
Psychosocial Impact of the COVID-19 Pandemic on Healthcare Workers and Initial Areas of Action for Intervention and Prevention—The egePan/VOICE Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Composition and Description of the Sample
3.2. Stress Factors and Problems Due to COVID-19 and Protective Factors
3.3. Gender Differences
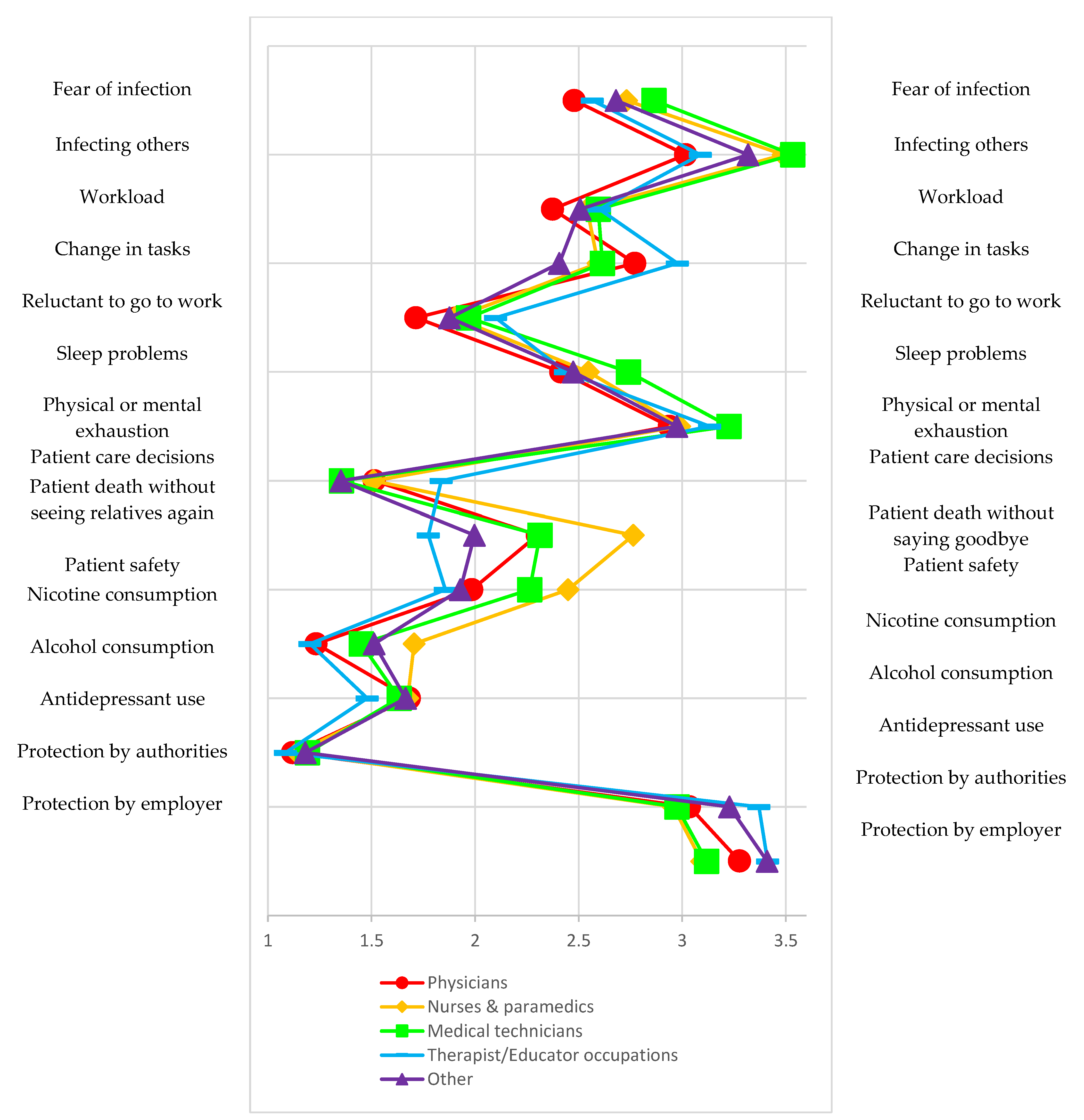
3.4. Comparison of Different Occupational Groups
3.5. Comparison of Persons with Contact versus Those without Contact
3.6. Other Characteristics (the Differences Depicted Refer to the Reference Group in Each Case, e.g., Respondents with a Migrant Background versus Those without One)—Home Office, Migrant Background, Living Alone, Caregiving Responsibilities and Age
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brooks, S.K.; Dunn, R.; Amlôt, R.; Rubin, G.J.; Greenberg, N. A systematic, thematic review of social and occupational factors associated with psychological outcomes in healthcare employees during an infectious disease outbreak. J. Occup. Environ. Med. 2018, 60, 248–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulfinger, N.; Lampl, J.; Dinkel, A.; Weidner, K.; Beutel, M.E.; Jarczok, M.N.; Hildenbrand, G.; Kruse, J.; Seifried-Dübon, T.; Junne, F. Psychological stress caused by epidemics among health care workers and implications for coping with the corona crisis: A literature review. Z. Psychosom. Med. Psychother. 2020, 66, 220–242. [Google Scholar]
- Magnavita, N.; Chirico, F.; Garbarino, S.; Bragazzi, N.L.; Santacroce, E.; Zaffina, S. SARS/MERS/SARS-CoV-2 outbreaks and Burnout Syndrome among healthcare workers. An umbrella systematic review. Int. J. Environ. Res. Public Health 2021, 18, 4361. [Google Scholar] [CrossRef] [PubMed]
- Bohlken, J.; Schömig, F.; Lemke, M.R.; Pumberger, M.; Riedel-Heller, S.G. COVID-19-pandemie: Belastungen des medizinischen personals. Psychiatr. Prax. 2020, 47, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Gilan, D.; Blessin, M.; Kunzler, A.; Stoffers-Winterling, J.; Müssig, M.; Yuen, K.S.; Tüscher, O.; Lieb, K.; Röthke, N.; Thrul, J. Psychische Belastungen, Resilienz, Risiko-und protektive Faktoren während der SARS-CoV-2-Pandemie’Systematische Literaturanalyse und Studienergebnisse aus dem deutschen COSMO-Panel. Dtsch. Arztebl. Int. 2020, 117, 625–632. [Google Scholar]
- Spoorthy, M.S.; Pratapa, S.K.; Mahant, S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic—A review. Asian J. Psychiatry 2020, 51, 102119. [Google Scholar] [CrossRef]
- Adhanom Ghebreyesus, T. Addressing mental health needs: An integral part of COVID-19 response. World Psychiatry 2020, 19, 129–130. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1002/wps.20768 (accessed on 28 September 2021). [CrossRef] [PubMed]
- Unützer, J.; Kimmel, R.J.; Snowden, M. Psychiatry in the age of COVID-19. World Psychiatry 2020, 19, 130–131. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1002/wps.20766 (accessed on 28 September 2021). [CrossRef]
- Marazziti, D.; Stahl, S.M. The relevance of COVID-19 pandemic to psychiatry. World Psychiatry 2020, 19, 261. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/wps.20764 (accessed on 28 September 2021). [CrossRef]
- Tyrer, P. COVID-19 health anxiety. World Psychiatry 2020, 19, 307–308. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1002/wps.20798 (accessed on 28 September 2021). [CrossRef]
