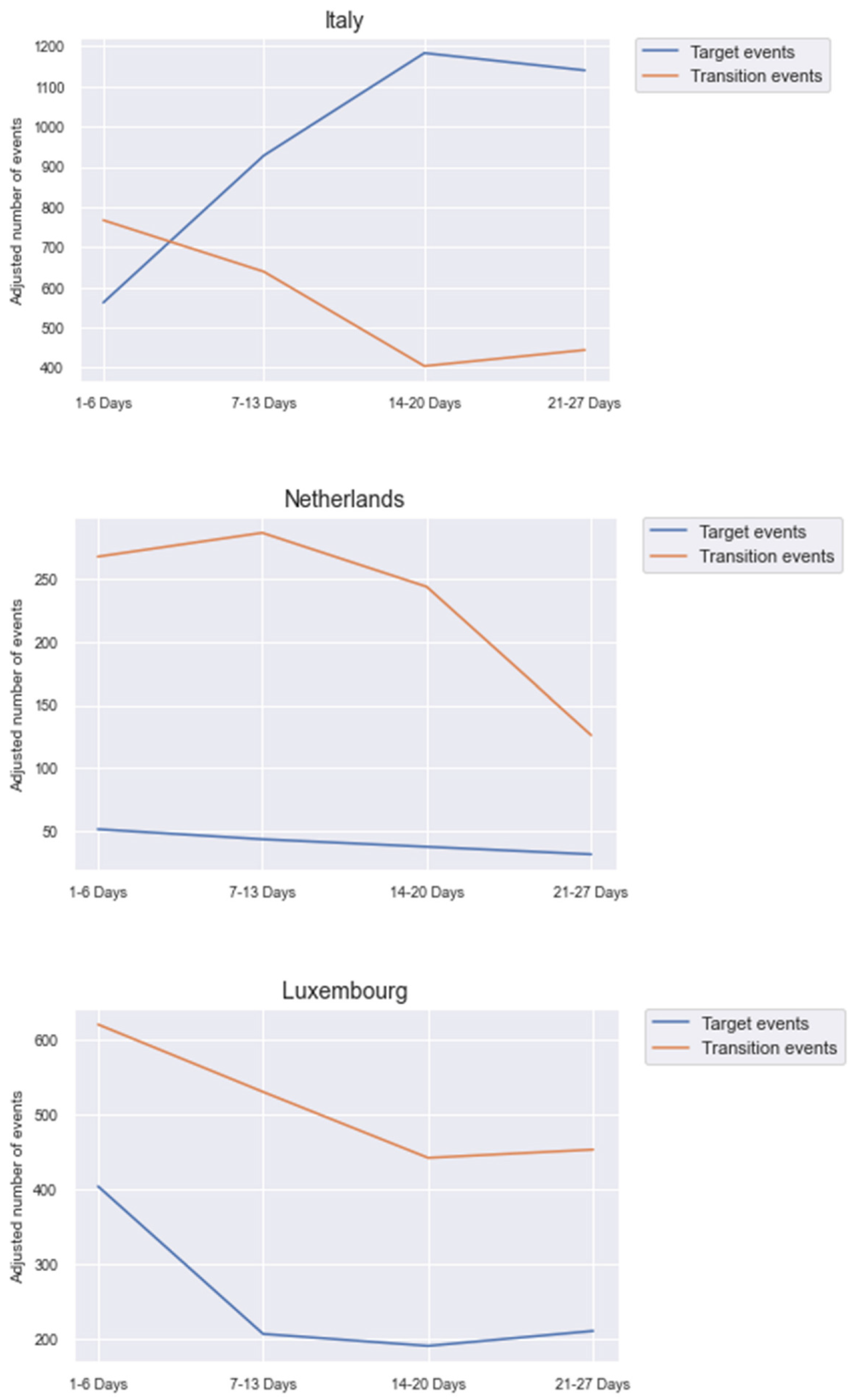
3.1. Telemetry Data and Usability
- Italy: 417 target events and 1.334 transition events
- Luxembourg: 252 target events and 984 transition events
- Netherlands: 90 target events and 572 transition events
- Early morning: From 6 to 8 o’clock
- Morning: From 9 to 10 o’clock
- Lunchtime: From 11 to 13 o’clock
- Afternoon: From 14 to 17 o’clock
- Evening: From 18 to 22 o’clock
- Night: From 23 to 5 o’clock
3.2. Closeness Scale and Role of Anne
- It is nice to have Anne in my room and to play the card game. I also have a paper agenda. I write everything down. I like that Anne speaks out about everything
- It makes me more confident about myself when Anne says what to do, and I can read it in my agenda
- I have a new buddy, that’s nice!
