A Technology-Mediated Interventional Approach to the Prevention of Metabolic Syndrome: A Systematic Review and Meta-Analysis


Abstract
:1. Background
2. Methods
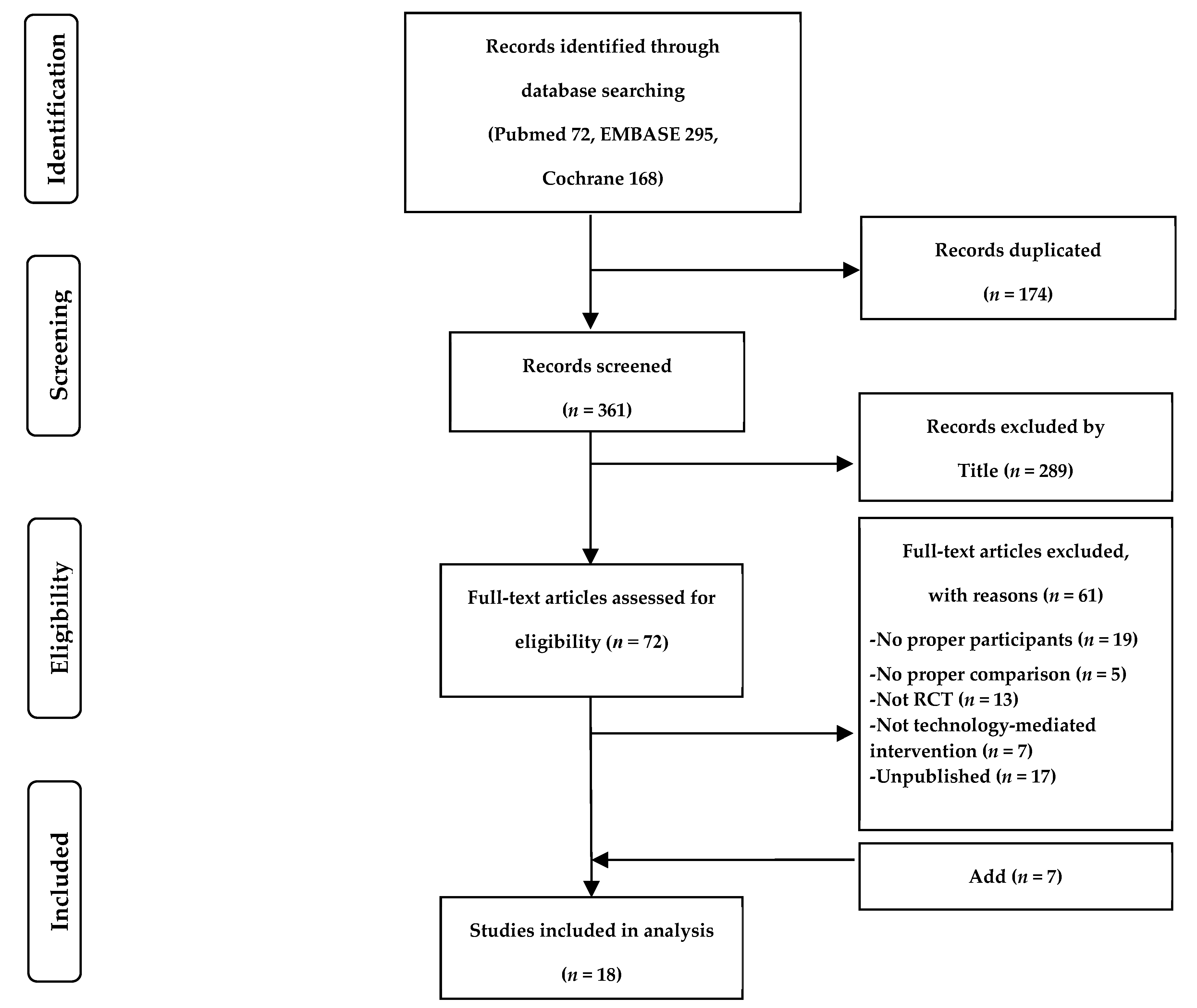
2.1. Search Strategy and Study Selection
2.2. Data Extraction
2.3. Risk of Bias Assessment
2.4. Statistical Analyses
3. Results
3.1. General Characteristics of the Studies
3.2. Methodological Quality and Risk of Bias
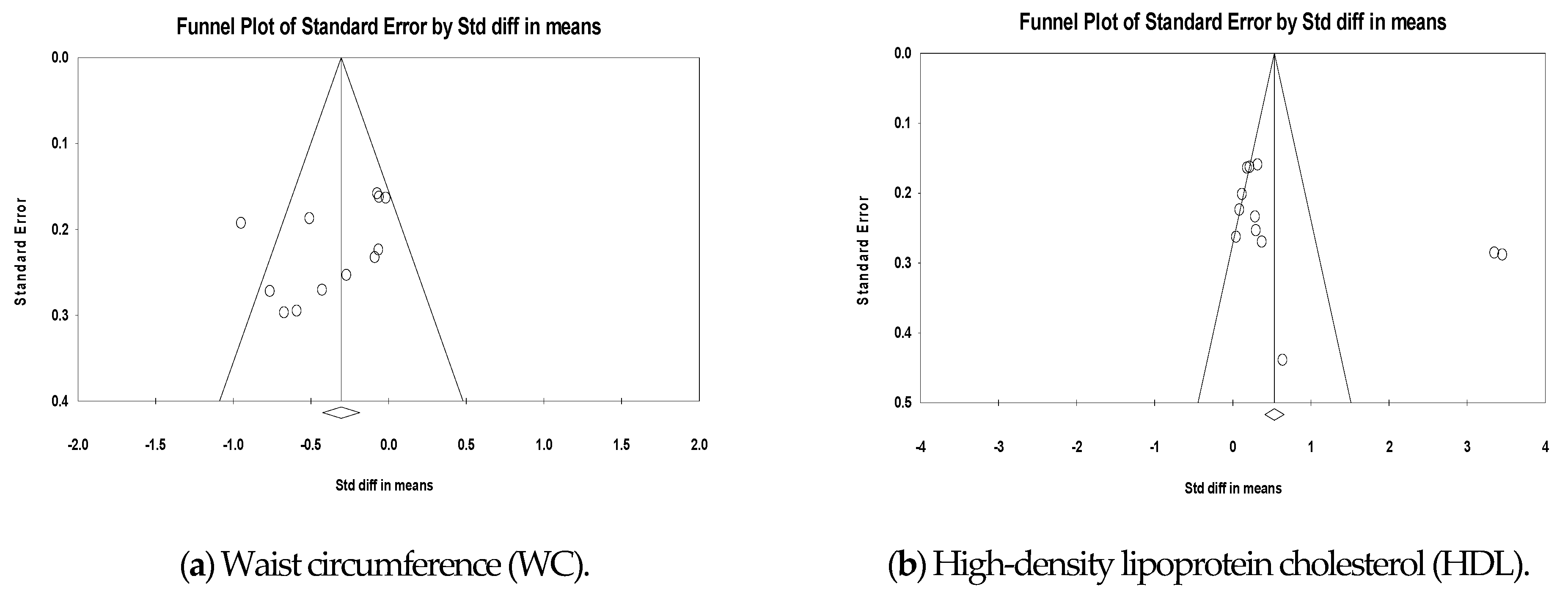
3.3. Publication Bias
3.4. Metabolic Syndrome-Related Outcomes
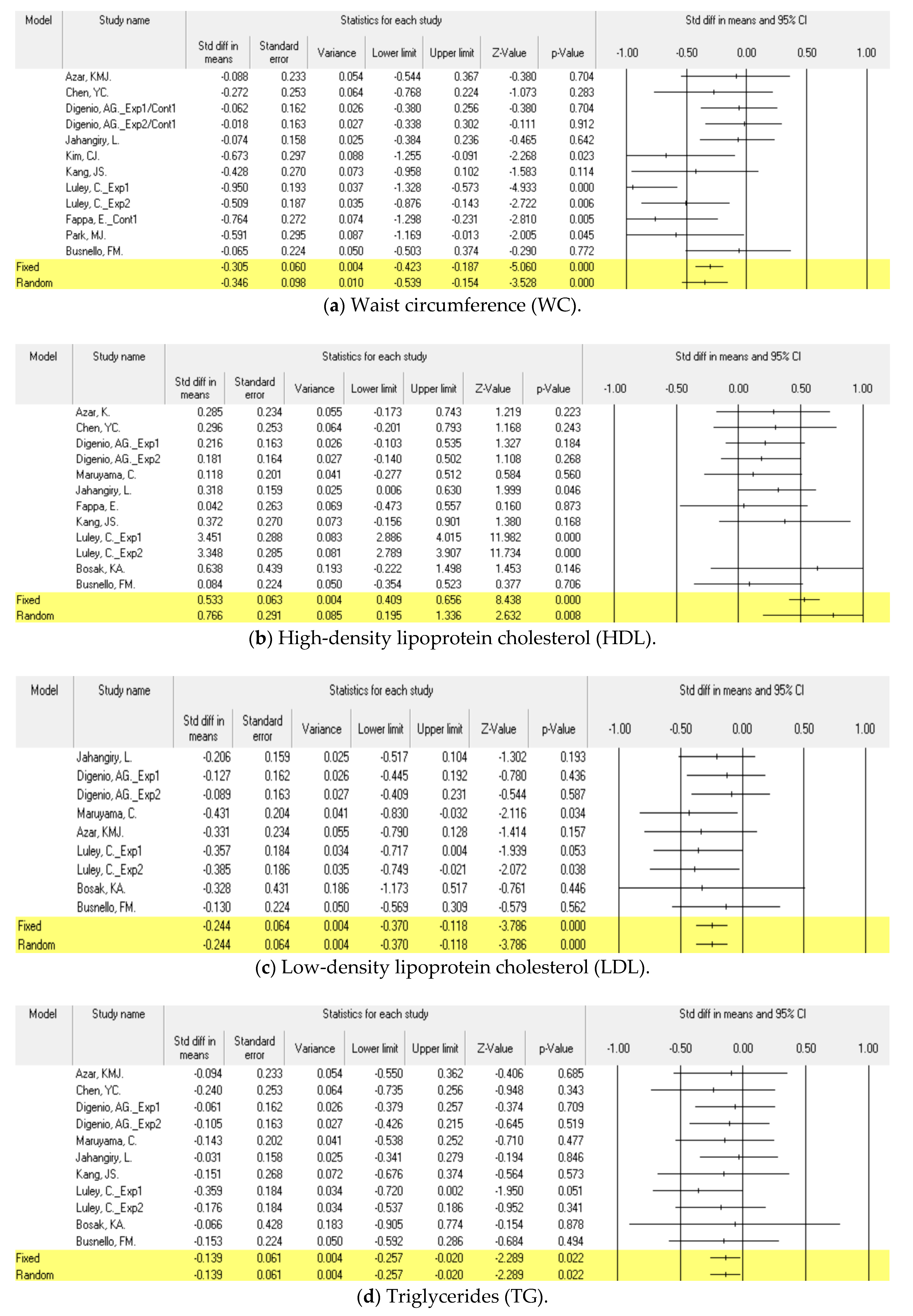
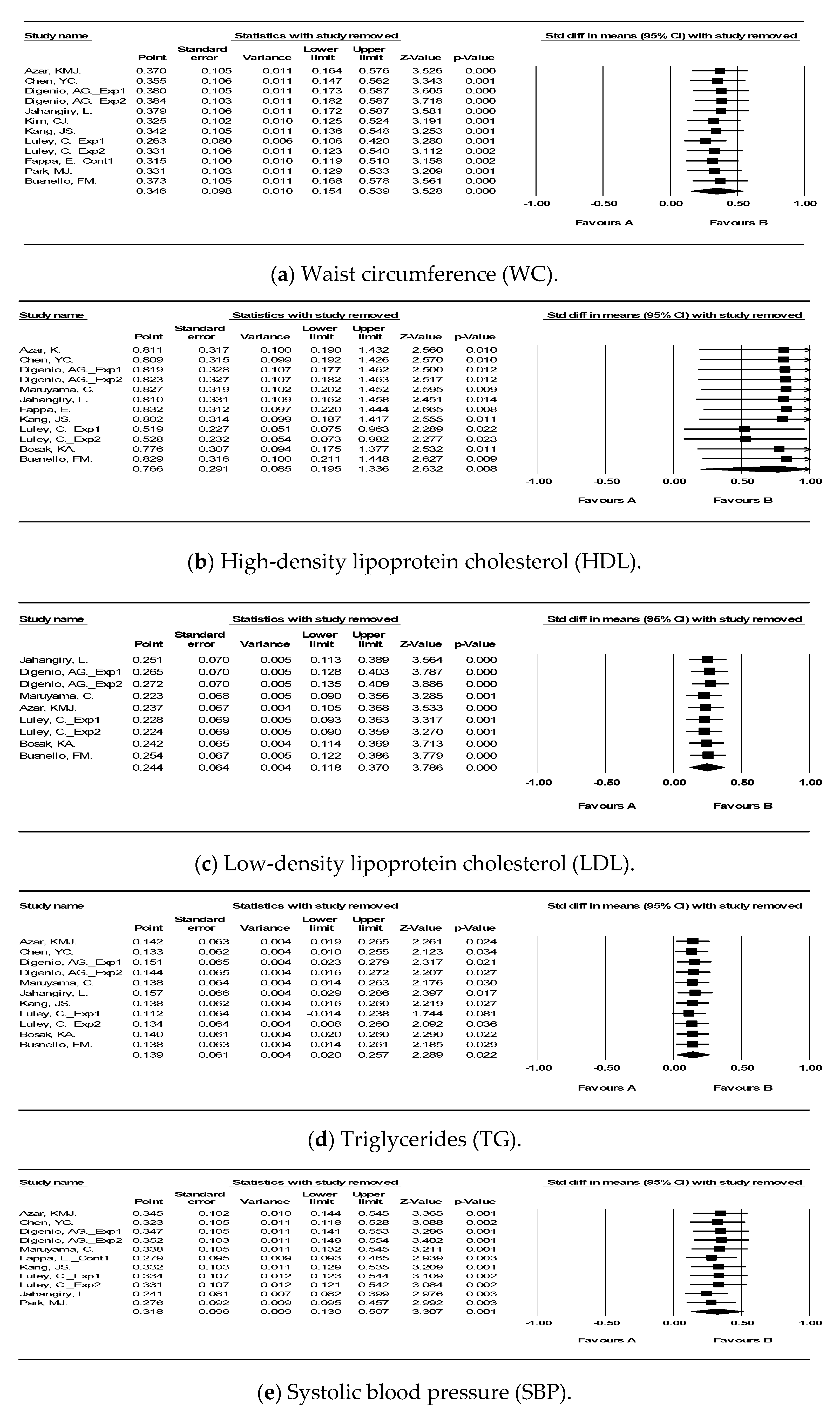
3.4.1. Waist Circumference (WC)
3.4.2. High-Density Lipoprotein Cholesterol (HDL)
3.4.3. Low-Density Lipoprotein Cholesterol (LDL)
3.4.4. Triglycerides (TG)
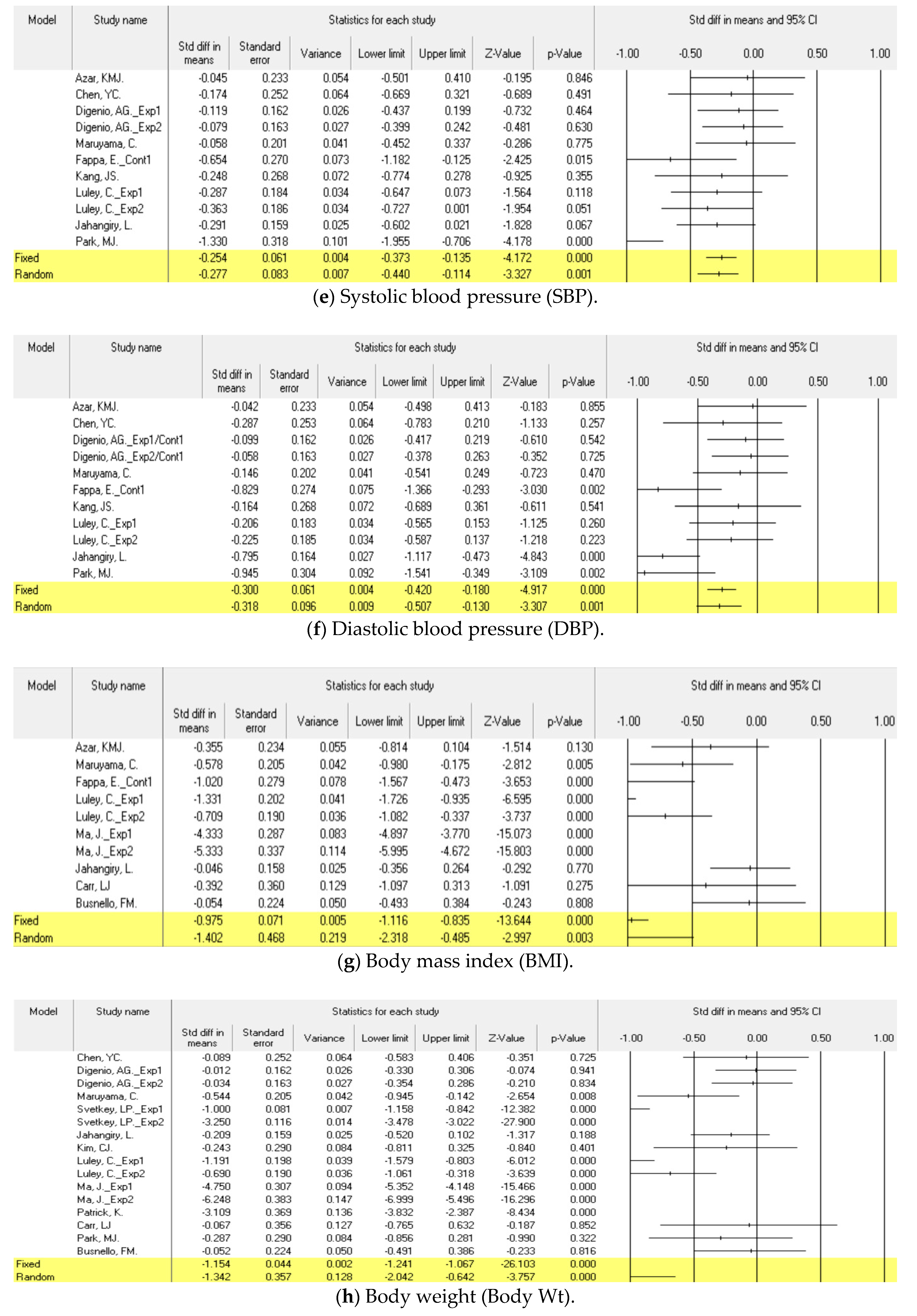
3.4.5. Systolic Blood Pressure (SBP)
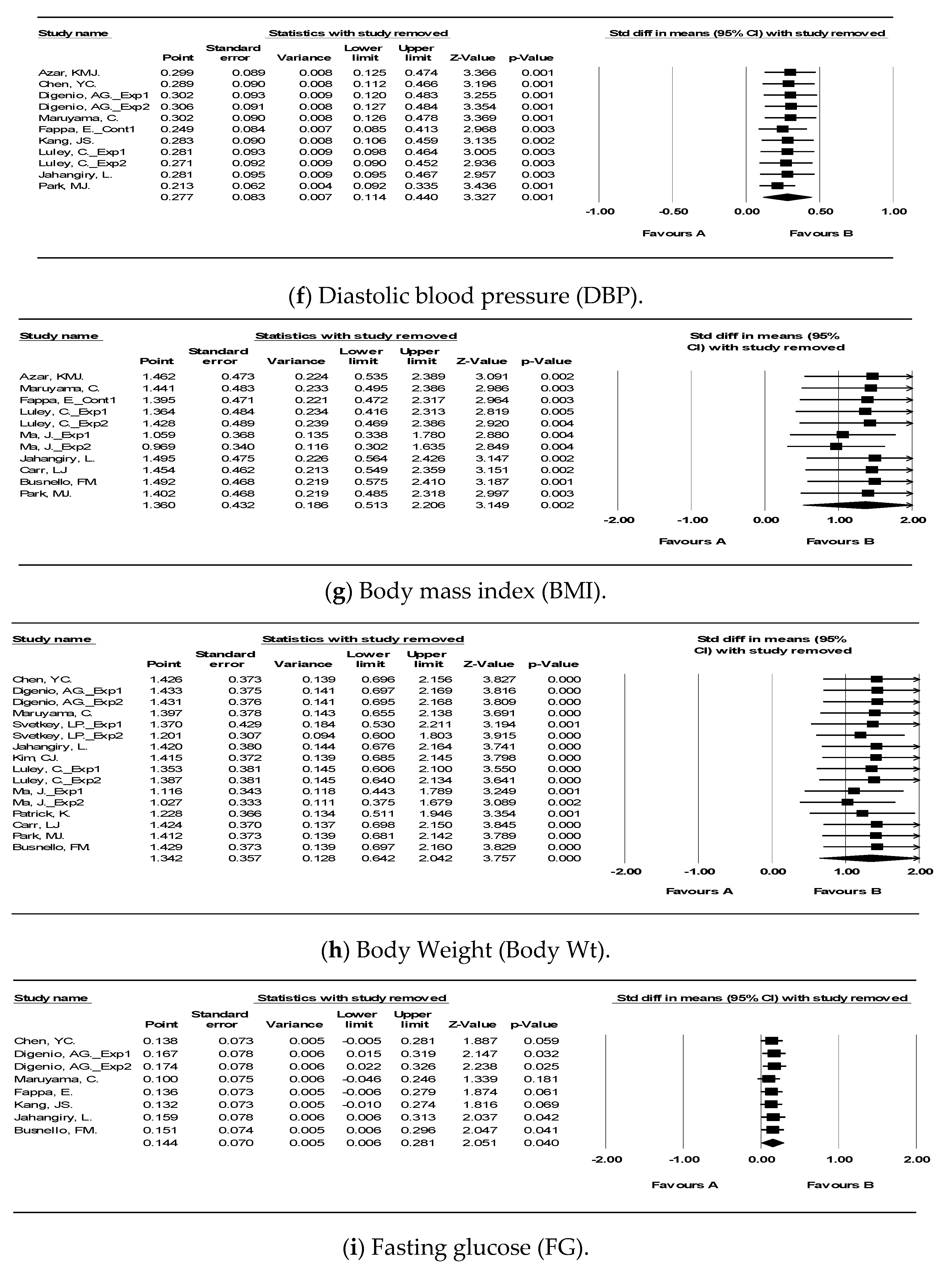
3.4.6. Diastolic Blood Pressure (DBP)
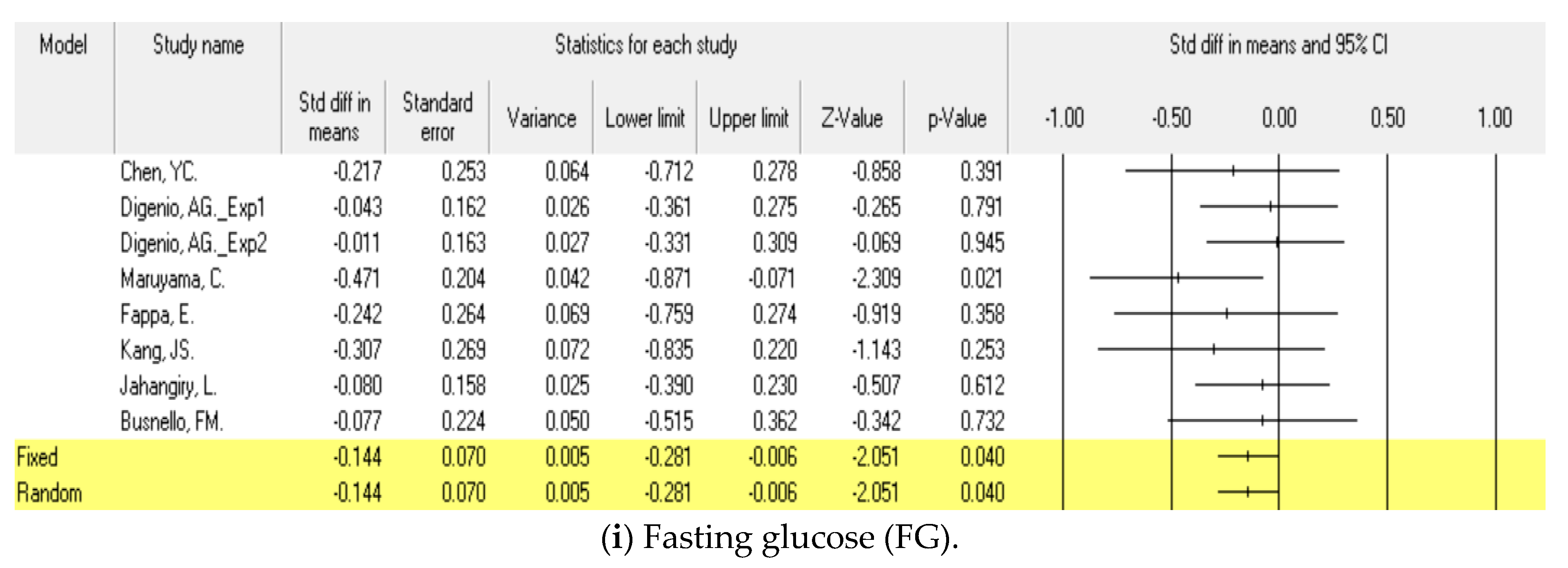
3.4.7. Fasting Glucose (FG)
3.5. Other Outcomes
3.5.1. Body Mass Index (BMI)
3.5.2. Body weight (Body Wt)
3.5.3. Hemoglobin A1c (HbA1c)
3.6. Sensitivity Analysis
4. Discussion
5. Recommendations for Future Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DBP | Diastolic blood pressure |
| FG | Fasting glucose |
| HbA1c | Hemoglobin A1c |
| HDL | High-density lipoprotein cholesterol |
| LDL | Low-density lipoprotein cholesterol |
| SBP | Systolic blood pressure |
| TG | Triglycerides |
| WC | Waist circumference |
| Wt | Weight |
References
- Schaan, C.W.; Cureau, F.V.; Salvo, D.; Kohl, H.W.; Schaan, B.D. Unhealthy snack intake modifies the association between screen-based sedentary time and metabolic syndrome in Brazilian adolescents. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 115. [Google Scholar] [CrossRef] [PubMed]
- Barice, J.; Andreotti, F.; Hennekens, C. Metabolic syndrome: The new silent killer. Med. Roundtable Gen. Med. Ed. 2019, 1, 28–33. [Google Scholar]
- Hirode, G.; Wong, R.J. Trends in the prevalence of metabolic syndrome in the United States, 2011–2016. JAMA 2020, 323, 2526–2528. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-H.; Lee, S.-H.; Shin, K.S.; Son, D.Y.; Kim, S.-H.; Joe, H.; Yoo, B.W.; Hong, S.H.; Cho, C.Y.; Shin, H.S.; et al. The Change of metabolic syndrome prevalence and its risk factors in Korean adults for decade: Korea National Health and Nutrition Examination Survey for 2008–2017. Korean J. Fam. Prac. 2020, 10, 44–52. [Google Scholar] [CrossRef]
- Tenorio-Jiménez, C.; Martínez-Ramírez, M.J.; Gil, Á.; Gómez-Llorente, C. Effects of probiotics on metabolic syndrome: A systematic review of randomized clinical trials. Nutrients 2020, 12, 124. [Google Scholar] [CrossRef] [Green Version]
- Who, J.; Consultation, F.E. Diet, Nutrition and the Prevention of Chronic Diseases; World Health Organization Technical Report Series; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Swindell, N.; Rees, P.; Fogelholm, M.; Drummen, M.; MacDonald, I.; Martinez, J.A.; Poppitt, S.D. Compositional analysis of the associations between 24-h movement behaviors and cardio-metabolic risk factors in overweight and obese adults with pre-diabetes from the PREVIEW study: Cross-sectional baseline analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–12. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, W.J.; Shultz, S.P.; Firestone, R.T.; George, L.; Kruger, R. Ethnic-specific suggestions for physical activity based on existing recreational physical activity preferences of New Zealand women. Aust. N. Z. J. Public Health 2019, 43, 443–450. [Google Scholar] [CrossRef] [Green Version]
