Effects of Hurricane Michael on Access to Care for Pregnant Women and Associated Pregnancy Outcomes

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Data Source
2.2. Affected Areas
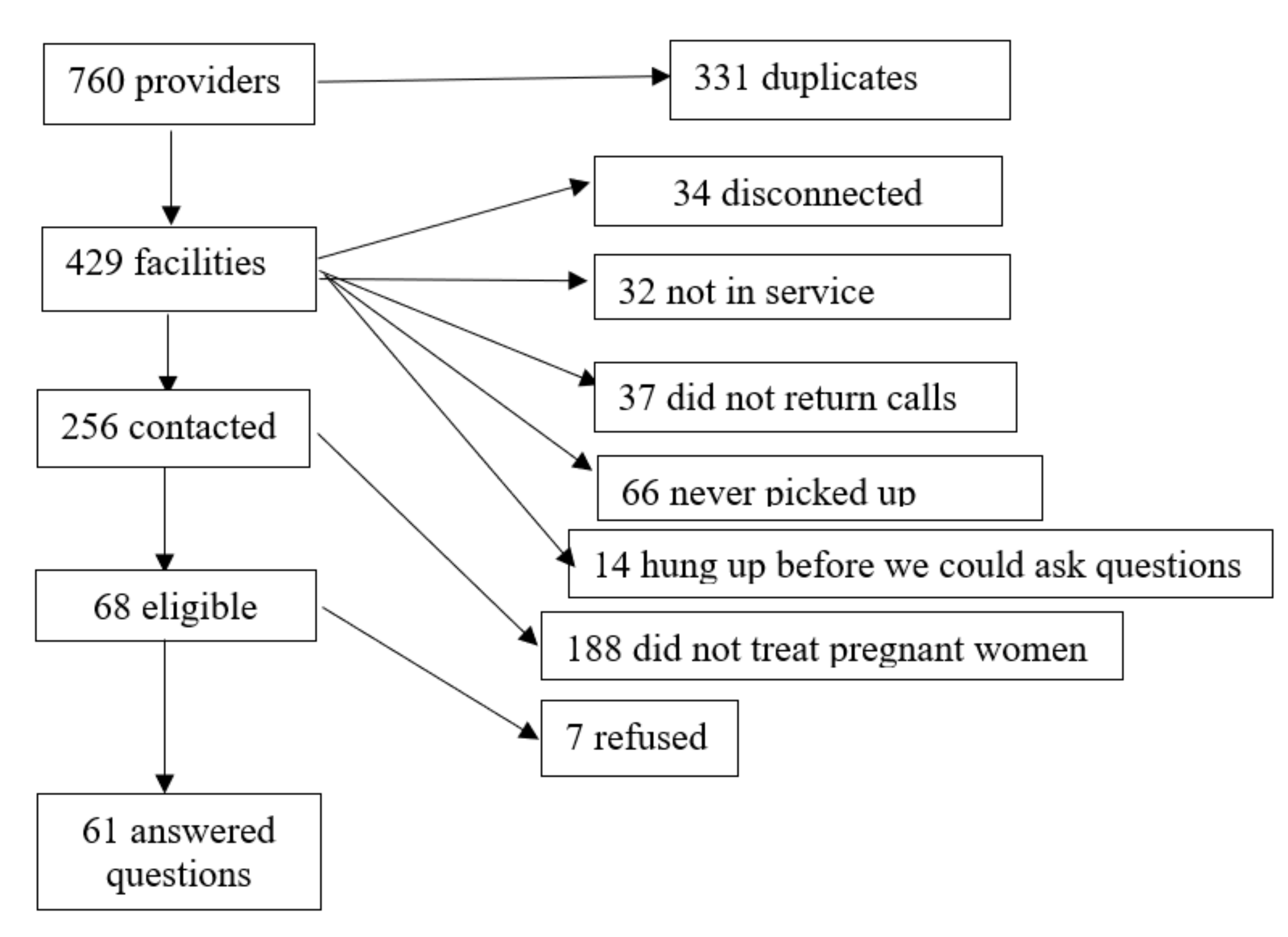
2.3. Health Care Availability
2.4. Outcomes
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Hurricane and PNC Use
3.2. Hurricane Michael and Maternity Care Availability
3.3. Hurricane Michael and Perinatal Outcomes by Maternity Care Availability
3.4. Mediation Analysis of PNC Use
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- March of Dimes. Nowhere to Go: Maternity Care Deserts across the U.S. 2018. Available online: https://www.marchofdimes.org/materials/Nowhere_to_Go_Final.pdf (accessed on 8 December 2020).