- No panic anymore, confident that I will not miss medication or appointments
- She does not correspond to my needs except the games
- She irritated me. She was constantly there and it made me aware that I am getting older
- I don’t like using technology. I didn’t find Anna interesting
- I have other APPs in my tablet that perform more and better. I do not need it now as it is but maybe in the future.
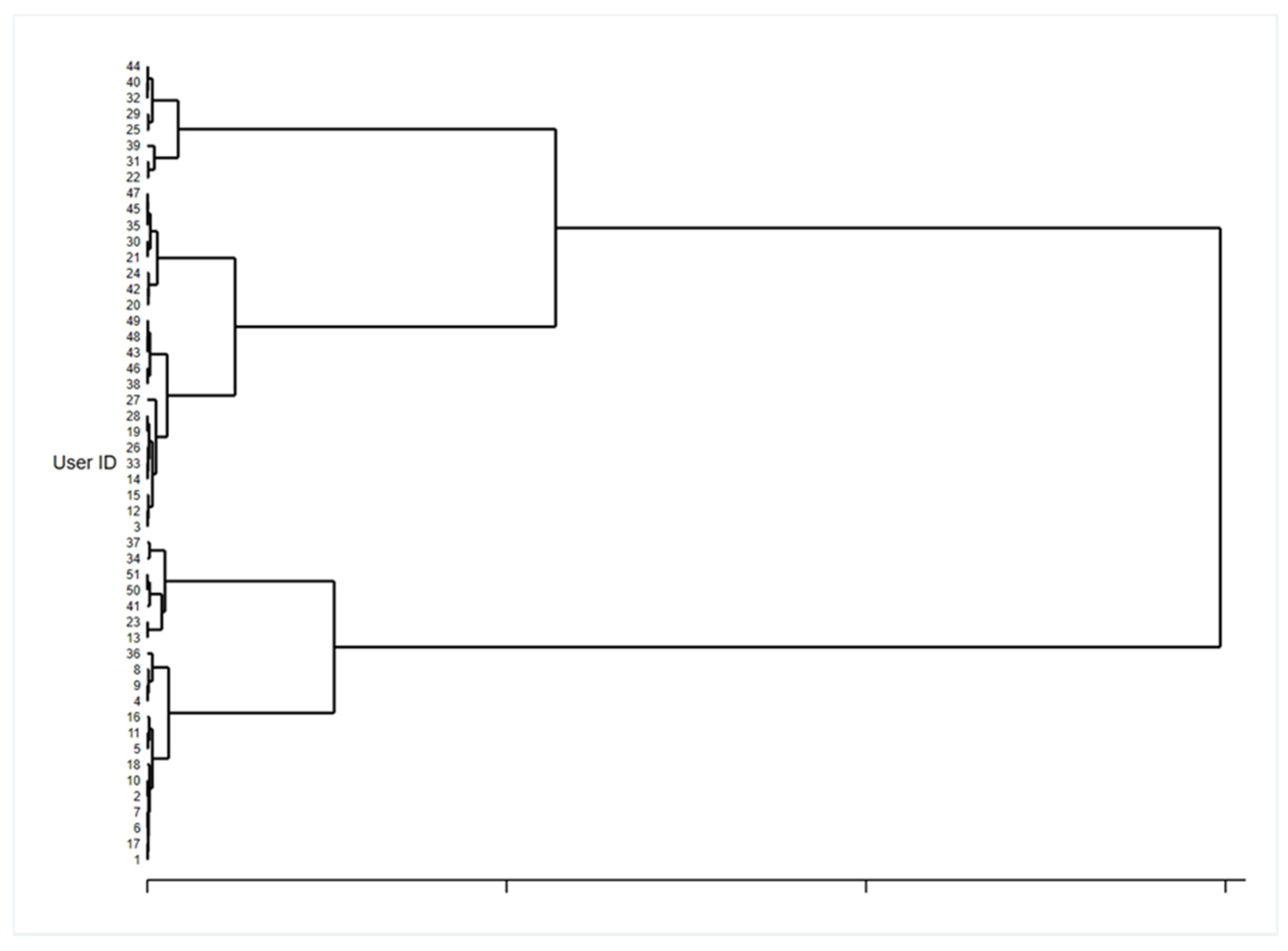
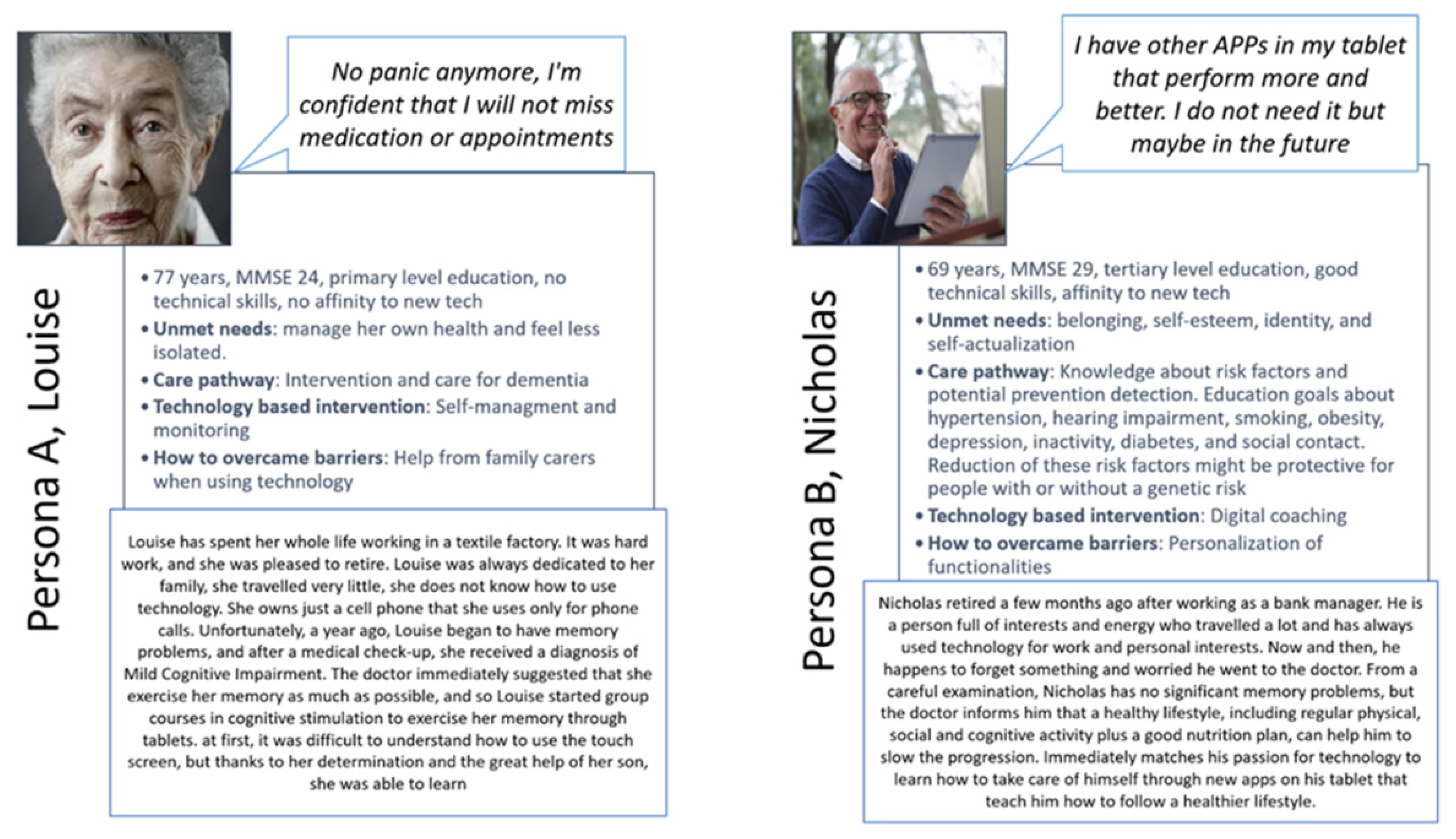
3.3. Cluster Analysis and Personas to Identify Technology-Based Intervention in the Care Pathway
4. Discussion
Comparison with Prior Works and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abd-Alrazaq, A.; Alajlani, M.; Alhuwail, D.; Schneider, J.; Al-Kuwari, S.; Shah, Z.; Hamdi, M.; Househ, M. Artificial Intelligence in the Fight Against COVID-19: Scoping Review. J. Med. Internet Res. 2020, 22, e20756. [Google Scholar] [CrossRef]
- Golinelli, D.; Boetto, E.; Carullo, G.; Nuzzolese, A.G.; Landini, M.P.; Fantini, M.P. Adoption of Digital Technologies in Health Care During the COVID-19 Pandemic: Systematic Review of Early Scientific Literature. J. Med. Internet Res. 2020, 22, e22280. [Google Scholar] [CrossRef] [PubMed]
- Irwin, K.; Sexton, C.; Daniel, T.; Lawlor, B.; Naci, L. Healthy Aging and Dementia: Two Roads Diverging in Midlife? Front. Aging Neurosci. 2018, 10, 275. [Google Scholar] [CrossRef] [Green Version]
- Alzheimer’s Association. 2020 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2020, 16, 391. [Google Scholar] [CrossRef] [PubMed]
- Øksnebjerg, L.; Woods, B.; Ruth, K.; Lauridsen, A.; Kristiansen, S.; Holst, H.D.; Waldemar, G. A Tablet App Supporting Self-Management for People With Dementia: Explorative Study of Adoption and Use Patterns. JMIR mHealth uHealth 2020, 8, e14694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meiland, F.; Innes, A.; Mountain, G.; Robinson, L.; Van Der Roest, H.; García-Casal, J.A.; Gove, D.; Thyrian, J.R.; Evans, S.; Dröes, R.-M.; et al. Technologies to Support Community-Dwelling Persons With Dementia: A Position Paper on Issues Regarding Development, Usability, Effectiveness and Cost-Effectiveness, Deployment, and Ethics. JMIR Rehabil. Assist. Technol. 2017, 4, e1. [Google Scholar] [CrossRef]
