Sleep, Prospective Memory, and Immune Status among People Living with HIV

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Methods
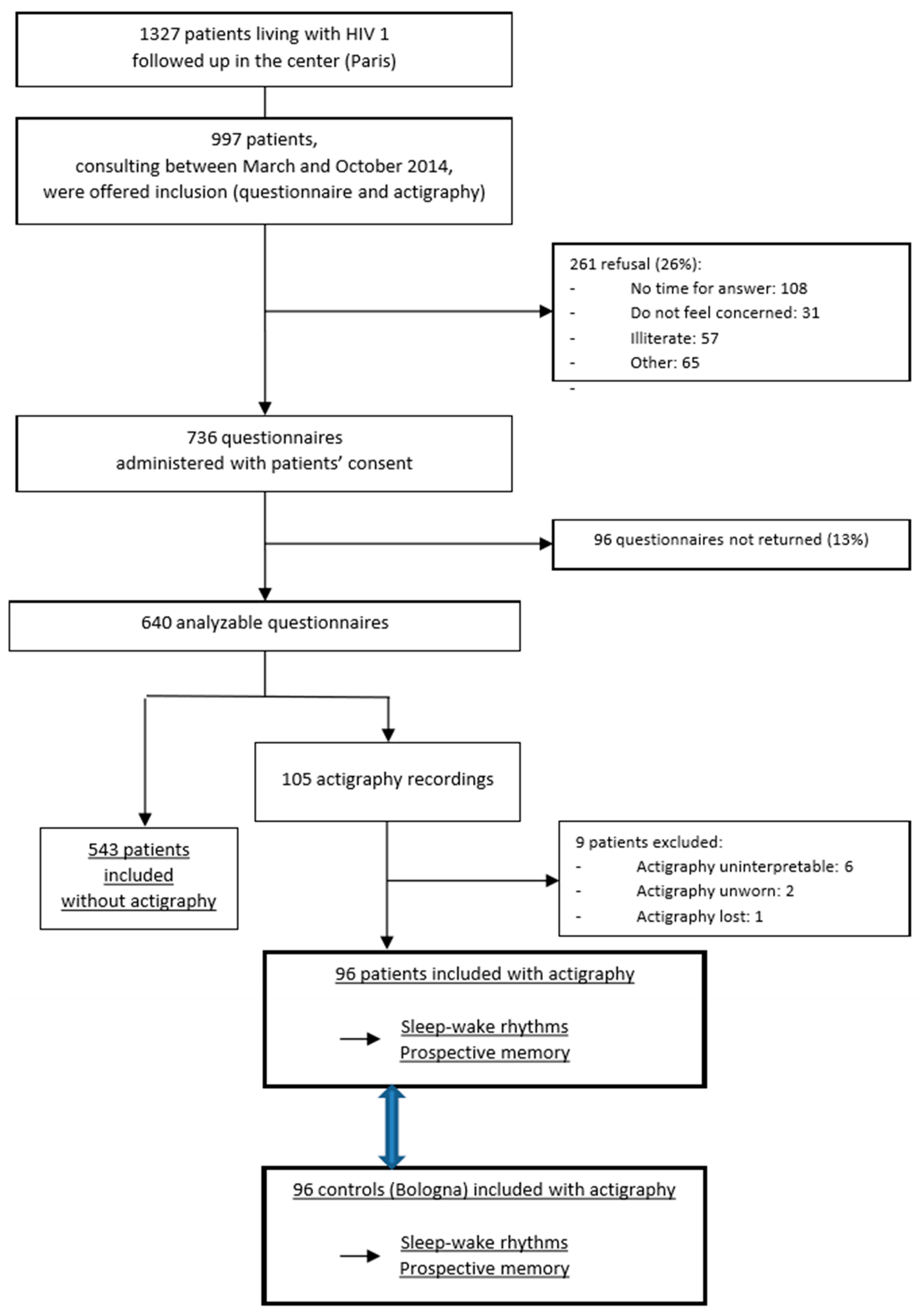
2.1. Study Design and Participants
2.2. Actigraphy
- Sleep start (SS): the start of sleep.
