
eHealth Interventions to Treat Substance Use in Pregnancy: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Data Analysis
2.5. Quality Assessment
2.6. Primary Outcome
3. Results
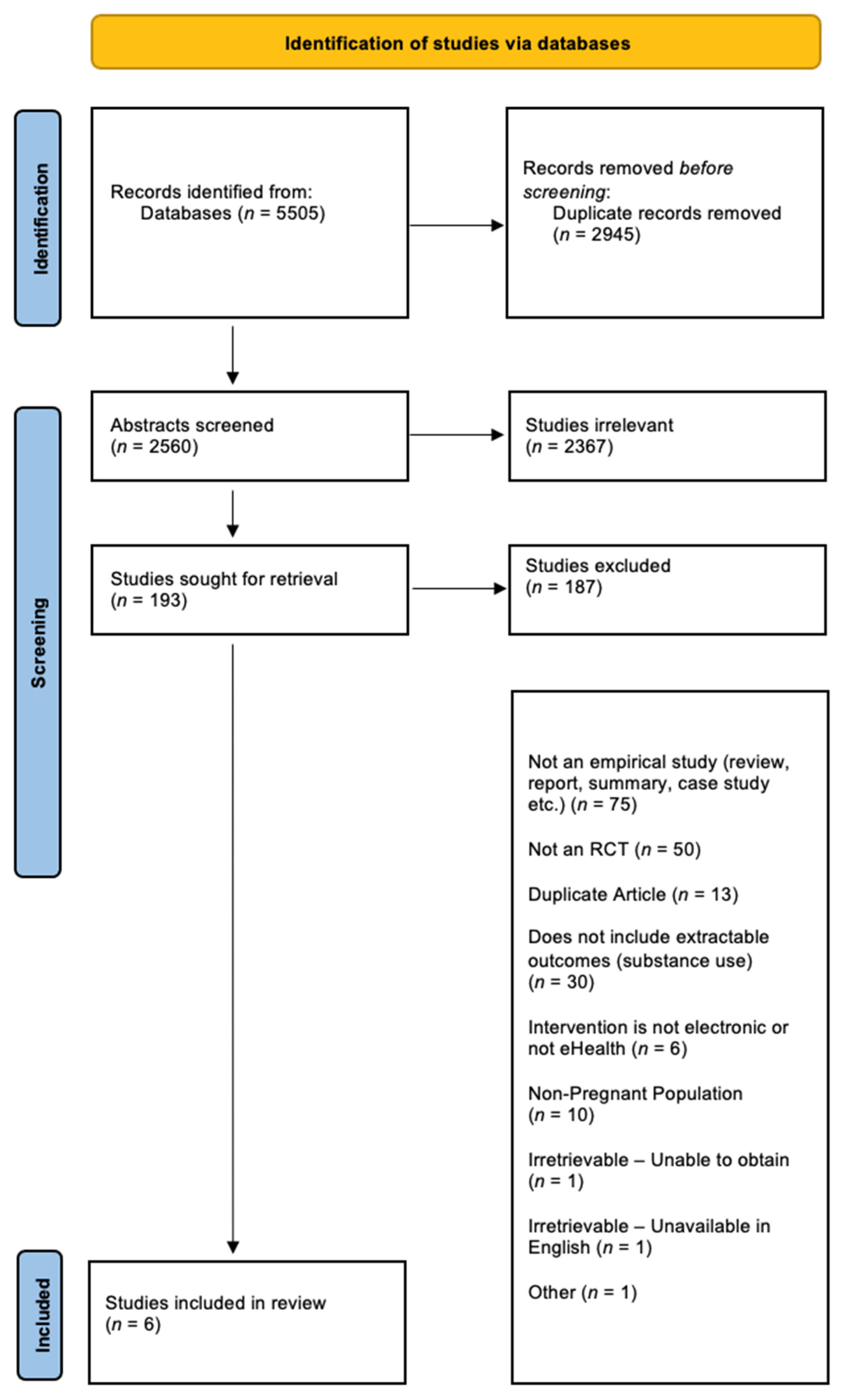
3.1. Study Selection
3.2. Characteristics of Included Studies
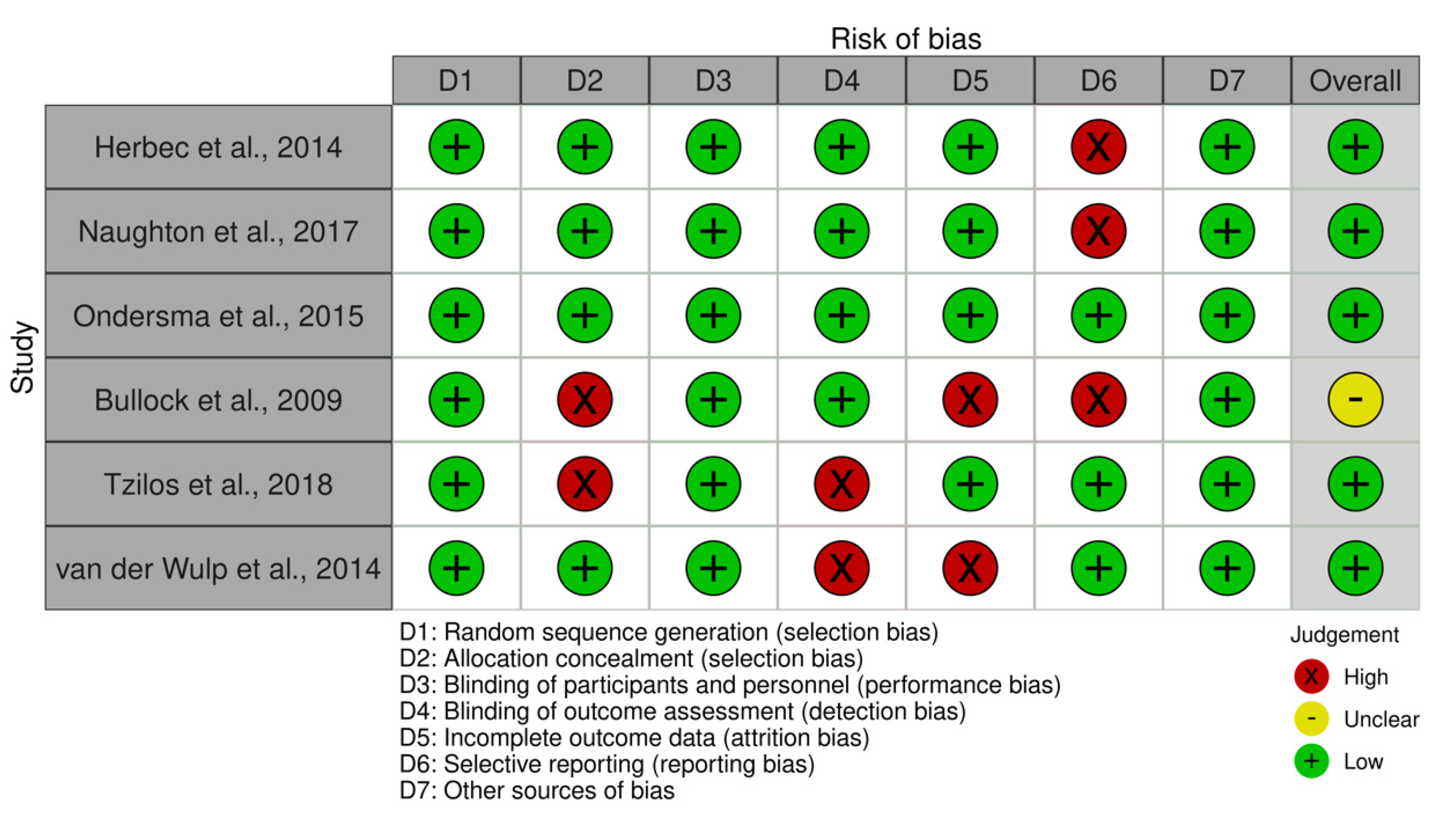
3.3. Risk of Bias in Included Studies RCTs
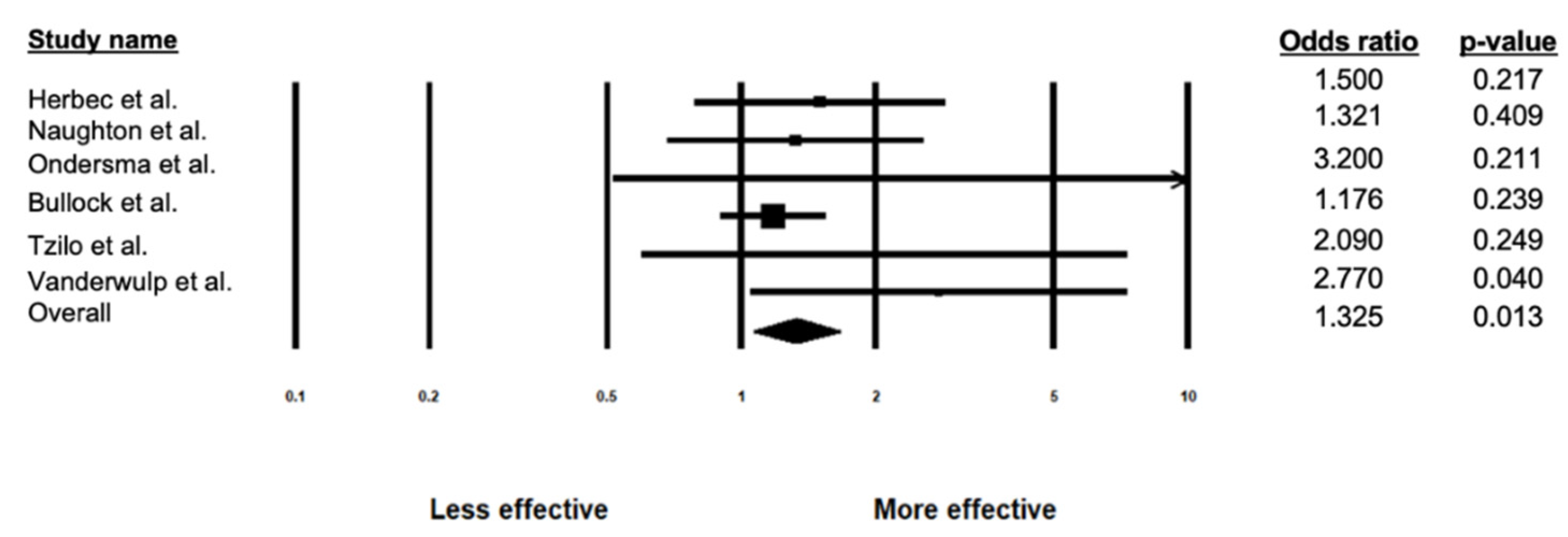
3.4. Efficacy of eHealth Interventions on Substance Use
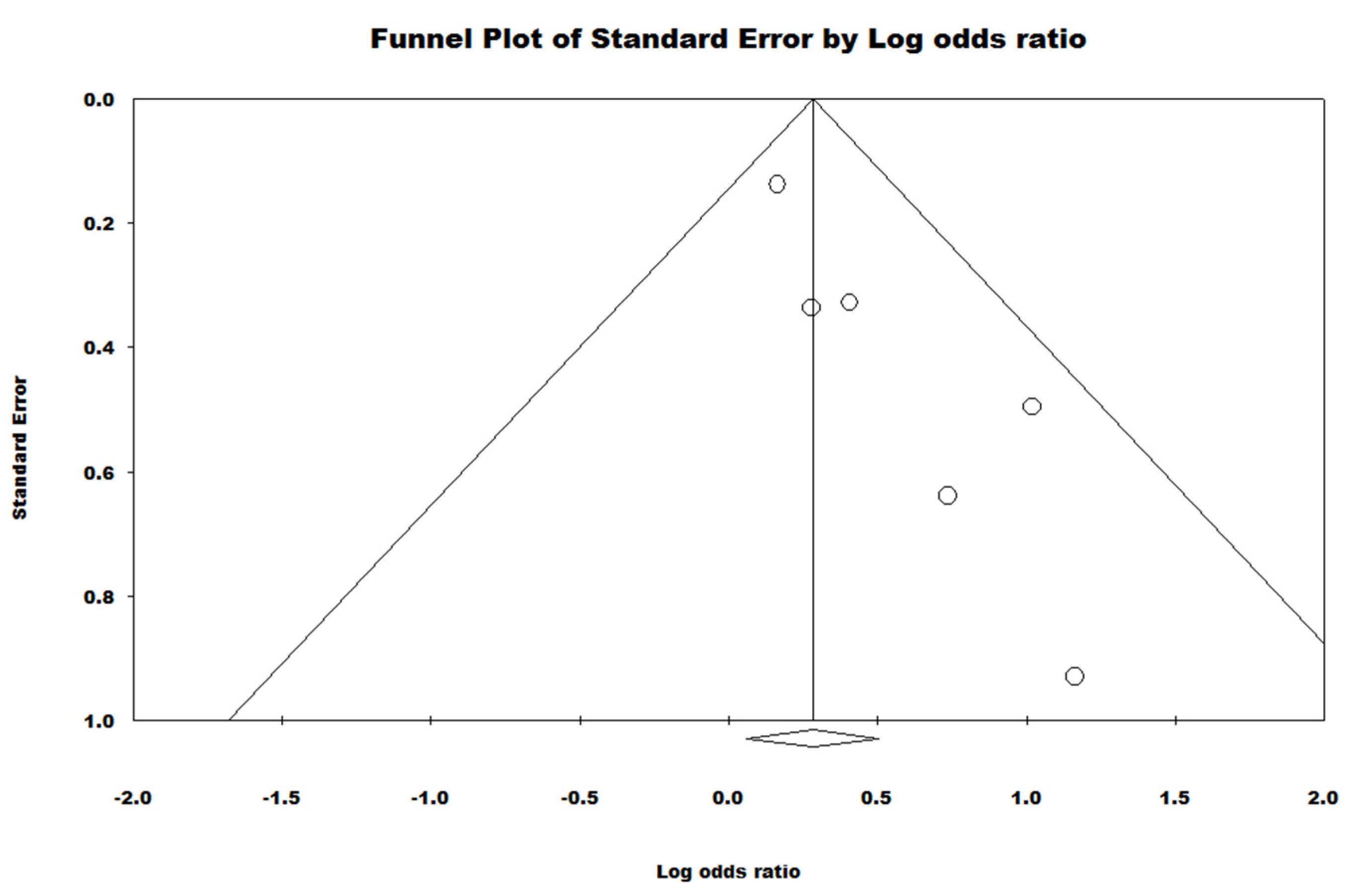
3.5. Sensitivity Analysis
4. Discussion
4.1. Primary Findings
4.2. Consistency with Existing Literature
4.3. Obstacles to eHealth Interventions
4.4. Strengths, Limitations and Future Directions
4.5. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| eHealth/Telepsychology | And | Study Design | And | Mental Health and Substance Use | And | Pregnancy |
|---|---|---|---|---|---|---|
| eHealth/e-Health | RCT | Substance Use | pregnant | |||
| internet | efficacy | externalizing | perinatal/peri-natal | |||
| online/on-line | random allocation | substance-related disorder/substance related disorder | prepartum/pre-partum | |||
| app/apps | effectiveness | substance abuse/ substance-abuse | antenatal/ante-natal | |||
| web-based/web based | randomized controlled trial | substance dependence/substance-dependence | birth | |||
| smart-phone/smartphone/smart phone | trial | addiction | childbirth/child-birth | |||
| mobile phone/mobile-phone | controlled clinical trial | drug abuse/drug-abuse | labor | |||
| mobile health | clinical trial | drug dependence/ drug-dependence | labour | |||
| mHealth | alcohol abuse/alcohol-abuse | gestation | ||||
| app-based | alcohol dependence/alcohol-dependence | |||||
| computer systems | alcoholism/alcoholic | |||||
| computers | ||||||
| cell phone/cell-phone/cellphone | ||||||
| website | ||||||
| computer | ||||||
| social media | ||||||
| web-based/web based | ||||||
| SMS | ||||||
| mobile | ||||||
