Effectiveness of Motor Imagery on Motor Recovery in Patients with Multiple Sclerosis: Systematic Review


 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Assessment of the Methodological Quality and Risk of Bias
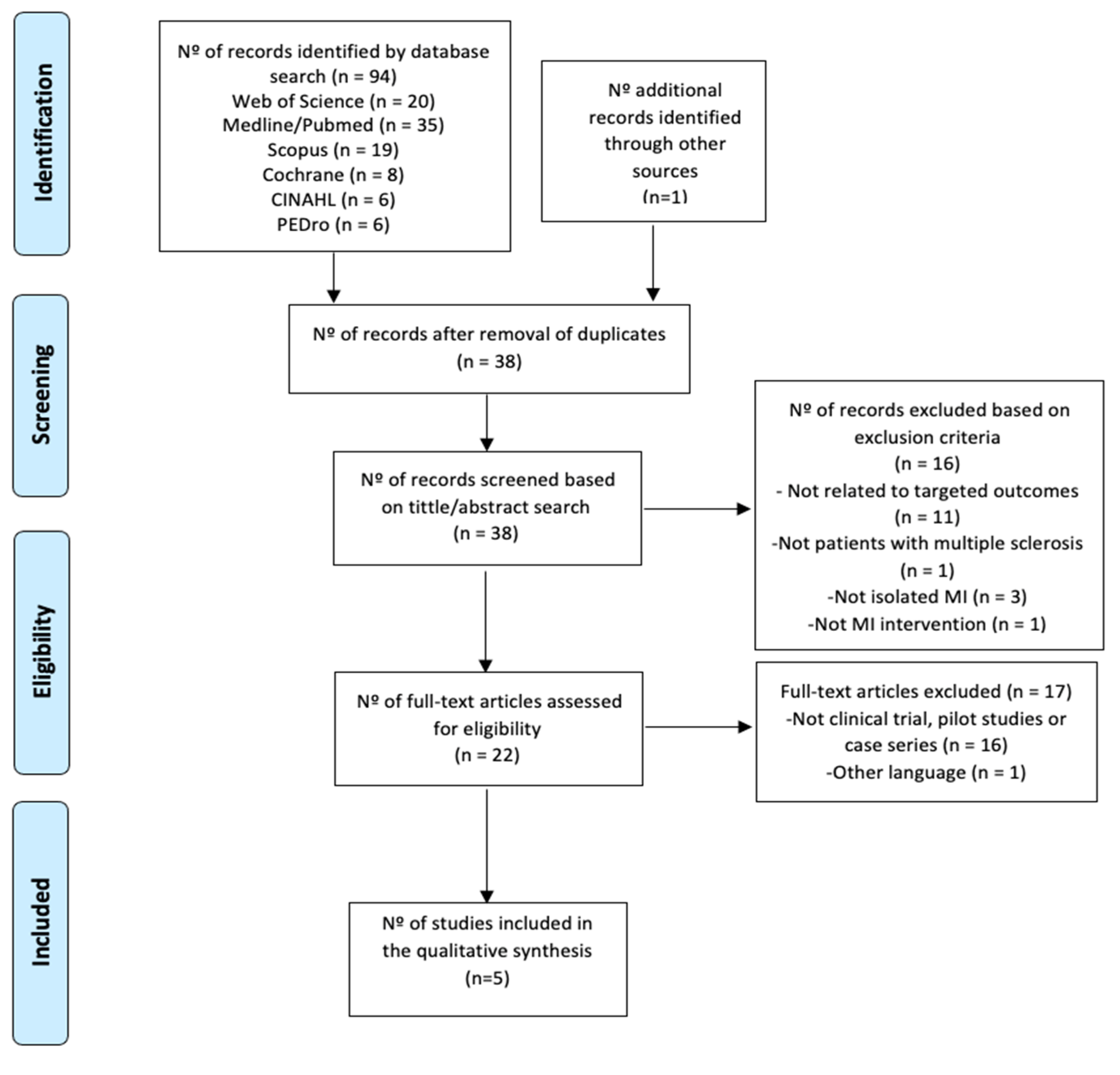
2.4. Selection Process and Data Extraction
3. Results
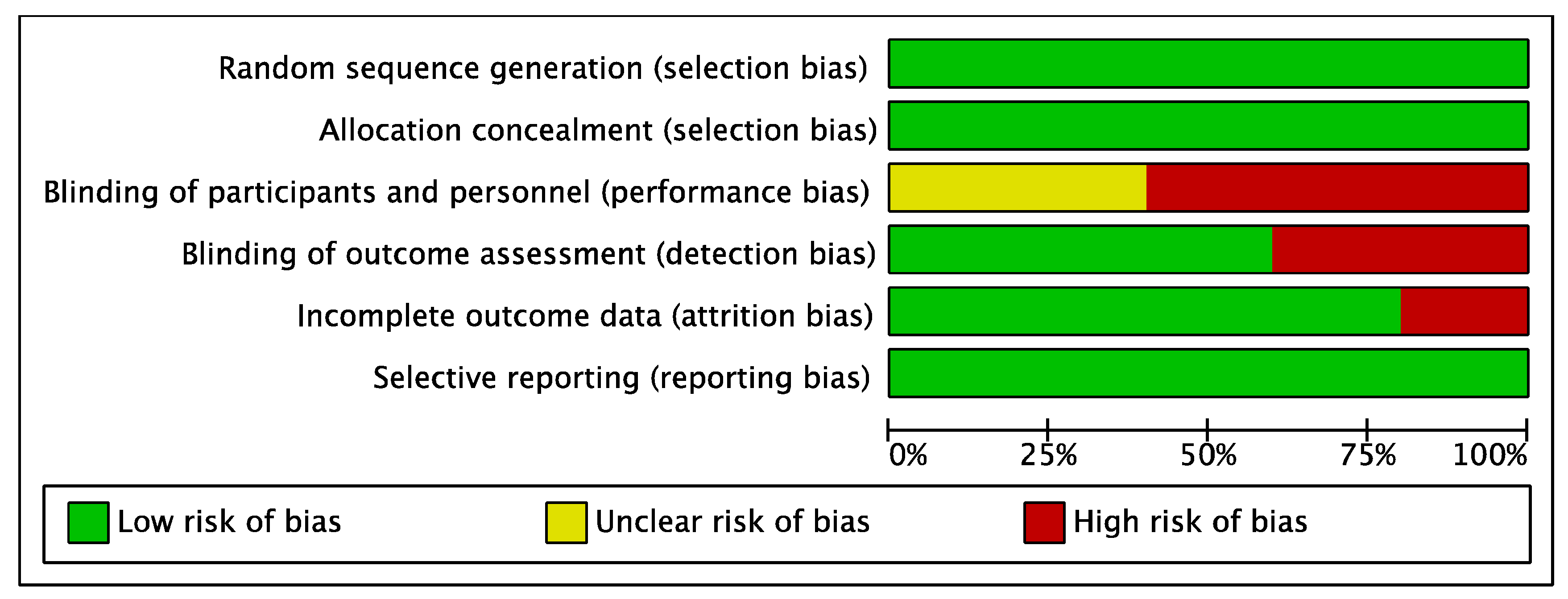
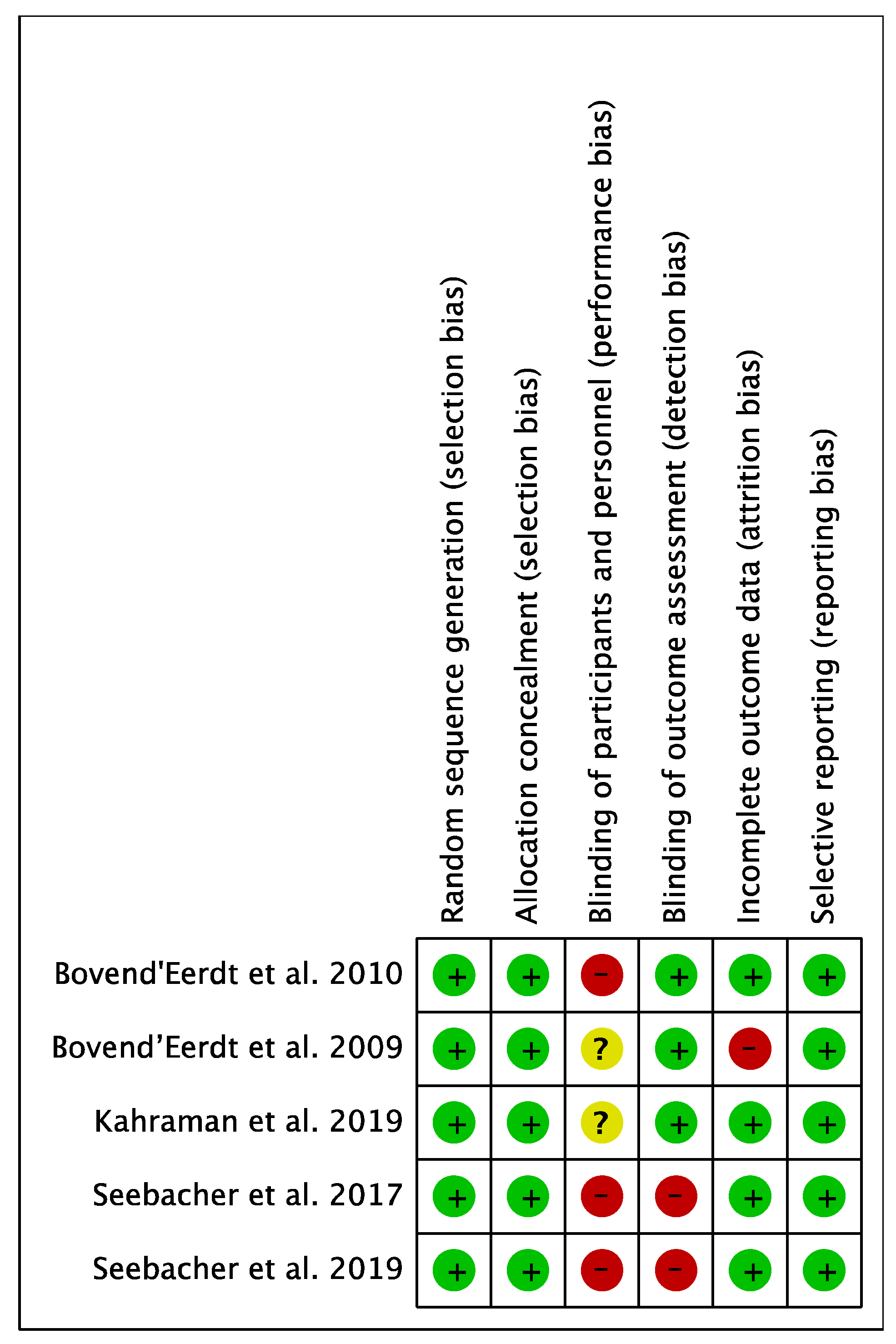
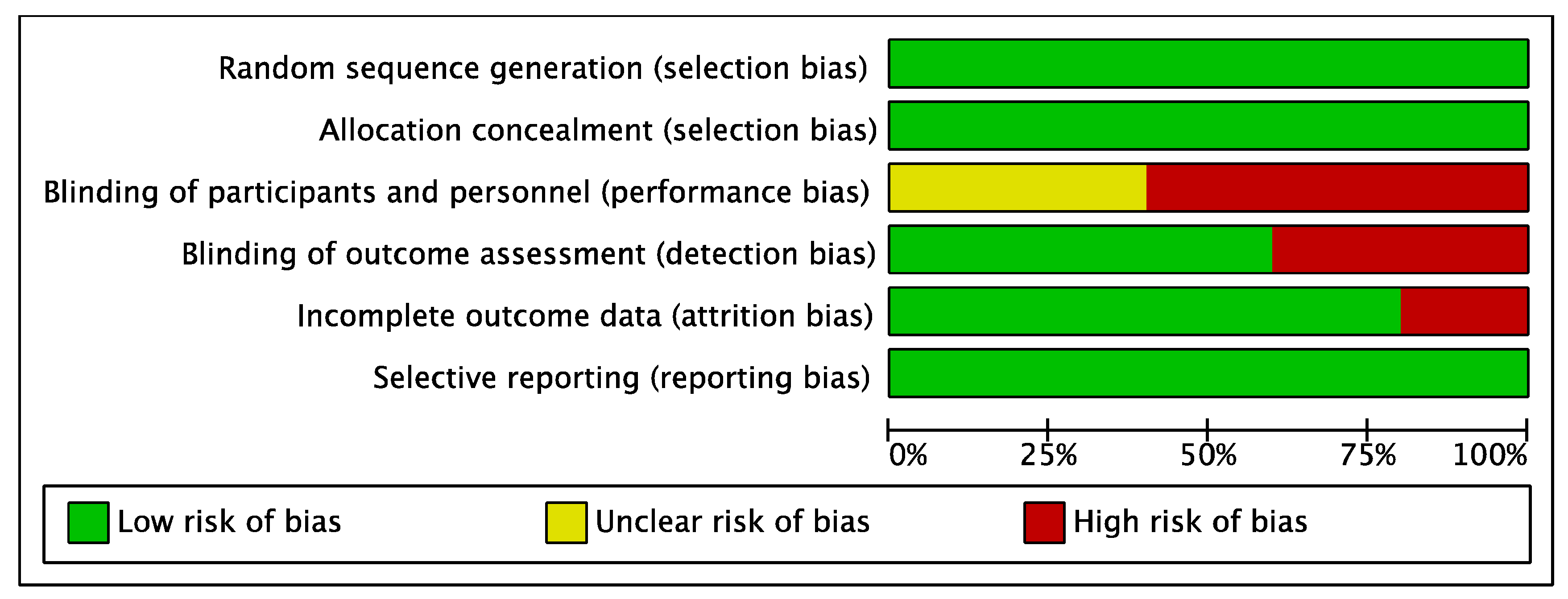
3.1. Methodological Quality and Risk of Bias
3.2. Synthesis of Results
3.3. Participant Characteristics
3.4. Intervention Characteristics
3.5. Outcomes Measures
3.5.1. Gait
3.5.2. Balance
3.5.3. Fatigue
3.5.4. Quality of Life
3.5.5. Secondary Outcomes
Upper Limb Function
Muscular Tone and Range of Movement
Functional Independence
4. Discussion
4.1. Gait
4.2. Balance
4.3. Fatigue
4.4. Quality of Life
4.5. Upper Limb Function
4.6. Muscular Tone and Range of Movement
4.7. Functional Independence
4.8. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- García Merino, A.; Ara Callizo, J.R.; Fernández Fernández, O.; Landete Pascual, L.; Moral Torres, E.; Rodríguez-Antigüedad Zarrantz, A. Consenso para el tratamiento de la esclerosis múltiple 2016. Neurología 2017, 32, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Fernández, O.; Fernández, V.E.; Guerrero, M. Esclerosis múltiple. Med. Programa Form. Médica Contin. Acreditado 2015, 11, 4610–4621. [Google Scholar] [CrossRef]
- Amatya, B.; Khan, F.; Galea, M. Rehabilitation for people with multiple sclerosis: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2019, 1, CD012732. [Google Scholar] [CrossRef] [PubMed]
- Kubsik-Gidlewska, A.; Kubsik-Gidlewska, A.M.; Klimkiewicz, P.; Klimkiewicz, R.; Janczewska, K.; Woldańska-Okońska, M. Rehabilitation in multiple sclerosis. Adv. Clin. Exp. Med. 2017, 26, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Massetti, T.; Lopes, I.; Arab, C.; Meire, F.; Ribeiro-papa, D.C.; Bandeira, C.; Monteiro, D.M. Virtual reality in multiple sclerosis—A systematic review. Mult. Scler. Relat. Disord. 2016, 8, 107–112. [Google Scholar] [CrossRef]
- Moran, A.; Guillot, A.; MacIntyre, T.; Collet, C. Re-imagining motor imagery: Building bridges between cognitive neuroscience and sport psychology. Br. J. Psychol. 2012, 103, 224–247. [Google Scholar] [CrossRef]