- Sleep end (ES): the end of sleep.
- Actual sleep time (AST): the amount of sleep.
- Actual wake time (AWT): the amount of time spent awake.
- Sleep latency (SL): the latency before sleep onset following bed time.
- Sleep efficiency (SE): the percentage of time spent asleep whilst in bed.
- Mean activity score (MAS): the average value of the activity counts per epoch over the assumed sleep period.
- Fragmentation index (FI): the percentage of immobility phases of 1 min as a proportion of the total number of immobility phases.
- Longest nap (LN): mean duration of the longest nap.
2.3. Prospective Memory Performance
2.4. HIV Parameters
2.5. Statistical Analysis
2.6. Ethics
3. Results
3.1. Actigraphic Night-Time and Daytime Parameters in PLWH and Healthy Controls
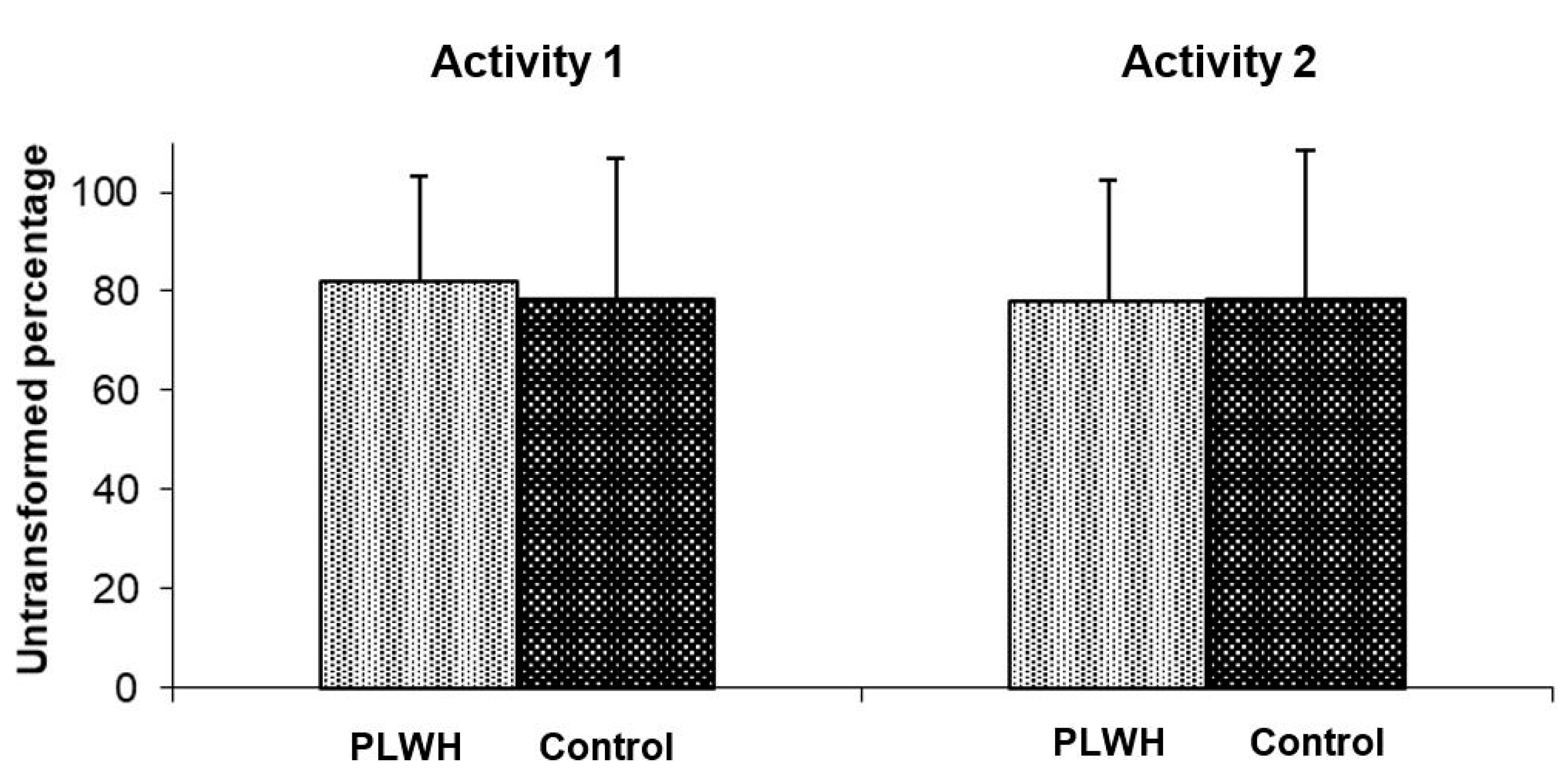
3.2. Activity-Based Prospective Memory Performance in HIV Patients and Healthy Controls
3.3. Actigraphic Night-Time Parameters and Activity-Based Prospective Memory Performance at Get-Up Time in PLWH and Controls
3.4. Factors Associated with Long Sleep in PLWH
4. Discussion
4.1. Sleep Alterations, Immune Activation and Possible Pathophysiological Mechanisms in PLWH
4.2. Cognitive Performance, Prospective Memory, and Sleep in PLWH
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, J.M. Clues to the functions of mammalian sleep. Nature 2005, 437, 1264–1271. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.R.; Wang, M.R.; Campomayor, C.O.; Collado-Hidalgo, A.; Cole, S. Sleep deprivation and activation of morning levels of cellular and genomic markers of inflammation. Arch. Intern. Med. 2006, 166, 1756–1762. [Google Scholar]
- Faraut, B.; Boudjeltia, K.Z.; Vanhamme, L.; Kerkhofs, M. Immune, inflammatory and cardiovascular consequences of sleep restriction and recovery. Sleep Med. Rev. 2012, 16, 137–149. [Google Scholar] [PubMed]
- Besedovsky, L.; Lange, T.; Haack, M. The Sleep-Immune Crosstalk in Health and Disease. Physiol. Rev. 2019, 99, 1325–1380. [Google Scholar] [PubMed] [Green Version]
- Buxton, O.M.; Marcelli, E. Short and long sleep are positively associated with obesity, diabetes, hypertension, and cardiovascular disease among adults in the United States. Soc. Sci. Med. 2010, 71, 1027–1036. [Google Scholar] [PubMed]
- Cappuccio, F.P.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Quantity and quality of sleep and incidence of type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2010, 33, 414–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irwin, M.R.; Olmstead, R.; Carroll, J.E. Sleep Disturbance, Sleep Duration, and Inflammation: A Systematic Review and Meta-Analysis of Cohort Studies and Experimental Sleep Deprivation. Biol. Psychiatry 2016, 80, 40–52. [Google Scholar] [PubMed] [Green Version]