- Fabricatore, C.; Radovic, D.; Lopez, X.; Grasso-Cladera, A.; Salas, C.E. When technology cares for people with dementia: A critical review using neuropsychological rehabilitation as a conceptual framework. Neuropsychol. Rehabil. 2019, 30, 1558–1597. [Google Scholar] [CrossRef]
- Rampioni, M.; Stara, V.; Felici, E.; Rossi, L.; Paolini, S. Embodied Conversational Agents for Patients with Dementia: Thematic Literature Analysis. JMIR mHealth uHealth 2021, 9, e2538. [Google Scholar] [CrossRef] [PubMed]
- Morandell, M.; Hochgatterer, A.; Fagel, S.; Wassertheurer, S. Avatars in assistive homes for the elderly: A user-friendly way of interaction? In Proceedings of the 4th Symposium of the Workgroup Human-Computer Interaction and Usability Engineering (HCI&UE) of the Austrian Computer Society, Graz, Austria, 20–21 November 2008; Springer: Berlin/Heidelberg, Germany, 2008; pp. 391–402. [Google Scholar]
- Carrasco, E.; Epelde, G.; Moreno, A.; Ortiz, A.; Garcia, I.; Buiza, C.; Urdaneta, E.; Etxaniz, A.; González, M.F.; Arruti, A. Natural interaction between avatars and persons with Alzheimer’s disease. In Proceedings of the 11th International Conference on Computers Helping People with Special Needs (ICCHP), Linz, Austria, 9–11 July 2008; Springer: Berlin/Heidelberg, Germany, 2008; pp. 38–45. [Google Scholar]
- Huang, H.-H.; Matsushita, H.; Kawagoe, K.; Sakai, Y.; Nonaka, Y.; Nakano, Y.; Yasuda, K. Toward a memory assistant companion for the individuals with mild memory impairment. In Proceedings of the 11th IEEE International Conference on Cognitive Informatics and Cognitive Computing (ICCI*CC), Kyoto, Japan, 22–24 August 2012; IEEE CS Press: Washington, DC, USA, 2012; pp. 295–299. [Google Scholar]