- Que, J.; Le Shi, J.D.; Liu, J.; Zhang, L.; Wu, S.; Gong, Y.; Huang, W.; Yuan, K.; Yan, W.; Sun, Y. Psychological impact of the COVID-19 pandemic on healthcare workers: A cross-sectional study in China. Gen. Psychiatry 2020, 33, e100259. [Google Scholar] [CrossRef] [PubMed]
- Trumello, C.; Bramanti, S.M.; Ballarotto, G.; Candelori, C.; Cerniglia, L.; Cimino, S.; Crudele, M.; Lombardi, L.; Pignataro, S.; Viceconti, M.L. Psychological adjustment of healthcare workers in Italy during the COVID-19 pandemic: Differences in stress, anxiety, depression, burnout, secondary trauma, and compassion satisfaction between frontline and non-frontline professionals. Int. J. Environ. Res. Public Health 2020, 17, 8358. [Google Scholar] [CrossRef] [PubMed]
- Torrente, M.; Sousa, P.A.; Sánchez-Ramos, A.; Pimentao, J.; Royuela, A.; Franco, F.; Collazo-Lorduy, A.; Menasalvas, E.; Provencio, M. To burn-out or not to burn-out: A cross-sectional study in healthcare professionals in Spain during COVID-19 pandemic. BMJ Open 2021, 11, e044945. [Google Scholar] [CrossRef] [PubMed]
- Martínez-López, J.Á.; Lázaro-Pérez, C.; Gómez-Galán, J.; Fernández-Martínez, M.d.M. Psychological impact of COVID-19 emergency on health professionals: Burnout incidence at the most critical period in Spain. J. Clin. Med. 2020, 9, 3029. [Google Scholar] [CrossRef] [PubMed]
- Martínez-López, J.Á.; Lázaro-Pérez, C.; Gómez-Galán, J. Burnout among Direct-Care Workers in Nursing Homes during the COVID-19 Pandemic in Spain: A Preventive and Educational Focus for Sustainable Workplaces. Sustainability 2021, 13, 2782. Available online: https://doaj.org/article/7e29ab5ffd56482d9e5cc00eb5dccfd6 (accessed on 28 September 2021). [CrossRef]
- Skoda, E.; Teufel, M.; Stang, A.; Jöckel, K.; Junne, F.; Weismüller, B.; Hetkamp, M.; Musche, V.; Kohler, H.; Dörrie, N. Psychological burden of healthcare professionals in Germany during the acute phase of the COVID-19 pandemic: Differences and similarities in the international context. J. Public Health 2020, 42, 688–695. [Google Scholar] [CrossRef]
- Zerbini, G.; Ebigbo, A.; Reicherts, P.; Kunz, M.; Messman, H. Psychosocial burden of healthcare professionals in times of COVID-19—A survey conducted at the University Hospital Augsburg. GMS Ger. Med. Sci. 2020, 18, Doc05. [Google Scholar]
- Morawa, E.; Schug, C.; Geiser, F.; Beschoner, P.; Jerg-Bretzke, L.; Albus, C.; Weidner, K.; Hiebel, N.; Borho, A.; Erim, Y. Psychosocial burden and working conditions during the COVID-19 pandemic in Germany: The VOICE survey among 3678 health care workers in hospitals. J. Psychosom Res. 2021, 144, 110415. [Google Scholar] [CrossRef]
- Steudte-Schmiedgen, S.; Stieler, L.; Erim, Y.; Morawa, E.; Geiser, F.; Beschoner, P.; Jerg-Bretzke, L.; Albus, C.; Hiebel, N.; Weidner, K. Correlates and Predictors of PTSD Symptoms Among Healthcare Workers During the COVID-19 Pandemic: Results of the egePan-VOICE Study. Front. Psychiatry 2021, 12, 686667. [Google Scholar] [CrossRef]
- Elbay, R.Y.; Kurtulmuş, A.; Arpacıoğlu, S.; Karadere, E. Depression, anxiety, stress levels of physicians and associated factors in COVID-19 pandemics. Psychiatry Res. 2020, 290, 113130. [Google Scholar] [CrossRef]
- Kaltwasser, A.; Pelz, S.; Nydahl, P.; Dubb, R.; Borzikowsky, C. Querschnittsstudie zu Arbeitsbedingungen und Versorgungsqualität in der Versorgung von COVID-19-Patienten. Anaesthesist 2021, 70, 1–8. [Google Scholar] [CrossRef]
- Shaukat, N.; Ali, D.M.; Razzak, J. Physical and mental health impacts of COVID-19 on healthcare workers: A scoping review. Int. J. Emerg. Med. 2020, 13, 40. [Google Scholar] [CrossRef]