| text-based/text based | ||||||
| digital | ||||||
| self-directed/self directed | ||||||
| technology-assisted/technology assisted | ||||||
| self-help/self help | ||||||
| self-guided/self guided | ||||||
| telecommunications/telecommunication |
References
- Whiteford, H.A.; Ferrari, A.J.; Degenhardt, L.; Feigin, V.; Vos, T. The global burden of mental, neurological and substance use disorders: An analysis from the Global Burden of Disease Study 2010. PLoS ONE 2015, 10, e0116820. [Google Scholar] [CrossRef] [Green Version]
- Compton, W.M.; Thomas, Y.F.; Stinson, F.S.; Grant, B.F. Prevalence, correlates, disability, and comorbidity of DSM-IV drug abuse and dependence in the United States: Results from the national epidemiologic survey on alcohol and related conditions. Arch. Gen. Psychiatry 2007, 64, 566–576. [Google Scholar] [CrossRef] [Green Version]
- Results from the 2010 National Survey on Drug Use and Health: Summary of National Finding. Available online: www.samhsa.gov/data/sites/default/files/NSDUHresults2010/NSDUHresults2010.htm (accessed on 10 September 2021).
- Chasnoff, I.J.; McGourty, R.F.; Bailey, G.W.; Hutchins, E.; Lightfoot, S.O.; Pawson, L.L.; Fahey, C.; May, B.; Brodie, P.; McCulley, L. The 4P’s Plus© screen for substance use in pregnancy: Clinical application and outcomes. J. Perinatol. 2005, 25, 368–374. [Google Scholar] [CrossRef] [Green Version]
- Havens, J.R.; Simmons, L.A.; Shannon, L.M.; Hansen, W.F. Factors associated with substance use during pregnancy: Results from a national sample. Drug Alcohol Depend. 2009, 99, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Garg, M.; Garrison, L.; Leeman, L.; Hamidovic, A.; Borrego, M.; Rayburn, W.F.; Bakhireva, L. Validity of self-reported drug use information among pregnant women. Matern. Child Health J. 2016, 20, 41–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avalos, L.A.; Roberts, S.C.; Kaskutas, L.A.; Block, G.; Li, D.