- Hétu, S.; Grégoire, M.; Saimpont, A.; Coll, M.-P.; Eugène, F.; Michon, P.-E.; Jackson, P.L. The neural network of motor imagery: An ALE meta-analysis. Neurosci. Biobehav. Rev. 2013, 37, 930–949. [Google Scholar] [CrossRef]
- Jeannerod, M. Motor Cognition; Oxford University Press: Oxford, UK, 2006; ISBN 9780198569657. [Google Scholar]
- Ruffino, C.; Papaxanthis, C.; Lebon, F. The influence of imagery capacity in motor performance improvement. Exp. Brain Res. 2017, 235, 3049–3057. [Google Scholar] [CrossRef]
- Richardson, A. Has mental practice any relevance to physiotherapy? Physiotherapy 1964, 50, 148–151. [Google Scholar]
- Malouin, F.; Jackson, P.L.; Richards, C.L. Towards the integration of mental practice in rehabilitation programs. A critical review. Front. Hum. Neurosci. 2013, 7, 576. [Google Scholar] [CrossRef] [Green Version]
- Jackson, P.L.; Lafleur, M.F.; Malouin, F.; Richards, C.; Doyon, J. Potential role of mental practice using motor imagery in neurologic rehabilitation. Arch. Phys. Med. Rehabil. 2001, 82, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- García Carrasco, D.; Aboitiz Cantalapiedra, J. Effectiveness of motor imagery or mental practice in functional recovery after stroke: A systematic review. Neurologia 2016, 31, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Simmons, L.; Sharma, N.; Baron, J.-C.; Pomeroy, V.M. Motor Imagery to Enhance Recovery After Subcortical Stroke: Who Might Benefit, Daily Dose, and Potential Effects. Neurorehabil. Neural Repair 2008, 22, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Guillot, A.; Di Rienzo, F.; MacIntyre, T.; Moran, A.; Collet, C. Imagining is Not Doing but Involves Specific Motor Commands: A Review of Experimental Data Related to Motor Inhibition. Front. Hum. Neurosci. 2012, 6, 247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanson, M.; Concialdi, M. Motor imagery in multiple sclerosis: Exploring applications in therapeutic treatment. J. Neurophysiol. 2019, 121, 347–349. [Google Scholar] [CrossRef] [Green Version]
- Braun, S.; Kleynen, M.; van Heel, T.; Kruithof, N.; Wade, D.; Beurskens, A. The effects of mental practice in neurological rehabilitation; a systematic review and meta-analysis. Front. Hum. Neurosci. 2013, 7. [Google Scholar] [CrossRef] [Green Version]
- Senders, A.; Wahbeh, H.; Spain, R.; Shinto, L. Mind-Body Medicine for Multiple Sclerosis: A Systematic Review. Autoimmune Dis. 2012, 2012, 567324. [Google Scholar] [CrossRef] [Green Version]
