Analyzing the Magnitude of Interlimb Asymmetries in Young Female Soccer Players: A Preliminary Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.2.1. Jumping Performance Tests
2.2.2. Change of Direction Ability (CODA)
2.2.3. Passive Range of Motion (ROM) Tests
2.2.4. Muscle Mass via Dual-Energy X-ray Absorptiometry (DXA)
2.3. Statistical Analysis
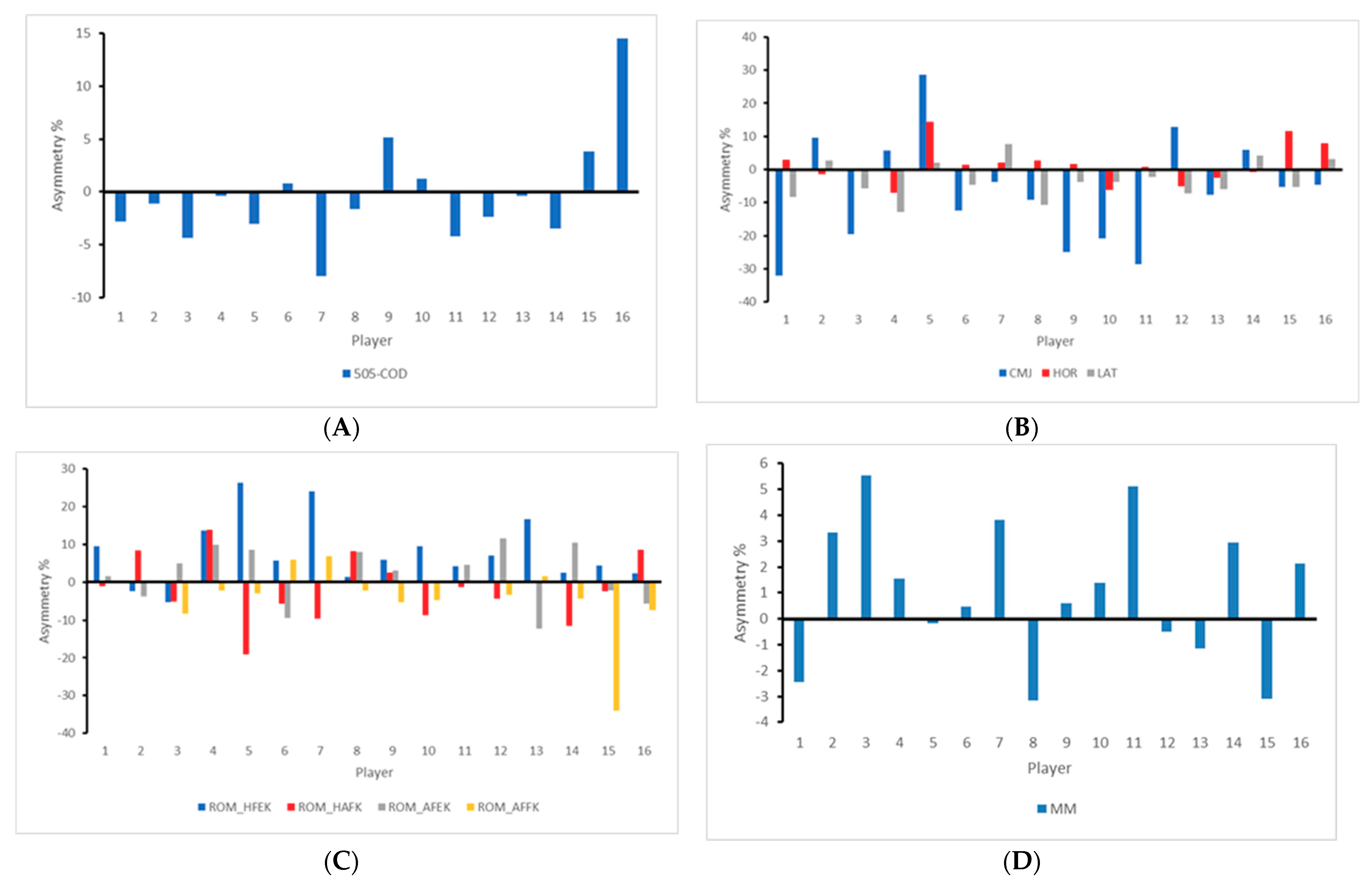
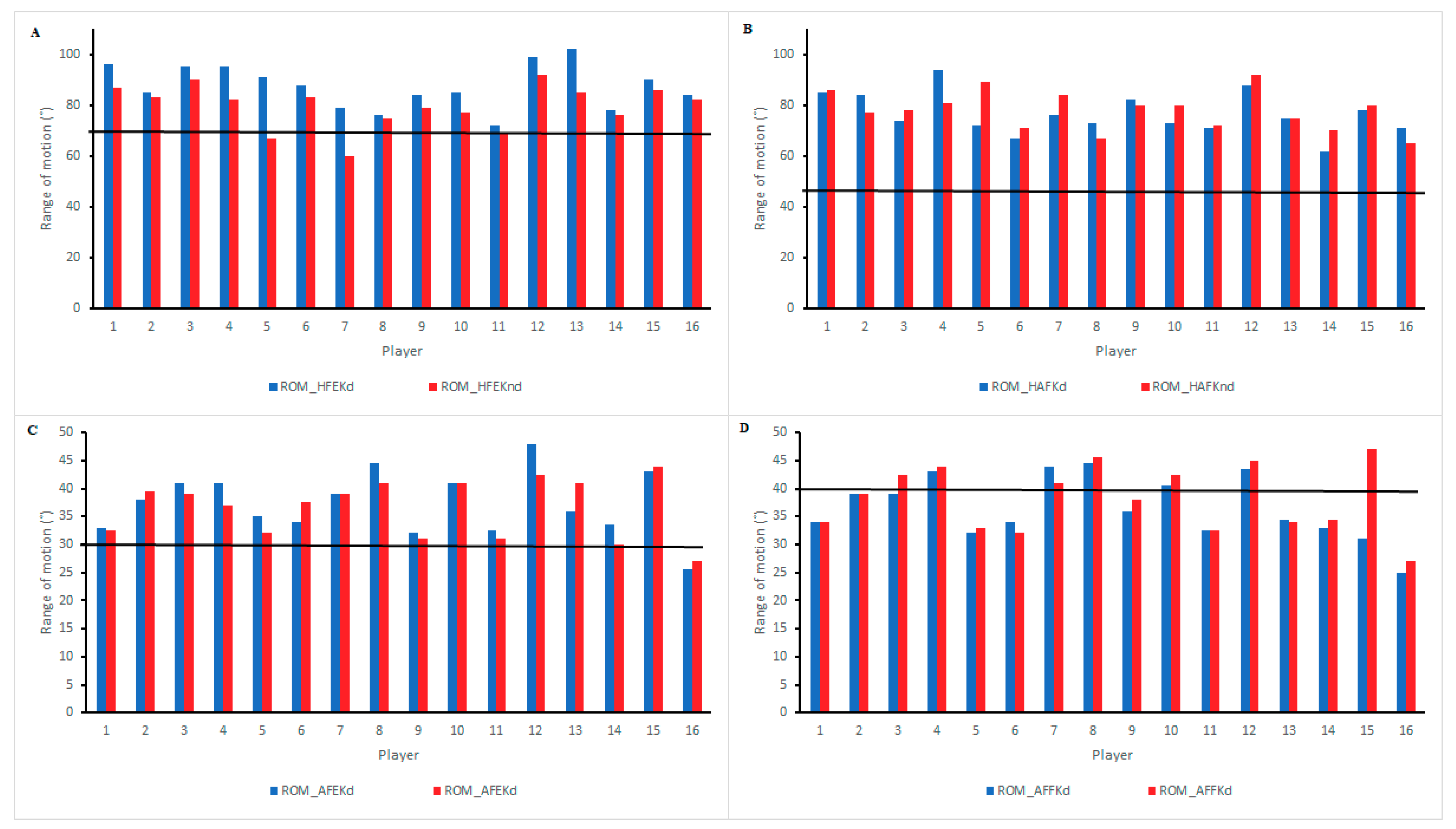
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Afonso, J.; Bessa, C.; Pinto, F.; Ribeiro, D.; Moura, B.; Rocha, T.; Vinícius, M.; Canário-Lemos, R.; Clemente, F.M. Structural and functional asymmetries in humans. In Asymmetry as a Foundational and Functional Requirement in Human Movement; Springer: Singapore, 2020; pp. 9–16. [Google Scholar]
- Ueberschär, O.; Fleckenstein, D.; Warschun, F.; Kränzler, S.; Walter, N.; Hoppe, M.W. Measuring biomechanical loads and asymmetries in junior elite long-distance runners through triaxial inertial sensors. Sport. Orthop. Traumatol. 2019, 35, 296–308. [Google Scholar] [CrossRef]
- Fohanno, V.; Nordez, A.; Smith, R.; Colloud, F. Asymmetry in elite rowers: Effect of ergometer design and stroke rate. Sport Biomech. 2015, 14, 310–322. [Google Scholar] [CrossRef] [PubMed]
- Pajek, M.B.; Hedbávný, P.; Kalichová, M.; Čuk, I. The asymmetry of lower limb load in balance beam routines. Sci. Gymnast. J. 2016, 8, 5–13. [Google Scholar]
- Afonso, J.; Bessa, C.; Pinto, F.; Ribeiro, D.; Rocha, T.; Vinícius, M.; Canário-Lemos, R.; Peixoto, R.; Clemente, F.M. Asymmetries in Athletic Performance. In Asymmetry as a Foundational and Functional Requirement in Human Movement; Springer: Singapore, 2020; pp. 21–25. [Google Scholar]
- Azevedo, R.R.; Da Rocha, E.S.; Franco, P.S.; Carpes, F.P. Plantar pressure asymmetry and risk of stress injuries in the foot of young soccer players. Phys. Ther. Sport 2017, 24, 39–43. [Google Scholar] [CrossRef]
- Afonso, J.; Bessa, C.; Pinto, F.; Riberio, D.; Moura, B.; Rocha, T.; Vinícius, M.; Canário-Lemos, R.; Peixoto, R.; Clemente, F.M. Injury prevention: From symmetry to asymmetry, to critical thresholds. In Asymmetry as a Foundational and Functional Requirement in Human Movement; Springer: Singapore, 2020; pp. 27–31. [Google Scholar]
- Cejudo, A.; Sainz de Baranda, P.; Ayala, F.; Santonja, F. Test-retest reliability of seven common clinical tests for assessing lower extremity muscle flexibility in futsal and handball players. Phys. Ther. Sport 2015, 16, 107–113. [Google Scholar] [PubMed]