- Kozhimannil, K.B.; Hung, P.; Henning-Smith, C.; Casey, M.M.; Prasad, S. Association Between Loss of Hospital-Based Obstetric Services and Birth Outcomes in Rural Counties in the United States. JAMA 2018, 319, 1239–1247. [Google Scholar] [CrossRef] [PubMed]
- Lorch, S.A.; Srinivas, S.K.; Ahlberg, C.; Small, D.S. The impact of obstetric unit closures on maternal and infant pregnancy outcomes. Health Serv. Res. 2013, 48, 455–475. [Google Scholar] [CrossRef] [PubMed]
- Wallace, M.; Dyer, L.; Felker-Kantor, E.; Benno, J.; Vilda, D.; Harville, E.; Theall, K. Maternity Care Deserts and Pregnancy-Associated Mortality in Louisiana. Women’s Health Issues 2020. S104938672030102X. [Google Scholar] [CrossRef] [PubMed]
- Harville, E.W.; Tran, T.; Xiong, X.; Buekens, P. Population Changes, Racial/Ethnic Disparities, and Birth Outcomes in Louisiana After Hurricane Katrina. Disaster Med. Public Health Prep. 2010, 4, S39–S45. [Google Scholar] [CrossRef] [PubMed]
- Eskenazi, B.; Marks, A.R.; Catalano, R.; Bruckner, T.; Toniolo, P.G. Low birthweight in New York City and upstate New York following the events of September 11th. Hum. Reprod. 2007, 22, 3013–3020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, V.T.; Zotti, M.E.; Hsia, J. Impact of the Red River Catastrophic Flood on Women Giving Birth in North Dakota, 1994–2000. Matern. Child Health J. 2011, 15, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Rosales-Rueda, M. The impact of early life shocks on human capital formation: Evidence from El Niño floods in Ecuador. J. Health Econ. 2018, 62, 13–44. [Google Scholar] [CrossRef] [PubMed]
- Zahran, S.; Snodgrass, J.G.; Peek, L.; Weiler, S. Maternal Hurricane Exposure and Fetal Distress Risk. Risk Analysis 2010, 30, 1590–1601. [Google Scholar] [CrossRef]
- Dowswell, T.; Carroli, G.; Duley, L.; Gates, S.; Gülmezoglu, A.M.; Khan-Neelofur, D.; Piaggio, G. Alternative versus standard packages of antenatal care for low-risk pregnancy. Cochrane Database Syst. Rev. 2015, CD000934. [Google Scholar] [CrossRef] [Green Version]
- Frick, K.; Lantz, P. Selection bias in prenatal care utilization: An interdisciplinary framework and review of the literature. Med. Care Res. Rev. 1996, 53, 371–396. [Google Scholar] [CrossRef] [Green Version]
- Currie, J. Weathering the Storm: Hurricanes and Birth Outcomes. J. Health Econ. 2013, 32, 487–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdo, M.; Ward, I.; O’Dell, K.; Ford, B.; Pierce, J.R.; Fischer, E.V.; Crooks, J.L. Impact of Wildfire Smoke on Adverse Pregnancy Outcomes in Colorado, 2007–2015. Int. J. Environ. Res. Public Health 2019, 16, 3720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wainstock, T.; Anteby, E.Y.; Glasser, S.; Lerner-Geva, L.; Shoham-Vardi, I. Exposure to life-threatening stressful situations and the risk of preterm birth and low birth weight. Int. J. Gynecol. Obstet. 2014, 125, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Ishii, K.; Goto, A.; Ota, M.; Yasumura, S.; Abe, M.; Fujimori, K. Factors Associated with Infant Feeding Methods after the Nuclear Power Plant Accident in Fukushima: Data from the Pregnancy and Birth Survey for the Fiscal Year 2011 Fukushima Health Management Survey. Matern. Child Health J. 2016, 20, 1704–1712. [Google Scholar] [CrossRef] [PubMed]
- Bahmanjanbeh, F.; Kohan, S.; Yarmohammadian, M.H.; Haghshenas, A. Evaluation of reproductive health indicators in women affected by East Azarbaijan earthquake on August 2012. Iran. J. Nurs Midwifery Res. 2016, 21, 504–509. [Google Scholar] [PubMed]
- Giarratano, G.; Harville, E.W.; de Mendoza, V.B.; Savage, J.; Parent, C.M. Healthy Start: Description of a Safety Net for Perinatal Support during Disaster Recovery. Matern. Child Health J. 2015, 19, 819–827. [Google Scholar] [CrossRef] [Green Version]
- Dhital, R.; Silwal, R.C.; Simkhada, P.; van Teijlingen, E.; Jimba, M. Assessing knowledge and behavioural changes on maternal and newborn health among mothers following post-earthquake health promotion in Nepal. PLoS ONE 2019, 14, e0220191. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Health Disparities in Rural Women. Committee Opinion No. 586. Obstet Gynecol. 2014, 123, 384–388. [Google Scholar] [CrossRef]
- National Advisory Committee on Rural Health and Human Services. Maternal and Obstetric Care Challenges in Rural America. Policy Brief and Recommendations to the Secretary. 2020. Available online: https://www.hrsa.gov/sites/default/files/hrsa/advisory-committees/rural/publications/2020-maternal-obstetric-care-challenges.pdf (accessed on 8 December 2020).
