Prioritizing Community-Based Intervention Programs for Improving Treatment Compliance of Patients with Chronic Diseases: Applying an Analytic Hierarchy Process

Abstract
:1. Introduction
1.1. Chronic Diseases Intervention Program and Rule of Halves
1.2. Chronic Diseases Management Policy and Analytic Hierarchy Process (AHP)
2. Materials and Methods
2.1. Developing the Analytic Hierarchy Process (AHP) Model
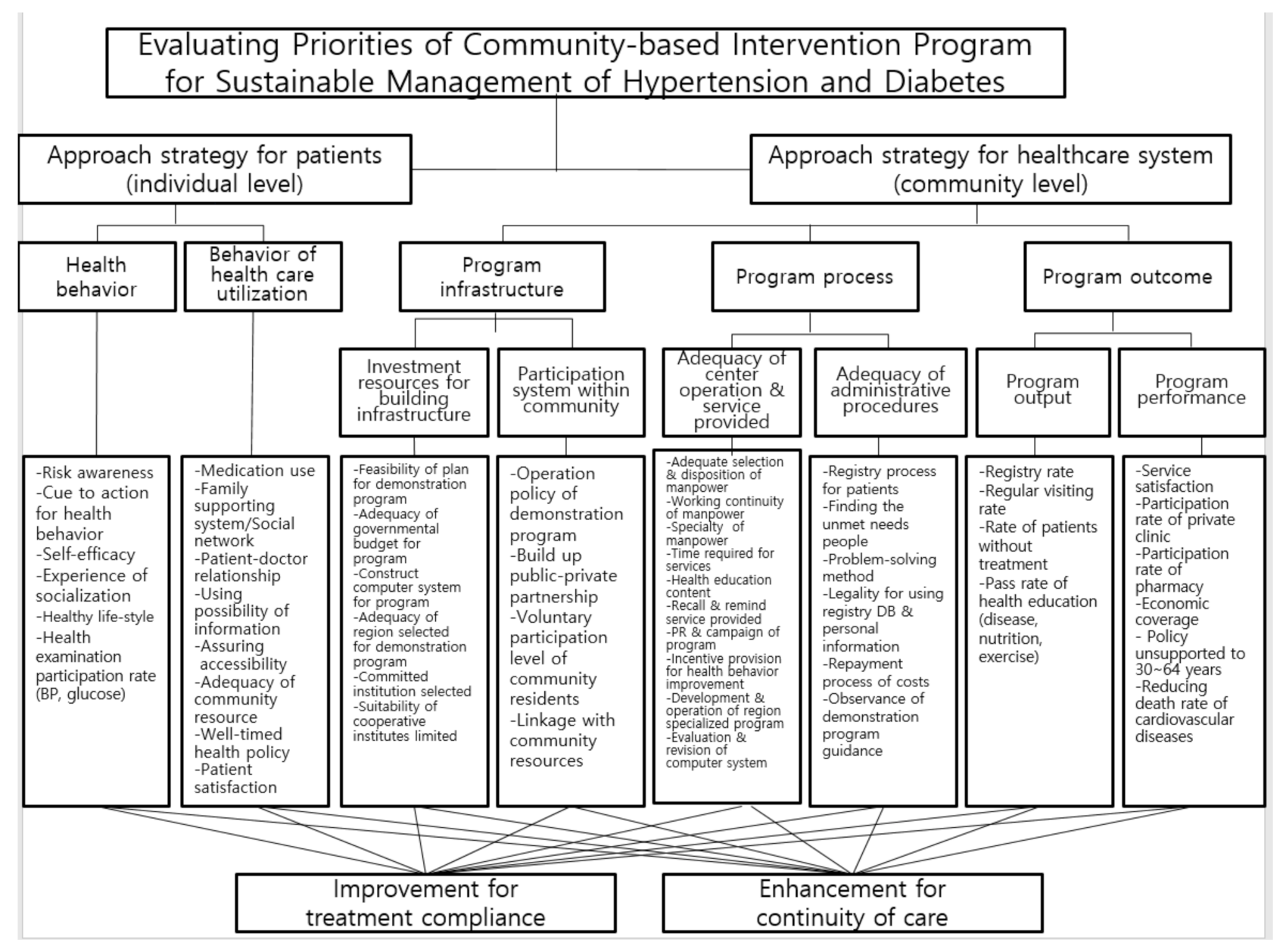
2.2. Decision Hierarchy Criteria for Selecting Prioritization
2.3. AHP Questionnaire Survey and Priority Analysis
3. Results
3.1. General Characteristics of AHP Survey Participants
3.2. Importance Evaluation to Approach Strategy for Patients and Healthcare System
3.3. Pairwise Comparison of Evaluation Criteria for Community-Based Intervention Program
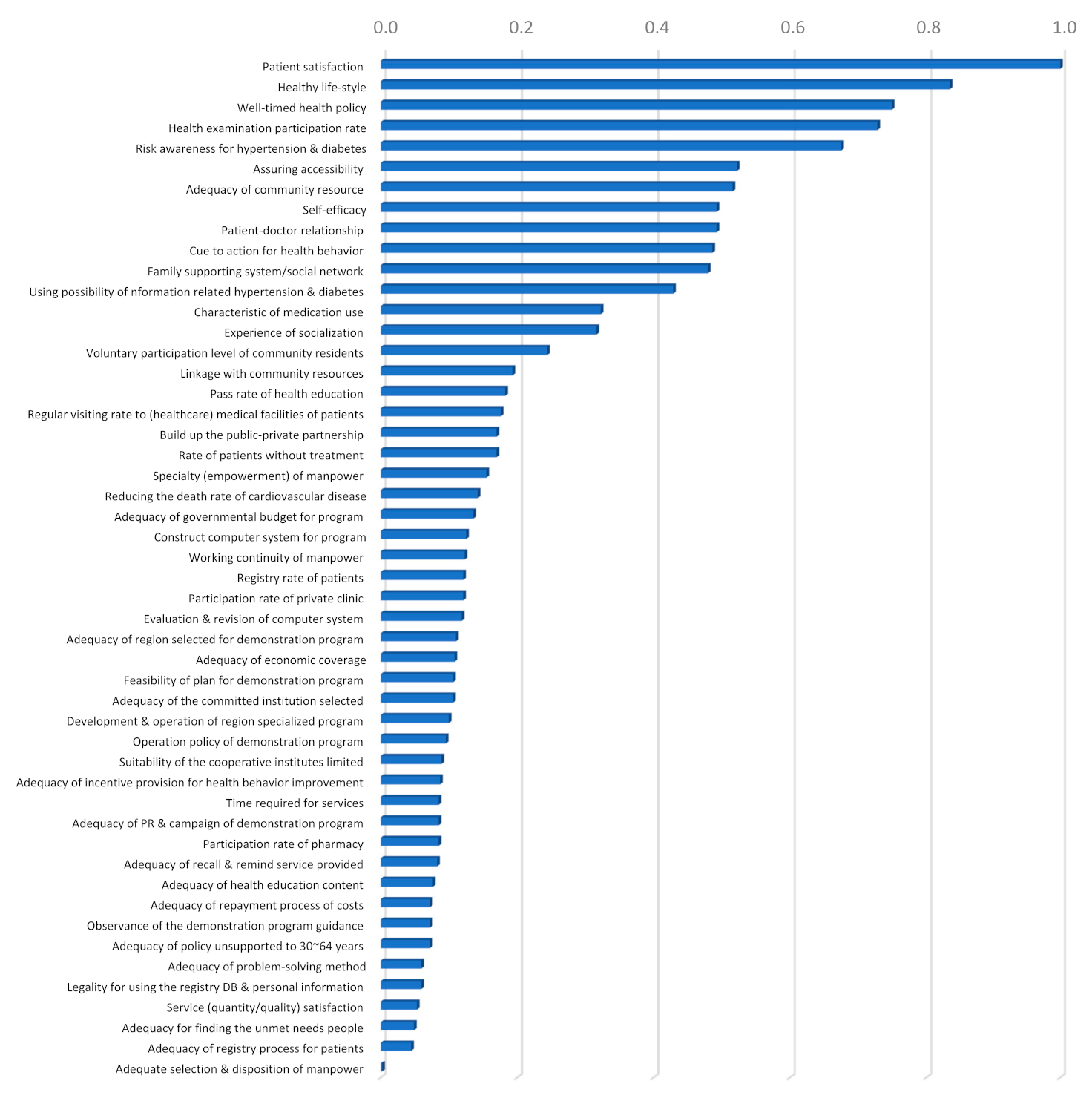
3.4. Comparison of Alternative Preference and Priorities Gap According to Evaluation Criteria
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Charlson, F.; Davis, A.; Degenhardt, L.; Dicker, D. Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- Naghavi, M.; Wang, H.; Lozano, R.; Davis, A.; Liang, X.; Zhou, M.; Vollset, S.E.; Ozgoren, A.A.; Abdalla, S.; Abd-Allah, F. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar] [CrossRef]
- Alwan, A.; Maclean, D.R.; Riley, L.M.; d’Espaignet, E.T.; Mathers, C.D.; Stevens, G.A.; Bettcher, D. Monitoring and surveillance of chronic non-communicable diseases: Progress and capacity in high-burden countries. Lancet 2010, 376, 1861–1868. [Google Scholar] [CrossRef]
- Mathers, C.D. History of global burden of disease assessment at the World Health Organization. Arch. Public Health 2020, 78, 77. [Google Scholar] [CrossRef] [PubMed]
- Huang, I.; Lim, M.A.; Pranata, R. Diabetes mellitus is associated with increased mortality and severity of disease in COVID-19 pneumonia: A systematic review, meta-analysis, and meta-regression. Diabetes Metab. Syndr. 2020, 14, 395–403. [Google Scholar] [CrossRef]
- Puska, P.; Koskela, K.; Pakarinen, H.; Puumalainen, P.; Soininen, V.; Tuomilehto, J. The North Karelia Project: A programme for community control of cardiovascular diseases. Scand. J. Soc. Med. 1976, 4, 57–60. [Google Scholar] [CrossRef]