- Davies, K.A.B.; Sprung, V.S.; Norman, J.A.; Thompson, A.; Mitchell, K.L.; Harrold, J.A.; Finlayson, G.; Gibbons, C.; Wilding, J.P.H.; Kemp, G.J.; et al. Physical activity and sedentary time: Association with metabolic health and liver fat. Med. Sci. Sports Exerc. 2019, 51, 1169–1177. [Google Scholar] [CrossRef] [Green Version]
- Vilchis-Gil, J.; Klünder-Klünder, M.; Flores-Huerta, S. Effect on the metabolic biomarkers in schoolchildren after a comprehensive intervention using electronic media and in-person sessions to change lifestyles: Community trial. J. Med. Internet Res. 2018, 20, e44. [Google Scholar] [CrossRef] [Green Version]
- National Cholesterol Education Program (US) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adults Treatment Panel III) Final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Kim, H.K.; Choi, K.H.; Lim, S.W.; Rhee, H.S. Development of prediction model for prevalence of metabolic syndrome using data mining: Korea National Health and Nutrition Examination Study. Convergence 2016, 14, 325–332. [Google Scholar] [CrossRef] [Green Version]
- Sung, E.J. Establishment of Roadmap for Intervention Study of Adolescent Obesity to Prevent and Control Metabolic Disease; Korea Centers for Disease Control and Prevention: Chungcheongbuk-do, Korea, 2016. [Google Scholar]
- Kim, H.S.; Yoo, B.N.; Lee, E.W. Evaluation of the national chronic diseases management policy: Performance and future directions. Public Health Aff. 2018, 2, 105–120. [Google Scholar] [CrossRef] [Green Version]
- Fynn, J.F.; Hardeman, W.; Milton, K.; Murphy, J.; Jones, A. A systematic review of the use and reporting of evaluation frameworks within evaluations of physical activity interventions. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Kang, M.A.; Lee, S.K. Effects of the e-Motivate4Change program on metabolic syndrome in young adults using health apps and wearable devices: Quasi-experimental study. J. Med. Internet Res. 2020, 2, e17031. [Google Scholar] [CrossRef] [PubMed]
- Jo, B.R. Comprehensive chronic disease management plan centered on local clinics seen as an overseas case. HIRA 2018, 12, 7–17. [Google Scholar]
- Lee, G.; Choi, H.Y.; Yang, S.J. Effects of dietary and physical activity interventions on metabolic syndrome: A meta-analysis. J. Korean Acad. Nurs. 2015, 45, 483–494. [Google Scholar] [CrossRef] [Green Version]
- Kim, N.H. Introduction of chronic disease management projects to strengthen local community-centered primary care and future development plans. HIRA 2018, 12, 18–27. [Google Scholar]
- Khang, Y.H.; Lee, S.I. Health inequalities policy in Korea: Current status and future challenges. J. Korean Med. Sci. 2012, 27, S33–S40. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Sa, J. Regional disparities in healthy eating and nutritional status in South Korea: Korea National Health and Nutrition Examination Survey 2017. Nutr. Res. Pract. 2020, 14, 679. [Google Scholar] [CrossRef]
- Reuter, C.; Bellettiere, J.; Liles, S.; Di, C.; Sears, D.D.; LaMonte, M.J.; Natarajan, L. Diurnal patterns of sedentary behavior and changes in physical function over time among older women: A prospective cohort study. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–11. [Google Scholar] [CrossRef]
- Kim, J.; Kim, I.; Sung, C.; Jeon, T.; Kim, T.; Kwon, S. Changes of maximal muscular strength, physical fitness and aerobic capacity in middle-aged male metabolic syndrome patients. J. Korea Sports 2018, 16, 339–347. [Google Scholar]