- Galea, S.; Merchant, R.M.; Lurie, N. The mental health consequences of COVID-19 and physical distancing: The need for prevention and early intervention. JAMA Intern. Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [Green Version]
- Walton, M.; Murray, E.; Christian, M.D. Mental health care for medical staff and affiliated healthcare workers during the COVID-19 pandemic. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 241–247. [Google Scholar] [CrossRef]
- Muller, R.A.E.; Stensland, R.S.Ø; van de Velde, R.S. The mental health impact of the COVID-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Res. 2020, 293, 113441. [Google Scholar] [CrossRef]
- Panagioti, M.; Geraghty, K.; Johnson, J.; Zhou, A.; Panagopoulou, E.; Chew-Graham, C.; Peters, D.; Hodkinson, A.; Riley, R.; Esmail, A. Association between physician burnout and patient safety, professionalism, and patient satisfaction: A systematic review and meta-analysis. JAMA Intern. Med. 2018, 178, 1317–1331. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.H.; Sermeus, W.; Van den Heede, K.; Sloane, D.M.; Busse, R.; McKee, M.; Bruyneel, L.; Rafferty, A.M.; Griffiths, P.; Moreno-Casbas, M.T. Patient safety, satisfaction, and quality of hospital care: Cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ 2012, 344, e1717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturm, H.; Rieger, M.A.; Martus, P.; Ueding, E.; Wagner, A.; Holderried, M.; Maschmann, J. WorkSafeMed Consortium Do perceived working conditions and patient safety culture correlate with objective workload and patient outcomes: A cross-sectional explorative study from a German university hospital. PLoS ONE 2019, 14, e0209487. [Google Scholar] [CrossRef] [Green Version]
- Thatrimontrichai, A.; Weber, D.J.; Apisarnthanarak, A. Mental health among healthcare personnel during COVID-19 in Asia: A systematic review. J. Formos. Med. Assoc. 2021, 120, 1296–1304. [Google Scholar] [CrossRef] [PubMed]
- Matsuishi, K.; Kawazoe, A.; Imai, H.; Ito, A.; Mouri, K.; Kitamura, N.; Miyake, K.; Mino, K.; Isobe, M.; Takamiya, S. Psychological impact of the pandemic (H1N1) 2009 on general hospital workers in Kobe. Psychiatry Clin. Neurosci. 2012, 66, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B (Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- De Pablo, G.S.; Vaquerizo-Serrano, J.; Catalan, A.; Arango, C.; Moreno, C.; Ferre, F.; Shin, J.I.; Sullivan, S.; Brondino, N.; Solmi, M. Impact of coronavirus syndromes on physical and mental health of health care workers: Systematic review and meta-analysis. J. Affect. Disord. 2020, 275, 48–57. [Google Scholar] [CrossRef]
- Busch, I.M.; Moretti, F.; Mazzi, M.; Wu, A.W.; Rimondini, M. What we have learned from two decades of epidemics and pandemics: A systematic review and meta-analysis of the psychological burden of frontline healthcare workers. Psychother. Psychosom. 2021, 90, 1–13. [Google Scholar] [CrossRef]
- Petzold, M.B.; Plag, J.; Ströhle, A. Dealing with psychological distress by healthcare professionals during the COVID-19 pandemia. Nervenarzt 2020, 91, 417–421. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/32221635 (accessed on 28 September 2021). [CrossRef] [PubMed] [Green Version]
- Tomlin, J.; Dalgleish-Warburton, B.; Lamph, G. Psychosocial Support for Healthcare Workers During the COVID-19 Pandemic. Front. Psychol. 2020, 11, 1960. Available online: https://0-search-proquest-com.brum.beds.ac.uk/docview/2437844434 (accessed on 28 September 2021). [CrossRef] [PubMed]