- Nissinen, A.; Tuomilehto, J.; Elo, J.; Salonen, J.T.; Puska, P. Implementation of a hypertension control program in the county of North Karelia, Finland. Public Health Rep. 1981, 96, 503–513. [Google Scholar]
- Tuomilehto, J.; Piha, T.; Nissinen, A.; Geboers, J.; Puska, P. Trends in stroke mortality and in antihypertensive treatment in Finland from 1972 to 1984 with special reference to North Karelia. J. Hum. Hypertens. 1987, 1, 201–208. [Google Scholar]
- Puska, P.; Jaini, P. The North Karelia Project: Prevention of cardiovascular disease in Finland through population-based lifestyle interventions. Am. J. Lifestyle Med. 2020, 14, 495–499. [Google Scholar] [CrossRef]
- Wilber, J.A. The problem of undetected and untreated hypertension in the community. Bull. N. Y. Acad. Med. 1973, 49, 510–520. [Google Scholar]
- Tuomilehto, J.; Puska, P.; Virtamo, J.; Nissinen, A. Hypertension control in North Karelia before the intervention of the North Karelia Project. Scand. J. Soc. Med. 1980, 8, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Smith, W.C.; Lee, A.J.; Crombie, I.K.; Tunstall-Pedoe, H. Control of blood pressure in Scotland: The rule of halves. Br. Med. J. 1990, 300, 981–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques-Vidal, P.; Tuomilehto, J. Hypertension awareness, treatment and control in the community: Is the ‘rule of halves’ still valid? J. Hum. Hypertens. 1997, 11, 213–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.Y.; Lee, K.S.; Khang, Y.H.; Yim, J.; Choi, Y.J.; Lee, H.K.; Lee, K.H.; Kim, Y.I. Health behaviors related to hypertension in rural population of Korea. Korean J. Prev. Med. 2000, 33, 56–68. [Google Scholar]
- Korea Centers for Disease Control and Prevention. Rates of Hypertension Awareness, Treatment, and Control among Korean Adults Aged 30 Years and Over, 2007–2018. Public Health Wkly. Rep. 2020, 13, 1425–1428. Available online: http://www.kdca.go.kr/board/board.es?mid=a30501000000&bid=0031&list_no=367220&act=view# (accessed on 3 November 2020).