- Kaur, J.; Ghosh, S.; Sahani, A.K.; Sinha, J.K. Mental imagery training for treatment of central neuropathic pain: A narrative review. Acta Neurol. Belg. 2019, 119, 175–186. [Google Scholar] [CrossRef]
- Seebacher, B.; Kuisma, R.; Glynn, A.; Berger, T. Effects and mechanisms of differently cued and non-cued motor imagery in people with multiple sclerosis: A randomised controlled trial. Mult. Scler. 2019, 25, 1593–1604. [Google Scholar] [CrossRef]
- Kahraman, T.; Savci, S.; Ozdogar, A.T.; Gedik, Z.; Idiman, E. Physical, cognitive and psychosocial effects of telerehabilitation-based motor imagery training in people with multiple sclerosis: A randomized controlled pilot trial. J. Telemed. Telecare 2020, 26, 251–260. [Google Scholar] [CrossRef]
- Li, R.-Q.; Li, Z.-M.; Tan, J.-Y.; Chen, G.-L.; Lin, W.-Y. Effects of motor imagery on walking function and balance in patients after stroke: A quantitative synthesis of randomized controlled trials. Complement. Ther. Clin. Pract. 2017, 28, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Lotze, M.; Halsband, U. Motor imagery. J. Physiol. Paris 2006, 99, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, C.M.D.C.; Pimenta, C.A.D.M.; Nobre, M.R.C. The PICO strategy for the research question construction and evidence search. Rev. Lat. Am. Enfermagem 2007, 15, 508–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Heal. 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Bovend’Eerdt, T.J.; Dawes, H.; Sackley, C.; Izadi, H.; Wade, D.T. Mental techniques during manual stretching in spasticity—A pilot randomized controlled trial. Clin. Rehabil. 2009, 23, 137–145. [Google Scholar] [CrossRef]
- Seebacher, B.; Kuisma, R.; Glynn, A.; Berger, T. The effect of rhythmic-cued motor imagery on walking, fatigue and quality of life in people with multiple sclerosis: A randomised controlled trial. Mult. Scler. 2017, 23, 286–296. [Google Scholar] [CrossRef]
- Bovend’Eerdt, T.J.; Dawes, H.; Sackley, C.; Izadi, H.; Wade, D.T. An Integrated Motor Imagery Program to Improve Functional Task Performance in Neurorehabilitation: A Single-Blind Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2010, 91, 939–946. [Google Scholar] [CrossRef]
- Meyer-Moock, S.; Feng, Y.-S.; Maeurer, M.; Dippel, F.-W.; Kohlmann, T. Systematic literature review and validity evaluation of the Expanded Disability Status Scale (EDSS) and the Multiple Sclerosis Functional Composite (MSFC) in patients with multiple sclerosis. BMC Neurol. 2014, 14, 58. [Google Scholar] [CrossRef] [Green Version]