-K. Volume and type of alcohol during early pregnancy and the risk of miscarriage. Subst. Use Misuse 2014, 49, 1437–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, S.; Dodd, S.; Walkinshaw, S.; Siney, C.; Kakkar, P.; Mousa, H. Substance abuse during pregnancy: Effect on pregnancy outcomes. Eur. J. Obstet. Gynecol. Reprod. Biol. 2010, 150, 137–141. [Google Scholar] [CrossRef]
- O’Leary, C.M.; Jacoby, P.J.; Bartu, A.; D’Antoine, H.; Bower, C. Maternal alcohol use and sudden infant death syndrome and infant mortality excluding SIDS. Pediatrics 2013, 131, e770–e778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, K.; Greenough, A. Sudden infant death syndrome (SIDS), substance misuse, and smoking in pregnancy. Res. Rep. Neonatol. 2012, 2, 95–101. [Google Scholar]
- Forray, A. Substance use during pregnancy. F1000Research 2016, 5, 887. [Google Scholar] [CrossRef] [PubMed]
- Warner, T.D.; Roussos-Ross, D.; Behnke, M. It’s not your mother’s marijuana: Effects on maternal-fetal health and the developing child. Clin. Perinatol. 2014, 41, 877–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, C.R.; Roane, J.; Hewitt, A.; Muhajarine, N.; Mushquash, C.; Sourander, A.; Lingley-Pottie, P.; McGrath, P.; Reynolds, J.N. Frequent behavioural challenges in children with fetal alcohol spectrum disorder: A needs-based assessment reported by caregivers and clinicians. J. Popul. Ther. Clin. Pharmacol. 2014, 21, 21. [Google Scholar]
- Fuglestad, A.J.; Whitley, M.L.; Carlson, S.M.; Boys, C.J.; Eckerle, J.K.; Fink, B.A.; Wozniak, J.R. Executive functioning deficits in preschool children with Fetal Alcohol Spectrum Disorders. Child Neuropsychol. 2015, 21, 716–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rangmar, J.; Hjern, A.; Vinnerljung, B.; Strömland, K.; Aronson, M.; Fahlke, C. Psychosocial outcomes of fetal alcohol syndrome in adulthood. Pediatrics 2015, 135, e52–e58. [Google Scholar] [CrossRef] [PubMed]