- World Health Organization. Innovative Care for Chronic Conditions: Building Blocks for Action. 2001. Available online: http://www.who.int/chp/knowledge/publications/icccreport/en/ (accessed on 10 November 2020).
- Rothman, A.A.; Wagner, E.H. Chronic illness management: What is the role of primary care? Ann. Intern. Med. 2003, 138, 256–261. [Google Scholar] [CrossRef]
- Wagner, E.H.; Austin, B.T.; Von Korff, M. Organizing care for patients with chronic illness. Milbank Q. 1996, 74, 511–544. [Google Scholar] [CrossRef]
- Reynolds, R.; Dennis, S.; Hasan, I.; Slewa, J.; Chen, W.; Tian, D.; Bobba, S.; Zwar, N. A systematic review of chronic disease management interventions in primary care. BMC Fam. Pract. 2018, 19, 11. [Google Scholar] [CrossRef]
- Lee, J.H.; Yang, D.H.; Park, H.S.; Cho, Y.; Jun, J.E.; Park, W.H.; Chun, B.Y.; Shin, J.Y.; Shin, D.H.; Lee, K.S.; et al. HYpertension-Diabetes Daegu Initiative Study Investigators. Incidence of hypertension in Korea: 5-year follow-up study. J. Korean Med. Sci. 2011, 26, 1286–1292. [Google Scholar] [CrossRef]
- Lee, H.J.; Lee, J.J.; Hwang, T.Y.; Kam, S. KHyDDI Project. Development and evaluation of a community staged education program for the cardiocerebrovascular disease high-risk patients. J. Agric. Med. Community Health 2012, 37, 167–180. [Google Scholar] [CrossRef] [Green Version]
- Korea Disease Control and Prevention Agency. Program for Prevention and Management for a Cardio-cerebrovascular Disease: Registration and Management Program for Hypertension/Diabetes. Available online: http://www.kdca.go.kr/contents.es?mid=a30335000000 (accessed on 30 November 2020).
- Lee, S.Y. Community based strategies and directions for the management of hypertension and diabetes. Korean J. Health Educ. Promot. 2016, 33, 67–77. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.S.; Lee, K.S.; Lee, J.J.; Hwang, T.Y.; Lee, J.Y.; Yoo, W.S.; Kim, K.Y.; Kim, S.K.; Kim, J.Y.; Park, K.S.; et al. Directions and current issues on the policy of prevention and management for hypertension and diabetes, and development of chronic disease prevention and management model in Korea. J. Agric. Med. Community Health 2020, 45, 13–40. [Google Scholar] [CrossRef]
- Kwon, S. Thirty years of national health insurance in South Korea: Lessons for achieving universal health care coverage. Health Policy Plan. 2009, 24, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Do, N.; Oh, J.; Lee, J.S. Moving toward universal coverage of health insurance in Vietnam: Barriers, facilitating factors, and lessons from Korea. J. Korean Med. Sci. 2014, 29, 919–925. [Google Scholar] [CrossRef]
- Ranabhat, C.L.; Jakovljevic, M.; Dhimal, M.; Kim, C.B. Structural factors responsible for universal health coverage in low- and middle-income countries: Results from 118 countries. Front. Public Health 2020, 7, 414. [Google Scholar] [CrossRef] [Green Version]
- Sohn, H.S.; Jang, S.; Lee, J.Y.; Han, E. Patient response to insurer-led intervention for medication adherence—A pilot study based on claims data in Korea. Int. J. Clin. Pharmacol. Ther. 2016, 54, 28–35. [Google Scholar] [CrossRef]
- Kim, H.S.; Suh, Y.; Kim, M.S.; Yoo, B.N.; Lee, E.J.; Lee, E.W.; Park, J.H. Effects of community-based primary care management on patients with hypertension and diabetes. Asia Pac. J. Public Health 2019, 31, 522–535. [Google Scholar] [CrossRef]
- Lee, H.Y.; Hahm, M.I.; Choi, K.S.; Jun, J.K.; Suh, M.; Nam, C.M.; Park, E.C. Different socioeconomic inequalities exist in terms of the prevention, diagnosis and control of diabetes. Eur. J. Public Health 2015, 25, 961–965. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.Y. Socioeconomic disparities in the prevalence, diagnosis, and control of hypertension in the context of a universal health insurance system. J. Korean Med. Sci. 2017, 32, 561–567. [Google Scholar] [CrossRef] [Green Version]
- Warren, J.R.; Falster, M.O.; Tran, B.; Jorm, L. Association of continuity of primary care and statin adherence. PLoS ONE 2015, 10, e0140008. [Google Scholar] [CrossRef] [Green Version]
- Citro, R.; Ghosh, S.; Churgin, P.G. Modeling and evaluation of continuity of care in a staff model HMO. MD Comput. 1998, 15, 298–306. [Google Scholar] [PubMed]
- Gulliford, M.; Naithani, S.; Morgan, M. What is ‘continuity of care’? J. Health Serv. Res. Policy 2006, 11, 248–250. [Google Scholar] [CrossRef] [PubMed]
- Naithani, S.; Gulliford, M.; Morgan, M. Patients’ perceptions and experiences of ‘continuity of care’ in diabetes. Health Expect. 2006, 9, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Smith-Rohrberg Maru, D.; Khakha, D.C.; Tahir, M.; Basu, S.; Sharma, S.K. Poor follow-up rates at a self-pay northern Indian tertiary AIDS clinic. Int. J. Equity Health 2007, 6, 14. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.A.; Kim, E.S.; Lee, E.K. Evaluation of the chronic disease management program for appropriateness of medication adherence and persistence in hypertension and type-2 diabetes patients in Korea. Medicine 2017, 96, e6577. [Google Scholar] [CrossRef]
- World Health Organization. The World Health Report 2008: Primary Health Care—Now More Than Ever; World Health Organization: Geneva, Switzerland, 2008; pp. 41–60. Available online: https://www.who.int/whr/2008/en/ (accessed on 14 December 2020).