- Zepinic, V. COVID-19: An Urgency to Address Mental Health Consequences. Psychology 2021, 12, 735–748. [Google Scholar] [CrossRef]
- Bellanti, F.; Lo Buglio, A.; Capuano, E.; Dobrakowski, M.; Kasperczyk, A.; Kasperczyk, S.; Ventriglio, A.; Vendemiale, G. Factors Related to Nurses’ Burnout during the First Wave of Coronavirus Disease-19 in a University Hospital in Italy. Int. J. Environ. Res. Public Health 2021, 18, 5051. Available online: https://0-search-proquest-com.brum.beds.ac.uk/docview/2536499315 (accessed on 28 September 2021). [CrossRef] [PubMed]
- Azoulay, E.; Pochard, F.; Reignier, J.; Argaud, L.; Bruneel, F.; Courbon, P.; Cariou, A.; Klouche, K.; Labbé, V.; Barbier, F.; et al. Symptoms of Mental Health Disorders in Critical Care Physicians Facing the Second COVID-19 Wave. Chest 2021, 160, 944–955. Available online: https://0-dx-doi-org.brum.beds.ac.uk/10.1016/j.chest.2021.05.023 (accessed on 28 September 2021). [CrossRef] [PubMed]
- Soklaridis, S.; Lin, E.; Lalani, Y.; Rodak, T.; Sockalingam, S. Mental health interventions and supports during COVID- 19 and other medical pandemics: A rapid systematic review of the evidence. Gen. Hosp. Psychiatry 2020, 66, 133–146. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Chung, R.C.; Bemak, F.; Kagawa-Singer, M. Gender differences in psychological distress among Southeast Asian refugees. J. Nerv. Ment. Dis. 1998, 186, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Albert, P.R. Why is depression more prevalent in women? J. Psychiatry Neurosci. JPN 2015, 40, 219. [Google Scholar] [CrossRef] [PubMed]
- Atzendorf, J.; Rauschert, C.; Seitz, N.; Lochbühler, K.; Kraus, L. Gebrauch von Alkohol, Tabak, illegalen Drogen und Medikamenten. Dtsch. Arztebl. Int. 2019, 116, 577–584. [Google Scholar]
- Barbosa, C.; Cowell, A.; Dowd, W. Alcohol Consumption in Response to the COVID-19 Pandemic in the United States. J. Addict. Med. 2020, 15, 341–344. Available online: https://0-search-proquest-com.brum.beds.ac.uk/docview/2454651385 (accessed on 28 September 2021). [CrossRef] [PubMed]
- Kabasakal, E.; Özpulat, F.; Akca, A.; Özcebe, L.H. Mental health status of health sector and community services employees during the COVID-19 pandemic. Int. Arch. Occup. Environ. Health 2021, 94, 1249–1262. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/33687541 (accessed on 28 September 2021). [CrossRef] [PubMed]
- Vanderbruggen, N.; Matthys, F.; Van Laere, S.; Zeeuws, D.; Santermans, L.; Van den Ameele, S.; Crunelle, C.L. Self-Reported Alcohol, Tobacco, and Cannabis Use during COVID-19 Lockdown Measures: Results from a Web-Based Survey. Eur. Addict. Res. 2020, 26, 309–315. Available online: https://www.karger.com/Article/FullText/510822 (accessed on 28 September 2021). [CrossRef] [PubMed]
- Bönke, T.; Glaubitz, R.; Göbler, K.; Harnack, A.; Pape, A.; Wetter, M. Die Entwicklung und Prognose von Lebenserwerbseinkommen in Deutschland; Freie Universität: Berlin, Germany, 2020. [Google Scholar]
- Zhang, W.; Wang, K.; Yin, L.; Zhao, W.; Xue, Q.; Peng, M.; Min, B.; Tian, Q.; Leng, H.; Du, J.; et al. Mental Health and Psychosocial Problems of Medical Health Workers during the COVID-19 Epidemic in China. Psychother. Psychosom. 2020, 89, 242–250. Available online: https://www.karger.com/Article/FullText/507639 (accessed on 28 September 2021). [CrossRef] [PubMed]