- Huh, J.H.; Kang, D.R.; Jang, J.-Y.; Shin, J.H.; Kim, J.-Y.; Choi, S.; Cho, E.J.; Park, J.-S.; Sohn, I.S.; Jo, S.-H.; et al. Metabolic syndrome epidemic among Korean adults: Korean survey of cardio metabolic syndrome. Atherosclerosis 2018, 277, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.J.; Kim, M.S.; Park, N.Y.; Lee, S.G.; Lee, Y.K. Effect of activity tracker & application use on adherence, metabolic syndrome factor and body composition in middle and senior-aged. Asian J. Kinesiol. 2018, 20, 28–37. [Google Scholar] [CrossRef]
- Huh, U.; Tak, Y.J.; Song, S.; Chung, S.W.; Sung, S.M.; Lee, C.W.; Ahn, H.Y. Feedback on physical activity through a wearable device connected to a mobile phone app in patients with metabolic syndrome: Pilot study. JMIR mHealth uHealth 2019, 7, e13381. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.G.; Salonurmi, T.; Jokelainen, T.; Karppinen, P.; Teeriniemi, A.; Han, J.; Savolainen, M.J. Lifestyle counselling by persuasive information and communications technology reduces prevalence of metabolic syndrome in a dose–response manner: A randomized clinical trial (PrevMetSyn). Ann. Med. 2020, 52, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.-G.; Lim, H.; Kim, Y.; Ju, Y.-S.; Lee, H.-J.; Jang, H.B.; Park, S.I.; Park, K.H. The effect of a multidisciplinary lifestyle intervention on obesity status, body composition, physical fitness, and cardiometabolic risk markers in children and adolescents with obesity. Nutrients 2019, 11, 137. [Google Scholar] [CrossRef] [Green Version]
- Tai, H.C.; Tzeng, I.; Liang, Y.C.; Liao, H.H.; Su, C.H.; Kung, W.M. Interventional effects of weight-loss policy in a healthy city among participants with metabolic syndrome. Int. J. Environ. Res. Public Health 2019, 16, 323. [Google Scholar] [CrossRef] [Green Version]
- Nolan, P.B.; Carrick-Ranson, G.; Stinear, J.W.; Reading, S.A.; Dalleck, L.C. Prevalence of metabolic syndrome and metabolic syndrome components in young adults: A pooled analysis. Prev. Med. Rep. 2017, 7, 211–215. [Google Scholar] [CrossRef]
- Carvalho, C.A.; Silva, A.A.M.; Assunção, M.C.F.; Fonseca, P.C.A.; Barbieri, M.A.; Bettiol, H.; Hébert, J.R. The dietary inflammatory index and insulin resistance or metabolic syndrome in young adults. Nutrition 2019, 58, 187–193. [Google Scholar] [CrossRef]
- Ghelani, D.P.; Moran, L.J.; Johnson, C.; Mousa, A.; Naderpoor, N. Mobile apps for weight management: A review of the latest evidence to inform practice. Front. Endocrinol. 2020, 11, 412. [Google Scholar] [CrossRef]
- Adamse, C.; Dekker-Van Weering, M.G.; van Etten-Jamaludin, F.; SStuiver, M.M. The effectiveness of exercise-based telemedicine on pain, physical activity and quality of life in the treatment of chronic pain: A systematic review. J. Telemed. Telecare 2018, 24, 511–526. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.R.; Park, H.R.; Lee, Y.M.; Lim, Y.S.; Song, K.H. Comparative study on prevalence and components of metabolic syndrome and nutritional status by occupation and gender: Based on the 2013 Korea National Health and Nutrition Examination Survey. J. Nutr. Health 2017, 50, 74–84. [Google Scholar] [CrossRef] [Green Version]
- Grisot, M.; Kempton, A.M.; Hagen, L.; Aanestad, M. Data-work for personalized care: Examining nurses’ practices in remote monitoring of chronic patients. Health Inform. J. 2019, 25, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Tonga, E.; Srikesavan, C.; Williamson, E.; E Lamb, S. Components, design and effectiveness of digital physical rehabilitation interventions for older people: A systematic review. J. Telemed. Telecare 2020, 6. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; He, X.; Shen, Y.; Yu, H.; Pan, J.; Zhu, W.; Zhou, J.; Bao, Y.; Hu, G.; Oehler, C. Effectiveness of smartphone app-based interactive management on glycemic control in Chinese patients with poorly controlled diabetes: Randomized controlled trial. J. Med. Internet Res. 2019, 21, e15401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yonker, L.M.; Zan, S.; Scirica, C.V.; Jethwani, K.; Kinane, T.B. “Friending” Teens: Systematic review of social media in adolescent and young adult health care. J. Med. Internet Res. 2015, 17, e4. [Google Scholar] [CrossRef] [Green Version]