- Yaghoubzadeh, R.; Kramer, M.; Pitsch, K.; Kopp, S. Virtual agents as daily assistants for elderly or cognitively impaired people. In Proceedings of the 13th International Workshop on Intelligent Virtual Agents (IVA), Edinburgh, UK, 29–31 August 2013; Springer: Berlin/Heidelberg, Germany, 2013; pp. 79–91. [Google Scholar]
- Yasuda, K.; Aoe, J.I.; Fuketa, M. Development of an agent system for conversing with individuals with dementia. In Proceedings of the 27th Annual Conference of the Japanese Society for Artificial Intelligence, Toyama, Japan, 4–7 June 2013; p. 3C1-IOS-1b-2. [Google Scholar]
- Tsiourti, C.; Quintas, J.; Ben-Moussa, M.; Hanke, S.; Nijdam, N.A.; Konstantas, D. The CaMeLi framework—a multimodal virtual companion for older adults. In Proceedings of the SAI Intelligent Systems Conference (IntelliSys), London, UK, 21–22 September 2016; Springer: Cham, Switzerland, 2018; pp. 196–217. [Google Scholar]
- Montenegro, J.L.Z.; da Costa, C.A.; Righi, R.D.R. Survey of conversational agents in health. Expert Syst. Appl. 2019, 129, 56–67. [Google Scholar] [CrossRef]
- Provoost, S.; Lau, H.M.; Ruwaard, J.; Riper, H. Embodied Conversational Agents in Clinical Psychology: A Scoping Review. J. Med. Internet Res. 2017, 19, e151. [Google Scholar] [CrossRef] [Green Version]
- Luria, M.; Reig, S.; Tan, X.Z.; Steinfeld, A.; Forlizzi, J.; Zimmerman, J. Re-Embodiment and Co-Embodiment: Exploration of social presence for robots and conversational agents. In Proceedings of the 2019 on Designing Interactive Systems Conference, San Diego, CA, USA, 18 June 2019; pp. 633–644. [Google Scholar]
- ter Stal, S.; Kramer, L.L.; Tabak, M.; Akker, H.O.D.; Hermens, H. Design Features of Embodied Conversational Agents in eHealth: A Literature Review. Int. J. Hum. Comput. Stud. 2020, 138, 102409. [Google Scholar] [CrossRef]