- Holmes, P.S.; Collins, D.J. The PETTLEP Approach to Motor Imagery: A Functional Equivalence Model for Sport Psychologists. J. Appl. Sport Psychol. 2001, 13, 60–83. [Google Scholar] [CrossRef]
- Harris, J.E.; Hebert, A. Utilization of motor imagery in upper limb rehabilitation: A systematic scoping review. Clin. Rehabil. 2015, 29, 1092–1107. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; Cohen, J.A.; Benedict, R.; Phillips, G.; LaRocca, N.; Hudson, L.D.; Rudick, R. Validity of the timed 25-foot walk as an ambulatory performance outcome measure for multiple sclerosis. Mult. Scler. J. 2017, 23, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Beckerman, H.; Heine, M.; van den Akker, L.E.; de Groot, V. The 2-minute walk test is not a valid method to determine aerobic capacity in persons with Multiple Sclerosis. NeuroRehabilitation 2019, 45, 239–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpinella, I.; Cattaneo, D.; Ferrarin, M. Quantitative assessment of upper limb motor function in Multiple Sclerosis using an instrumented Action Research Arm Test. J. Neuroeng. Rehabil. 2014, 11, 67. [Google Scholar] [CrossRef] [PubMed]
- Haas, J. Pathophysiology, assessment and management of multiple sclerosis spasticity: An update. Expert Rev. Neurother. 2011, 11, 3–8. [Google Scholar] [CrossRef]
- Nicholl, L.; Hobart, J.; Dunwoody, L.; Cramp, F.; Lowe-Strong, A. Measuring disability in multiple sclerosis: Is the Community Dependency Index an improvement on the Barthel Index? Mult. Scler. J. 2004, 10, 447–450. [Google Scholar] [CrossRef]
- Heremans, E.; Nieuwboer, A.; Spildooren, J.; De Bondt, S.; D’hooge, A.-M.; Helsen, W.; Feys, P. Cued motor imagery in patients with multiple sclerosis. Neuroscience 2012, 206, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Heremans, E.; D’Hooge, A.M.; De Bondt, S.; Helsen, W.; Feys, P. The relation between cognitive and motor dysfunction and motor imagery ability in patients with multiple sclerosis. Mult. Scler. 2012, 18, 1303–1309. [Google Scholar] [CrossRef] [Green Version]
- Tabrizi, Y.M.; Mazhari, S.; Nazari, M.A.; Zangiabadi, N.; Sheibani, V.; Azarang, S. Compromised motor imagery ability in individuals with multiple sclerosis and mild physical disability: An ERP study. Clin. Neurol. Neurosurg. 2013, 115, 1738–1744. [Google Scholar] [CrossRef]