- Jun, M.-K.; Ha, J.-Y. Effect of smartphone apps applying BodyThink program on obesity in adolescent girls. J. Korean Acad. Nurs. 2016, 46, 390–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilliard, M.E.; Eshtehardi, S.S.; Minard, C.G.; Saber, R.; Thompson, D.; Karaviti, L.P.; Rojas, Y.; Anderson, B. Strengths-based behavioral intervention for parents of adolescents with type 1 diabetes using an mHealth app (Type 1 doing well): Protocol for a pilot randomized controlled trial. JMIR Res. Protoc. 2018, 7, e77. [Google Scholar] [CrossRef]
- Wang, J.B.; Cadmus-Bertram, L.A.; Natarajan, L.; White, M.M.; Madanat, H.; Nichols, J.F.; Ayala, G.X.; Pierce, J.P. Wearable sensor/device (Fitbit One) and SMS text-messaging prompts to increase physical activity in overweight and obese adults: A randomized controlled trial. Telemed. e-Health 2015, 21, 782–792. [Google Scholar] [CrossRef] [Green Version]
- Chong, K.P.; Guo, J.Z.; Deng, X.; Woo, B.K. Consumer perception of wearable technology device: Retrospective review and analysis (Preprint). JMIR mHealth uHealth 2020, 8, e17544. [Google Scholar] [CrossRef]
- Oh, B.; Cho, B.; Han, M.K.; Choi, H.; Lee, M.N.; Kang, H.-C.; Lee, C.H.; Yun, H.; Kim, Y. The Effectiveness of mobile phone-based care for weight control in metabolic syndrome patients: Randomized controlled trial. JMIR mHealth uHealth 2015, 3, e83. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Bosak, K.A.; Yates, B.; Pozehl, B. Effects of an Internet Physical activity intervention in adults with metabolic syndrome. West. J. Nurs. Res. 2010, 32, 5–22. [Google Scholar] [CrossRef] [PubMed]
- Busnello, F.M.; Bodanese, L.C.; Pellanda, L.C.; Santos, Z.E.D.A. Intervenção nutricional e o impacto na adesão ao tratamento em pacientes com síndrome Metabólica. Arq. Bras. Cardiol. 2011, 97, 217–224. [Google Scholar] [CrossRef] [Green Version]
- Fappa, E.; Yannakoulia, M.; Ioannidou, M.; Skoumas, Y.; Pitsavos, C.; Stefanadis, C. Telephone counseling intervention improves dietary habits and metabolic parameters of patients with the metabolic syndrome: A randomized controlled trial. Rev. Diabet. Stud. 2012, 9, 36–45. [Google Scholar] [CrossRef] [Green Version]
- Jahangiry, L.; Shojaeizadeh, D.; Farhangi, M.A.; Yaseri, M.; Mohammad, K.; Najafi, M.; Montazeri, A. Interactive web-based lifestyle intervention and metabolic syndrome: Findings from the Red Ruby (a randomized controlled trial). Trials 2015, 16, 418. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.S.; Kang, H.S.; Jeong, Y. A web-based health promotion program for patients with metabolic syndrome. Asian Nurs. Res. 2014, 8, 82–89. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.-J.; Schlenk, E.A.; Kang, S.-W.; Park, J.-B. Effects of an internet-based lifestyle intervention on cardio-metabolic risks and stress in Korean workers with metabolic syndrome: A controlled trial. Patient Educ. Couns. 2015, 98, 111–119. [Google Scholar] [CrossRef]
- Luley, C.; Blaik, A.; Götz, A.; Kicherer, F.; Kropf, S.; Isermann, B.; Stumm, G.; Westphal, S. Weight loss by telemonitoring of nutrition and physical activity in patients with metabolic syndrome for 1 year. J. Am. Coll. Nutr. 2014, 33, 363–374. [Google Scholar] [CrossRef]