- Binnie, A.; Moura, K.; Moura, C.; D’Aragon, F.; Tsang, J.L.Y. Psychosocial distress amongst Canadian intensive care unit healthcare workers during the acceleration phase of the COVID-19 pandemic. PLoS ONE 2021, 16, e0254708. Available online: https://0-search-proquest-com.brum.beds.ac.uk/docview/2561483836 (accessed on 28 September 2021). [CrossRef]
- Ghimire, S.; Hallett, J.; Gray, C.; Lobo, R.; Crawford, G. What Works? Prevention and Control of Sexually Transmitted Infections and Blood-Borne Viruses in Migrants from Sub-Saharan Africa, Northeast Asia and Southeast Asia Living in High-Income Countries: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1287. [Google Scholar] [CrossRef] [Green Version]
- Koschollek, C.; Kuehne, A.; Müllerschön, J.; Amoah, S.; Batemona-Abeke, H.; Dela Bursi, T.; Mayamba, P.; Thorlie, A.; Mputu Tshibadi, C.; Wangare Greiner, V. Knowledge, information needs and behavior regarding HIV and sexually transmitted infections among migrants from sub-Saharan Africa living in Germany: Results of a participatory health research survey. PLoS ONE 2020, 15, e0227178. [Google Scholar] [CrossRef] [Green Version]
- Navarro, M.; Perez-Ayala, A.; Guionnet, A.; Perez-Molina, J.A.; Navaza, B.; Estevez, L.; Norman, F.; Flores-Chávez, M.; Lopez-Velez, R. Targeted screening and health education for Chagas disease tailored to at-risk migrants in Spain, 2007 to 2010. Eurosurveillance 2011, 16, 19973. [Google Scholar] [CrossRef] [Green Version]
- Wilson, W.; Raj, J.P.; Rao, S.; Ghiya, M.; Nedungalaparambil, N.M.; Mundra, H.; Mathew, R. Prevalence and predictors of stress, anxiety, and depression among healthcare workers managing COVID-19 pandemic in India: A nationwide observational study. Indian J. Psychol. Med. 2020, 42, 353–358. [Google Scholar] [CrossRef]
- Nwachukwu, I.; Nkire, N.; Shalaby, R.; Hrabok, M.; Vuong, W.; Gusnowski, A.; Surood, S.; Urichuk, L.; Greenshaw, A.J.; Agyapong, V.I. COVID-19 pandemic: Age-related differences in measures of stress, anxiety and depression in Canada. Int. J. Environ. Res. Public Health 2020, 17, 6366. [Google Scholar] [CrossRef]
- Arslan, H.N.; Karabekiroglu, A.; Terzi, O.; Dundar, C. The effects of the COVID-19 outbreak on physicians’ psychological resilience levels. Postgrad. Med. 2021, 133, 223–230. [Google Scholar] [CrossRef]
- Jerg-Bretzke, L.; Limbrecht, K. Where have they gone?–a discussion on the balancing act of female doctors between work and family. GMS Z. Med. Ausbild. 2012, 29, Doc19. [Google Scholar] [PubMed]
- Jerg-Bretzke, L.; Krüsmann, P.; Traue, H.C.; Limbrecht-Ecklundt, K. “Was ihr wollt ”, Ergebnisse einer empirischen Bedarfsanalyse zur Verbesserung der Vereinbarkeit von Familie und Beruf bei Ärztinnen und Ärzten. Das Gesundh. 2018, 80, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Feeley, T.; Ffrench-O’Carroll, R.; Tan, M.H.; Magner, C.; L’Estrange, K.; O’Rathallaigh, E.; Whelan, S.; Lyons, B.; O’Connor, E. A model for occupational stress amongst paediatric and adult critical care staff during COVID-19 pandemic. Int. Arch. Occup. Environ. Health 2021, 94, 1721–1737. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/33630134 (accessed on 28 September 2021). [CrossRef] [PubMed]
- Fang, X.; Wu, L.; Lu, L.; Kan, X.; Wang, H.; Xiong, Y.; Ma, D.; Wu, G. Mental health problems and social supports in the COVID-19 healthcare workers: A Chinese explanatory study. BMC Psychiatry 2021, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Schmuck, J.; Hiebel, N.; Rabe, M.; Schneider, J.; Erim, Y.; Morawa, E.; Jerg-Bretzke, L.; Beschoner, P.; Albus, C.; Hannemann, J.; et al. Sense of coherence, social support and religiosity as resources for medical personnel during the COVID-19 pandemic: A web-based survey among 4324 health care workers within the German Network University Medicine. PLoS ONE 2021, 16, e0255211. Available online: https://0-search-proquest-com.brum.beds.ac.uk/docview/2555636986 (accessed on 28 September 2021). [CrossRef]