- Léger, D.; Beck, F.; Richard, J.-B.; Sauvet, F.; Faraut, B. The risks of sleeping «too much». Survey of a National Representative Sample of 24671 adults (INPES health barometer). PLoS ONE 2014, 9, e106950. [Google Scholar]
- Cheng-Mayer, C.; Rutka, J.T.; Rosenblum, M.L.; McHugh, T.; Stites, D.P.; Levy, J.A. Human immunodeficiency virus can productively infect cultured human glial cells. Proc. Natl. Acad. Sci. USA 1987, 84, 3526–3530. [Google Scholar]
- Wang, T.; Jiang, Z.; Hou, W.; Li, Z.; Cheng, S.; Green, L.; Wang, Y.; Wen, X.; Cai, L.; Clauss, M.; et al. HIV Tat protein affects circadian rhythmicity by interfering with the circadian system. HIV Med. 2014, 15, 565–570. [Google Scholar]
- Darko, D.F.; Mitler, M.M.; Henriksen, S.J. Lentiviral infection, immune response peptides and sleep. Adv. Neuroimmunol. 1995, 5, 57–77. [Google Scholar] [CrossRef]
- Lee, K.A.; Gay, C.; Portillo, C.J.; Coggins, T.; Davis, H.; Pullinger, C.R.; Aouizerat, B.E. Types of sleep problems in adults living with HIV/AIDS. J. Clin. Sleep Med. 2012, 8, 67–75. [Google Scholar] [PubMed]
- Crum-Cianflone, N.F.; Roediger, M.P.; Moore, D.J.; Hale, B.; Weintrob, A.; Ganesan, A.; Eberly, L.E.; Johnson, E.; Agan, B.K.; Scott Letendre, S. Prevalence and factors associated with sleep disturbances among early-treated HIV-infected persons. Clin. Infect. Dis. 2012, 54, 1485–1494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girardin, J.-L.; Weber, K.M.; Aouizerat, B.E.; Levine, A.M.; Maki, P.M.; Liu, C.; Anastos, K.M.; Milam, J.; Keri, N.; Althoff, K.N.; et al. Insomnia symptoms and HIV infection among participants in the Women’s Interagency HIV Study. Sleep 2012, 35, 131–137. [Google Scholar]
- Allavena, C.; Guimard, T.; Billaud, E.; de la Tullaye, S.; Reliquet, V.; Pineau, S.; Hüe, H.; Supiot, C.; Chennebault, J.M.; Michau, C.; et al. Prevalence and risk factors of sleep disturbances in a large HIV-infected adult population. AIDS Behav. 2016, 20, 339–344. [Google Scholar] [PubMed]
- Faraut, B.; Malmartel, A.; Ghosn, J.; Duracinsky, M.; Leger, D.; Grabar, S.; Viard, J.-P. Sleep disturbance and total sleep time in HIV-infected persons: A cross-sectional study. AIDS Behav. 2018, 22, 2877–2887. [Google Scholar] [CrossRef] [PubMed]
- Gamaldo, C.E.; Spira, A.P.; Hock, R.S.; Salas, R.E.; McArthur, J.C.; David, P.M.; Mbeo, G.; Smith, M.T. Sleep, function and HIV: A multi-method assessment. AIDS Behav. 2013, 17, 2808–2815. [Google Scholar]
- Avci, G.; Sheppard, D.P.; Savanna, M.T.; Kordovski, V.M.; Sullivan, K.L.; Woods, S.P. A systematic review of prospective memory in HIV disease: From the laboratory to daily life. Clin. Neuropsychol. 2018, 32, 858–890. [Google Scholar]
- Heaton, R.K.; Franklin, D.R.; Ellis, R.J.; McCutchan, J.A.; Letendre, S.L.; LeBlanc, S.; Collier, A.C. HIV-associated neurocognitive disorders before and during the era of combination antiretroviral therapy: Differences in rates, nature, and predictors. J. Neurovirol. 2011, 17, 3–16. [Google Scholar]