- Azar, K.M.; Koliwad, S.K.; Poon, T.; Xiao, L.; Lv, N.; Griggs, R.; Ma, J. The electronic CardioMetabolic program (eCMP) for patients with cardiometabolic risk: A randomized controlled trial. J. Med. Internet Res. 2016, 18, e134. [Google Scholar] [CrossRef]
- Carr, L.J.; Bartee, R.T.; Dorozynski, C.; Broomfield, J.F.; Smith, M.L.; Smith, D.T. Internet-delivered behavior change program increases physical activity and improves cardiometabolic disease risk factors in sedentary adults: Results of a randomized controlled trial. Prev. Med. 2008, 46, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Tsao, L.I.; Huang, C.H.; Yu, Y.Y.; Liu, I.L.; Jou, H.J. An Internet-based health management platform may effectively reduce the risk factors of metabolic syndrome among career women in Taiwan. J. Obstet. Gynecol. 2013, 52, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Digenio, A.G.; Mancuso, J.P.; Gerber, R.A.; Dvorak, R.V. Comparison of methods for delivering a lifestyle modification program for obese patients: A randomized trial. Ann. Intern. Med. 2009, 150, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Yank, V.; Xiao, L.; Lavori, P.W.; Wilson, S.R.; Rosas, L.G.; Stafford, R.S. Translating the diabetes prevention program lifestyle intervention for weight loss into primary care: A randomized trial. JAMA Intern. Med. 2013, 173, 113–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruyama, C.; Kimura, M.; Okumura, H.; Hayashi, K.; Arao, T. Effect of a worksite-based intervention program on metabolic parameters in middle-aged male white-collar workers: A randomized controlled trial. Prev. Med. 2010, 51, 11–17. [Google Scholar] [CrossRef]
- Park, M.-J.; Kim, H.-S.; Kim, K.-S. Cellular phone and Internet-based individual intervention on blood pressure and obesity in obese patients with hypertension. Int. J. Med. Inform. 2009, 78, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Patrick, K.; Raab, F.; A Adams, M.; Dillon, L.; Zabinski, M.; Rock, C.L.; Griswold, W.G.; Norman, G.J. A text message–based intervention for weight loss: Randomized controlled trial. J. Med. Internet Res. 2009, 11, e1. [Google Scholar] [CrossRef]
- Petrella, R.J.; Stuckey, M.I.; Shapiro, S.; Gill, D.P. Mobile health, exercise and metabolic risk: A randomized controlled trial. BMC Public Health 2014, 14, 1082. [Google Scholar] [CrossRef] [Green Version]
- Ueki, K.; Sakurai, N.; Tochikubo, O. Weight loss and blood pressure reduction in obese subjects in response to nutritional guidance using information communication technology. Clin. Exp. Hypertens. 2009, 31, 231–240. [Google Scholar] [CrossRef]
- Svetkey, L.P.; Stevens, V.J.; Brantley, P.J.; Appel, L.J.; Hollis, J.F.; Loria, C.M.; Vollmer, W.M.; Gullion, C.M.; Funk, K.; Smith, P.; et al. Comparison of strategies for sustaining weight loss: The weight loss maintenance randomized controlled trial. JAMA 2008, 299, 1139–1148. [Google Scholar] [CrossRef] [Green Version]
- Lagan, B.M.; Sinclair, M.; Kernohan, W.G. Internet use in pregnancy informs women’s decision making: A web-based survey. Birth 2010, 37, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Daud, M.H.; Ramli, A.S.; Abdul-Razak, S.; Isa, M.R.; Yusoff, F.H.; Baharudin, N.; Mohd-Nawawi, H. The EMPOWER-SUSTAIN e-Health intervention to improve patient activation and self-management behaviors among individuals with metabolic syndrome in primary care: Study protocol for a pilot randomized controlled trial. Trials 2020, 21, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aida, A.; Svensson, T.; Svensson, A.K.; Urushiyama, H.; Okushin, K.; Oguri, G.; Kubota, N.; Koike, K.; Nangaku, M.; Kadowaki, T.; et al. Using mHealth to provide mobile app users with visualization of health checkup data and educational videos on lifestyle-related diseases: Methodological framework for content development. JMIR mHealth uHealth 2020, 8, e20982. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.M.J.; Lee, J.H.; Shim, J.-S.; Yeom, H.; Lee, S.J.; Jeon, Y.W.; Kim, H.C. Effect of smartphone-based lifestyle coaching app on community-dwelling population with moderate metabolic abnormalities: Randomized controlled trial. J. Med. Internet Res. 2020, 22, e17435. [Google Scholar] [CrossRef] [PubMed]