- Loturco, I.; Pereira, L.A.; Kobal, R.; Abad, C.C.C.; Rosseti, M.; Carpes, F.P.; Bishop, C. Do asymmetry scores influence speed and power performance in elite female soccer players? Biol. Sport 2019, 36, 209–216. [Google Scholar] [PubMed]
- Menzel, H.-J.; Chagas, M.H.; Szmuchrowski, L.A.; Araujo, S.R.S.; De Andrade, A.G.P.; De Jesus-Moraleida, F.R. Analysis of lower limb asymmetries by isokinetic and vertical jump tests in soccer players. J. Strength Cond. Res. 2013, 27, 1370–1377. [Google Scholar] [CrossRef]
- Bishop, C.; Read, P.; McCubbine, J.; Turner, A. Vertical and horizontal asymmetries are related to slower sprinting and jump performance in elite youth female soccer players. J. Strength Cond. Res. 2021, 35, 56–63. [Google Scholar]
- Coratella, G.; Beato, M.; Schena, F. Correlation between quadriceps and hamstrings inter-limb strength asymmetry with change of direction and sprint in U21 elite soccer-players. Hum. Mov. Sci. 2018, 59, 81–87. [Google Scholar]
- Raya-González, J.; Bishop, C.; Gómez-Piqueras, P.; Veiga, S.; Viejo-Romero, D.; Navandar, A. Strength, jumping, and change of direction speed asymmetries are not associated with athletic performance in elite academy soccer players. Front. Psychol. 2020, 11, 1–8. [Google Scholar]
- Bishop, C.; Turner, A.; Maloney, S.; Lake, J.; Loturco, I.; Bromley, T.; Read, P. Drop jump asymmetry is associated with reduced sprint and change-of-direction speed performance in adult female soccer players. Sports 2019, 7, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lockie, R.G.; Callaghan, S.J.; Berry, S.P.; Cooke, E.R.A.; Jordan, C.A.; Luczo, T.M.; Jeffriess, M.D. Relationship between unilateral jumping ability and asymmetry on multidirectional speed in team-sport athletes. J. Strength Cond. Res. 2014, 28, 3557–3566. [Google Scholar] [PubMed] [Green Version]
- Loturco, I.; Pereira, L.A.; Kobal, R.; Abad, C.C.C.; Komatsu, W.; Cunha, R.; Arliani, G.; Ejnisman, B.; de Castro Pochini, A.; Nakamura, F.Y.; et al. Functional screening tests: Interrelationships and ability to predict vertical jump performance. Int. J. Sports Med. 2018, 39, 189–197. [Google Scholar]
