Identification of Risk Factors to Predict the Occurrences of Relapses in Individuals with Schizophrenia Spectrum Disorder in Iran

 , , and
, , and 
Abstract
:1. Introduction
2. Method
2.1. Procedure
2.2. Data Collection Based on the Medical Records: Variables of Interest
2.3. Definition of Relapse
2.4. Definition of Medication Adherence
2.5. Sample Selection
2.6. Statistical Analysis
3. Results
3.1. General Pbservations
3.2. Relapses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kahn, R.S.; Sommer, I.E.; Murray, R.M.; Meyer-Lindenberg, A.; Weinberger, D.R.; Cannon, T.D.; O’Donovan, M.; Correll, C.U.; Kane, J.M.; van Os, J.; et al. Schizophrenia. Nat. Rev. Dis. Primers 2015, 1, 15067. [Google Scholar] [CrossRef] [PubMed]
- Falkai, P.; Rossner, M.J.; Schulze, T.G.; Hasan, A.; Brzózka, M.M.; Malchow, B.; Honer, W.G.; Schmitt, A. Kraepelin revisited: Schizophrenia from degeneration to failed regeneration. Mol. Psychiatry 2015, 20, 671–676. [Google Scholar] [CrossRef]
- Leucht, S.; Hasan, A.; Jäger, M.; Vauth, R. Schizophrenien und andere psychotische Störungen (schizophrenia and further psychotic disorders). In Psychische Erkrankungen; Klinik und Therapie (Psychiatric Disorders, Symptoms and Therapy); Berger, M., Ed.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 301–362. [Google Scholar]
- Olabi, B.; Ellison-Wright, I.; McIntosh, A.M.; Wood, S.J.; Bullmore, E.; Lawrie, S.M. Are there progressive brain changes in schizophrenia? A meta-analysis of structural magnetic resonance imaging studies. Biol. Psychiatry 2011, 70, 88–96. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, S.; Northstone, K.; Gadd, C.; Walker, J.; Margelyte, R.; Richards, A.; Whiting, P. Models to predict relapse in psychosis: A systematic review. PLoS ONE 2017, 12, e0183998. [Google Scholar] [CrossRef] [Green Version]
- Dazzan, P.; Arango, C.; Fleischacker, W.; Galderisi, S.; Glenthøj, B.; Leucht, S.; Meyer-Lindenberg, A.; Kahn, R.; Rujescu, D.; Sommer, I.; et al. Magnetic resonance imaging and the prediction of outcome in first-episode schizophrenia: A review of current evidence and directions for future research. Schizophr. Bull. 2015, 41, 574–583. [Google Scholar] [CrossRef] [Green Version]
- Chee, T.T.; Chua, L.; Morrin, H.; Lim, M.F.; Fam, J.; Ho, R. Neuroanatomy of Patients with Deficit Schizophrenia: An Exploratory Quantitative Meta-Analysis of Structural Neuroimaging Studies. Int. J. Environ. Res. Public Health 2020, 17, 6227. [Google Scholar] [CrossRef]
- Eisner, E.; Drake, R.; Lobban, F.; Bucci, S.; Emsley, R.; Barrowclough, C. Comparing early signs and basic symptoms as methods for predicting psychotic relapse in clinical practice. Schizophr. Res. 2018, 192, 124–130. [Google Scholar] [CrossRef]
- Emsley, R.; Chiliza, B.; Asmal, L.; Harvey, B.H. The nature of relapse in schizophrenia. BMC Psychiatry 2013, 13, 50. [Google Scholar] [CrossRef] [Green Version]
- Jablensky, A. Schizophrenia: Recent epidemiologic issues. Epidemiol. Rev. 1995, 17, 10–20. [Google Scholar] [CrossRef]
- World Health Organization. Schizophrenia: A Multinational Study, a Summary of the Initial Evaluation Phase of the International Pilot Study of Schizophrenia; World Health Organization: Geneva, Switzerland, 1975. [Google Scholar]