- Willcox, J.; Campbell, K.; McCarthy, E.A.; Wilkinson, S.A.; Lappas, M.; Ball, K.; Fjeldsoe, B.S.; Griffiths, A.; Whittaker, R.; Maddison, R.; et al. Testing the feasibility of a mobile technology intervention promoting healthy gestational weight gain in pregnant women (txt4two)—Study protocol for a randomized controlled trial. Trials 2015, 16, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, D.; Kongpakpaisarn, K.; Bohra, C. Trends in the prevalence of metabolic syndrome and its components in the United States 2007–2014. Int. J. Cardiol. 2018, 259, 216–219. [Google Scholar] [CrossRef]
- Jenkins, D.J.; Kendall, C.; Augustin, L.S.; Franceschi, S.; Hamidi, M.; Marchie, A.; Jenkins, A.L.; Axelsen, M. Glycemic index: Overview of implications in health and disease. Am. J. Clin. Nutr. 2002, 76, 266S–273S. [Google Scholar] [CrossRef]
- Rainie, L.; Zickuhr, K. Americans’ views on mobile etiquette. Pew Res. Cent. 2015, 26, 948–958. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Public Year | Ref No | Country | Subject | Criteria | Intervention | Control | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| N (M:F) | Age (Years) Mean (SD) | Inclusion | Intervention (Contents) | Intervention (Components and Technique) | Duration (Months) | f/u (Months) | ||||
| Bosak, KA., 2010 | [46] | USA | 22 (16:6) | 50.94 (7.81) | Adults with metabolic syndrome | Exercise | Web-based education programme (Internet physical activity intervention) based on the ATP III guidelines Self-efficacy strategies e-mail feedback, Quiz (week 5, week 6) Discussion via electronic discussion board | 1.5 | 1.5 | Usual care |
| Busnello, FM., 2011 | [47] | Brazil | 80 (23:57) | 58.50 (8.50) | Patients with metabolic syndrome | Diet | Individual standard diet and a “Manual of Nutritional Guidelines for Patients with Metabolic Syndrome” Telephone counselling Different printed material about nutrition guidelines | 4 | 4 | Usual care (nutritional guidance) |
| Fappa, E., 2012 (1) Cont 1 (2) Cont 2 | [48] | Greece | 87 (50:37) | 49.00 (11.80) | Patients with metabolic syndrome | Exercise, Diet | Based on the goal setting theory Motivational and behavioral strategies -Telephone counselling intervention (1~2 times/month, total 7 times) | 6 | 6 | Cont. 1: Usual care Cont. 2: Face-to face counselling (1~2 times/month, total 7 times) |
| Jahangiry, L., 2015 | [49] | Iran | 160 (106:54) | 44.05 (10.05) | Patients with metabolic syndrome | Exercise, Diet | Interactive web-based programme lifestyle intervention (the Healthy Heart Profile: Education, diet information, estimation of FSR, personal health records), ∙e-mail and encouraged | 6 | 6 | |
| Kang, JS., 2014 | [50] | Korea | 56 (46:10) | 37.93 (10.13) | Adults with metabolic syndrome | Exercise, Diet | Web-based health promotion programme (audio-video clips on diet and exercise using the internet) One of researchers contacted the participants by telephone to reinforcement No offline coaching | 2 | 2 | Usual care (Brief booklet) |