- Stara, V.; Vera, B.; Bolliger, D.; Rossi, L.; Felici, E.; Di Rosa, M.; de Jong, M.; Paolini, S. Usability and Acceptance of the Embodied Conversational Agent Anne by People with Dementia and their Caregivers: An exploratory study in home environment settings (Preprint). JMIR mHealth uHealth 2020, 9, e25891. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. ‘Mini-mental state’. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Benkaouar, W.; Vaufreydaz, D. Multi-sensors Engagement Detection with a Robot Companion in a Home Environment. In Proceedings of the Workshop on Assistance and Service Robotics in a Human Environment at IEEE International Conference on Intelligent Robots and Systems, Vilamoura, Algarve, Portugal, 7–12 October 2012. [Google Scholar]
- Qol Logsdon, R.; Gibbons, L.; McCurry, S.; Teri, L. Quality of life in Alzheimer’s disease: Patient and caregiver reports. J. Ment. Health Age 1999, 5, 21–32. [Google Scholar]
- Logsdon, R.G.; Gibbons, L.E.; McCurry, S.M.; Teri, L. Assessing Quality of Life in Older Adults With Cognitive Impairment. Psychosom. Med. 2002, 64, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Brooke, J. SUS: A ‘Quick and Dirty’ Usability Scale. Usability Eval. Ind. 1996, 189, 4–7. [Google Scholar]
- Sauro, J.R. Lewis, Quantifying the User Experience: Practical Statistics for User Research; Elsevier: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Gaechter, S.; Starmer, C.; Tufano, F. Measuring the Closeness of Relationships: A Comprehensive Evaluation of the ’Inclusion of the Other in the Self’ Scale. PLoS ONE 2015, 10, e0129478. [Google Scholar] [CrossRef]
- Goodman, E.; Kuniavsky, M.; Moed, A. Observing the User Experience: A Practitioner’s Guide to User Research (Second Edition). IEEE Trans. Dependable Secur. Comput. 2013, 56, 260–261. [Google Scholar] [CrossRef]
- Kitwood, T. The Experience of Dementia. Aging Ment. Health 1997, 1, 13–22. [Google Scholar] [CrossRef]
- European Commission. Blueprint Digital Transformation of Health and Care for the Ageing Society. Available online: https://ec.europa.eu/eip/ageing/blueprint_en (accessed on 15 June 2021).
