Twelve Years of the Italian Program to Enhance Relational and Communication Skills (PERCS)

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. The PERCS-Italy Program
2.2. Participants
2.3. Measures
2.4. Data Analysis
2.5. Ethics
3. Results
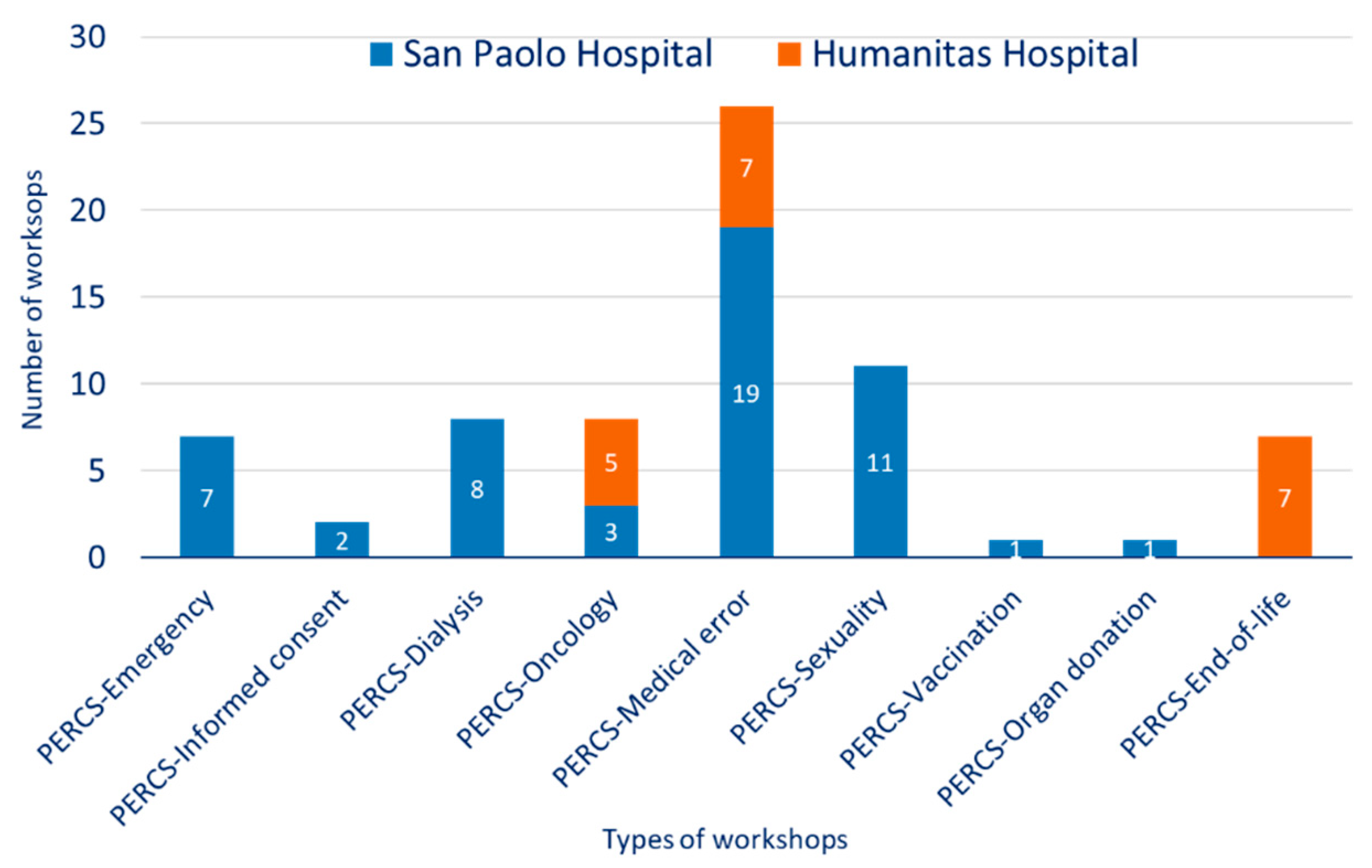
3.1. Sustainability and Development of PERCS Workshops
3.2. Participants’ Characteristics
3.3. Perceived Improvements after PERCS Workshops
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lautrette, A.; Darmon, M.; Megarbane, B.; Joly, L.M.; Chevret, S.; Adrie, C.; Barnoud, D.; Bleichner, G.; Bruel, C.; Choukroun, G.; et al. A Communication Strategy and Brochure for Relatives of Patients Dying in the ICU. N. Engl. J. Med. 2007, 356, 469–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mack, J.W.; Hilden, J.M.; Watterson, J.; Moore, C.; Turner, B.; Grier, H.E.; Weeks, J.C.; Wolfe, J. Parent and physician perspectives on quality of care at the end of life in children with cancer. J. Clin. Oncol. 2005, 23, 9155–9161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Canale, S.; Louis, D.Z.; Maio, V.; Wang, X.; Rossi, G.; Hojat, M.; Gonnella, J.S. The Relationship Between Physician Empathy and Disease Complications: An Empirical Study of Primary Care Physicians and Their Diabetic Patients in Parma, Italy. Acad. Med. 2012, 87, 1243–1249. [Google Scholar] [CrossRef] [PubMed]
- Levinson, W.; Roter, D.L.; Mullooly, J.P.; Dull, V.T.; Frankel, R.M. Physician-patient communication: The relationship with malpractice claims among primary care physicians and surgeons. JAMA 1997, 277, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.A.; Zhang, B.; Ray, A.; Mack, J.W.; Trice, E.; Balboni, T.; Mitchell, S.L.; Jackson, V.A.; Block, S.D.; Maciejewski, P.K.; et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA 2008, 300, 1665–1673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meier, D.E.; Back, A.L.; Morrison, R.S. The inner life of physicians and care of the seriously ill. JAMA 2001, 286, 3007–3014. [Google Scholar] [CrossRef] [Green Version]
- Martin, E.B.; Mazzola, N.M.; Brandano, J.; Luff, D.; Zurakowski, D.; Meyer, E.C. Clinicians’ recognition and management of emotions during difficult healthcare conversations. Patient Educ. Couns. 2015, 98, 1248–1254. [Google Scholar] [CrossRef]
- Lamiani, G.; Barello, S.; Browning, D.M.; Vegni, E.; Meyer, E.C. Uncovering and validating clinicians’ experiential knowledge when facing difficult conversations: A cross-cultural perspective. Patient Educ. Couns. 2012, 87, 307–312. [Google Scholar] [CrossRef]
- Salmon, P.; Young, B. Creativity in clinical communication: From communication skills to skilled communication. Med. Educ. 2011, 45, 217–226. [Google Scholar] [CrossRef]
- Browning, D.M.; Meyer, E.C.; Truog, R.D.; Solomon, M.Z. Difficult conversations in health care: Cultivating relational learning to address the hidden curriculum. Acad. Med. 2007, 82, 905–913. [Google Scholar] [CrossRef]
- Lipkin, M.; Kaplan, C.; Clark, W.; Novack, D.H. Teaching Medical Interviewing: The Lipkin Model. In The Medical Interview; Lipkin, M., Putnam, S.M., Lazare, A., Carroll, J.G., Frankel, R.M., Eds.; Frontiers of Primary Care: New York, NY, USA, 1995; pp. 422–435. [Google Scholar]