- Lock, R. Hurricane Michael After-Action Report/Improvement Plan (AAR/IP). 2019. Available online: https://portal.floridadisaster.org/SERT/AfterActionReports/Real-World%20AARs/Hurricane%20Michael%20AAR-IP%201-7-19.pdf (accessed on 8 December 2020).
- Florida Hurricane Michael (DR-4399)|FEMA.gov. Available online: https://www.fema.gov/disaster/4399 (accessed on 16 April 2020).
- AtoZdatabases.Heinz. AtoZdatabases.com. The Premier Job Search, Reference and Mailing List Database. Available online: http://www.atozdatabases.com (accessed on 29 September 2020).
- Kotelchuck, M. The Adequacy of Prenatal Care Utilization Index: Its US distribution and association with low birthweight. Am. J. Public Health 1994, 84, 1486–1489. [Google Scholar] [CrossRef] [Green Version]
- Klebanoff, M.A.; Yossef-Salameh, L.; Latimer, C.; Oza-Frank, R.; Kachoria, R.; Reagan, P.B.; Oliver, E.A.; Buhimschi, C.S.; Buhimschi, I.A. Development and Validation of an Algorithm to Determine Spontaneous versus Provider-Initiated Preterm Birth in US Vital Records: Spontaneous vs. provider-initiated preterm birth. Paediatr. Perinat. Epidemiol. 2016, 30, 134–140. [Google Scholar] [CrossRef]
- Mandy, G.T.; Weisman, L.E.; Kim, M.S. Infants with fetal (intrauterine) growth restriction. In UpToDate; Post, T.W., Ed.; UpToDate: Waltham, MA, USA, 2020. [Google Scholar]
- United States Census Bureau. 2010 Census Urban and Rural Classification and Urban Area Criteria. Available online: https://www.census.gov/programs-surveys/geography/guidance/geo-areas/urban-rural/2010-urban-rural.html (accessed on 16 September 2020).
- Grubesic, T.H.; Matisziw, T.C. On the use of ZIP codes and ZIP code tabulation areas (ZCTAs) for the spatial analysis of epidemiological data. Int. J. Health Geogr. 2006, 5, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ZCTA to ZIP Code Crosswalk—UDS Mapper. Available online: https://www.udsmapper.org/zcta-crosswalk.cfm (accessed on 16 September 2020).
- Harville, E.; Pan, K.; Beitsch, L. Hurricane Michael and Adverse Birth Outcomes in the Florida Panhandle: Analysis of Vital Statistics Data. under review.
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Interactive Mediation Tests. Available online: http://quantpsy.org/sobel/sobel.htm (accessed on 2 October 2020).
- Allweiss, P. Diabetes and Disasters: Recent Studies and Resources for Preparedness. Curr. Diab. Rep. 2019, 19, 131. [Google Scholar] [CrossRef] [PubMed]
- Hospital Disaster Preparedness for Obstetricians and Facilities Providing Maternity Care. Available online: https://www.acog.org/en/Clinical/Clinical Guidance/Committee Opinion/Articles/2017/12/Hospital Disaster Preparedness for Obstetricians and Facilities Providing Maternity Care (accessed on 30 September 2020).
- Disaster Planning for Obstetrical Services. Available online: https://obgyn.stanford.edu/divisions/mfm/disaster-planning.html (accessed on 30 September 2020).