- Sung, N.J.; Choi, Y.J.; Lee, J.H. Primary care comprehensiveness can reduce emergency department visits and hospitalization in people with hypertension in South Korea. Int. J. Environ. Res. Public Health 2018, 15, 272. [Google Scholar] [CrossRef] [Green Version]
- Saaty, T.L. Multicriteria Decision Making: The Analytic Hierarchy Process: Planning, Priority Setting, Resource Allocation, 1st ed.; McGraw-Hill: Pittsburgh, PA, USA, 1980. [Google Scholar]
- Saaty, T.L.; Wong, M.M. Projecting average family size in rural India by the analytic hierarchy process. J. Math. Sociol. 1983, 9, 181–209. [Google Scholar] [CrossRef]
- Saaty, T.L. Decision making with the analytic hierarchy process. Int. J. Serv. Sci. 2008, 1, 83–98. [Google Scholar] [CrossRef] [Green Version]
- Hannan, E.L.; O’Donnell, J.; Freedland, T. A priority assignment model for standards and conditions in a long term care survey. Socioecon. Plann. Sci. 1981, 15, 277–289. [Google Scholar] [CrossRef]
- Weingarten, M.S.; Erlich, F.; Nydick, R.L.; Liberatore, M.J. A pilot study of the use of the analytic hierarchy process for the selection of surgery residents. Acad. Med. 1997, 72, 400–402. [Google Scholar] [CrossRef]
- Hariharan, S.; Dey, P.K.; Chen, D.R.; Moseley, H.S.L.; Kumar, A.Y. Application of analytic hierarchy process for measuring and comparing the global performance of intensive care units. J. Crit. Care 2005, 20, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Shin, T.; Kim, C.B.; Ahn, Y.H.; Kim, H.Y.; Cha, B.H.; Uh, Y.; Lee, J.H.; Hyun, S.J.; Lee, D.H.; Go, U.Y. The comparative evaluation of expanded national immunization policies in Korea using an analytic hierarchy process. Vaccine 2009, 27, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Dolan, J.G. Multi-criteria clinical decision support: A primer on the use of multiple criteria decision making methods to promote evidence-based, patient-centered healthcare. Patient 2010, 3, 229–248. [Google Scholar] [CrossRef] [PubMed]
- Mühlbacher, A.C.; Juhnke, C. Patient preferences versus physicians’ judgement: Does it make a difference in healthcare decision making? Appl. Health Econ. Health Policy 2013, 11, 163–180. [Google Scholar] [CrossRef] [PubMed]
- Hashemian, M.; Ghardashi, F.; Izadi, A.R.; Akbarzadeh, R. Prioritizing the health education needs based on community participation: AHP method. J. Educ. Health Promot. 2019, 8, 127. [Google Scholar] [CrossRef]
- Nasiri, T.; Bahadori, M.; Ravangard, R.; Meskarpour Amiri, M. Factors affecting the failure to report medical errors by nurses using the analytical hierarchy process (AHP). Hosp. Top. 2020, 98, 135–144. [Google Scholar] [CrossRef]
- Schmidt, K.; Aumann, I.; Hollander, I.; Damm, K.; von der Schulenburg, J.M. Applying the analytic hierarchy process in healthcare research: A systematic literature review and evaluation of reporting. BMC Med. Inform. Decis. Mak. 2015, 15, 112. [Google Scholar] [CrossRef] [Green Version]
- Liberatore, M.J.; Nydick, R.L. The analytic hierarchy process in medical and health care decision making: A literature review. Eur. J. Oper. Res. 2008, 189, 194–207. [Google Scholar] [CrossRef]
- Becker, M.H.; Drachman, R.H.; Kirscht, J.P. A new approach to explaining sick-role behavior in low-income populations. Am. J. Public Health 1974, 64, 205–216. [Google Scholar] [CrossRef] [Green Version]