- Bell, S.K.; Langer, T.; Luff, D.; Rider, E.A.; Brandano, J.; Meyer, E.C. Interprofessional Learning to Improve Communication in Challenging Healthcare Conversations: What Clinicians Learn From Each Other. J. Contin. Educ. Health Prof. 2019, 39, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Fallowfield, L.; Lipkin, M.; Hall, A. Teaching senior oncologists communication skills: Results from phase I of a comprehensive longitudinal program in the United Kingdom. J. Clin. Oncol. 1998, 16, 1961–1968. [Google Scholar] [CrossRef] [PubMed]
- Back, A.L.; Arnold, R.M.; Baile, W.F.; Fryer-Edwards, K.A.; Stewart, C.A.; Barley, G.E.; Gooley, T.A.; Tulsky, J.A. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Arch. Intern. Med. 2007, 167, 453–460. [Google Scholar] [CrossRef] [Green Version]
- Baile, W.F.; De Panfilis, L.; Tanzi, S.; Moroni, M.; Walters, R.; Biasco, G. Using sociodrama and psychodrama to teach communication in end-of-life care. J. Palliat. Med. 2012, 15, 1006–1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bays, A.M.; Engelberg, R.A.; Back, A.L.; Ford, D.W.; Downey, L.; Shannon, S.E.; Doorenbos, A.Z.; Edlund, B.; Christianson, P.; Arnold, R.W.; et al. Interprofessional communication skills training for serious illness: Evaluation of a small-group, simulated patient intervention. J. Palliat. Med. 2014, 17, 159–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, A.W.M.; Düsman, H.; Tan, L.H.C.; Jansen, J.J.M.; Grol, R.P.T.M.; Van Der Vleuten, C.P.M. Acquisition of communication skills in postgraduate training for general practice. Med. Educ. 2004, 38, 158–167. [Google Scholar] [CrossRef] [Green Version]
- Hulsman, R.L.; Ros, W.J.G.; Winnubst, J.A.M.; Bensing, J.M. Teaching clinically experienced physicians communication skills. A review of evaluation studies. Med. Educ. 1999, 33, 655–668. [Google Scholar] [CrossRef] [Green Version]
- Lamiani, G.; Meyer, E.C.; Leone, D.; Vegni, E.; Browning, D.M.; Rider, E.A.; Truog, R.D.; Moja, E. A Cross-cultural adaptation of an innovative approach to learning about difficult conversations in healthcare. Med. Teach. 2011, 33, e57–e64. [Google Scholar] [CrossRef] [Green Version]
- Oteri, R.; Borghi, L.; Leone, D.; Vegni, E.; Lamiani, G. The experience of the Program to Enhance Relational and Communication Skills 10 years after its inception in Italy. Recenti. Prog. Med. 2020, 111, 142–148. [Google Scholar]
- Truog, R.D.; Browning, D.M.; Johnson, J.A.; Gallagher, T.H.; Leape, L. Talking with Patients and Families about Medical Error: A Guide for Education and Practice; Johns Hopkins University Press: Washington, DC, USA, 2011. [Google Scholar]
- Rogers, C. The facilitation of significant learning. In Contemporary Theories of Instruction; Siegel, L., Ed.; Chandler: San Francisco, CA, USA, 1967. [Google Scholar]
- Bell, S.K.; Pascucci, R.; Fancy, K.; Coleman, K.; Zurakowski, D.; Meyer, E.C. The educational value of improvisational actors to teach communication and relational skills: Perspectives of interprofessional learners, faculty, and actors. Patient Educ. Couns. 2014, 96, 381–388. [Google Scholar] [CrossRef]