| Kim, CJ., 2015 | [51] | Korea | 48 (48:0) | 39.63 (7.27) | Male workers with metabolic syndrome | Exercise, Diet | Internet-based Best Exercise Super Trainer (BEST program: Multi-component WBI incorporating physical activity/weight control, personal counselling) lifestyle intervention Based on transtheoretical model (TTM) Internet-based online counselling (1 times/week) Short mobile text messages (SMS) | 4 | 4 | Usual care (Brief booklet)+ SMS |
| Luley, C., 2014 (1) Exp 1 (2) Exp 2 | [52] | Germany | 178 (105:73) | 50.25 (7.96) | Patients with metabolic syndrome | Exercise, Diet | Mobile technology based lifestyle intervention (nutrition and physical activity): Both intervention groups were issued accelerometers (Aipermotion 440), which measured physical activity, recorded daily weight and calorie intake, and transmitted these data to a central server for use by patient carers. +Exp 1: Active Body Control (ABC) lifestyle program, information and motivation by letters (1 times/week) +Exp 2: 4 sigma coaching intervention, Telephone counselling (1 times/month) | 12 | 4,8,12 | Usual care |
| Azar, KMJ., 2016 | [53] | USA | 74 (30:44) | 59.70 (11.20) | Adults with cardiometabolic risk (1) BMI ≥ 35 kg/m2 and prediabetes, previous gestational diabetes and/or metabolic syndrome (2) BMI ≥ 30 kg/m2 and type 2 diabetes and/or cardiovascular disease | Exercise, Diet | Electronic CardioMetabolic Program (eCMP, web-based comprehensive program) The delivery of evidence-based curricula using online tools Pre-recorded didactic videos presented by physicians, nutritionists, exercise physiologists, and lifestyle coaches. -A comprehensive online platform and participant portal for hosting programme materials (e.g., homework assignments, didactic videos, and calendars) Face-to-face group meetings (1 times/week) via web-based video conferencing Mobile monitoring devices: Self-monitoring, bio-feedback, remote data capture (wireless body scale (Fitbit and Withings Smart Scale), pedometer) Coach-led virtual small groups via real-time, encrypted, web-based videoconferencing (4 times/month) Coach-led in-person sessions (periodic 7 sessions) | 6 | 3, 6 | No treatment |
| Carr, LJ., 2008 | [54] | USA | 32 (6:26) | 45.90 (2.75) | Adults with metabolic syndrome risk Sedentary overweight (BMI ≥ 25.0 kg/m2) | Exercise | The ALED-I (active living every day internet-delivered) theory-based behavior change programme (based on transtheoretical model (TTM)) Website content and functionality (Blair et al., 2001): Interactive activities and behavior modification strategies | 4 | 4 | No treatment |
| Chen, YC., 2013 | [55] | Taiwan | 63 (0:63) | 43.80 (9.07) | Full time career women with metabolic syndrome risk | Exercise, Diet | Internet-based Health Management Platform (HMP) program The Internet platform included a health examination database, nutrition management system, and exercise management system. Participants were able to log into the system with individual passwords to check personal test data and upload personal dietary and exercise records. Health management experts also provided nutrition and exercise recommendations and advice according to these records. | 1.5 | 1.5 | No treatment |
| Digenio, AG., 2009 (1) Exp 1/Cont 1 (2) Exp 1/Cont 2 (3) Exp 1/Cont 3 (4) Exp 2/Cont 1 (5) Exp 2/Cont 2 (6) Exp 2/Cont 3 | [56] | USA | 376 (50:326) | 43.79 (9.51) | Patients with metabolic syndrome risk 30 kg/m2 < BMI < 40 kg/m2 | Exercise, Diet | Lifestyle modification counselling -Exp 1: High frequency telephone counselling (2~4 times/month) -Exp 2: High frequency E-mail counselling (2~4 times/month) | 6 | 0.5, 1, 3, 6 | -Cont 1: No treatment -Cont 2: High frequency face to face counselling (2~4 times/month) -Cont 3: Low frequency fact to face counselling (1 times/month) |