- Aday, L.A.; Andersen, R. A framework for the study of access to medical care. Health Serv. Res. 1974, 9, 208–220. [Google Scholar]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Cockerham, W.C. Health lifestyle theory and the convergence of agency and structure. J. Health Soc. Behav. 2005, 46, 51–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.C.; Kim, J.T.; Kim, J.S.; Sim, J.Y.; Lee, H.R.; Jo, H.S. Medication compliance in the elderly and the factors associated with compliance. Korean J. Fam. Med. 1999, 20, 1216–1223. [Google Scholar]
- Hu, H.; Liang, W.; Liu, M.; Li, L.; Li, Z.; Li, T.; Wang, J.; Shi, T.; Han, S.; Su, M.; et al. Establishment and evaluation of a model of a community health service in an underdeveloped area of China. Public Health 2010, 124, 206–217. [Google Scholar] [CrossRef]
- Overland, J.; Yue, D.K.; Mira, M. Continuity of care in diabetes: To whom does it matter? Diabetes Res. Clin. Pract. 2001, 52, 55–61. [Google Scholar] [CrossRef]
- Ferraretto, F.; Salmaso, D.; Pegoraro, C. Continuity of care: Community care in Italy and Sweden—A comparison. Prof. Inferm. 2005, 58, 80–82. [Google Scholar]
- Menec, V.H.; Sirski, M.; Attawar, D. Does continuity of care matter in a universally insured population? Health Serv. Res. 2005, 40, 389–400. [Google Scholar] [CrossRef] [Green Version]
- Alazri, M.H.; Heywood, P.; Neal, R.D.; Leese, B. UK GPs’ and practice nurses’ views of continuity of care for patients with type 2 diabetes. Fam. Pract. 2007, 24, 128–137. [Google Scholar] [CrossRef]
- Chen, C.C.; Chen, S.H. Better continuity of care reduces costs for diabetic patients. Am. J. Manag. Care 2011, 17, 420–427. [Google Scholar]
- Raivio, R.; Jääskeläinen, J.; Holmberg-Marttila, D.; Mattila, K.J. Decreasing trends in patient satisfaction, accessibility and continuity of care in Finnish primary health care—A 14-year follow-up questionnaire study. BMC Fam. Pract. 2014, 15, 98. [Google Scholar] [CrossRef] [Green Version]
- Shin, D.W.; Cho, J.; Yang, H.K.; Park, J.H.; Lee, H.; Kim, H.; Oh, J.; Hwang, S.; Cho, B.; Guallar, E. Impact of continuity of care on mortality and health care costs: A nationwide cohort study in Korea. Ann. Fam. Med. 2014, 12, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Orleans, C.T.; Wagner, E.H. Does the chronic care model serve also as a template for improving prevention? Milbank Q. 2001, 79, 579–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, E.H.; Glasgow, R.E.; Davis, C.; Bonomi, A.E.; Provost, L.; McCulloch, D.; Carver, P.; Sixta, C. Quality improvement in chronic illness care: A collaborative approach. Jt. Comm. J. Qual. Improv. 2001, 27, 63–80. [Google Scholar] [CrossRef]
- Bodenheimer, T.; Wagner, E.H.; Grumbach, K. Improving primary care for patients with chronic illness: The chronic care model, part 2. JAMA 2002, 288, 1909–1914. [Google Scholar] [CrossRef] [PubMed]
- Margetts, B. Feedback on WHO/FAO global report on diet, nutrition and prevention of chronic diseases (NCD). Public Health Nutr. 2003, 6, 423–424. [Google Scholar] [CrossRef] [PubMed]
- Hariharan, S.; Dey, P.K.; Moseley, H.S.L.; Kumar, A.Y.; Gora, J. A new tool for measurement of process-based performance of multispecialty tertiary care hospitals. Int. J. Health Care Qual. Assur. Inc. Leadersh. Health Serv. 2004, 17, 302–312. [Google Scholar] [CrossRef]
- Expertchoice® for Collaboration Decision Making. Expert Choice Desktop for Academy (EC). Available online: https://www.expertchoice.com/analytic-hierarchy-process-experts (accessed on 10 October 2020).