- Meyer, E.C.; Sellers, D.E.; Browning, D.M.; McGuffie, K.; Solomon, M.Z.; Truog, R.D. Difficult conversations: Improving communication skills and relational abilities in health care. Pediatr. Crit. Care Med. 2009, 10, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Meyer, E.C.; Brodsky, D.; Hansen, A.R.; Lamiani, G.; Sellers, D.E.; Browning, D.M. An interdisciplinary, family-focused approach to relational learning in neonatal intensive care. J. Perinatol. 2011, 31, 212–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, M.R.; Thiel, M.M.; Shirkey, K.; Zurakowski, D.; Meyer, E.C. Efficacy of training interprofessional spiritual care generalists. J. Palliat. Med. 2016, 19, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.D.; Callahan, M.J.; Browning, D.M.; Lebowitz, R.L.; Bell, S.K.; Jang, J.; Meyer, E.C. Radiology trainees’ comfort with difficult conversations and attitudes about error disclosure: Effect of a communication skills workshop. J. Am. Coll. Radiol. 2014, 11, 781–787. [Google Scholar] [CrossRef]
- Luff, D.; Fernandes, S.; Soman, A.; Meyer, E.C.; Brown, S.D. The influence of communication and relational education on radiologists’ early posttraining practice. J. Am. Coll. Radiol. 2016, 13, 445–448. [Google Scholar] [CrossRef]
- Mishra, A.; Browning, D.; Haviland, M.J.; Jackson, M.L.; Luff, D.; Meyer, E.C.; Talcott, K.; Kloek, C.E. Communication skills training in ophthalmology: Results of a needs assessment and pilot training program. J. Surg. Educ. 2018, 75, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Rogers, R.W. Attitude change and information integration in fear appeals. Psychol. Rep. 1985, 56, 179–182. [Google Scholar] [CrossRef]
- Thiel, M.M.; Luff, D.; Kerr, E.E.; Robinson, M.R.; Meyer, E.C. Healthcare professionals’ reflections on their learning as spiritual generalists and integration into practice. J. Contin. Educ. Health Prof. 2020, 40, 228–234. [Google Scholar] [PubMed]
- Sullivan, A.M.; Rock, L.K.; Gadmer, N.M.; Norwich, D.E.; Schwartzstein, R.M. The Impact of Resident Training on Communication with Families in the Intensive Care Unit. Resident and Family Outcomes. Ann Am Thorac Soc. 2016, 13, 512–521. [Google Scholar]
- Rachwal, C.M.; Langer, T.; Trainor, B.P.; Bell, M.A.; Browning, D.M.; Meyer, E.C. Navigating communication challenges in clinical practice: A new approach to team education. Crit. Care Nurse 2018, 38, 15–22. [Google Scholar] [CrossRef]


{kind=link}
| Strategies | Activities |
|---|---|
| Warm-up | Pre-test assessment |
| Introduction of PERCS principles | |
| Participants introductions | |
| Brainstorming | Sharing perspectives on “what works in difficult conversations…” |
| Didactic lecture | Theoretical framework |
| Active learning | Simulation I with actor |
| Group debriefing | |
| Simulation II with actor | |
| Group debriefing | |
| Cognitive integration | Take-home points |
| Post-test assessment |
| Case scenario I—Massimo Pecca | Case Scenario II—Lucia Molteni | |
|---|---|---|
| Massimo Pecca is a 65-year-old man hospitalized for a lung lobectomy due to a tumor of the lung. After surgery, the physician orders an infusion of morphine for pain management at 1.0 mg/h, using the “trailing zero”, a practice prohibited by hospital policy. The nurse, not accustomed to the trailing zero, reads the order as 10 mg/h, not the intended 1 mg/h. The nurse calls the physician to express her concern about the high dose and asks the reason for such a high dose, without specifically mentioning