- Mokha, M.; Sprague, P.A.; Gatens, D.R. Predicting musculoskeletal injury in national collegiate athletic association division II athletes from asymmetries and individual-test versus composite functional movement screen scores. J. Athl. Train. 2016, 51, 276–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stiffler, M.R.; Bell, D.R.; Sanfilippo, J.L.; Hetzel, S.J.; Pickett, K.A.; Heiderscheit, B.C. Star excursion balance test anterior asymmetry is associated with injury status in division i collegiate athletes. J. Orthop. Sports Phys. Ther. 2017, 47, 339–346. [Google Scholar] [CrossRef]
- Zvijac, J.E.; Toriscelli, T.A.; Merrick, S.; Kiebzak, G.M. Isokinetic concentric quadriceps and hamstring strength variables from the NFL scouting combine are not predictive of hamstring injury in first-year professional football players. Am. J. Sports Med. 2013, 41, 1511–1518. [Google Scholar]
- Castillo, D.; Dominguez, R.; Rodriguez-Fernandez, A.; Raya-Gonzalez, J. Effects of caffeine supplementation on power performance in a flywheel device: A randomised, double-blind cross-over study. Nutrients 2019, 11, 255. [Google Scholar]
- Rohman, E.; Steubs, J.T.; Tompkins, M. Changes in involved and uninvolved limb function during rehabilitation after anterior cruciate ligament reconstruction: Implications for Limb Symmetry Index measures. Am. J. Sports Med. 2015, 43, 1391–1398. [Google Scholar]
- López-Valenciano, A.; Ayala, F.; Vera-García, F.J.; De Ste Croix, M.; Hernández-Sánchez, S.; Ruiz-Pérez, I.; Cejudo, A.; Santonja, F. Comprehensive profile of hip, knee and ankle ranges of motion in professional football players. J. Sports Med. Phys. Fitness 2019, 59, 102–109. [Google Scholar]
- Palmer, M.L.; Epler, M.E. Fundamentos de las Técnicas de Evaluación Musculoesquelética; Paidotribo: Barcelona, Spain, 2002. [Google Scholar]
- Gerhardt, J. Documentation of Joint Motion; Isomed: Portland, OR, USA, 1994. [Google Scholar]
- Norris, C.M. La Guía Completa de los Estiramientos; Paidotribo: Barcelona, Spain, 2004. [Google Scholar]
- Sáez de Villarreal, E.; Suarez-Arrones, L.; Requena, B.; Haff, G.G.; Ferrete, C. Effects of plyometric and sprint training on physical and technical skill performance in adolescent soccer players. J. Strength Cond. Res. 2015, 29, 1894–1903. [Google Scholar]
- Gonzalo-Skok, O.; Tous-Fajardo, J.; Arjol-Serrano, J.L.; Suarez-Arrones, L.; Antonio Casajús, J.; Mendez-Villanueva, A. Improvement of repeated-sprint ability and horizontal-jumping performance in elite young basketball players with low-volume repeated-maximal-power training. Int. J. Sports Physiol. Perform. 2016, 11, 464–473. [Google Scholar] [PubMed]