- McInnes, K.; Friesen, C.; Boe, S. Specific Brain Lesions Impair Explicit Motor Imagery Ability: A Systematic Review of the Evidence. Arch. Phys. Med. Rehabil. 2016, 97, 478–489.e1. [Google Scholar] [CrossRef] [PubMed]
- Mulder, T.; Hochstenbach, J.B.H.; van Heuvelen, M.J.G.; den Otter, A.R. Motor imagery: The relation between age and imagery capacity. Hum. Mov. Sci. 2007, 26, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Scalzitti, D.A.; Harwood, K.J.; Maring, J.R.; Leach, S.J.; Ruckert, E.A.C.E. Validation of the 2-Minute Walk Test with the 6-Minute Walk Test and Other Functional Measures in Persons with Multiple Sclerosis. Int. J. MS Care. 2018, 20, 158–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W.; Glenney, S.S. Minimal clinically important difference for change in comfortable gait speed of adults with pathology: A systematic review. J. Eval. Clin. Pract. 2014, 20, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Moumdjian, L.; Sarkamo, T.; Leone, C.; Leman, M.; Feys, P. Effectiveness of music-based interventions on motricity or cognitive functioning in neurological populations: A systematic review. Eur. J. Phys. Rehabil. Med. 2017, 53, 466–482. [Google Scholar] [CrossRef] [PubMed]
- Sosnoff, J.J.; Socie, M.J.; Boes, M.K.; Sandroff, B.M.; Pula, J.H.; Suh, Y.; Weikert, M.; Balantrapu, S.; Morrison, S.; Motl, R.W. Mobility, balance and falls in persons with multiple sclerosis. PLoS ONE 2011, 6, e28021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuda, P.N.; Shumway-Cook, A.; Bamer, A.M.; Johnson, S.L.; Amtmann, D.; Kraft, G.H. Falls in Multiple Sclerosis. PM&R 2011, 3, 624–632. [Google Scholar] [CrossRef]
- Peebles, A.T.; Bruetsch, A.P.; Lynch, S.G.; Huisinga, J.M. Dynamic balance in persons with multiple sclerosis who have a falls history is altered compared to non-fallers and to healthy controls. J. Biomech. 2017, 63, 158–163. [Google Scholar] [CrossRef]
- Sun, R.; McGinnis, R.; Sosnoff, J.J. Novel technology for mobility and balance tracking in patients with multiple sclerosis: A systematic review. Expert Rev. Neurother. 2018, 18, 887–898. [Google Scholar] [CrossRef]
- Harrison, S.L.; Laver, K.E.; Ninnis, K.; Rowett, C.; Lannin, N.A.; Crotty, M. Effectiveness of external cues to facilitate task performance in people with neurological disorders: A systematic review and meta-analysis. Disabil. Rehabil. 2019, 41, 1874–1881. [Google Scholar] [CrossRef] [Green Version]