- Adunlin, G.; Diaby, V.; Xiao, H. Application of multicriteria decision analysis in health care: A systematic review and bibliometric analysis. Health Expect. 2015, 18, 1894–1905. [Google Scholar] [CrossRef] [Green Version]
- Hughes, C.M. Medication non-adherence in the elderly: How big is the problem? Drugs Aging 2004, 21, 793–811. [Google Scholar] [CrossRef]
- Murray, M.D.; Morrow, D.G.; Weiner, M.; Clark, D.O.; Tu, W.; Deer, M.M.; Brater, D.C.; Weinberger, M. A conceptual framework to study medication adherence in older adults. Am. J. Geriatr. Pharmacother. 2004, 2, 36–43. [Google Scholar] [CrossRef]
- Gellad, W.F.; Grenard, J.L.; Marcum, Z.A. A systematic review of barriers to medication adherence in the elderly: Looking beyond cost and regimen complexity. Am. J. Geriatr. Pharmacother. 2011, 9, 11–23. [Google Scholar] [CrossRef] [Green Version]
- Gosmanova, E.O.; Lu, J.L.; Streja, E.; Cushman, W.C.; Kalantar-Zadeh, K.; Kovesdy, C.P. Association of medical treatment nonadherence with all-cause mortality in newly treated hypertensive US veterans. Hypertension 2014, 64, 951–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, A.; Breton, M.; Loslier, J. Providing continuity of care to a specific population: Attracting new family physicians. Can. Fam. Physician 2016, 62, e256–e262. [Google Scholar] [PubMed]
- Byun, D.H.; Kim, E.J.; Park, M.B.; Son, H.R.; Park, H.K.; Kim, C.B. Accessible strategy of the registration & management of hypertension and diabetes mellitus patients through the public-private partnership: Policy implications from the Hongcheon-gun Case. Korean J. Health Educ. Promot. 2013, 30, 111–123. [Google Scholar] [CrossRef] [Green Version]
- Son, K.J.; Son, H.R.; Park, B.; Kim, H.J.; Kim, C.B. A community-based intervention for improving medication adherence for elderly patients with hypertension in Korea. Int. J. Environ. Res. Public Health 2019, 16, 721. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.B.; Chung, M.K. Primary Health Care: Tikapur Nepal Meets Ganghwa Republic of Korea!—The Link and Performance of International and Regional Development, 1st ed.; Pakyoungsa: Seoul, Korea, 2019. [Google Scholar]
- Mühlbacher, A.C.; Bethge, S.; Kaczynski, A.; Juhnke, C. Objective criteria in the medicinal therapy for Type II Diabetes: An analysis of the patients’ perspective with analytic hierarchy process and best-worst scaling. Gesundheitswesen 2016, 78, 326–336. [Google Scholar] [CrossRef]
- Dintsios, C.M.; Chernyak, N.; Grehl, B.; Icks, A. Quantified patient preferences for lifestyle intervention programs for diabetes prevention—A protocol for a systematic review. Syst. Rev. 2018, 7, 214. [Google Scholar] [CrossRef] [Green Version]
- Youngkong, S.; Baltussen, R.; Tantivess, S.; Mohara, A.; Teerawattananon, Y. Multicriteria decision analysis for including health interventions in the universal health coverage benefit package in Thailand. Value Health 2012, 15, 961–970. [Google Scholar] [CrossRef] [Green Version]
- Marsh, K.; Dolan, P.; Kempster, J.; Lugon, M. Prioritizing investments in public health: A multi-criteria decision analysis. J. Public Health 2013, 35, 460–466. [Google Scholar] [CrossRef] [Green Version]
- Ham, C. The ten characteristics of the high-performing chronic care system. Health Econ. Policy Law 2010, 5 Pt 1, 71–90. [Google Scholar] [CrossRef] [Green Version]
- Shahaj, O.; Denneny, D.; Schwappach, A.; Pearce, G.; Epiphaniou, E.; Parke, H.L.; Taylor, S.J.C.; Pinnock, H. Supporting self-management for people with hypertension: A meta-review of quantitative and qualitative systematic reviews. J. Hypertens. 2019, 37, 264–279. [Google Scholar] [CrossRef]
- Fletcher, B.R.; Hinton, L.; Hartmann-Boyce, J.; Roberts, N.W.; Bobrovitz, N.; McManus, R.J. Self-monitoring blood pressure in hypertension, patient and provider perspectives: A systematic review and thematic synthesis. Patient Educ. Couns. 2016, 99, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Wagner, E.H.; Austin, B.T.; Davis, C.; Hindmarsh, M.; Schaefer, J.; Bonomi, A. Improving chronic illness care: Translating evidence into action. Health Aff. 2001, 20, 64–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gholamzadeh Nikjoo, R.; Jabbari Beyrami, H.; Jannati, A.; Asghari Jaafarabadi, M. Prioritizing public-private partnership models for public hospitals of Iran based on performance indicators. Health Promot. Perspect. 2012, 2, 251–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, D.; Wang, G.; Joo, H. A systematic review of economic evidence on community hypertension interventions. Am. J. Prev. Med. 2017, 53, S121–S130. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Category | AHP Survey Participants | Valid Respondents * | ||
|---|---|---|---|---|---|
| No. | % | No. | % | ||
| Sex | Male | 17 | 12.8 | 12 | 17.1 |
| Female | 116 | 87.2 | 58 | 82.9 | |
| Age group | 20–29 | 20 | 15.0 | 14 | 20.0 |
| 30–39 | 56 | 42.1 | 32 | 45.7 | |
| 40–49 | 39 | 29.3 | 17 | 24.3 | |
| 50–59 | 17 | 12.8 | 6 | 8.6 | |
| 60+ | 1 | 0.8 | 1 | 1.4 | |
| Education level | Bachelor | 97 | 72.9 | 54 | 77.1 |
| Master | 14 | 10.5 | 6 | 8.6 | |
| Ph.D. | 13 | 9.8 | 6 | 8.6 | |
| Others | 9 | 6.8 | 4 | 5.7 | |
| Major | Medicine | 10 | 7.5 | 6 | 8.6 |
| Nursing | 72 | 54.1 | 41 | 58.6 | |
| Nutrition | 30 | 22.6 | 14 | 20.0 | |
| Athletics | 5 | 3.8 | 4 | 5.7 | |
| Public health | 3 | 2.3 | 0 | 0.0 | |
| Others | 13 | 9.8 | 5 | 7.1 | |