- WHO (World Health Organisation). Global Action Plan on the Public Health Response to Dementia, 2017–2025; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- WHO (World Health Organisation). Dementia: A Public Health Priority; World Health Organisation: Geneva, Switzerland, 2012; ISBN 978-92-4-156445-8. [Google Scholar]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Volpe, U.; Amin, H.; Ayinde, O.; Burns, A.; Chan, W.C.; David, R.; Dejanovic, S.D.; Djokic, G.; Eraslan, D.; Fischer, G.A.; et al. Pathways to care for people with dementia: An international multicentre study. Int. J. Geriatr. Psychiatry 2019, 35, 163–173. [Google Scholar] [CrossRef]
- Samsi, K.; Manthorpe, J. Care pathways for dementia: Current perspectives. Clin. Interv. Aging 2014, 9, 2055–2063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boger, J.; Craig, T.; Mihailidis, A. Examining the impact of familiarity on faucet usability for older adults with dementia. BMC Geriatr. 2013, 13, 63. [Google Scholar] [CrossRef] [Green Version]
- Burmeister, O.K. The development of assistive dementia technology that accounts for the values of those affected by its use. Ethic. Inf. Technol. 2016, 18, 185–198. [Google Scholar] [CrossRef]
- Wargnier, P.; Malaise, A.; Jacquemot, J.; Benveniste, S.; Jouvelot, P.; Pino, M.; Rigaud, A.-S. Towards Attention Monitoring of Older Adults with Cognitive Impairment during Interaction with an Embodied Conversational Agent. In Proceedings of the Third International Workshop on Virtual and Augmented Assistive Technology, Arles, France, 23–23 March 2015; p. 6. [Google Scholar]
- Holthe, T.; Halvorsrud, L.; Karterud, D.; Hoel, K.-A.; Lund, A. Usability and acceptability of technology for community-dwelling older adults with mild cognitive impairment and dementia: A systematic literature review. Clin. Interv. Aging 2018, 13, 863–886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO clinical consortium on healthy ageing: Topic focus: Frailty and intrinsic capacity. In WHO Clinical Consortium on Healthy Ageing Topic Focus: Frailty and Intrinsic Capacity; World Health Organization: Geneva, Switzerland, 1 December 2016; pp. 1–22. [Google Scholar]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Koo, B.M.; Vizer, L.M. Examining Mobile Technologies to Support Older Adults with Dementia through the Lens of Personhood and Human Needs: Scoping Review. JMIR mHealth uHealth 2019, 7, e15122. [Google Scholar] [CrossRef] [PubMed]
- Person-Centred Care. United Kingdom: Alzheimer’s Society. Available online: https://www.alzheimers.org.uk/about-dementia/treatments/person-centred-care (accessed on 2 August 2021).