- Castillo, D.; Lago-Rodríguez, A.; Domínguez-Díez, M.; Sánchez-Díaz, S.; Rendo-Urteaga, T.; Soto-Célix, M.; Raya-González, J. Relationships between players’ physical performance and small-sided game external responses in a youth soccer training context. Sustainability 2020, 12, 4482. [Google Scholar]
- American Academy of Orthopaedic Surgeons. Joint Motion: Method of Measuring and Recording; Churchill Livingstone: London, UK, 1986. [Google Scholar]
- Furness, J.; Johnstone, S.; Hing, W.; Abbott, A.; Climstein, M. Assessment of shoulder active range of motion in prone versus supine: A reliability and concurrent validity study. Physiother. Theory Pract. 2015, 31, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nana, A.; Slater, G.J.; Hopkins, W.G.; Halson, S.L.; Martin, D.T.; West, N.P.; Burke, L.M. Importance of standardized DXA protocol for assessing physique changes in athletes. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 259–267. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar]
- Cormack, S.J.; Newton, R.U.; McGuigan, M.R.; Doyle, T.L.A. Reliability of measures obtained during single and repeated countermovement jumps. Int. J. Sports Physiol. Perform. 2008, 3, 131–144. [Google Scholar] [CrossRef] [Green Version]
- Impellizzeri, F.M.; Rampinini, E.; Maffiuletti, N.; Marcora, S.M. A vertical jump force test for assessing bilateral strength asymmetry in athletes. Med. Sci. Sports Exerc. 2007, 39, 2044–2050. [Google Scholar]
- Bishop, C.; Lake, J.; Loturco, I.; Papadopoulos, K.; Turner, A.; Read, P. Interlimb asymmetries: The need for an individual approach to data analysis. J. Strength Cond. Res. 2018, 1. [Google Scholar] [CrossRef]
- Bishop, C.; Brashill, C.; Abbott, W.; Read, P.; Lake, J.; Turner, A. Jumping asymmetries are associated with speed, change of direction speed, and jump performance in elite academy soccer players. J. Strength Cond. Res. 2019. [Google Scholar] [CrossRef]
- Pardos-Mainer, E.; Casajús, J.A.; Gonzalo-Skok, O. Adolescent female soccer players’ soccer-specific warm-up effects on performance and inter-limb asymmetries. Biol. Sport 2019, 36, 199–207. [Google Scholar]