| Work place | University | 15 | 11.3 | 11 | 15.7 |
| HyDiREC | 78 | 58.6 | 45 | 64.3 | |
| Health Center | 40 | 30.1 | 14 | 20.0 | |
| Total | 133 | 100.0 | 70 | 100.0 | |
| First Sub-Criteria | Third Sub-Criteria | Mean Score | Rank |
|---|---|---|---|
| Health behavior | Risk awareness for hypertension & diabetes (likelihood/severity) | 6.23 | 2 |
| Cue to action for health behavior | 5.99 | 4 | |
| Self-efficacy | 5.80 | 6 | |
| Experience of socialization | 5.39 | 14 | |
| Healthy life-style (anti-smoking, reducing alcohol, nutrition, physical activities) | 6.26 | 1 | |
| Health examination participation rate (blood pressure/glucose test) | 6.14 | 3 | |
| Behavior of health care utilization | Characteristic of medication use (dosage, frequency, drug form) | 5.68 | 10 |
| Family supporting system/social network | 5.62 | 11 | |
| Patient-doctor relationship (family doctor etc.) | 5.55 | 13 | |
| Using possibility of information related hypertension & diabetes | 5.62 | 11 | |
| Assuring accessibility (economic/geographic/psychologic) | 5.73 | 8 | |
| Adequacy of community resource (workforce and facilities, delivery system) | 5.70 | 9 | |
| Well-timed health policy | 5.77 | 7 | |
| Patient satisfaction | 5.99 | 4 |
| First Sub-Criteria | Second Sub-Criteria | Third Sub-Criteria | Mean Score | Rank |
|---|---|---|---|---|
| Program infrastructure | Investment resources for building infrastructure | Feasibility of plan for demonstration program | 5.89 | 16 |
| Adequacy of governmental budget for program | 5.96 | 11 | ||
| Construct computer system for program | 6.00 | 9 | ||
| Adequacy of region selected for demonstration program | 5.53 | 28 | ||
| Adequacy of the committed institution selected | 5.47 | 30 | ||
| Suitability of the cooperative institutes limited | 5.37 | 36 | ||
| Participation system within community | Operation policy of demonstration program | 5.53 | 28 | |
| Build up the public-private partnership | 5.95 | 12 | ||
| Voluntary participation level of community residents | 6.06 | 6 | ||
| Linkage with community resources | 6.01 | 8 | ||
| Program process | Adequacy of center operation & service provided | Adequate selection & disposition of manpower | 6.18 | 4 |
| Working continuity of manpower | 6.23 | 2 | ||
| Specialty (empowerment) of manpower | 6.27 | 1 | ||
| Time required for services (counselling/repayment cost) | 5.66 | 21 | ||
| Adequacy of health education content (disease, nutrition, exercise) | 6.19 | 3 | ||
| Adequacy of recall & remind service provided | 5.64 | 23 | ||
| Adequacy of PR & campaign of demonstration program | 5.75 | 19 | ||
| Adequacy of incentive provision for health behavior improvement | 5.47 | 30 | ||
| Development & operation of region specialized program | 5.73 | 20 | ||
| Evaluation & revision of computer system | 5.92 | 15 | ||
| Adequacy of administrative procedures | Adequacy of registry process for patients | 5.62 | 24 | |
| Adequacy for finding the unmet needs people | 5.40 | 35 | ||
| Adequacy of problem-solving method | 5.56 | 26 | ||
| Legality for using the registry DB & personal information | 5.55 | 27 | ||
| Adequacy of repayment process of costs | 5.43 | 33 | ||
| Observance of the demonstration program guidance | 5.42 | 34 | ||
| Program outcome | Program output | Registry rate of patients | 5.60 | 25 |
| Regular visiting rate to (healthcare) medical facilities of patients | 5.83 | 17 | ||
| Rate of patients without treatment | 5.80 | 18 | ||
| Pass rate of health education (disease, nutrition, exercise) | 5.66 | 21 | ||
| Program performance | Service (quantity/quality) satisfaction | 5.95 | 12 | |
| Participation rate of private clinic | 6.17 | 5 | ||
| Participation rate of pharmacy | 6.03 | 7 | ||
| Adequacy of economic coverage (medical fee + drug cost) | 5.93 | 14 | ||
| Adequacy of policy unsupported to 30~64 years | 5.44 | 32 | ||
| Reducing the death rate of cardiovascular diseases (long-term effect) | 5.99 | 10 |
| Main Criteria | First Sub-Criteria | Second Sub-Criteria | Third Sub-Criteria | Priorities (Global Weights) | Importance Rank |
|---|---|---|---|---|---|
| Approach strategy for patients (individual level) (Global weight: 0.525, Importance rank: 1) | Health behavior (Global weight: 0.391, Importance rank: 2) | - | Risk awareness for hypertension & diabetes (likelihood/severity) | 0.0318 | 5 |
| Cue to action for health behavior | 0.0229 | 10 | |||
| Self-efficacy | 0.0232 | 8 | |||
| Experience of socialization | 0.0149 | 14 | |||
| Healthy life-style (anti-smoking, reducing alcohol, nutrition, physical activities) | 0.0393 | 2 | |||
| Health examination participation rate (blood pressure/glucose test) | 0.0343 | 4 | |||
| Behavior of health care utilization (Global weight: 0.461, Importance rank: 1) | - | Characteristic of medication use (dosage, frequency, drug form) | 0.0152 | 13 | |
| Family supporting system/social network | 0.0226 | 11 | |||
| Patient-doctor relationship (family doctor etc.) | 0.0232 | 8 | |||
| Using possibility of information related hypertension & diabetes | 0.0202 | 12 | |||
| Assuring accessibility (economic/geographic/psychologic) | 0.0246 | 6 | |||
| Adequacy of community resource (workforce and facilities, delivery system) | 0.0243 | 7 | |||
| Well-timed health policy | 0.0353 | 3 | |||
| Patient satisfaction | 0.0471 | 1 | |||