- Saloner, B.; Karthikeyan, S. Changes in substance abuse treatment use among individuals with opioid use disorders in the United States, 2004–2013. JAMA 2015, 314, 1515–1517. [Google Scholar] [CrossRef] [PubMed]
- Substance Abuse and Mental Health Services Administration. 2017 National Survey on Drug Use and Health: Detailed Tables; Substance Abuse and Mental Health Services Administration Rockville: Rockville, MD, USA, 2018. [Google Scholar]
- Xu, J.; Rapp, R.C.; Wang, J.; Carlson, R.G. The multidimensional structure of external barriers to substance abuse treatment and its invariance across gender, ethnicity, and age. Subst. Abus. 2008, 29, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Substance Abuse and Mental Health Services Administration. National Survey on Drug Use and Health; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2014. [Google Scholar]
- Stone, R. Pregnant women and substance use: Fear, stigma, and barriers to care. Health Justice 2015, 3, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Frazer, Z.; McConnell, L.M. Treatment for substance use disorders in pregnant women: Motivators and barriers. Drug Alcohol Depend. 2019, 205, 107652. [Google Scholar] [CrossRef]
- World Health Organization. mHealth: New Horizons for Health through Mobile Technologies; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Ondersma, S.J.; Walters, S.T. Clinician’s Guide to Evaluating and Developing eHealth Interventions for Mental Health. Psychiatr. Res. Clin. Pract. 2020, 2, 26–33. [Google Scholar] [CrossRef]
- Smit, F.; Lokkerbol, J.; Riper, H.; Majo, C.; Boon, B.; Blankers, M. Modeling the cost-effectiveness of health care systems for alcohol use disorders: How implementation of eHealth interventions improves cost-effectiveness. J. Med. Internet Res. 2011, 13, e56. [Google Scholar] [CrossRef]
- Friedrichs, A.; Spies, M.; Härter, M.; Buchholz, A. Patient preferences and shared decision making in the treatment of substance use disorders: A systematic review of the literature. PLoS ONE 2016, 11, e0145817. [Google Scholar] [CrossRef] [PubMed]