- Addressing Chronic Conditions in Disasters. Available online: https://spherestandards.org/addressing-chronic-conditions-in-disasters/ (accessed on 30 September 2020).
- Committee on Best Practices for Assessing Mortality and Significant Morbidity Following Large-Scale Disasters; Board on Health Sciences Policy; Health and Medicine Division; National Academies of Sciences, Engineering, and Medicine. A Framework for Assessing Mortality and Morbidity After Large-Scale Disasters; MacKenzie, E.J., Wollek, S.H., Yost, O.C., Cork, D.L., Eds.; National Academies Press: Washington, DC, USA, 2020; p. 25863. ISBN 978-0-309-68025-7. [Google Scholar]
- Harville, E.; Beitsch, L.; Uejio, C. Assessing the Effects of Disaster and Its Aftermath on Pregnant Women: A Conceptual Model. under review.
- Vidaeff, A.C.; Franzini, L.; Low, M.D. The unrealized potential of prenatal care. A population health approach. J. Reprod. Med. 2003, 48, 837–842. [Google Scholar]
- Special Supplemental Nutrition Program for Women, Infants, and Children (WIC)|USDA-FNS. Available online: https://www.fns.usda.gov/wic (accessed on 24 December 2020).
- Substance Use and Medication Safety|WIC Works Resource System. Available online: https://wicworks.fns.usda.gov/resources/substance-use-and-medication-safety (accessed on 26 December 2020).
- WIC Guidance for Screening and Referring Women with or at Risk for Depression|WIC Works Resource System. Available online: https://wicworks.fns.usda.gov/resources/wic-guidance-screening-and-referring-women-or-risk-depression (accessed on 26 December 2020).
- Zotti, M.E.; Williams, A.M.; Wako, E. Post-disaster Health Indicators for Pregnant and Postpartum Women and Infants. Matern. Child Health J. 2015, 19, 1179–1188. [Google Scholar] [CrossRef]
- Bitler, M.P.; Currie, J. Does WIC Work? The Effects of WIC on Pregnancy and Birth Outcomes. J. Policy Anal. Manag. 2005, 24, 73–91. [Google Scholar] [CrossRef]
- Kotelchuck, M.; Schwartz, J.B.; Anderka, M.T.; Finison, K.S. WIC participation and pregnancy outcomes: Massachusetts Statewide Evaluation Project. Am. J. Public Health 1984, 74, 1086–1092. [Google Scholar] [CrossRef] [Green Version]
- Wemette, M.; Hilts, A.S.; Mack, S.R.; Li, Y.; Eidson, M.; Santilli, L.A.; Nguyen, T.; Birkhead, G.S. Superstorm Sandy’s impact on the provision of WIC (Special Supplemental Nutrition Program for Women, Infants, and Children) services in New York State. Public Health Nutr. 2018, 21, 1388–1398. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| FEMA Individual a (Area A) | FEMA Public (Area B) | Not Affected (Area C) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | p-Value | Before | After | p-Value | Before | After | p-Value | |
| Mean (SE)/N (%) | Mean (SE)/N (%) | Mean (SE)/N (%) | |||||||
| Total number of births | 7555 | 7261 | 0.492 | 4334 | 4406 | 0.213 | 207014 | 206299 | 0.417 |
| Maternal age | 27.73 (5.72) | 27.86 (5.75) | 0.157 | 27.92 (5.89) | 28.19 (5.63) | 0.024 | 29.18 (5.83) | 29.33 (5.85) | <0.0001 |
| Maternal education level | |||||||||