| Approach strategy for healthcare system (community level) (Global weight: 0.332, Importance rank: 2) | Program infrastructure (Global weight: 0.295, Importance rank: 1) | Investment resources for building infrastructure (Global weight: 0.420, Importance rank: 2) | Feasibility of plan for demonstration program | 0.0050 | 31 |
| Adequacy of governmental budget for program | 0.0064 | 23 | |||
| Construct computer system for program | 0.0059 | 24 | |||
| Adequacy of region selected for demonstration program | 0.0052 | 29 | |||
| Adequacy of the committed institution selected | 0.0050 | 31 | |||
| Suitability of the cooperative institutes limited | 0.0042 | 35 | |||
| Participation system within community (Global weight: 0.436, Importance rank: 1) | Operation policy of demonstration program | 0.0045 | 34 | ||
| Build up the public-private partnership | 0.0080 | 19 | |||
| Voluntary participation level of community residents | 0.0115 | 15 | |||
| Linkage with community resources | 0.0091 | 16 | |||
| Program process (Global weight: 0.272, Importance rank: 2) | Adequacy of center operation & service provided (Global weight: 0.672, Importance rank: 1) | Adequate selection & disposition of manpower | 0.0001 | 50 | |
| Working continuity of manpower | 0.0058 | 25 | |||
| Specialty (empowerment) of manpower | 0.0073 | 21 | |||
| Time required for services (counselling/repayment cost) | 0.0040 | 37 | |||
| Adequacy of health education content (disease, nutrition, exercise) | 0.0036 | 41 | |||
| Adequacy of recall & remind service provided | 0.0039 | 40 | |||
| Adequacy of PR & campaign of demonstration program | 0.0040 | 37 | |||
| Adequacy of incentive provision for health behavior improvement | 0.0041 | 36 | |||
| Development & operation of region specialized program | 0.0047 | 33 | |||
| Evaluation & revision of computer system | 0.0056 | 28 | |||
| Adequacy of administrative procedures (Global weight: 0.249, Importance rank: 2) | Adequacy of registry process for patients | 0.0021 | 49 | ||
| Adequacy for finding the unmet needs people | 0.0023 | 48 | |||
| Adequacy of problem-solving method | 0.0028 | 45 | |||
| Legality for using the registry DB & personal information | 0.0028 | 45 | |||
| Adequacy of repayment process of costs | 0.0034 | 42 | |||
| Observance of the demonstration program guidance | 0.0034 | 42 | |||
| Program outcome (Global weight: 0.248, Importance rank: 3) | Program output (Global weight: 0.453, Importance rank: 1) | Registry rate of patients | 0.0057 | 26 | |
| Regular visiting rate to (healthcare) medical facilities of patients | 0.0083 | 18 | |||
| Rate of patients without treatment | 0.0080 | 19 | |||
| Pass rate of health education (disease, nutrition, exercise) | 0.0086 | 17 | |||
| Program performance (Global weight: 0.430, Importance rank: 2) | Service (quantity/quality) satisfaction | 0.0025 | 47 | ||
| Participation rate of private clinic | 0.0057 | 26 | |||
| Participation rate of pharmacy | 0.0040 | 37 | |||
| Adequacy of economic coverage (medical fee + drug cost) | 0.0051 | 30 | |||
| Adequacy of policy unsupported to 30~64 years | 0.0034 | 42 | |||
| Reducing the death rate of cardiovascular diseases (long-term effect) | 0.0067 | 22 |
| Alternative Policy | Priorities (Alternative Preference) |
|---|---|
| Improvement for treatment compliance | 0.550 |
| Enhancement for continuity of care | 0.396 |
| Level | Evaluation Criteria | Improvement for Treatment Compliance | Enhancement for Continuity of Care | Gap |
|---|---|---|---|---|
| Main criteria | Approach strategy for patients | 0.3719 | 0.2246 | 0.1473 |
| Approach strategy for healthcare system | 0.1990 | 0.2011 | −0.0021 | |
| First sub-criteria | Health behavior | 0.1779 | 0.0950 | 0.0829 |
| Behavior of health care utilization | 0.1940 | 0.1296 | 0.0644 | |
| Program infrastructure | 0.0633 | 0.0726 | −0.0093 | |
| Program process | 0.0691 | 0.0785 | −0.0094 | |
| Program outcome | 0.0734 | 0.0539 | 0.0195 | |
| Second sub-criteria | Investment resources for building infrastructure | 0.0434 | 0.0313 | 0.0121 |
| Participation system within community | 0.0320 | 0.0302 | 0.0018 | |
| Adequacy of center operation & service provided | 0.0276 | 0.0450 | −0.0174 | |
| Adequacy of administrative procedures | 0.0173 | 0.0460 | −0.0287 | |
| Program output | 0.0323 | 0.0216 | 0.0107 | |
| Program performance | 0.0382 | 0.0352 | 0.0030 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byun, D.H.; Chang, R.S.; Park, M.-B.; Son, H.-R.; Kim, C.-B. Prioritizing Community-Based Intervention Programs for Improving Treatment Compliance of Patients with Chronic Diseases: Applying an Analytic Hierarchy Process. Int. J. Environ. Res. Public Health 2021, 18, 455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020455
Byun DH, Chang RS, Park M-B, Son H-R, Kim C-B. Prioritizing Community-Based Intervention Programs for Improving Treatment Compliance of Patients with Chronic Diseases: Applying an Analytic Hierarchy Process. International Journal of Environmental Research and Public Health. 2021; 18(2):455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020455
Chicago/Turabian StyleByun, Do Hwa, Rho Soon Chang, Myung-Bae Park, Hyo-Rim Son, and Chun-Bae Kim. 2021. "Prioritizing Community-Based Intervention Programs for Improving Treatment Compliance of Patients with Chronic Diseases: Applying an Analytic Hierarchy Process" International Journal of Environmental Research and Public Health 18, no. 2: 455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020455