- Lecomte, T.; Potvin, S.; Samson, C.; Francoeur, A.; Hache-Labelle, C.; Gagné, S.; Boucher, J.; Bouchard, M.; Mueser, K.T. Predicting and preventing symptom onset and relapse in schizophrenia-A metareview of current empirical evidence. J. Abnorm. Psychol. 2019, 128, 840–854. [Google Scholar] [CrossRef]
- Mortensen, P.B.; Pedersen, C.B.; Westergaard, T.; Wohlfahrt, J.; Ewald, H.; Mors, O.; Andersen, P.K.; Melbye, M. Effects of family history and place and season of birth on the risk of schizophrenia. N. Engl. J. Med. 1999, 340, 603–608. [Google Scholar] [CrossRef]
- Rahmati, M.; Rahgozar, M.; Fadaei, F.; Bakhshi, E.; Cheraghi, L. Identifying Some Risk Factors of Time to Relapses in Schizophrenic Patients using Bayesian Approach with Event-Dependent Frailty Model. Iran. J. Psychiatry 2015, 10, 123–127. [Google Scholar]
- David, A.S.; Prince, M. Psychosis following head injury: A critical review. J. Neurol. Neurosurg. Psychiatry 2005, 76, i53–i60. [Google Scholar] [CrossRef]
- Noorbala, A.A.; Akhondzadeh, S. Mental health study process into prevalence of mental disorders in Iran. Arch. Iran. Med. 2015, 18, 74–75. [Google Scholar]
- Mohammadi, M.R.; Davidian, H.; Noorbala, A.A.; Malekafzali, H.; Naghavi, H.R.; Pouretemad, H.R.; Yazdi, S.A.; Rahgozar, M.; Alaghebandrad, J.; Amini, H.; et al. An epidemiological survey of psychiatric disorders in Iran. Clin. Pract. Epidemiol. Ment. Health 2005, 1, 16. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Morisky, D.E.; Ang, A.; Krousel-Wood, M.; Ward, H.J. Predictive validity of a medication adherence measure in an outpatient setting. J. Clin. Hypertens 2008, 10, 348–354. [Google Scholar] [CrossRef] [Green Version]
- Morisky, D.E.; Green, L.W.; Levine, D.M. Concurrent and predictive validity of a self-reported measure of medication adherence. Med. Care 1986, 24, 67–74. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders 5th Edition: DSM 5; American Psychiatric Association: Arlington VA, USA, 2013. [Google Scholar]
- Barkhof, E.; Meijer, C.J.; de Sonneville, L.M.; Linszen, D.H.; de Haan, L. Interventions to improve adherence to antipsychotic medication in patients with schizophrenia—A review of the past decade. Eur. Psychiatry 2012, 27, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Zhao, S.; Sampson, S.; Xia, J.; Jayaram, M.B. Psychoeducation (brief) for people with serious mental illness. Cochrane Database Syst. Rev. 2015, 4, Cd010823. [Google Scholar] [CrossRef]
- Sendt, K.V.; Tracy, D.K.; Bhattacharyya, S. A systematic review of factors influencing adherence to antipsychotic medication in schizophrenia-spectrum disorders. Psychiatry Res. 2015, 225, 14–30. [Google Scholar] [CrossRef] [PubMed]
- Hegedüs, A.; Kozel, B. Does adherence therapy improve medication adherence among patients with schizophrenia? A systematic review. Int. J. Ment. Health Nurs. 2014, 23, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Gray, R.; Bressington, D.; Ivanecka, A.; Hardy, S.; Jones, M.; Schulz, M.; von Bormann, S.; White, J.; Anderson, K.H.; Chien, W.T. Is adherence therapy an effective adjunct treatment for patients with schizophrenia spectrum disorders? A systematic review and meta-analysis. BMC Psychiatry 2016, 16, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petry, N.M.; Rash, C.J.; Byrne, S.; Ashraf, S.; White, W.B. Financial reinforcers for improving medication adherence: Findings from a meta-analysis. Am. J. Med. 2012, 125, 888–896. [Google Scholar] [CrossRef] [Green Version]