- Brecl Jakob, G.; Remšak, T.; Olenšek, J.; Perellón-Alfonso, R.; Šega Jazbec, S.; Rot, U. Visual but not verbal working memory interferes with balance in patients after optic neuritis suggestive of multiple sclerosis. Neurosci. Lett. 2019, 707, 134288. [Google Scholar] [CrossRef] [PubMed]
- Mills, R.J.; Young, C.A.; Pallant, J.F.; Tennant, A. Rasch analysis of the Modified Fatigue Impact Scale (MFIS) in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2010, 81, 1049–1051. [Google Scholar] [CrossRef] [PubMed]
- Meca-Lallana, V.; Brañas-Pampillón, M.; Higueras, Y.; Candeliere-Merlicco, A.; Aladro-Benito, Y.; Rodríguez-De la Fuente, O.; Salas-Alonso, E.; Maurino, J.; Ballesteros, J. Assessing fatigue in multiple sclerosis: Psychometric properties of the five-item Modified Fatigue Impact Scale (MFIS-5). Mult. Scler. J. Exp. Transl. Clin. 2019, 5, 205521731988798. [Google Scholar] [CrossRef] [PubMed]
- Guillemin, C.; Lommers, E.; Delrue, G.; Gester, E.; Maquet, P.; Collette, F. Subjective feeling of fatigue and cognitive performances: A specific link in multiple sclerosis. Front. Neurosci. 2019, 12. [Google Scholar] [CrossRef]
- Coghe, G.; Corona, F.; Pilloni, G.; Porta, M.; Frau, J.; Lorefice, L.; Fenu, G.; Cocco, E.; Pau, M. Is There Any Relationship between Upper and Lower Limb Impairments in People with Multiple Sclerosis? A Kinematic Quantitative Analysis. Mult. Scler. Int. 2019, 2019, 9149201. [Google Scholar] [CrossRef] [Green Version]
- Wininger, M.; Craelius, W.; Settle, J.; Robinson, S.; Isaac, B.; Maloni, H.; Moradi, M.; Newby, N.A.; Wallin, M. Biomechanical analysis of spasticity treatment in patients with multiple sclerosis. Ther. Adv. Neurol. Disord. 2015, 8, 203–211. [Google Scholar] [CrossRef] [Green Version]
- Prodinger, B.; O’Connor, R.; Stucki, G.; Tennant, A. Establishing score equivalence of the Functional Independence Measure motor scale and the Barthel Index, utilising the International Classification of Functioning, Disability and Health and Rasch measurement theory. J. Rehabil. Med. 2017, 49, 416–422. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Databases | Search |
|---|---|
| Medline/PubMed, Scopus, CINAHL, Cochrane, Web of Science | (“motor imagery” OR “mental imagery” OR “mental practice”) AND “multiple sclerosis” AND rehabilitation |
| PEDro | Motor imagery in multiple sclerosis |