- Sanmarti, M.; Ibáñez, L.; Huertas, S.; Badenes, D.; Dalmau, D.; Slevin, M.; Krupinski, J.; Aurel Popa-Wagner, A.; Jaen, A. HIV-associated neurocognitive disorders. J. Mol. Psychiatry 2014, 2, 2. [Google Scholar] [CrossRef] [Green Version]
- Banks, S.; Dinges, D.F. Behavioral and physiological consequencesof sleep restriction. J. Clin. Sleep Med. 2007, 3, 519–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gamaldo, C.E.; Gamaldo, A.; Creighton, J.; Salas, R.E.; Selnes, O.A.; David, P.M.; Mbeo, G.; Parker, B.S.; Brown, A.; McArthur, J.C.; et al. Evaluating sleep and cognition in HIV. J. Acquir. Immune Defic. Syndr. 2013, 63, 609–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byun, E.; Gay, C.L.; Lee, K.A. Sleep, fatigue, and problems with cognitive function in adults living with HIV. J. Assoc. Nurses AIDS Care 2016, 27, 5–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Einstein, G.O.; McDaniel, M.A.; Smith, R.E.; Shaw, P. Habitual prospective memory and aging: Remembering intentions and forgetting actions. Psychol. Sci. 1998, 9, 284–288. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [Green Version]
- Netzer, N.C.; Stoohs, R.A.; Netzer, C.M.; Clark, K.; Strohl, K.P. Using the Berlin questionnaire to identify patients at risk for the sleep apnea syndrome. Ann. Intern. Med. 1999, 131, 485–491. [Google Scholar] [CrossRef]
- Blais, F.C.; Gendron, L.; Mimeault, V.; Morin, C.M. evaluation of insomnia: Validity of 3 questionnaires. L’Encephale 1997, 23, 447–453. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Collet, L. The shortened Beck depression inventory (13 items). Study of the concurrent validity with the Hamilton scale and Widlöcher’s retardation scale. L’Encéphale 1986, 12, 77–79. [Google Scholar]
- Gandek, B.; Ware, J.E.; Aaronson, N.K.; Apolone, G.; Bjorner, J.B.; Brazier, J.E.; MBullinger, M.; Kaasa, S.; Leplege, A.; Prieto, L.; et al. Cross-validation of item selection and scoring for the SF-12 Health Survey in nine countries: Results from the International Quality of Life Assessment. J. Clin. Epidemiol. 1998, 51, 1171–1178. [Google Scholar] [CrossRef]
- Duracinsky, M.; Lalanne, C.; Le Coeur, S.; Herrmann, S.; Berzins, B.; Armstrong, A.R.; Tak Fai Lau, J.; Fournier, I.; Chassany, O. Psychometric validation of the PROQOLHIV questionnaire, a new health-related quality of life instrument- specific to HIV disease. J. Acquir. Immune Defic. Syndr. 2012, 59, 506–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonetti, L.; Pasquini, F.; Fabbri, M.; Belluzzi, M.; Natale, V. Comparison of two different actigraphs with polysomnography in healthy young subjects. Chronobiol. Int. 2008, 25, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, L. Validity of the Morningness–Eveningness Questionnaire for Adolescent (MEQ-A). Sleep Hypn. 2007, 9, 47–51. [Google Scholar]