- Marchand, K.; Beaumont, S.; Westfall, J.; MacDonald, S.; Harrison, S.; Marsh, D.C.; Schechter, M.T.; Oviedo-Joekes, E. Conceptualizing patient-centered care for substance use disorder treatment: Findings from a systematic scoping review. Subst. Abus. Treat. Prev. Policy 2019, 14, 37. [Google Scholar] [CrossRef]
- Boumparis, N.; Karyotaki, E.; Schaub, M.P.; Cuijpers, P.; Riper, H. Internet interventions for adult illicit substance users: A meta-analysis. Addiction 2017, 112, 1521–1532. [Google Scholar] [CrossRef]
- Dutra, L.; Stathopoulou, G.; Basden, S.L.; Leyro, T.M.; Powers, M.B.; Otto, M.W. A meta-analytic review of psychosocial interventions for substance use disorders. Am. J. Psychiatry 2008, 165, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada. Your Guide to a Healthy Pregnancy. Available online: https://www.canada.ca/en/public-health/services/health-promotion/healthy-pregnancy/healthy-pregnancy-guide.html (accessed on 2 June 2021).
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Covidence Systematic Review Software. Available online: www.covidence.org (accessed on 15 July 2021).
- Veritas Health Innovation. Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia, 2017. [Google Scholar]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Meta-Analysis; Version 3 Biostat: Englewood, NJ, USA, 2013. [Google Scholar]
- Bullock, L.; Everett, K.D.; Mullen, P.D.; Geden, E.; Longo, D.R.; Madsen, R. Baby BEEP: A randomized controlled trial of nurses’ individualized social support for poor rural pregnant smokers. Matern. Child Health J. 2009, 13, 395–406. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Silang, K.A.; Sohal, P.R.; Bright, K.; Leason, J.; Roos, L.; Lebel, G.G.; Tomfohr-Madsen, L.M. eHealth Interventions for Treatment and Prevention of Depression, Anxiety and Insomnia during Pregnancy: A Systematic Review and Meta-Analysis. J. Med. Internet Res. submitted for publication.