- Amiri-Khorasani, M.; Abu Osman, N.A.; Yusof, A. Acute effect of static anddynamic stretching on hip dynamic range of motion during instep kicking in professional soccer players. J. Strength Cond. Res. 2011, 25, 1647–1652. [Google Scholar] [CrossRef] [PubMed]
- Dos’Santos, T.; Thomas, C.A.; Jones, P.; Comfort, P. Asymmetries in single and triple hop are not detrimental to change of direction speed. J. Trainol. 2017, 6, 35–41. [Google Scholar]
- Fort-Vanmeerhaeghe, A.; Montalvo, A.M.; Sitjà-Rabert, M.; Kiefer, A.W.; Myer, G.D. Neuromuscular asymmetries in the lower limbs of elite female youth basketball players and the application of the skillful limb model of comparison. Phys. Ther. Sport 2015, 16, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.R.; Ratamess, N.A.; Klatt, M.; Faigenbaum, A.D.; Kang, J. Do bilateral power deficits influence direction-specific movement patterns? Res. Sports Med. 2007, 15, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Bishop, C.; Pereira, L.A.; Reis, V.P.; Read, P.; Turner, A.N.; Loturco, I. Comparing the magnitude and direction of asymmetry during the squat, countermovement and drop jump tests in elite youth female soccer players. J. Sports Sci. 2020, 38, 1296–1303. [Google Scholar] [CrossRef] [PubMed]
- Rey, E.; Padrón-Cabo, A.; Barcala-Furelos, R.; Mecías-Calvo, M. Effect of high and low flexibility levels on physical fitness and neuromuscular properties in professional soccer players. Int. J. Sports Med. 2016, 37, 878–883. [Google Scholar] [CrossRef] [PubMed]
- Bradley, P.S.; Portas, M.D. The relationship between preseason range of motion and muscle strain injury in elite soccer players. J. Strength Cond. Res. 2007, 21, 1155–1159. [Google Scholar]
- Ade, J.; Fitzpatrick, J.; Bradley, P.S. High-intensity efforts in elite soccer matches and associated movement patterns, technical skills and tactical actions. Information for position-specific training drills. J. Sports Sci. 2016, 34, 2205–2214. [Google Scholar]
- Hart, N.H.; Nimphius, S.; Weber, J.; Spiteri, T.; Rantalainen, T.; Dobbin, M.; Newton, R.U. Musculoskeletal asymmetry in football athletes. Med. Sci. Sport. Exerc. 2016, 48, 1379–1387. [Google Scholar] [CrossRef]
- Ekstrand, J.; Waldén, M.; Hägglund, M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: A 13-year longitudinal analysis of the UEFA Elite Club injury study. Br. J. Sports Med. 2016, 50, 731–737. [Google Scholar] [CrossRef] [Green Version]