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Ryan, R.; Deci, E. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, Wellness; Guilford: New York, NY, USA, 2017. [Google Scholar]
- Tam, M.T.; Dosso, J.A.; Robillard, J.M. The Impact of a Global Pandemic on People Living with Dementia and Their Care Partners: Analysis of 417 Lived Experience Reports. J. Alzheimer’s Dis. 2021, 80, 865–875. [Google Scholar] [CrossRef]
- Bacsu, J.-D.; O’Connell, M.E.; Cammer, A.; Azizi, M.; Grewal, K.; Poole, L.; Green, S.; Sivananthan, S.; Spiteri, R.J. Using Twitter to Understand the COVID-19 Experiences of People With Dementia: Infodemiology Study. J. Med. Internet Res. 2021, 23, e26254. [Google Scholar] [CrossRef]
- Rai, H.K.; Barroso, A.C.; Yates, L.; Schneider, J.; Orrell, M. Involvement of People with Dementia in the Development of Technology-Based Interventions: Narrative Synthesis Review and Best Practice Guidelines. J. Med. Internet Res. 2020, 22, e17531. [Google Scholar] [CrossRef]
- Vander Plas, J. Python Data Science Handbook; O’Reiliy Media: Sebastopol, CA, USA, 2016; ISBN 9781491912058. [Google Scholar]
- Stricker, R.; Hommel, S.; Martin, S.; Gross, H.M. Realtime User Attention and Emotion Estimation on a mobile Robot. In Proceedings of the Crossing Borders within the ABC: Automation, Biomedical Engineering and Computer Science, Universität Ilmenau, Herausgeber, Germany, 13–17 September 2010; Volume 55, pp. 629–634. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IT N = 20 | LUX N = 20 | NL N = 15 | TOTAL N = 55 | |
|---|---|---|---|---|
| Age, mean (SD) | 75.5 (4.2) | 71.5 (11.2) | 63.6 (9.7) | 70.8 (9.9) |
| Gender (%) | ||||
| Male | 30.0 | 45.0 | 33.3 | 36.4 |
| Female | 70.0 | 55.0 | 66.7 | 63.6 |
| Marital status (%) | ||||
| Married | 85.0 | 35.0 | 13.3 | 47.3 |
| Full time relationship | 0.0 | 0.0 | 0.0 | 0.0 |
| Separated | 0.0 | 5.0 | 0.0 | 1.8 |
| Divorced | 5.0 | 20.0 | 0.0 | 9.1 |
| Single | 5.0 | 15.0 | 86.7 | 30.9 |
| Widowed | 5.0 | 25.0 | 0.0 | 10.9 |
| Education (%) | ||||
| No education | 0.0 | 0.0 | 13.3 | 3.6 |
| Primary | 35.0 | 20.0 | 53.3 | 34.6 |
| Secondary | 20.0 | 70.0 | 33.4 | 41.8 |
| Tertiary | 45.0 | 10.0 | 0.0 | 20.0 |
| MMSE, mean (SD) | 25.2 (1.3) | 29.2 (1.2) | 26.6 (2.0) | 27.0 (2.3) |
| QoL pre, mean (SD) | 28.5 (6.6) | 35.9 (6.3) | 37.4 (3.7) | 28.5 (6.6) |
| QoL post, mean (SD) | 28.9 (7.8) | 35.6 (4.8) | 38.0 (2.3) | 28.9 (7.8) |
| delta Qol, mean (SD) | 0.4 (4.6) | −0.3 (5.3) | 0.8 (1.6) | 0.4 (4.6) |
| SUS Items | IT | LUX | NL | TOT |
|---|---|---|---|---|
| Item 1. I think that I would like to use this system frequently | 3.8 (1.3) | 2.5 (1.4) | 3.5 (0.8) | 3.2 (1.3) |
| Item 2. I found the system unnecessary complex | 1.8 (1.0) | 1.7 (1.4) | 1.8 1.0) | 1.7 (1.1) |
| Item 3. I thought the system was easy to use | 4.1 (1.2) | 3.8 (1.4) | 3.1 (1.2) | 3.8 (1.3) |
| Item 4. I think that I would need the support of a technical person | 2.9 (1.5) | 2.2 (1.2) | 2.2 (1.2) | 2.2 (1.4) |
| Item 5. I found the various functions well integrated | 3.7 (0.9) | 3.1 (1.2) | 2.5 (0.5) | 3.1 (1.0) |