| High School or GED or less | 3173 (42.67%) | 3109 (43.83%) | 0.001 | 1858 (43.35%) | 1980 (45.30%) | 0.015 | 86579 (42.26%) | 86503 (42.27%) | <0.0001 |
| Some College Credit, but no Degree or Associate Degree | 2370 (31.87%) | 2069 (29.17%) | 1412 (32.94%) | 1314 (30.06%) | 59307 (28.95%) | 57797 (28.24%) | |||
| Bachelor’s Degree and above | 1893 (25.46%) | 1915 (27.00%) | 1016 (23.71%) | 1077 (24.64%) | 58962 (28.78%) | 60360 (29.49%) | |||
| Maternal ethnicity | |||||||||
| Non-Hispanic white | 4455 (59.55%) | 4191 (58.51%) | 0.003 | 2955 (68.29%) | 2925 (66.64%) | 0.298 | 83808 (41.16%) | 83183 (40.71%) | <0.0001 |
| Hispanic white | 387 (5.17%) | 450 (6.28%) | 498 (11.51%) | 526 (11.98%) | 61018 (29.97%) | 62365 (30.52%) | |||
| Black | 2206 (29.49%) | 2169 (30.28%) | 552 (12.76%) | 613 (13.97%) | 45250 (22.22%) | 44801 (21.92%) | |||
| Other | 433 (5.79%) | 353 (4.93%) | 323 (7.44%) | 325 (7.40%) | 13526 (6.64%) | 13998 (6.85%) | |||
| WIC program | 3772 (50.98%) | 3346 (46.51%) | <0.0001 | 1762 (41.62%) | 1735 (39.54%) | 0.050 | 91147 (44.50%) | 85758 (42.14%) | <0.0001 |
| Prepregnancy BMI | 27.81 (7.31) | 27.86 (7.38) | 0.702 | 27.07 (6.76) | 27.32 (7.02) | 0.096 | 26.76 (6.50) | 26.95 (6.60) | <0.0001 |
| Smoking during pregnancy | 534 (7.10%) | 597 (8.28%) | 0.007 | 445 (10.29%) | 506 11.50%) | 0.070 | 8126 (3.94%) | 7755 (3.77%) | 0.004 |
| PNC started month | 2.76 (1.58) | 2.91 (1.72) | <0.0001 | 2.56 (1.55) | 2.65 (1.59) | 0.006 | 2.66 (1.68) | 2.69 (1.70) | <0.0001 |
| Whether received PNC | 7423 (98.84%) | 7097 (97.98%) | <0.0001 | 4263 (98.70%) | 4336 (98.55%) | 0.527 | 201876 (98.11%) | 200220 (98.09%) | 0.629 |
| Kotelchuck Index | |||||||||
| Inadequate | 918 (14.14%) | 1202 (18.60%) | <0.0001 | 460 (13.10%) | 562 (15.05%) | 0.001 | 29990 (16.57%) | 30309 (16.95%) | 0.001 |
| Intermediate | 656 (10.11%) | 714 (11.05%) | 343 (9.77%) | 431 (11.54%) | 22696 (12.54%) | 21812 (12.20%) | |||
| Adequate | 2938 (45.26%) | 2847 (44.06%) | 1518 (43.22%) | 1463 (39.18%) | 74243 (41.01%) | 73336 (41.00%) | |||
| Adequate plus | 1979 (30.49%) | 1699 (26.29%) | 1191 (33.91%) | 1278 (34.23%) | 54109 (29.89%) | 53399 (29.86%) | |||
| Univariate Model | Multivariable Model * | ||||||
|---|---|---|---|---|---|---|---|
| Area A & | Area B & | Area C & | Area A & | Area B & | Area C & | ||
| Whether received PNC services | N | 14,753 | 8719 | 409,899 | 14,753 | 8719 | 409,899 |
| RR@ (95% CI) | 0.992 (0.988, 0.997) | 0.998 (0.993, 1.003) | 1.000 (0.999, 1.001) | 0.994 (0.990, 0.998) | 0.999 (0.994, 1.004) | 1.000 (0.999, 1.001) | |
| p-value # | 0.001 | 0.382 | - | 0.003 | 0.652 | - | |
| Gestational month of first PNC | N | 12,222 | 7306 | 355,541 | 12,222 | 7306 | 355,541 |
| Difference @ (95% CI) | 0.107 (0.050, 0.165) | 0.094 (0.023, 0.165) | 0.027 (0.016, 0.039) | 0.112 (0.055, 0.169) | 0.088 (0.017, 0.159) | 0.034 (0.023, 0.045) | |
| p-value # | 0.007 | 0.071 | - | 0.008 | 0.139 | - | |
| Inadequate PNC ^ | N | 12,953 | 7246 | 359,894 | 12,953 | 7246 | 359,894 |
| RR@ (95% CI) | 1.215 (1.145, 1.288) | 1.180 (1.087, 1.281) | 0.999 (0.989, 1.009) | 1.193 (1.127, 1.264) | 1.154 (1.064, 1.251) | 1.0004 (0.991, 1.011) | |