- Bishop, C.; Turner, A.; Jarvis, P.; Chavda, S.; Read, P. Considerations for selecting field-based strength and power fitness tests to measure asymmetries. J. Strength Cond. Res. 2017, 31, 2635–2644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Read, P.J.; Oliver, J.L.; De Ste Croix, M.B.A.; Myer, G.D.; Lloyd, R.S. A review of field-based assessments of neuromuscular control and their utility in male youth soccer players. J. Strength Cond. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Read, P.J.; Oliver, J.L.; Myer, G.D.; De Ste Croix, M.B.A.; Lloyd, R.S. The effects of maturation on measures of asymmetry during neuromuscular control tests in elite male youth soccer players. Pediatr. Exerc. Sci. 2017, 30, 168–175. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Fitness Test | Mean ± SD | ICC (95% CI) | CV (95% CI) |
|---|---|---|---|
| 505-CODd (s) | 2.54 ± 0.09 | 0.79 (0.48–0.89) | 2.9 (2.2–4.5) |
| 505-CODnd (s) | 2.63 ± 0.14 | 0.72 (0.43–0.87) | 4.0 (3.0–6.1) |
| CMJd (cm) | 12.59 ± 2.67 | 0.96 (0.91–0.98) | 3.9 (3.0–6.0) |
| CMJnd (cm) | 10.61 ± 1.76 | 0.84 (0.66–0.93) | 5.5 (4.2–8.5) |
| SBJd (cm) | 139.44 ± 11.10 | 0.96 (0.91–0.98) | 2.0 (1.5–3.1) |
| SBJnd (cm) | 133.81 ± 14.97 | 0.82 (0.62–0.92) | 4.7 (3.5–7.2) |
| LATd (cm) | 140.13 ± 15.44 | 0.97 (0.93–0.99) | 2.2 (1.6–3.3) |
| LATnd (cm) | 132.06 ± 13.95 | 0.94 (0.86–0.97) | 3.0 (2.2–4.5) |
| ROM_HFEKd (°) | 87.44 ± 8.63 | 0.97 (0.92–0.99) | 3.0 (2.3–4.6) |
| ROM_HFEKnd (°) | 79.56 ± 8.63 | 0.95 (0.90–0.98) | 2.9 (1.9–3.8) |
| ROM_HAFKd (°) | 80.06 ± 7.73 | 0.97 (0.92–0.99) | 2.2 (1.6–3.3) |
| ROM_HAFKnd (°) | 74.44 ± 7.15 | 0.97 (0.93–0.99) | 3.0 (2.3–4.6) |
| ROM_AFEKd (°) | 38.09 ± 5.53 | 0.96 (0.90–0.98) | 2.0 (1.5–3.1) |
| ROM_AFEKnd (°) | 35.78 ± 5.11 | 0.94 (0.89–0.97) | 3.3 (2.5–4.8) |
| ROM_AFFKd (°) | 38.56 ± 5.93 | 0.92 (0.87–0.97) | 2.7 (1.9–3.5) |
| ROM_AFFKnd (°) | 36.25 ± 5.46 | 0.88 (0.69–0.91) | 5.1 (4.0–8.1) |
| MMd (kg) | 6.40 ± 0.86 | - | - |
| MMnd (kg) | 6.24 ± 0.81 | - | - |
| Fitness Test | Mean Asymmetry ± SD (%) | Injury Risk |
|---|---|---|
| 505-COD | 3.58 ± 3.54 $ | No & |
| CMJ | 14.50 ± 9.80 *,$ | Yes & |
| SBJ | 4.24 ± 4.16 * | No & |
| LAT | 5.65 ± 3.09 * | No & |
| ROM_HFEK | 8.80 ± 7.66 * | Yes # |
| ROM_HAFK | 6.89 ± 5.13 * | No # |
| ROM_AFEK | 5.96 ± 4.05 * | No # |
| ROM_AFFK | 5.56 ± 8.04 * | No # |
| MM | 2.34 ± 1.64 | No & |
| Fitness Test | 505-COD | CMJ | SBJ | LAT | ROM_HFEK | ROM_HAFK | ROM_AFEK | ROM_AFFK |