- Kishimoto, T.; Hagi, K.; Nitta, M.; Leucht, S.; Olfson, M.; Kane, J.M.; Correll, C.U. Effectiveness of Long-Acting Injectable vs Oral Antipsychotics in Patients With Schizophrenia: A Meta-analysis of Prospective and Retrospective Cohort Studies. Schizophr. Bull. 2018, 44, 603–619. [Google Scholar] [CrossRef] [Green Version]
- Kishimoto, T.; Robenzadeh, A.; Leucht, C.; Leucht, S.; Watanabe, K.; Mimura, M.; Borenstein, M.; Kane, J.M.; Correll, C.U. Long-acting injectable vs oral antipsychotics for relapse prevention in schizophrenia: A meta-analysis of randomized trials. Schizophr. Bull. 2014, 40, 192–213. [Google Scholar] [CrossRef] [Green Version]
- Park, S.C.; Choi, M.Y.; Choi, J.; Park, E.; Tchoe, H.J.; Suh, J.K.; Kim, Y.H.; Won, S.H.; Chung, Y.C.; Bae, K.Y.; et al. Comparative Efficacy and Safety of Long-acting Injectable and Oral Second-generation Antipsychotics for the Treatment of Schizophrenia: A Systematic Review and Meta-analysis. Clin. Psychopharmacol. Neurosci. 2018, 16, 361–375. [Google Scholar] [CrossRef]
- Saucedo Uribe, E.; Carranza Navarro, F.; Guerrero Medrano, A.F.; García Cervantes, K.I.; Álvarez Villalobos, N.A.; Acuña Rocha, V.D.; Méndez Hernández, M.; Millán Alanís, J.M.; Hinojosa Cavada, C.M.; Zúñiga Hernández, J.A.; et al. Preliminary efficacy and tolerability profiles of first versus second-generation Long-Acting Injectable Antipsychotics in schizophrenia: A systematic review and meta-analysis. J. Psychiatr. Res. 2020, 129, 222–233. [Google Scholar] [CrossRef]
- Olagunju, A.T.; Clark, S.R.; Baune, B.T. Long-acting atypical antipsychotics in schizophrenia: A systematic review and meta-analyses of effects on functional outcome. Aust. N. Z. J. Psychiatry 2019, 53, 509–527. [Google Scholar] [CrossRef] [Green Version]
- Lafeuille, M.H.; Dean, J.; Carter, V.; Duh, M.S.; Fastenau, J.; Dirani, R.; Lefebvre, P. Systematic review of long-acting injectables versus oral atypical antipsychotics on hospitalization in schizophrenia. Curr. Med Res. Opin. 2014, 30, 1643–1655. [Google Scholar] [CrossRef]
- Rubio, J.M.; Schoretsanitis, G.; John, M.; Tiihonen, J.; Taipale, H.; Guinart, D.; Malhotra, A.K.; Correll, C.U.; Kane, J.M. Psychosis relapse during treatment with long-acting injectable antipsychotics in individuals with schizophrenia-spectrum disorders: An individual participant data meta-analysis. Lancet Psychiatry 2020, 7, 749–761. [Google Scholar] [CrossRef]
- Gvion, Y.; Levi-Belz, Y.; Hadlaczky, G.; Apter, A. On the role of impulsivity and decision-making in suicidal behavior. World J. Psychiatry 2015, 5, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Calati, R.; Nemeroff, C.B.; Lopez-Castroman, J.; Cohen, L.J.; Galynker, I. Candidate biomarkers of suicide crisis syndrome: What to test next? A concept paper. Int. J. Neuropsychopharmacol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Jahangard, L.; Shayganfard, M.; Ghiasi, F.; Salehi, I.; Haghighi, M.; Ahmadpanah, M.; Sadeghi Bahmani, D.; Brand, S. Serum oxytocin concentrations in current and recent suicide survivors are lower than in healthy controls. J. Psychiatr. Res. 2020, 128, 75–82. [Google Scholar] [CrossRef]
- Joiner, T.E.; Hom, M.A.; Hagan, C.R.; Silva, C. Suicide as a derangement of the self-sacrificial aspect of eusociality. Psychol. Rev. 2016, 123, 235–254. [Google Scholar] [CrossRef] [Green Version]