the actual dosage. The physician replies that the dose he ordered (1 mg/h) is appropriate for the intervention. The nurse then starts the infusion at 10 mg/h precipitating a respiratory arrest and transfer to the ICU. After admission in the ICU, Massimo recovers completely. The physician and the nurse meet with the daughter, while Massimo is recovered in the ICU, to communicate the error. | Lucia Molteni is a 41-year-old woman who has been hospitalized for a caesarean section. On the first post-partum day, the physician advises a transfusion of two bags of blood components due to blood loss (around 900 cc) and anemia. The patient agrees to the transfusion but asks that the bags be covered because of an aversion to the blood. The nurse submits the physician’s request to the transfusion center, where only one operator is present. The transfusion center operator, being the only two bags required in the morning, delivers the bags without checking them. The nurse having asked for Lucia Molteni’s bags, takes the bags without checking the name of the request and performs the transfusion by covering the bags as requested. After a while, Lucia begins to feel unwell, trembles, and sweats, and the doctor decides to suspend the infusion. The patient receives 1 gr of flebocortid and 1 mg of a benzodiazepine, with an immediate resolution of the symptoms. Upon discarding the bag, the clinical team realizes they have administered blood to Lucia which is incompatible with blood type. The patient’s change in renal function parameters is so compromised that it requires treatment of two sessions of dialysis. The healthcare team have to communicate to Lucia the error and the new treatment required. |
| Characteristics | Total Participants (n = 830) | San Paolo University Hospital (n = 602) | Humanitas University Hospital (n = 228) |
|---|---|---|---|
| Discipline, N (%) Nurses Physicians Psychosocial professionals a Other professionals b Valid N | 297 (37) 269 (33) 80 (10) 171 (20) 807 (100) | 200 (34) 195 (33) 71 (12) 118 (20) 584 (100) | 97 (44) 74 (33) 9 (4) 43 (19) 223 (100) |
| Years of experience, mean (sd), range | 15.8 (10.6), 0–45 | 16.1 (11), 0–45 | 15.0 (9.3), 1–40 |
| Age, mean (sd), range | 41.6 (10.5), 20–68 | 42 (10.7), 20–66 | 40.1 (9.7), 22–68 |
| Gender, N (%) Female Valid N | 647(81) 802 (100) | 458 (79) 580 (100) | 189 (85) 222 (100) |
| Ethnicity, N (%) Italians Valid N | 768 (96) 801 (100) | 567 (98) 579 (100) | 201 (91) 222 (100) |
| Previous learning experience in communication, N (%) None Coursework Practical experience Residency Continuing education Other Multiple choice of above Valid N | 299 (36) 45 (5.4) 165 (19.9) 66 (7.9) 74 (8.9) 56 (6.7) 125 (15.1) 830 (100) | 220 (36.6) 29 (4.8) 109 (18.1) 41 (6.8) 46 (7.6) 32 (5.3) 125 (20.8) 602 (100) | 79 (34.6) 16 (7) 56 (24.6) 25 (11) 28 (12.3) 24 (10.5) 0 (0) 228 (100) |
| Mentor/role model, N (%) Yes Valid N | 260 (33) 784 (100) | 184 (33) 566 (100) | 76 (35) 218 (100) |
| Type of PERCS, N (%) PERCS-Emergency Medicine PERCS-Dialysis PERCS-Oncology PERCS-Informed Consent PERCS-Medical Error PERCS-Sexuality PERCS-Organ Donation PERCS-Vaccination PERCS-End of Life Valid N | 86 (11) 84 (10) 99 (12) 24 (3) 309 (37) 127 (15) 16 (2) 10 (1) 75 (9) 830 (100) | 86 (14) 84 (14) 37 (6) 24 (4) 218 (36) 127 (21) 16 (3) 10 (2) - 602 (100) | - - 62 (27) - 91 (40) - - - 75 (33) 228 (100) |