| p-value # | <0.0001 | <0.0001 | - | <0.0001 | 0.001 | - | |
| Univariate Model | Multivariable Model * | ||||||
|---|---|---|---|---|---|---|---|
| Both Clinic and Hospital Available | Either Clinic or Hospital Available | None | Both Clinic and Hospital Available | Either Clinic or Hospital Available | None | ||
| RR (95% CI) # | RR (95% CI) # | ||||||
| Low birth weight (LBW) | After vs. before | 1.048 (0.869, 1.263) | 1.133 (0.838, 1.530) | 1.234 (1.062, 1.433) | 1.102 (0.970, 1.252) | 1.128 (0.857, 1.485) | 1.218 (1.054, 1.406) |
| p-value for interaction | - | - | 0.446 | - | - | 0.615 | |
| Spontaneous preterm birth (SPTB) | After vs. before | 1.124 (0.813, 1.553) | 1.068 (0.806, 1.414) | 0.880 (0.744, 1.041) | 1.253 (0.826, 1.902) | 1.024 (0.777, 1.350) | 0.864 (0.730, 1.024) |
| p-value for interaction | - | - | 0.314 | - | - | 0.208 | |
| Induced preterm birth (IPTB) | After vs. before | 0.813 (0.551, 1.200) | 1.218 (1.055, 1.406) | 0.949 (0.759, 1.186) | 0.852 (0.564, 1.287) | 1.187 (1.001, 1.407) | 0.932 (0.741, 1.172) |
| p-value for interaction | - | - | 0.188 | - | - | 0.303 | |
| Small for gestational age (SGA) | After vs. before | 1.425 (1.286, 1.579) | 0.979 (0.812, 1.181) | 1.146 (1.012, 1.296) | 1.389 (1.190, 1.621) | 1.002 (0.850, 1.182) | 1.121 (1.003, 1.253) |
| p-value for interaction | - | - | 0.159 | - | - | 0.244 | |
| Caesarean section | After vs. before | 1.035 (0.883, 1.212) | 1.041 (0.945, 1.147) | 1.003 (0.937, 1.074) | 1.056 (0.912, 1.221) | 1.049 (0.951, 1.156) | 0.995 (0.929, 1.066) |
| p-value for interaction | - | - | 0.807 | - | - | 0.620 | |
| No breast-feeding | After vs. before | 1.004 (0.962, 1.047) | 0.886 (0.778, 1.010) | 1.029 (0.964, 1.099) | 1.045 (0.961, 1.137) | 0.882 (0.928, 1.080) | 1.001 (0.928, 1.080) |
| p-value for interaction | - | - | 0.304 | - | - | 0.421 | |
| Area A & | Area B & | Area C & | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | p-Value ^ | Before | After | p-Value ^ | Before | After | p-Value ^ | |
| RR (95% CI) * | RR (95% CI) * | RR (95% CI) * | |||||||
| Low birth weight (LBW) | |||||||||
| Inadequate | 2.238 (1.644, 3.046) | 1.873 (1.455, 2.411) | 0.809 | 2.659 (1.778, 3.977) | 3.908 (2.672, 5.718) | 0.398 | 1.766 (1.675, 1.862) | 1.873 (1.777, 1.974) | 0.228 |
| Intermediate | 1.238 (0.814, 1.884) | 1.094 (0.760, 1.576) | 1.893 (1.164, 3.080) | 1.706 (1.027, 2.836) | 1.057 (0.986, 1.134) | 1.135 (1.059, 1.217) | |||
| Adequate plus | 4.026 (3.181, 5.096) | 3.888 (3.169, 4.770) | 3.213 (2.327, 4.437) | 3.839 (2.811, 5.518) | 3.045 (2.920, 3.176) | 3.076 (2.948, 3.207) | |||
| Spontaneous preterm birth (SPTB) | |||||||||
| Inadequate | 1.245 (0.898, 1.727) | 1.666 (1.223, 2.268) | 0.145 | 1.780 (1.125, 2.815) | 1.686 (1.0816, 2.631) | 0.493 | 1.468 (1.388, 1.553) | 1.563 (1.478, 1.654) | 0.347 |
| Intermediate | 1.902 (1.390, 2.603) | 1.718 (1.199, 2.461) | 1.467 (0.859, 2.505) | 1.773 (1.115, 2.820) | 1.289 (1.207, 1.375) | 1.378 (1.290, 1.472) | |||
| Adequate plus | 2.196 (1.741, 2.771) | 2.985 (2.320, 3.842) | 1.565 (1.078, 2.272) | 2.174 (1.537, 3.073) | 2.119 (2.025, 2.218) | 2.199 (2.099, 2.303) | |||