- Naughton, F.; Cooper, S.; Foster, K.; Emery, J.; Leonardi-Bee, J.; Sutton, S.; Jones, M.; Ussher, M.; Whitemore, R.; Leighton, M. Large multi-centre pilot randomized controlled trial testing a low-cost, tailored, self-help smoking cessation text message intervention for pregnant smokers (MiQuit). Addiction 2017, 112, 1238–1249. [Google Scholar] [CrossRef] [PubMed]
- Herbec, A.; Brown, J.; Tombor, I.; Michie, S.; West, R. Pilot randomized controlled trial of an internet-based smoking cessation intervention for pregnant smokers (‘MumsQuit’). Drug Alcohol Depend. 2014, 140, 130–136. [Google Scholar] [CrossRef] [Green Version]
- Ondersma, S.J.; Beatty, J.R.; Svikis, D.S.; Strickler, R.C.; Tzilos, G.K.; Chang, G.; Divine, G.W.; Taylor, A.R.; Sokol, R.J. Computer-delivered screening and brief intervention for alcohol use in pregnancy: A pilot randomized trial. Alcohol. Clin. Exp. Res. 2015, 39, 1219–1226. [Google Scholar] [CrossRef] [Green Version]
- Wernette, G.T.; Plegue, M.; Kahler, C.W.; Sen, A.; Zlotnick, C. A pilot randomized controlled trial of a computer-delivered brief intervention for substance use and risky sex during pregnancy. J. Women’s Health 2018, 27, 83–92. [Google Scholar] [CrossRef]
- van der Wulp, N.Y.; Hoving, C.; Eijmael, K.; Candel, M.J.; van Dalen, W.; De Vries, H. Reducing alcohol use during pregnancy via health counseling by midwives and internet-based computer-tailored feedback: A cluster randomized trial. J. Med. Internet Res. 2014, 16, e274. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Egger, M. Regression methods to detect publication and other bias in meta-analysis. Publ. Bias Meta-Anal. Prev. Assess. Adjust. 2005, 99, 110. [Google Scholar]
- Qureshi, Q.A.; Shah, B.; Kundi, G.M.; Nawaz, A.; Miankhel, A.K.; Chishti, K.A.; Qureshi, N.A. Infrastructural barriers to e-health implementation in developing countries. Eur. J. Sustain. Dev. 2013, 2, 163. [Google Scholar]
- Eggertson, L. Stigma a major barrier to treatment for pregnant women with addictions. Can. Med. Assoc. 2013, 185, 1562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geraghty, A.W.; Torres, L.D.; Leykin, Y.; Pérez-Stable, E.J.; Muñoz, R.F. Understanding attrition from international internet health interventions: A step towards global eHealth. Health Promot. Int. 2013, 28, 442–452. [Google Scholar] [CrossRef] [Green Version]
- Riper, H.; Spek, V.; Boon, B.; Conijn, B.; Kramer, J.; Martin-Abello, K.; Smit, F. Effectiveness of E-self-help interventions for curbing adult problem drinking: A meta-analysis. J. Med. Internet Res. 2011, 13, e42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hai, A.H.; Hammock, K.; Velasquez, M.M. The efficacy of technology-based interventions for alcohol and illicit drug use among women of childbearing age: A systematic review and meta-analysis. Alcohol. Clin. Exp. Res. 2019, 43, 2464–2479. [Google Scholar] [CrossRef]
- Jensen, C.D.; Cushing, C.C.; Aylward, B.S.; Craig, J.T.; Sorell, D.M.; Steele, R.G. Effectiveness of motivational interviewing interventions for adolescent substance use behavior change: A meta-analytic review. J. Consult. Clin. Psychol. 2011, 79, 433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Licciardone, J.C.; Pandya, V. Feasibility Trial of an eHealth Intervention for Health-Related Quality of Life: Implications for Managing Patients with Chronic Pain during the COVID-19 Pandemic. Healthcare 2020, 8, 381. [Google Scholar] [CrossRef] [PubMed]
- Milward, J.; Drummond, C.; Fincham-Campbell, S.; Deluca, P. What makes online substance-use interventions engaging? A systematic review and narrative synthesis. Digit. Health 2018, 4, 2055207617743354. [Google Scholar] [CrossRef]
- Taylor, G.M.; Dalili, M.N.; Semwal, M.; Civljak, M.; Sheikh, A.; Car, J. Internet-based interventions for smoking cessation. Cochrane Database Syst. Rev. 2017, 2017, CD007078. [Google Scholar] [CrossRef] [Green Version]
- Magill, M.; Ray, L.A. Cognitive-behavioral treatment with adult alcohol and illicit drug users: A meta-analysis of randomized controlled trials. J. Stud. Alcohol Drugs 2009, 70, 516–527. [Google Scholar] [CrossRef] [Green Version]
- Cournoyer, L.G.; Brochu, S.; Landry, M.; Bergeron, J. Therapeutic alliance, patient behaviour and dropout in a drug rehabilitation programme: The moderating effect of clinical subpopulations. Addiction 2007, 102, 1960–1970. [Google Scholar] [CrossRef]
- de Paiva Azevedo, J.; Delaney, H.; Epperson, M.; Jbeili, C.; Jensen, S.; McGrail, C.; Weaver, H.; Baglione, A.; Barnes, L.E. Gamification of ehealth interventions to increase user engagement and reduce attrition. In Proceedings of the 2019 Systems and Information Engineering Design Symposium (SIEDS), Charlottesville, VA, USA, 26 April 2019; pp. 1–5. [Google Scholar]
- Eysenbach, G.; Group, C.-E. CONSORT-EHEALTH: Improving and standardizing evaluation reports of Web-based and mobile health interventions. J. Med. Internet Res. 2011, 13, e126. [Google Scholar] [CrossRef]
- Lai, H.M.X.; Cleary, M.; Sitharthan, T.; Hunt, G.E. Prevalence of comorbid substance use, anxiety and mood disorders in epidemiological surveys, 1990–2014: A systematic review and meta-analysis. Drug Alcohol Depend. 2015, 154, 1–13. [Google Scholar] [CrossRef]