| Item 6. I thought there was too much inconsistency | 2.4 (1.3) | 2.6 (1.2) | 2.3 (1.1) | 2.6 (1.2) |
| Item 7. I would imagine that most people would learn quickly | 3.9 (0.9) | 3.7 (1.0) | 3.3 (0.8) | 3.7 (0.9) |
| Item 8. I found the system very cumbersome | 2.0 (1.1) | 2.2 (1.3) | 1.7 (0.9) | 2.2 (1.2) |
| Item 9. I felt very confident using the system | 3.3 (1.5) | 3.5 (1.2) | 3.4 (1.0) | 3.5 (1.3) |
| Item 10. I needed to learn a lot of things before I could get going | 2.9 (1.3) | 2.4 (1.3) | 2.8 (1.0) | 2.4 (1.4) |
| SUS Score | 67.1 (23.3) | 65.3 (16.7) | 66.3 (15.2) | 66.2 (19.0) |
| Total | Cluster 1 | Cluster 2 | p-Value | |
|---|---|---|---|---|
| N = 51 (4 Missing) | N = 21 | N = 30 | ||
| Cluster analysis variables | ||||
| Gender, n (%) | 0.917 | |||
| Female | 32 (62.7) | 13 (61.9) | 19 (63.3) | |
| Male | 19 (37.3) | 8 (38.1) | 11 (36.7) | |
| Age class, n (%) | 0.000 | |||
| <70 | 23 (45.1) | 0 (0.0) | 23 (76.7) | |
| 71+ | 28 (54.9) | 21 (100.0) | 7(23.3) | |
| Education, n (%) | 0.813 | |||
| Low | 20 (39.2) | 8 (38.1) | 12 (40.0) | |
| Medium | 21 (41.2) | 8 (38.1) | 13 (43.3) | |
| High | 10 (19.6) | 5 (23.8) | 5 (16.7) | |
| MMSE score, n (%) | 0.020 | |||
| 24–27 | 29 (56.9) | 16 (76.2) | 13 (43.3) | |
| 28–30 | 22 (43.1) | 5 (23.8) | 17 (56.7) | |
| Have you ever used a tabletbefore this experience? n (%) | 0.004 | |||
| Yes | 22 (43.1) | 4 (19.0) | 18 (60.0) | |
| No | 29 (56.9) | 17 (81.0) | 12 (40.0) | |
| Outcome variables | ||||
| SUS score, mean (SD) | 66.22 (19.6) | 60.48 (24.8) | 70.87 (12.8) | 0.070 |
| Closeness scale, mean (SD) | 2.40 (1.4) | 2.14 (1.3) | 2.62 (1.6) | 0.273 |
| Role of Anne, n (%) | 0.027 | |||
| Friend, Assistant, Reminder | 37 (77.1) | 13 (61.9) | 24 (88.9) | |
| No Role | 11 (22.9) | 8 (38.1) | 3 (11.1) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stara, V.; Vera, B.; Bolliger, D.; Paolini, S.; de Jong, M.; Felici, E.; Koenderink, S.; Rossi, L.; Von Doellen, V.; di Rosa, M. Toward the Integration of Technology-Based Interventions in the Care Pathway for People with Dementia: A Cross-National Study. Int. J. Environ. Res. Public Health 2021, 18, 10405. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910405
Stara V, Vera B, Bolliger D, Paolini S, de Jong M, Felici E, Koenderink S, Rossi L, Von Doellen V, di Rosa M. Toward the Integration of Technology-Based Interventions in the Care Pathway for People with Dementia: A Cross-National Study. International Journal of Environmental Research and Public Health. 2021; 18(19):10405. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910405
Chicago/Turabian StyleStara, Vera, Benjamin Vera, Daniel Bolliger, Susy Paolini, Michiel de Jong, Elisa Felici, Stephanie Koenderink, Lorena Rossi, Viviane Von Doellen, and Mirko di Rosa. 2021. "Toward the Integration of Technology-Based Interventions in the Care Pathway for People with Dementia: A Cross-National Study" International Journal of Environmental Research and Public Health 18, no. 19: 10405. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910405