| Induced preterm birth (IPTB) | |||||||||
| Inadequate | 1.259 (0.870, 1.822) | 1.734 (1.257, 2.392) | 0.411 | 1.576 (1.008, 2.466) | 1.388 (0.967, 1.991) | 0.119 | 1.353 (1.270, 1.440) | 1.502 (1.414, 1.596) | 0.064 |
| Intermediate | 1.475 (1.007, 2.160) | 1.776 (1.222, 2.581) | 2.087 (1.332, 3.271) | 1.020 (0.651, 1.601) | 1.253 (1.168, 1.344) | 1.374 (1.282, 1.472) | |||
| Adequate plus | 2.733 (2.145, 3.454) | 3.560 (2.798, 4.631) | 2.971 (2.201, 4.010) | 2.109 (1.623, 2.740) | 2.688 (2.569, 2.812) | 2.779 (2.656, 2.908) | |||
| Small for gestational age (SGA) | |||||||||
| Inadequate | 1.672 (1.372, 2.038) | 1.374 (1.152, 1.639) | 0.344 | 2.063 (1.505, 2.829) | 2.519 (1.899, 3.341) | 0.802 | 1.346 (1.295, 1.398) | 1.361 (1.309, 1.414) | 0.855 |
| Intermediate | 0.911 (0.681, 1.219) | 0.994 (0.781, 1.265) | 1.087 (0.699, 1.689) | 1.169 (0.793, 1.723) | 0.982 (0.936, 1.031) | 0.962 (0.915, 1.011) | |||
| Adequate plus | 1.874 (1.592, 2.205) | 1.881 (1.622, 2.182) | 2.102 (1.899, 3.341) | 2.196 (1.718, 2.807) | 1.585 (1.535, 1.637) | 1.579 (1.528, 1.631) | |||
| Cesarean section | |||||||||
| Inadequate | 1.044 (0.927, 1.175) | 1.053 (0.950, 1.168) | 0.916 | 1.197 (1.024, 1.399) | 1.032 (0.896, 1.187) | 0.061 | 0.950 (0.932, 0.969) | 0.951 (0.933, 0.970) | 0.733 |
| Intermediate | 0.966 (0.845, 1.104) | 0.924 (0.812, 1.050) | 1.076 (0.893, 1.295) | 0.814 (0.678, 0.977) | 0.982 (0.962, 1.003) | 0.990 (0.969, 1.011) | |||
| Adequate plus | 1.207 (1.114, 1.307) | 1.233 (1.137, 1.338) | 1.254 (1.121, 1.402) | 1.053 (0.948, 1.174) | 1.162 (1.146, 1.179) | 1.153 (1.137, 1.170) | |||
| No breastfeeding | |||||||||
| Inadequate | 1.140 (1.000, 1.300) | 1.240 (1.099, 1.399) | 0.602 | 1.132 (0.911, 1.406) | 1.230 (1.001, 1.512) | 0.190 | 1.380 (1.334, 1.427) | 1.484 (1.437, 1.533) | <0.0001 |
| Intermediate | 1.161 (1.002, 1.346) | 1.109 (0.947, 1.298) | 0.993 (0.717, 1.308) | 1.073 (0.833, 1.381) | 1.078 (1.033, 1.126) | 1.132 (1.086, 1.180) | |||
| Adequate plus | 0.941 (0.832, 1.063) | 1.011 (0.890, 1.149) | 0.872 (0.717, 1.060) | 1.161 (0.973, 1.384) | 1.281 (1.241, 1.322) | 1.174 (1.138, 1.212) | |||
| Area A & | Area B & | Area C & | |||||
|---|---|---|---|---|---|---|---|
| Difference @ | 95% CI @ | RD @ | 95% CI @ | RD @ | 95% CI @ | ||
| Hurricane and Gestational month of first PNC * | After vs. Before | 0.112 | 0.055, 0.169 | 0.088 | 0.017, 0.159 | 0.034 | 0.023, 0.045 |
| Low birth weight (LBW) | |||||||
| RR @ | 95% CI @ | RR @ | 95% CI @ | RR @ | 95% CI @ | ||
| Gestational month of first PNC and # | 1.003 | 0.967, 1.041 | 1.049 | 0.999, 1.100 | 0.956 | 0.949, 0.963 | |
| Hurricane and LBW ^ | After vs. Before | 1.188 | 1.059, 1.334 | 1.025 | 0.875, 1.202 | 1.011 | 0.989, 1.202 |
| Hurricane and LBW adjusting for gestational month of first PNC ^ | After vs. Before | 1.194 | 1.064, 1.340 | 1.029 | 0.877, 1.206 | 1.013 | 0.990, 1.036 |
| Spontaneous preterm birth (SPTB) | |||||||
| Gestational month of first PNC and SPTB # | 0.897 | 0.851, 0.945 | 0.881 | 0.812, 0.955 | 0.870 | 0.862, 0.879 | |