- Cerullo, M.A.; Strakowski, S.M. The prevalence and significance of substance use disorders in bipolar type I and II disorder. Subst. Abus. Treat. Prev. Policy 2007, 2, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Emmerik-van Oortmerssen, K.; van de Glind, G.; van den Brink, W.; Smit, F.; Crunelle, C.L.; Swets, M.; Schoevers, R.A. Prevalence of attention-deficit hyperactivity disorder in substance use disorder patients: A meta-analysis and meta-regression analysis. Drug Alcohol Depend. 2012, 122, 11–19. [Google Scholar] [CrossRef]
- Wu, L.-T.; Zhu, H.; Ghitza, U.E. Multicomorbidity of chronic diseases and substance use disorders and their association with hospitalization: Results from electronic health records data. Drug Alcohol Depend. 2018, 192, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Rioux, C.; Huet, A.-S.; Castellanos-Ryan, N.; Fortier, L.; Le Blanc, M.; Hamaoui, S.; Geoffroy, M.-C.; Renaud, J.; Séguin, J.R. Substance use disorders and suicidality in youth: A systematic review and meta-analysis with a focus on the direction of the association. PLoS ONE 2021, 16, e0255799. [Google Scholar] [CrossRef] [PubMed]
- Grella, C.E.; Stein, J.A. Impact of program services on treatment outcomes of patients with comorbid mental and substance use disorders. Psychiatr. Serv. 2006, 57, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines for Identification and Management of Substance Use and Substance Use Disorders in Pregnancy; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Shidhaye, R.; Lund, C.; Chisholm, D. Closing the treatment gap for mental, neurological and substance use disorders by strengthening existing health care platforms: Strategies for delivery and integration of evidence-based interventions. Int. J. Ment. Health Syst. 2015, 9, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scogin, F.R.; Hanson, A.; Welsh, D. Self-administered treatment in stepped-care models of depression treatment. J. Clin. Psychol. 2003, 59, 341–349. [Google Scholar] [CrossRef]
- National Institute for Health and Clinical Excellence. Descriptions of Services for Pregnant Women with Complex Social Factors. Available online: https://www.nice.org.uk/guidance/cg110/resources/service-descriptions-pdf-136153837 (accessed on 1 September 2021).
- Downs, R. UN: Majority of World’s Population Lacks Internet Access. Available online: https://www.upi.com/Top_News/World-News/2017/09/18/UN-Majority-of-worlds-population-lacks-internet-access/6571505782626/ (accessed on 3 June 2021).
- Canadian Radio-television and Telecommunications Commission. Communication Monitoring Report; Canadian Radio-television and Telecommunications Commission: Ottawa, Canada, 2018; pp. 138–143. [Google Scholar]
- Alvarez-Risco, A.; Del-Aguila-Arcentales, S.; Yáñez, J.A. Telemedicine in Peru as a result of the COVID-19 pandemic: Perspective from a country with limited internet access. Am. J. Trop. Med. Hyg. 2021, 105, 6. [Google Scholar]
- Roberts, E.T.; Mehrotra, A. Assessment of disparities in digital access among Medicare beneficiaries and implications for telemedicine. JAMA Intern. Med. 2020, 180, 1386–1389. [Google Scholar] [CrossRef]
- Baumeister, H.; Reichler, L.; Munzinger, M.; Lin, J. The impact of guidance on Internet-based mental health interventions—A systematic review. Internet Interv. 2014, 1, 205–215. [Google Scholar] [CrossRef] [Green Version]




| References | Title | Year | Country | Intervention (N); Control (N) | Intervention, Age of Sample (M, SD), Range (y) | Control, Age of Sample (M, SD), Range (y) | Intervention, Gestational Age (M, SD), Range (w) Control, Gestational Age (M, SD), Range (w) | Type of eHealth Intervention | Description of Intervention | Time of Follow Up |
|---|---|---|---|---|---|---|---|---|---|---|
| Bullock, L., et al. [36] | Baby BEEP: A Randomized Controlled Trial of Nurses’ Individualized Social Support for Poor Rural Pregnant Smokers | 2009 | United States | Telephone Social Support Group and Booklet Group (117), Control (119) | Telephone Social Support Group and Booklet Group (23.1, 4.3) Telephone Social Support Only Group (24.0, 4.7) Booklet Only Group (23.6, 4.8) | Control (23.9, 4.8) | 13.5 weeks 13.5 weeks | Telephone Intervention | Baby BEEP intervention consisted of a scheduled weekly telephone call and 24-h access to the nurse for any additional social support needed | T2 (28–32 weeks gestation; T3: 6 weeks postpartum) |
| Naughton, F. [41] | Large multi-centre pilot randomized controlled trialtesting a low-cost, tailored, self-help smoking cessationtext message intervention for pregnant smokers (MiQuit) | 2017 | England | 203 204 | 26.6 (5.7), 16.9–40.0 | 26.4 (5.7), 16.6–41.3 | 14.6 weeks (4.2), 4–23 14.7 weeks (4.5), 3–24 | Text Message Based Intervention | MiQuit is an automated text support service that delivers information or motivational messages | 4 weeks post-randomization up until 36 weeks gestation |
| Herbec, A., et al. [42] | Pilot randomized controlled trial of an internet-based smoking cessation intervention for pregnant smokers (‘MumsQuit’) | 2014 | England | 99 101 | 27.6 (6.0) | 26.1 (5.8) | NR | Internet-Based Intervention | MumsQuit is a personalized, interactive quitting plan that mimics advisory support from a smoking cessation expert | 8 weeks post baseline |