- Morganstein, J.C.; Flynn, B.W. Enhancing Psychological Sustainment & Promoting Resilience in Healthcare Workers During COVID-19 & Beyond: Adapting Crisis Interventions from High-Risk Occupations. J. Occup. Environ. Med. 2021, 63, 482–489. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/33710105 (accessed on 28 September 2021). [CrossRef] [PubMed]
- Fiorillo, A.; Gorwood, P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur. Psychiatry 2020, 63, e32. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/32234102 (accessed on 28 September 2021). [CrossRef] [PubMed] [Green Version]
- Kuzman, M.R.; Curkovic, M.; Wasserman, D. Principles of mental health care during the COVID-19 pandemic. Eur. Psychiatry 2020, 63, e45. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/32431255 (accessed on 28 September 2021). [CrossRef] [PubMed]
- Stewart, D.E.; Appelbaum, P.S. COVID-19 and psychiatrists’ responsibilities: A WPA position paper. World Psychiatry 2020, 19, 406–407. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1002/wps.20803 (accessed on 28 September 2021). [CrossRef]


{kind=link}
| Occupation | Physicians N = 1906 | Nurses and Paramedics N = 1422 | Medical Technicians N = 1727 | Therapist/Educator Occupations N = 1601 | Other N = 886 | Total | |
|---|---|---|---|---|---|---|---|
| Gender | Male | 744 (41.87%) | 379 (21.33%) | 221 (12.44%) | 210 (11.82%) | 223 (12.55%) | 1777 (23.6%) |
| Female | 1157 (20.13%) | 1036 (18.03%) | 1506 (26.21%) | 1388 (24.15%) | 660 (11.48%) | 5747 (76.2%) | |
| Diverse | 5 (27.78%) | 7 (38.88%) | 0 (0.00%) | 3 (16.67%) | 3 (16.67%) | 18 (0.2%) | |
| Age groups | 18–30 | 154 (10.92%) | 441 (31.28%) | 377 (26.74%) | 239 (16.95%) | 199 (14.11%) | 1410 (18.7%) |
| 31–40 | 453 (26.58%) | 342 (20.07%) | 389 (22.83%) | 305 (17.90%) | 215 (12.62%) | 1704 (22.6%) | |
| 41–50 | 466 (26.80%) | 290 (16.68%) | 391 (22.48%) | 410 (23.58%) | 182 (10.47%) | 1739 (23.1%) | |
| 51–60 | 604 (28.04%) | 296 (13.74%) | 489 (22.70%) | 519 (24.09%) | 246 (11.42%) | 2154 (28.6%) | |
| 61–70 | 208 (41.27%) | 50 (9.92%) | 81 (16.07%) | 124 (24.60%) | 41 (8.13%) | 504 (6.7%) | |
| >70 | 21 (67.74%) | 3 (9.68%) | 0 (0.00%) | 4 (12.90%) | 3 (9.68%) | 31 (0.4%) | |
| Contaminated materials/infected individuals | Contact | 956 (26.55%) | 866 (24.05%) | 1285 (35.68%) | 252 (7.00%) | 242 (6.72%) | 3601 (47.7%) |
| No contact | 950 (24.11%) | 556 (14.11%) | 442 (11.22%) | 1349 (34.23%) | 644 (16.34%) | 3941 (52.3%) | |
| Home office | Yes | 467 (28.32%) | 84 (5.09%) | 166 (10.07%) | 609 (36.93%) | 323 (19.59%) | 1649 (21.9%) |
| No | 1439 (24.42%) | 1338 (22.70%) | 1561 (26.49%) | 992 (16.83%) | 563 (9.55%) | 5893 (78.1%) | |
| Caregiving | Yes | 1363 (28.91%) | 770 (16.33%) | 969 (20.56%) | 1083 (22.97%) | 529 (11.22%) | 4714 (62.5%) |
| No | 543 (19.20%) | 652 (23.06%) | 758 (26.80%) | 518 (18.32%) | 357 (12.62%) | 2828 (37.5%) | |
| Migrant background | Yes | 238 (28.88%) | 166 (20.15%) | 166 (20.15%) | 132 (16.02%) | 122 (14.81%) | 824 (10.9%) |
| No | 1667 (24.83%) | 1254 (18.68%) | 1561 (23.25%) | 1468 (21.86%) | 764 (11.38%) | 6714 (89.1%) | |
| Living situation | Living alone | 303 (18.39%) | 380 (23.06%) | 427 (25.91%) | 311 (18.87%) | 227 (13.77%) | 1648 (21.9%) |