|---|---|---|---|---|---|---|---|---|
| 505-COD | - | - | - | - | - | - | - | - |
| CMJ | 0.16 (−0.36–0.61) | - | - | - | - | - | - | - |
| SBJ | −0.13 (−0.59–0.39) | −0.07 (−0.50–0.49) | - | - | - | - | - | - |
| LAT | 0.27 (−0.26–0.67) | −0.32 (−0.70–0.21) | −0.08 (−0.55–0.44) | - | - | - | - | - |
| ROM_HFEK | 0.06 (−0.45–0.54) | 0.11 (−0.41–0.58) | 0.39 (−0.13–0.74) | 0.09 (−0.42–0.56) | - | - | - | - |
| ROM_HAFK | −0.03 (−0.52–0.47) | −0.15 (−0.60–0.38) | 0.47 (−0.30–0.78) | 0.03 (−0.47–0.52) | 0.42 (−0.10-0.76) | - | - | - |
| ROM_AFEK | 0.32 (−0.21–0.70) | −0.27 (−0.68–0.26) | 0.02 (−0.48–0.51) | 0.18 (−0.35–0.62) | 0.01 (−0.49–0.50) | 0.17 (−0.36–0.61) | - | - |
| ROM_AFFK | −0.19 (−0.63–0.33) | −0.33 (−0.71–0.20) | 0.44 (−0.07–0.77) | −0.07 (−0.54–0.45) | -0.49 (−0.59–0.39) | −0.16 (−0.61–0.36) | −0.28 (−0.68–0.26) | - |
| MM | −0.22 (−0.64–0.31) | −0.04 (−0.53–0.46) | −0.43 (−0.76–0.09) | 0.01 (−0.49–0.50) | −0.31 (−0.70–0.22) | −0.21 (−0.64–0.32) | −0.39 (−0.74-0.13) | 0.12 (−0.40–0.58) |
| Fitness Test | Mean ± SD | Reference Value | Injury Risk |
|---|---|---|---|
| ROM_HFEKd (°) | 87.44 ± 8.63 | <70° 1 | No |
| ROM_HFEKnd (°) | 79.56 ± 8.63 | No | |
| ROM_HAFKd (°) | 80.06 ± 7.73 | <50° 2 | No |
| ROM_HAFKnd (°) | 74.44 ± 7.15 | No | |
| ROM_AFEKd (°) | 38.09 ± 5.53 | <30° 3 | No |
| ROM_AFEKnd (°) | 35.78 ± 5.11 | No | |
| ROM_AFFKd (°) | 38.56 ± 5.93 | <40° 4 | Yes |
| ROM_AFFKnd (°) | 36.25 ± 5.46 | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raya-González, J.; Clemente, F.M.; Castillo, D. Analyzing the Magnitude of Interlimb Asymmetries in Young Female Soccer Players: A Preliminary Study. Int. J. Environ. Res. Public Health 2021, 18, 475. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020475
Raya-González J, Clemente FM, Castillo D. Analyzing the Magnitude of Interlimb Asymmetries in Young Female Soccer Players: A Preliminary Study. International Journal of Environmental Research and Public Health. 2021; 18(2):475. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020475
Chicago/Turabian StyleRaya-González, Javier, Filipe Manuel Clemente, and Daniel Castillo. 2021. "Analyzing the Magnitude of Interlimb Asymmetries in Young Female Soccer Players: A Preliminary Study" International Journal of Environmental Research and Public Health 18, no. 2: 475. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020475