| Ondersma, S. J., et al. [43] | Computer-Delivered Screening and Brief Intervention for Alcohol Use in Pregnancy: A Pilot Randomized Trail | 2015 | United States | 24 24 | 18–25 (50.0%) 26–33 (33.3%) 34–37 (16.7%) | 18–25 (58.3%) 26–33 (33.3%) 34–37 (8.3%) | 12.5 weeks (5.6) 12.0 weeks (5.3) | Computer-delivered screening and brief intervention (eSBI) | A brief 20-min video was delivered via tablet while waiting for a prenatal care appointment and three separated tailored mailings followed | 3 month follow up |
| Tzilos, Wernette. G., et al. [44] | A Pilot Randomized Controlled Trial of a Computer-Delivered Brief Intervention for Substance Use and Risky Sex During Pregnancy | 2018 | United States | 31 19 | 25.1 (5.79) | 23.2 (4.21) | 12.9 (4.76) 13.9 (4.21) | Computer Delivered Intervention | A single motivational session and a booster session | 4 month follow up |
| van de Wulp, N., et al. [45] | Reducing Alcohol Use During Pregnancy Via Health Counseling by Midwives and Internet-Based Computer-Tailored Feedback: A Cluster Randomized Trial | 2014 | Netherlands | Computer tailoring (111); Usual care (124) | 32.31 (4.22) | 33.53; (3.85) | 7.73 weeks (2.06) 7.92 weeks (1.99) | Computer delivered intervention | Respondents in the computer-tailoring group received usual care from their midwife and computer-tailored feedback via the Internet. This feedback was tailored to the participant’s alcohol use, knowledge, risk perception, attitude, social influence, self-efficacy, intention, and action and coping plans | 6 months after baseline |
| References | Title | Year | Type of Substance | Measurement used for Assessment | Intervention Effect on Substance Use | Odds Ratio | Confidence Interval | p-Value | Quality Assessment Rating |
|---|---|---|---|---|---|---|---|---|---|
| Bullock, L., et al. [36] | Baby BEEP: A Randomized Controlled Trial of Nurses’ Individualized Social Support for Poor Rural Pregnant Smokers | 2009 | Smoking | Readiness to Stop Smoking, The Fagerstrom Test for Nicotine Dependence and Dosage (cotinine < 30ng/mL) | The nurse-delivered social support telephone intervention was not more effective than booklets alone or usual care in reducing smoking behaviour. | 1.18 | 0.90–1.54 | 0.239 | 3 |
| Naughton, F. [41] | Large multi-centre pilot randomized controlled trial testing a low-cost, tailored, self-help smoking cessation text message intervention for pregnant smokers (MiQuit) | 2017 | Smoking | Validated 4-week continuous abstinence (CO readings < 9ppm), Self-reported 4-week continuous abstinence, 7-day point prevalence for 4-weeks continuous abstinence | No statistical significance was found between the MiQuit intervention group and the usual care control group. | 1.32 | 0.68–2.56 | 0.409 | 1 |
| Herbec, A., et al. [42] | Pilot randomized controlled trial of an internet-based smoking cessation intervention for pregnant smokers (‘MumsQuit’) | 2014 | Smoking | Self-reported 4-week continuous abstinence | The analysis determined no significant difference when measuring continuous abstinence rates between the MumsQuit intervention and control group. | 1.50 | 0.79–2.86 | 0.217 | 1 |
| Ondersma, S. J., et al. [43] | Computer-Delivered Screening and Brief Intervention for Alcohol Use in Pregnancy: A Pilot Randomized Trail | 2015 | Alcohol Use | Self-reported 90-day abstinence period | No statistical significance was found between the intervention group and the control group when comparing abstinence. | 3.20 | 0.52–19.78 | 0.211 | 0 |
| Tzilos, Wernette. G., et al. [44] | A Pilot Randomized Controlled Trial of a Computer-Delivered Brief Intervention for Substance Use and Risky Sex During Pregnancy | 2018 | General substance use | Self-reported substance use behaviours using a calendar and multiple prompts | The final analysis determined no significant reduction of substance use in the intervention group compared to the control group. | 2.06 | 0.59–7.31 | 0.249 | 2 |
| van de Wulp, N., et al. [45] | Reducing Alcohol Use During Pregnancy Via Health Counseling by Midwives and Internet-Based Computer-Tailored Feedback: A Cluster Randomized Trial | 2014 | Alcohol | Average alcohol consumption during pregnancy was assessed with the 5-item Dutch Quantity-Frequency-Variability (QFV) Questionnaire | The final analysis showed that computer-tailoring respondents used alcohol significantly less often when compared to usual care respondents. | 2.77 | 1.05–7.32 | 0.040 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silang, K.; Sanguino, H.; Sohal, P.R.; Rioux, C.; Kim, H.S.; Tomfohr-Madsen, L.M. eHealth Interventions to Treat Substance Use in Pregnancy: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 9952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18199952
Silang K, Sanguino H, Sohal PR, Rioux C, Kim HS, Tomfohr-Madsen LM. eHealth Interventions to Treat Substance Use in Pregnancy: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(19):9952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18199952
Chicago/Turabian StyleSilang, Katherine, Hangsel Sanguino, Pooja R. Sohal, Charlie Rioux, Hyoun S. Kim, and Lianne M. Tomfohr-Madsen. 2021. "eHealth Interventions to Treat Substance Use in Pregnancy: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 19: 9952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18199952