- Natale, V.; Macieck, D.; Erbacci, A.; Tonetti, L.; Fabbri, M.; Martoni, M. Monitoring sleep with a smartphone accelerometer. Sleep Biol. Rhyth. 2012, 10, 287–292. [Google Scholar] [CrossRef]
- Natale, V.; Lehnkering, H.; Siegmund, R. Handedness and circadian motor activity asymmetries in humans: Preliminary findings. Physiol. Behav. 2010, 100, 322–326. [Google Scholar] [CrossRef]
- Picardi, A.; Abeni, D.; Mazzotti, E.; Fassone, G.; Lega, I.; Ramieri, L.; Sagoni, E.; Tiago, A.; Pasquini, P. Screening for psychiatry disorders in patients with skin diseases. A performance study of the 12-item General Health Questionnaire. J. Psychosom. Res. 2004, 57, 219–223. [Google Scholar] [CrossRef]
- Violani, C.; Devoto, A.; Lucidi, F.; Lombardo, C.; Russo, P.M. Validity of a Short Insomnia Questionnaire: The SQD. Brain Res. Bull. 2004, 63, 415–421. [Google Scholar] [CrossRef]
- Mc Nair, D.; Lorr, M.; Droppleman, L.F. Manual for the Profile of Mood States; Educational and Industrial Testing Service: San Diego, CA, USA, 1971. [Google Scholar]
- Natale, V.; Leger, D.; Martoni, M.; Bayon, V.; Erbacci, A. The role of actigraphy in the assessment of primary insomnia: A retrospective study. Sleep Med. 2014, 15, 111–115. [Google Scholar] [CrossRef]
- Tonetti, L.; Occhionero, M.; Boreggiani, M.; Conca, A.; Dondi, P.; Elbaz, M.; Fabbri, M.; Gauriau, C.; Giupponi, G.; Leger, D.; et al. Sleep and Prospective Memory: A Retrospective Study in Different Clinical Populations. Int. J. Environ. Res. Public Health 2020, 17, 6113. [Google Scholar] [CrossRef]
- Wu, J.; Wu, H.; Lu, C.; Guo, L.; Li, P. Self-reported sleep disturbances in HIV-infected people: A meta-analysis of prevalence and moderators. Sleep Med. 2015, 16, 901–907. [Google Scholar] [CrossRef]
- Chaponda, M.; Aldhouse, N.; Kroes, M.; Wild, L.; Robinson, C.; Smith, A. Systematic review of the prevalence of psychiatric illness and sleep disturbance as co-morbidities of HIV infection in the UK. Int. J. STD AIDS 2018, 29, 704–713. [Google Scholar] [CrossRef] [PubMed]
- Manzar, M.D.; Sony, P.; Salahuddin, M.; Kumalo, A.; Geneto, M.; Pandi-Perumal, S.R.; Moscovitch, A.; BaHammam, A.S. Electrolyte imbalance and sleep problems during anti-retroviral therapy: An under-recognized problem. Sleep Sci. 2017, 10, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Darko, D.F.; Miller, J.C.; Gallen, C.; White, J.; Koziol, J.; Brown, S.J.; Atkinson, J.H.; Assmus, J.; Munnell, D.T. Sleep electroencephalogram delta-frequency amplitude, night plasma levels of tumor necrosis factor alpha, and human immunodeficiency virus infection. Proc. Natl. Acad. Sci. USA 1995, 92, 12080–12084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taibi, D.M. A