| Kahraman et al. 2019 [21] | Seebacher et al. 2019 [20] | Seebacher et al. 2017 [29] | Bovend’Eerdt et al. 2010 [30] | Bovend’Eerdt et al. 2009 [28] | |
|---|---|---|---|---|---|
| 1. Study quality | |||||
| Hypothesis/aim | 1 | 1 | 1 | 1 | 1 |
| Outcomes | 1 | 1 | 1 | 1 | 1 |
| Eligibility criteria | 1 | 1 | 1 | 1 | 1 |
| Interventions | 1 | 1 | 1 | 1 | 1 |
| Confounders | 0 | 0 | 0 | 0 | 0 |
| Findings | 1 | 1 | 1 | 1 | 1 |
| Random variability | 1 | 1 | 1 | 1 | 1 |
| Adverse events | 1 | 0 | 0 | 1 | 1 |
| Lost to follow-up | 1 | 1 | 1 | 1 | 1 |
| Probability values | 1 | 1 | 1 | 1 | 1 |
| 2. External validity (study bias) | |||||
| Source population | 0 | 0 | 0 | 0 | 0 |
| Illustrative sample | 0 | 0 | 0 | 0 | 0 |
| Illustrative treat | 1 | 0 | 0 | 0 | 0 |
| 3. Internal validity (study bias) | |||||
| Blinding of subjects | 1 | 0 | 0 | 0 | 0 |
| Blinding | 1 | 1 | 1 | 1 | 0 |
| “Data dredging” | 1 | 1 | 1 | 1 | 1 |
| Follow-up adjusts | 1 | 1 | 1 | 1 | 1 |
| Statistical tests | 1 | 1 | 1 | 1 | 1 |
| Compliance | 1 | 1 | 1 | 0 | 1 |
| Outcomes | 1 | 1 | 1 | 0 | 1 |
| 4. Internal validity (confounding and selection bias) | |||||
| Source of patients | 1 | 0 | 1 | 0 | 0 |
| Recruitment period | 1 | 1 | 1 | 1 | 1 |
| Randomization | 1 | 1 | 1 | 0 | 0 |
| Concealment | 0 | 1 | 1 | 0 | 0 |
| Analysis | 0 | 0 | 0 | 0 | 0 |
| Loss to follow-up | 1 | 0 | 0 | 0 | 0 |
| 5. Power | |||||
| Effect | 1 | 0 | 0 | 1 | 0 |
| TOTAL SCORE | 21 | 19 | 19 | 14 | 12 |
| PORCENTAGE (%) * | 61 | 59 | 59 | 42 | 38 |
| Authors (Year) | Sample | Type of MI | Age (Average) | Stadium | N Sessions, Temporality | Performance of Measurement | Results |
|---|---|---|---|---|---|---|---|
| Kahraman et al. 2019 [21] | N = 33 TRBM = 19 C = 14 | No guided Tele-MI, PETTLEP | 35.2 (38.3–42.7) | (average EDSS = 2) Chronicity 4 years. | 16 sessions (30 min), 0/1 session/day, 2 days/week, 8 weeks | T25FW, TUG, 2MWT, MSWS-12, DGI, ABC, LOS, PST, MFIS, MUSIQOL | In the intervention group, significant improvements in walking speed (p = 0.007), perceived walking ability (p = 0.008), dynamic balance (p = 0.002), fatigue (p = 0.001) and quality of life (p = 0.002) |