| Not living alone | 1603 (27.20%) | 1042 (17.68%) | 1300 (22.06%) | 1290 (21.89%) | 659 (11.18%) | 5894 (78.1%) | |
| Place of work | Clinic | 1039 (21.56%) | 1228 (25.49%) | 1296 (26.90%) | 506 (10.50%) | 749 (15.55%) | 4818 (63.9%) |
| Doctor’s office | 482 (67.70%) | 4 (0.56%) | 173 (24.30%) | 48 (6.74%) | 5 (0.70%) | 712 (9.4%) | |
| Community health center | 46 (19.83%) | 11 (4.74%) | 160 (68.97%) | 5 (2.16%) | 10 (4.31%) | 232 (3.1%) | |
| Other | 321 (18.30%) | 177 (10.09%) | 93 (5.30%) | 1042 (59.41%) | 121 (6.90%) | 1754 (23.3%) | |
| During the First Wave of the Pandemic… | N | M | SD |
|---|---|---|---|
| Problems | |||
| … I was afraid of becoming infected. | 7542 | 2.66 | 1.24 |
| … I was afraid of infecting loved ones or family. | 7542 | 3.27 | 1.34 |
| … I was stressed by the increased workload. | 7542 | 2.52 | 1.24 |
| … I was stressed by changes to my tasks. | 7542 | 2.70 | 1.31 |
| … I was reluctant to go to work. | 7542 | 1.91 | 1.10 |
| … I had problems sleeping. | 7542 | 2.53 | 1.36 |
| … I felt physically or mentally exhausted. | 7542 | 3.06 | 1.30 |
| … I was afraid of having to choose who would receive care and who would not. | 7542 | 1.53 | 0.98 |
| ... I was worried my patients would die without seeing their relatives again. | 7542 | 2.24 | 1.44 |
| ... I felt that patient safety suffered from the higher workload. | 7542 | 2.10 | 1.19 |
| … I smoked more cigarettes. | 7542 | 1.40 | 1.02 |
| … I drank more alcohol. | 7542 | 1.62 | 1.10 |
| … I took more antidepressants/sedatives. | 7542 | 1.14 | 0.59 |
| Protective Factors | |||
| … I felt protected by the actions of national and local authorities. | 7542 | 3.10 | 1.07 |
| … I felt protected as an employee by measures taken by my employer. | 7542 | 3.25 | 1.17 |
| 1 = Strongly Disagree | 2 = Somewhat Disagree | 3 = Partly Agree, Partly Disagree | 4 = Somewhat Agree | 5 = Strongly Agree | |
|---|---|---|---|---|---|
| Fear of infection | 1500 (19.9%) | 2271 (30.1%) | 1820 (24.1%) | 1217 (16.1%) | 734 (9.7%) |
| Infecting others | 956 (12.7%) | 1488 (19.7%) | 1332 (17.7%) | 2062 (27.3%) | 1704 (22.6%) |
| Workload | 1904 (25.2%) | 2219 (29.4%) | 1593 (21.1%) | 1245 (16.5%) | 581 (7.7%) |
| Change in tasks | 1766 (23.4%) | 1885 (25.0%) | 1484 (19.7%) | 1636 (21.6%) | 771 (10.2%) |
| Reluctant to go to work | 3659 (48.5%) | 1978 (26.2%) | 1069 (14.2%) | 604 (8.0%) | 232 (3.1%) |
| Sleep problems | 2441 (32.4%) | 1526 (20.2%) | 1497 (19.8%) | 1326 (17.6%) | 752 (10.0%) |
| Physical or mental exhaustion | 1237 (16.4%) | 1349 (17.9%) | 1747 (23.2%) | 2148 (28.5%) | 1061 (14.1%) |
| Patient care decisions | 5348 (70.9%) | 1119 (14.8%) | 541 (7.2%) | 366 (4.9%) | 168 (2.2%) |
| Patient dies without seeing relatives again | 3626 (48.1%) | 1142 (15.1%) | 923 (12.2%) | 1008 (13.4%) | 843 (11.2%) |
| Patient safety | 3131 (41.5%) | 2015 (26.7%) | 1245 (16.5%) | 795 (10.5%) | 356 (4.7%) |
| Nicotine consumption | 6370 (84.5%) | 260 (3.4%) | 264 (3.5%) | 371 (4.9%) | 277 (3.7%) |
| Alcohol consumption | 5310 (70.4%) | 727 (9.6%) | 726 (9.6%) | 582 (7.7%) | 197 (2.6%) |
| Antidepressant use | 7035 (93.3%) | 190 (2.5%) | 150 (2.0%) | 104 (1.4%) | 63 (0.8%) |
| Protection by authorities | 690 (9.1%) | 1395 (18.5%) | 2453 (32.5%) | 2474 (32.8%) | 530 (7.0%) |
| Protection by employer | 685 (9.1%) | 1339 (17.8%) | 2017 (26.7%) | 2403 (31.9%) | 1098 (14.6%) |
| Problems and Protective Factors Associated with COVID-19 | Testing Statistics of the Analysis of Variance |