Pilot Study of Sleep Quality and Rest-Activity Patterns in persons living with HIV. J. Assoc. Nurses AIDS Care 2013, 24, 411–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, S.B.; Lu, M.; Glaze, D.G.; Reuben, J.M.; Harris, L.L.; Cohen, E.N.; Lee, B.N.; Zhao, E.; Paul, M.E.; Schwarzwald, H.; et al. Associations of cytokines, sleep patterns, and neurocognitive function in youth with HIV infection. Clin. Immunol. 2012, 144, 13–23. [Google Scholar] [CrossRef] [Green Version]
- Faraut, B.; Touchette, E.; Gamble, H.; Royant-Parola, S.; Safar, M.E.; Varsat, B.; Leger, D. Short sleep duration and increased risk of hypertension: A primary care medicine investigation. J. Hypertens. 2012, 30, 1354–1363. [Google Scholar] [CrossRef] [PubMed]
- Opp, M.R.; Rady, P.L.; Hughes, T.K., Jr.; Cadet, P.; Tyring, S.K.; Smith, E.M. Human immunodeficiency virus envelope glycoprotein 120 alters sleep and induces cytokine mRNA expression in rats. Am. J. Physiol. Regul. Integr. Comp. Physiol. 1996, 270, R963–R970. [Google Scholar] [CrossRef]
- Mantua, J.; Spencer, R.M.C. The interactive effects of nocturnal sleep and daytime naps in relation to serum C-reactive protein. Sleep Med. 2015, 16, 1213–1216. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Zhao, M.; Ren, J.; Qi, X.; Sun, H.; Qu, L.; Yan, C.; Zheng, T.; Wu, Q.; Cui, Y. Identifying factors associated with depression among men living with HIV/AIDS and undergoing antiretroviral therapy: A cross-sectional study in Heilongjiang, China. Health Qual. Life Outcomes 2018, 16, 190. [Google Scholar]
- Lewden, C.; Bouteloup, V.; De Wit, S.; Sabin, C.; Mocroft, A.; Wasmuth, J.C.; Ard van Sighem, A.; Kirk, O.; Obel, N.; Panos, G.; et al. Collaboration of Observational HIV Epidemiological Research Europe (COHERE) in EuroCoord, All-cause mortality in treated HIV-infected adults with CD4 ≥ 500/mm3 compared with the general population: Evidence from a large European observational cohort collaboration. Int. J. Epidemiol. 2012, 41, 433–445. [Google Scholar]
- Sherr, L.; Clucas, C.; Harding, R.; Sibley, E.; Catalan, J. HIV and depression—A systematic review of interventions. Psychol. Health Med. 2011, 16, 493–527. [Google Scholar] [CrossRef] [PubMed]
- Dhwanil, D.A.; Ozuna, L.; Harvey, B.H.; Viljoen, M.; Schetz, J.A. Adverse Neuropsychiatric Events and Recreational Use of Efavirenz and Other HIV-1 Antiretroviral Drugs. Pharmacol. Rev. 2018, 70, 684–711. [Google Scholar]
- Dorey-Stein, Z.; Amorosa, V.K.; Kostman, J.R.; Lo Re, V.; Shannon, R.P. Severe weight gain, lipodystrophy, dyslipidemia, and obstructive sleep apnea in a human immunodeficiency virus-infected patient following highly active antiretroviral therapy. J. Cardiometab. Syndr. 2008, 3, 111–114. [Google Scholar] [PubMed]