| Ma, J., 2013 (1) Exp 1 (2) Exp 2 | [57] | USA | 241 (129:112) | 52.90 (10.60) | Patients with metabolic syndrome risk BMI ≥ 25 kg/m2 fasting glucose level 100–125 mg/dL | Exercise, Diet | ∙Lifestyle intervention -Exp 1: A coach-led, group delivered intervention (group Lifestyle Balance, GLB, 12 session), web-based education, e-mail (or telephone) motivational message -Exp 2: A self-directed home-based DVD intervention | 15 (Intensive intervention 3, maintenance 12) | 15 | Usual care |
| Maruyama, C., 2010 | [58] | Japan | 101 (101:0) | 39.49 (7.89) | Patients with metabolic syndrome risk | Exercise, Diet | Life Style Modification web-based counselling programme (Physical Activity and Nutrition), counselling (1 times/month), web site advice (1 times/month) | 4 | 4 | No treatment |
| Park, MJ., 2009 | [59] | Korea | 49 (26:23) | 53.8 (8.89) | Patients with metabolic syndrome risk (hypertension and obesity) BP > 120/80 mmHg BMI > 23 kg/m2 | Exercise | Cellular telephone and Internet-based individual intervention Web-based diary through the internet or by cellular telephones (weekly) Internet recommendation and SMS message | 2 | 2 | No treatment |
| Patrick, K., 2009 | [60] | USA | 65 (13:52) | 44.90 (7.70) | Patients with metabolic syndrome risk Overweight (BMI > 25–39.9 kg/m2) | Exercise, Diet | Text Message-based intervention (weight loss program) Counselling sessions & web site advice (1 times/month) SMS or MMS 2~5 times/day | 4 | 4 | Usual care (Printed educational materials) |
| Petrella, R., 2014 | [61] | Canada | 149 (38:111) | 57.83 (9.10) | Patients with ≥ 2 metabolic syndrome risk | Exercise | Mobile health intervention (Individualized exercise prescription) Technology kit (telephone with anywhere health monitoring application, Bluetooth™ enabled blood pressure monitor, a glucometer, and a pedometer) for home monitoring of biometrics and physical activity | 12 | 3, 6, 12 | Individualized active exercise prescription |
| Svetkey, LP., 2008 (1) Exp 1 (2) Exp 2 | [62] | USA | 1032 (378:654) | 55.60 (8.70) | Patients with metabolic syndrome risk BMI 25–45 kg/m2 Taking medication for hypertension, dyslipidemia, or both | Exercise, Diet | Weight loss maintenance interventions -Exp 1: Interactive technology-based intervention (monthly), Web site education, e-mail, telephone (2 times/month) -Exp 2: Personal contact (1 hrs/month), telephone (5–15 min/month) | 12, 30 | 12, 30 | No treatment |
| Ueki, K., 2009 | [63] | Japan | 52 (22:19) | 55.37 (11.64) | Patients with metabolic syndrome risk | Diet | Information Communication Technology (ICT) method Using sensors attached to the BP monitor, scale, and pedometer, the data were transmitted via the Internet or telephone circuitry from a telemetric information terminal Nutritional guidance using Telemetric-communication technology (e-mail or fax) | 3 | 3 | Face-to face guidance |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, G.; Lee, J.-S.; Lee, S.-K. A Technology-Mediated Interventional Approach to the Prevention of Metabolic Syndrome: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 512. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020512
Kim G, Lee J-S, Lee S-K. A Technology-Mediated Interventional Approach to the Prevention of Metabolic Syndrome: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(2):512. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020512
Chicago/Turabian StyleKim, Gaeun, Ji-Soo Lee, and Soo-Kyoung Lee. 2021. "A Technology-Mediated Interventional Approach to the Prevention of Metabolic Syndrome: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 2: 512. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020512