| Hurricane and SPTB ^ | After vs. Before | 0.895 | 0.779, 1.027 | 1.186 | 0.968, 1.453 | 1.003 | 0.977, 1.029 |
| Hurricane and SPTB adjusting for gestational month of first PNC ^ | After vs. Before | 0.903 | 0.787, 1.037 | 1.198 | 0.978, 1.468 | 1.007 | 0.982, 1.034 |
| Induced preterm birth (IPTB) | |||||||
| Gestational month of first PNC and IPTB # | 0.835 | 0.783, 0.890 | 0.932 | 0.881, 0.985 | 0.879 | 0.871, 0.887 | |
| Hurricane and IPTB ^ | After vs. Before | 0.977 | 0.850, 1.123 | 1.072 | 0.916, 1.255 | 1.015 | 0.989, 1.042 |
| Hurricane and IPTB adjusting for inadequate/intermediate PNC ^ | After vs. Before | 0.991 | 0.862, 1.138 | 1.086 | 0.927, 1.271 | 1.019 | 0.993, 1.046 |
| Small for gestational age (SGA) | |||||||
| Gestational month of first PNC and SGA # | 1.067 | 1.040, 1.094 | 1.101 | 1.060, 1.143 | 1.031 | 1.025, 1.036 | |
| Hurricane and SGA ^ | After vs. Before | 1.130 | 1.031, 1.238 | 1.059 | 0.922, 1.216 | 0.986 | 0.968, 1.005 |
| Hurricane and SGA adjusting for Gestational month of first PNC ^ | After vs. Before | 1.126 | 1.028, 1.234 | 1.056 | 0.919, 1.212 | 0.985 | 0.967, 1.003 |
| Cesarean section | |||||||
| Gestational month of first PNC and Cesarean-section # | 0.991 | 0.975, 1.007 | 1.014 | 0.993, 1.036 | 0.976 | 0.973, 0.978 | |
| Hurricane and Cesarean section ^ | After vs. Before | 1.011 | 0.963, 1.061 | 0.999 | 0.9365 1.067 | 0.988 | 0.980, 0.997 |
| Hurricane and Cesarean section adjusting for Gestational month of first PNC ^ | After vs. Before | 1.015 | 0.967, 1.065 | 1.001 | 0.938, 1.069 | 0.989 | 0.980, 0.997 |
| No breastfeeding | |||||||
| Gestational month of first PNC and no breastfeeding # | 1.009 | 0.988, 1.029 | 1.006 | 0.973, 1.040 | 1.021 | 1.016, 1.026 | |
| Hurricane and no breastfeeding ^ | After vs. Before | 0.972 | 0.909, 1.041 | 1.057 | 0.950, 1.177 | 1.051 | 1.033, 1.070 |
| Hurricane and no breastfeeding adjusting for Gestational month of first PNC ^ | After vs. Before | 0.970 | 0.906, 1.038 | 1.055 | 0.948, 1.175 | 1.050 | 1.032, 1.069 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, K.; Beitsch, L.; Gonsoroski, E.; Sherchan, S.P.; Uejio, C.K.; Lichtveld, M.Y.; Harville, E.W. Effects of Hurricane Michael on Access to Care for Pregnant Women and Associated Pregnancy Outcomes. Int. J. Environ. Res. Public Health 2021, 18, 390. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020390
Pan K, Beitsch L, Gonsoroski E, Sherchan SP, Uejio CK, Lichtveld MY, Harville EW. Effects of Hurricane Michael on Access to Care for Pregnant Women and Associated Pregnancy Outcomes. International Journal of Environmental Research and Public Health. 2021; 18(2):390. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020390
Chicago/Turabian StylePan, Ke, Leslie Beitsch, Elaina Gonsoroski, Samendra P. Sherchan, Christopher K. Uejio, Maureen Y. Lichtveld, and Emily W. Harville. 2021. "Effects of Hurricane Michael on Access to Care for Pregnant Women and Associated Pregnancy Outcomes" International Journal of Environmental Research and Public Health 18, no. 2: 390. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020390