- Moeller, A.A.; Wiegand, M.; Oechsner, M.; Krieg, J.C.; Holsboer, F.; Emminger, C. Effects of zidovudine on EEG sleep in HIV-infected men. J. Acquir. Immune Defic. Syndr. 1992, 5, 636–637. [Google Scholar] [PubMed]
- Clifford, D.B.; Evans, S.; Yang, Y.; Acosta, E.P.; Ribaudo, H.; Gulick, R.M. Long-Term Impact of Efavirenz on Neuropsychological Performance and Symptoms in HIV-Infected Individuals (ACTG 5097s). HIV Clin. Trials 2009, 10, 343–355. [Google Scholar] [CrossRef]
- Moyle, G.; Fletcher, C.; Brown, H.; Mandalia, S.; Gazzard, B. Changes in sleep quality and brain wave patterns following initiation of an efavirenz-containing triple antiretroviral regimen. HIV Med. 2006, 7, 243–247. [Google Scholar] [CrossRef]
- Simen, A.A.; Ma, J.; Svetnik, V.; Mayleben, D.; Maynard, J.; Roth, A.; Mixson, L.; Mogg, R.; Shera, D.; George, L.; et al. Efavirenz modulation of sleep spindles and sleep spectral profile. Sleep Res. 2015, 24, 66–73. [Google Scholar]
- Kliegel, M.; Jäger, T.; Altgassen, M.; Shum, D. Clinical neuropsychology of prospective memory. In Prospective Memory: Cognitive, Neuroscience, Developmental, and Applied Perspectives; Kliegel, M., McDaniel, M.A., Einstein, G.O., Eds.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2008; pp. 283–288. [Google Scholar]
- Heaton, R.K.; Clifford, D.B.; Franklin, D.R.; Woods, S.P.; Ake, C.; Vaida, F.; Ellis, R.J.; Letendre, S.L.; Marcotte, T.D.; Atkinson, J.H.; et al. HIV-associated neurocognitive disorders persist in the era of potent antiretroviral therapy: CHARTER Study. Neurology 2010, 75, 2087–2096. [Google Scholar] [CrossRef] [Green Version]
- Scullin, M.K.; McDaniel, M.A. Remembering to execute a goal: Sleep on it! Psychol. Sci. 2010, 21, 1028–1035. [Google Scholar] [CrossRef]
- Diekelmann, S.; Wilhelm, I.; Wagner, U.; Born, J. Sleep to implement an intention. Sleep 2013, 36, 149–153. [Google Scholar]
- Occhionero, M.; Tonetti, L.; Fabbri, M.; Boreggiani, M.; Martoni, M.; Giovagnoli, S.; Natale, V. Prospective memory, sleep, and age. Brain Sci. 2020, 10, 422. [Google Scholar] [CrossRef] [PubMed]
- Fortier-Brochu, É.; Beaulieu-Bonneau, S.; Ivers, H.; Morin, C.M. Insomnia and daytime cognitive performance: A meta-analysis. Sleep. Med. Rev. 2012, 16, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, Z.; Hammond, A.; Nunez, R.A.; Irwin, M.R.; Thames, A.D. Effects of Sleep Health on Cognitive Function in HIV+ and HIV- Adults. J. Int. Neuropsychol. Soc. 2018, 24, 1038–1046. [Google Scholar] [CrossRef]
- Leong, R.L.F.; Shirley, Y.J.; Koh, S.Y.J.; Chee, M.W.L.; Lo, J.C. Slow wave sleep facilitates spontaneous retrieval in prospective memory. Sleep 2019, 42, zsz003. [Google Scholar] [CrossRef] [PubMed]
- Scullin, M.K.; Gao, C.; Fillmore, P.; Roberts, R.L.; Pruett, N.; Bliwise, D.L. Rapid eye movement sleep mediates age-related decline in prospective memory consolidation. Sleep 2019, 42, zsz055. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PLWH | Controls | Statistics | ||