| Seebacher et al. 2019 [20] | N = 59 MVMI = 19 MMI = 20 MING = 20 | Guided by music and verbal and no guided | 44.36 (39.5–49.5) | (EDSS 2.6) Chronicity + 3 months | 24 sessions (17 min), 0/1 session/day, 6 days/week, 4 weeks | T25FW, 6MWT, MFIS, MSIS-29 | Within-group comparisons showed that all three interventions significantly improved walking speed and walking distance. Between-group analyses show significant improvements, in MVMI group, in distance (p = 0.024) and walking speed (p = 0.001), in fatigue (p = 0.030) and quality of life (p = 0.024) |
| Seebacher et al. 2017 [29] | N= 101 MVMI = 34 MTVMI = 34 C = 33 | Guided by verbal, music, or metronome | 44.1 (39.6–46.3) | (EDSS 2) Chronicity + de 3 months | 24 sessions (17 min), 0/1 session/day, 6 days/week, 4 weeks | T25FW, 6MWT, MSWS-12, MFIS, MSIS-29, SF36, EQ-5D-3L | Significant improvements in walking speed (p < 0.0001) and distance (p < 0.0001) (within-group comparisons). Physical fatigue (p = 0.001) (only significant in the MVMI group) quality of life (only significant in MVMI group) (p = 0.005) |
| Bovend’Eerdt et al. 2010 [30] | N = 30 C = 0 MS MIG = 1 MS | Guided by verbal | 51.2 ± 11 | EDSS low Chronicity 10 years | 10 sessions, 3 days/week, 3 weeks 2 days/week, 2 weeks | TUG, RMI, ARAT, NEAD, GAS | Poor adherence to the treatment. Significant improvements post-intervention only in GAS (p < 0.001) but not over time (p = 0.845) |
| Bovend’Eerdt et al. 2009 [28] | N = 11(4 MS) PMR = 1 MS MI = 3 MS | No guided | 48.25 ± 10 | EDSS not detailed Chronicity 19 years. | 8–56 sessions, 8 weeks | RMI, MAS, EG, BI | No significant differences were found between groups after intervention (p > 0.05). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gil-Bermejo-Bernardez-Zerpa, A.; Moral-Munoz, J.A.; Lucena-Anton, D.; Luque-Moreno, C. Effectiveness of Motor Imagery on Motor Recovery in Patients with Multiple Sclerosis: Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 498. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020498
Gil-Bermejo-Bernardez-Zerpa A, Moral-Munoz JA, Lucena-Anton D, Luque-Moreno C. Effectiveness of Motor Imagery on Motor Recovery in Patients with Multiple Sclerosis: Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(2):498. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020498
Chicago/Turabian StyleGil-Bermejo-Bernardez-Zerpa, Ana, Jose A. Moral-Munoz, David Lucena-Anton, and Carlos Luque-Moreno. 2021. "Effectiveness of Motor Imagery on Motor Recovery in Patients with Multiple Sclerosis: Systematic Review" International Journal of Environmental Research and Public Health 18, no. 2: 498. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020498