| Dimensions | Baseline Mean (sd) | Post-Test Mean (sd) | Paired-Sample t-Test | Cohen’s d | 95% Confidence Interval |
|---|---|---|---|---|---|
| Preparation Communication Relationship Confidence Anxiety | 2.60 (0.93) 2.80 (0.84) 3.14 (0.89) 2.72 (0.88) 3.06 (1.00) | 3.33 (0.73) 3.35 (0.73) 3.47 (0.72) 3.37 (0.75) 2.77 (0.85) | −23.74 * −19.22 * −10.72 * −22.49 * 8.84 * | −0.87 −0.71 −0.40 −0.83 0.33 | −0.80–−0.68 −0.61–−0.50 −0.38–−0.26 −0.71–−0.60 0.22–0.35 |
| Discipline | Preparation | Communication Skills | Relationship | Confidence | Anxiety | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline Mean (sd) | Post-Test Mean (sd) | F | Baseline Mean (sd) | Post-Test Mean (sd) | F | Baseline Mean (sd) | Post-Test Mean (sd) | F | Baseline Mean (sd) | Post-Test Mean (sd) | F | Baseline Mean (sd) | Post-Test Mean (sd) | F | |
| 4.23 * | 5.89 ** | 2.27 | 3.37 * | 1.18 | |||||||||||
| Physicians | 2.83 (0.95) | 3.52 (0.68) | 3.10 (0.79) | 3.50 (0.68) | 3.36 (0.79) | 3.57 (0.66) | 2.96 (0.88) | 3.52 (0.76) | 2.93 (0.99) | 2.69 (0.85) | |||||
| Nurses | 2.59 (0.81) | 3.22 (0.68) | 2.70 (0.78) | 3.29 (0.71) | 3.02 (0.84) | 3.41 (0.68) | 2.67 (0.81) | 3.32 (0.69) | 3.10 (0.97) | 2.85 (0.83) | |||||
| Psychosocial professionals | 2.73 (0.99) | 3.51 (0.68) | 2.94 (0.90) | 3.39 (0.70) | 3.26 (0.93) | 3.54 (0.71) | 2.81 (0.91) | 3.39 (0.68) | 3.03 (0.98) | 2.64 (0.87) | |||||
| Others | 2.17 (0.96) | 3.15 (0.86) | 2.37 (0.87) | 3.15 (0.83) | 2.90 (1.07) | 3.31 (0.89) | 2.33 (0.91) | 3.21 (0.80) | 3.19 (1.04) | 2.78 (0.91) | |||||
| Total | 2.60 (0.93) | 3.34 (0.73) | 2.80 (0.86) | 3.34 (0.73) | 3.14 (0.90) | 3.46 (0.73) | 2.72 (0.89) | 3.37 (0.74) | 3.05 (0.99) | 2.76 (0.86) | |||||
| Partecipants’ Satisfaction | Physicians | Nurses | Psychosocial Professionals a | Others b | X2 | p |
|---|---|---|---|---|---|---|
| Usefulness of the program, % Not at all/little Somewhat Quite/very useful | 0.8 11 88.2 | 0 4.9 95.1 | 0 4.1 95.9 | 0.6 6 93.4 | 18.37 | 0.244 |
| Quality of the program, % Poor/fair Good Very good/excellent | 1.6 20 78.4 | 0.7 11.5 87.8 | 1.4 17.8 80.8 | 0.7 10.1 89.2 | 14.61 | 0.263 |
| Recommendation of the program, % Yes | 98.4 | 99.6 | 98.6 | 100 | 4.85 | 0.563 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borghi, L.; Meyer, E.C.; Vegni, E.; Oteri, R.; Almagioni, P.; Lamiani, G. Twelve Years of the Italian Program to Enhance Relational and Communication Skills (PERCS). Int. J. Environ. Res. Public Health 2021, 18, 439. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020439
Borghi L, Meyer EC, Vegni E, Oteri R, Almagioni P, Lamiani G. Twelve Years of the Italian Program to Enhance Relational and Communication Skills (PERCS). International Journal of Environmental Research and Public Health. 2021; 18(2):439. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020439
Chicago/Turabian StyleBorghi, Lidia, Elaine C. Meyer, Elena Vegni, Roberta Oteri, Paolo Almagioni, and Giulia Lamiani. 2021. "Twelve Years of the Italian Program to Enhance Relational and Communication Skills (PERCS)" International Journal of Environmental Research and Public Health 18, no. 2: 439. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020439