|---|---|
| Fear of infection | F(4, 7537) = 25.73, p < 0.001, η² = 0.01 |
| Infecting others | F(4, 7537) = 51.78, p < 0.001, η² = 0.03 |
| Workload | F(4, 7537) = 9.98, p < 0.001, η² = 0.01 |
| Change in tasks | F(4, 7537) = 35.16, p < 0.001, η² = 0.02 |
| Reluctant to go to work | F(4, 7537) = 28.59, p < 0.001, η² = 0.02 |
| Sleep problems | F(4, 7537) = 16.22, p < 0.001, η² = 0.01 |
| Physical or mental exhaustion | F(4, 7537) = 14.72, p < 0.001, η² = 0.01 |
| Patient care decisions | F(4, 7537) = 62.91, p < 0.001, η² = 0.03 |
| Patient dies without saying goodbye | F(4, 7537) = 101.79, p < 0.001, η² = 0.05 |
| Patient safety | F(4, 7537) = 66.63, p < 0.001, η² = 0.03 |
| Nicotine consumption | F(4, 7537) = 65.19, p < 0.001, η² = 0.03 |
| Alcohol consumption | F(4, 7537) = 9.44, p < 0.001, η² = 0.01 |
| Antidepressant use | F(4, 7537) = 8.50, p < 0.001, η² = 0.01 |
| Protection by authorities | F(4, 7537) = 43.62, p < 0.001, η² = 0.02 |
| Protection by employer | F(4, 7537) = 23.98, p < 0.001, η² = 0.01 |
| Infecting Others | Patient Dies without Seeing Relatives again | Patient Safety | Alcohol Consumption | Protection by Authorities | Protection by Employer | |
|---|---|---|---|---|---|---|
| Test statistics | F(5, 7561) = 36.90, p < 0.001, η² = 0.02 | F(5, 7561) = 5.12, p < 0.001, η² = 0.003 | F(5, 7561) = 18.79, p < 0.001, η² = 0.01 | F(5, 7561) = 10.18, p < 0.001, η² = 0.01 | F(5, 7561) = 8.41, p < 0.001, η² = 0.01 | F(5, 7561) = 5.66, p < 0.001, η² = 0.004 |
| 18–30 (N = 1411) | 3.59 (1.29) | 2.40 (1.46) | 2.33 (1.27) | 1.71 (1.17) | 2.96 (1.04) | 3.13 (1.12) |
| 31–40 (N = 1706) | 3.43 (1.31) | 2.27 (1.45) | 2.16 (1.22) | 1.73 (1.18) | 3.07 (1.06) | 3.21 (1.15) |
| 41–50 (N = 1745) | 3.20 (1.35) | 2.15 (1.43) | 2.05 (1.16) | 1.62 (1.09) | 3.15 (1.05) | 3.29 (1.17) |
| 51–60 (N = 2161) | 3.08 (1.35) | 2.21 (1.43) | 1.98 (1.14) | 1.53 (1.00) | 3.17 (1.10) | 3.31 (1.21) |
| 61–70 (N = 507) | 2.99 (1.33) | 2.23 (1.49) | 1.96 (1.09) | 1.46 (0.92) | 3.14 (1.14) | 3.31 (1.27) |
| >70 (N = 32) | 2.53 (1.48) | 2.16 (1.54) | 1.72 (1.02) | 1.50 (1.19) | 2.97 (1.33) | 2.88 (1.56) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jerg-Bretzke, L.; Kempf, M.; Jarczok, M.N.; Weimer, K.; Hirning, C.; Gündel, H.; Erim, Y.; Morawa, E.; Geiser, F.; Hiebel, N.; et al. Psychosocial Impact of the COVID-19 Pandemic on Healthcare Workers and Initial Areas of Action for Intervention and Prevention—The egePan/VOICE Study. Int. J. Environ. Res. Public Health 2021, 18, 10531. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910531
Jerg-Bretzke L, Kempf M, Jarczok MN, Weimer K, Hirning C, Gündel H, Erim Y, Morawa E, Geiser F, Hiebel N, et al. Psychosocial Impact of the COVID-19 Pandemic on Healthcare Workers and Initial Areas of Action for Intervention and Prevention—The egePan/VOICE Study. International Journal of Environmental Research and Public Health. 2021; 18(19):10531. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910531
Chicago/Turabian StyleJerg-Bretzke, Lucia, Maximilian Kempf, Marc Nicolas Jarczok, Katja Weimer, Christian Hirning, Harald Gündel, Yesim Erim, Eva Morawa, Franziska Geiser, Nina Hiebel, and et al. 2021. "Psychosocial Impact of the COVID-19 Pandemic on Healthcare Workers and Initial Areas of Action for Intervention and Prevention—The egePan/VOICE Study" International Journal of Environmental Research and Public Health 18, no. 19: 10531. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910531