|---|---|---|---|---|
| Mean ± SD (IC 95%) | Mean ± SD (IC 95%) | t(190) | pa | |
| Night-time parameters | ||||
| SS | 24:35 ± 1:23 (24:18–24:52) | 24:12 ± 1:05 (23:59–24:25) | 2.15 | 0.03 |
| ES | 08:05 ± 1:25 (07:47–08:22) | 07:39 ± 1:09 (07:25–07:53) | 2.31 | 0.02 |
| AST | 420 ± 61.47 (407.55–432.45) | 416.26 ± 51.73 (405.77–426.74) | 0.46 | 0.65 |
| AWT | 29.88 ± 13.45 (27.16–32.61) | 31.19 ± 11.74 (28.81–33.57) | −0.72 | 0.47 |
| SL | 11.65 ± 8.22 (9.98–13.32) | 7.88 ± 6.50 (6.57–9.20) | 3.52 | <0.001 |
| SE | 90.25 ± 3.60 (89.52–90.98) | 90.46 ± 3.10 (89.83–91.09) | −0.42 | 0.67 |
| MAS | 13.40 ± 5.76 (12.23–14.57) | 13.79 ± 5.29 (12.72–14.87) | −0.49 | 0.62 |
| FI | 32.83 ± 8.58 (31.09–34.57) | 27.84 ± 7.40 (26.34–29.34) | 4.32 | <0.001 |
| Daytime parameter | ||||
| LN | 32.49 ± 12.13 (30.03–34.95) | 22.98 ± 12.19 (20.51–25.45) | 5.42 | <0.001 |
| PLWH | Controls | |
|---|---|---|
| PM Performance | PM Performance | |
| Night-time parameters | ||
| SS | −0.13 | 0.08 |
| ES | −0.15 | −0.11 |
| AST | −0.02 | −0.17 |
| AWT | −0.09 | −0.20 |
| SL | −0.06 | −0.28 ** |
| SE | 0.10 | 0.26 * |
| MAS | −0.14 | −0.21 * |
| FI | −0.01 | −0.13 |
| Long Sleepers n (%) or Mean (sd) n = 41 | Short and Typical Sleepers n (%) or Mean (sd) n = 55 | OR (IC 95%) (n = 96) | p | |
|---|---|---|---|---|
| AIDS status | 11 (27) | 5 (9) | 4.45 (1.29–15.28) | <0.01 |
| Log2(Nadir CD4) | 7.75 (7.22) | 8.26 (7.23) | 0.66 (0.48–0.91) | 0.01 |
| CD4 cell countn (%) | ||||
| ≥500 cells/mm3 | 27 (64) | 36 (65) | 1 | |
| <499 cells/mm3 | 15 (36) | 19 (35) | 1.08 (0.46–2.53) | 0.86 |
| CD4/CD8 ratio < 1 | 30 (71) | 29 (54) | 2.37 (1.00–5.62) | 0.04 |
| Daytime napping | 41 (98) | 27 (49) | 20.78 (4.55–94.82) | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faraut, B.; Tonetti, L.; Malmartel, A.; Grabar, S.; Ghosn, J.; Viard, J.-P.; Natale, V.; Léger, D. Sleep, Prospective Memory, and Immune Status among People Living with HIV. Int. J. Environ. Res. Public Health 2021, 18, 438. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020438
Faraut B, Tonetti L, Malmartel A, Grabar S, Ghosn J, Viard J-P, Natale V, Léger D. Sleep, Prospective Memory, and Immune Status among People Living with HIV. International Journal of Environmental Research and Public Health. 2021; 18(2):438. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020438
Chicago/Turabian StyleFaraut, Brice, Lorenzo Tonetti, Alexandre Malmartel, Sophie Grabar, Jade Ghosn, Jean-Paul Viard, Vincenzo Natale, and Damien Léger. 2021. "Sleep, Prospective Memory, and Immune Status among People Living with HIV" International Journal of Environmental Research and Public Health 18, no. 2: 438. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020438