- Nazarzadeh, M.; Bidel, Z.; Ayubi, E.; Asadollahi, K.; Carson, K.V.; Sayehmiri, K. Determination of the social related factors of suicide in Iran: A systematic review and meta-analysis. BMC Public Health 2013, 13, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmadpanah, M.; Astinsadaf, S.; Akhondi, A.; Haghighi, M.; Sadeghi Bahmani, D.; Nazaribadie, M.; Jahangard, L.; Holsboer-Trachsler, E.; Brand, S. Early maladaptive schemas of emotional deprivation, social isolation, shame and abandonment are related to a history of suicide attempts among patients with major depressive disorders. Compr. Psychiatry 2017, 77, 71–79. [Google Scholar] [CrossRef]
- Ahmadpanah, M.; Rahighi, A.H.; Haghighi, M. Female Gender, Marital and Family Problems, and Feelings of Guilt Are Related to Self-Immolation Suicide Attempts. Neuropsychobiology 2017, 76, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, G.; Baxi, M.; Witte, T.; Robinson, J.L. A Neural Basis for the Acquired Capability for Suicide. Front. Psychiatry 2016, 7, 125. [Google Scholar] [CrossRef] [Green Version]
- Bryan, C.J.; Rudd, M.D. Advances in the assessment of suicide risk. J. Clin. Psychol. 2006, 62, 185–200. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Nock, M.K. The psychology of suicidal behaviour. Lancet Psychiatry 2014, 1, 73–85. [Google Scholar] [CrossRef]
- Rezayat, F.; Mohammadi, E.; Fallahi-Khoshknab, M. The process of responding to stigma in people with schizophrenia spectrum disorders and families: A grounded theory study. Perspect. Psychiatr Care 2020, 56, 564–573. [Google Scholar] [CrossRef] [PubMed]
- Rezayat, F.; Mohammadi, E.; Fallahi-Khoshknab, M.; Sharifi, V. Experience and the meaning of stigma in patients with schizophrenia spectrum disorders and their families: A qualitative study. Jpn. J. Nurs. Sci. 2019, 16, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, H.; Seyedfatemi, N.; Namdar Areshtanab, H.; Ranjbar, F.; Thornicroft, G.; Whitehead, B.; Rahmani, F. Barriers to Family Caregivers’ Coping With Patients With Severe Mental Illness in Iran. Qual. Health Res. 2018, 28, 987–1001. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Vancampfort, D.; Hallgren, M.; Firth, J.; Veronese, N.; Solmi, M.; Brand, S.; Cordes, J.; Malchow, B.; Gerber, M.; et al. EPA guidance on physical activity as a treatment for severe mental illness: A meta-review of the evidence and Position Statement from the European Psychiatric Association (EPA), supported by the International Organization of Physical Therapists in Mental Health (IOPTMH). Eur. Psychiatry 2018, 54, 124–144. [Google Scholar]
- Dauwan, M.; Begemann, M.J.; Heringa, S.M.; Sommer, I.E. Exercise Improves Clinical Symptoms, Quality of Life, Global Functioning, and Depression in Schizophrenia: A Systematic Review and Meta-analysis. Schizophr. Bull. 2016, 42, 588–599. [Google Scholar] [CrossRef]
- Every-Palmer, S.; Huthwaite, M.A.; Elmslie, J.L.; Grant, E.; Romans, S.E. Long-term psychiatric inpatients’ perspectives on weight gain, body satisfaction, diet and physical activity: A mixed methods study. BMC Psychiatry 2018, 18, 300. [Google Scholar] [CrossRef] [Green Version]
- Knochel, C.; Oertel-Knochel, V.; O’Dwyer, L.; Prvulovic, D.; Alves, G.; Kollmann, B.; Hampel, H. Cognitive and behavioural effects of physical exercise in psychiatric patients. Prog. Neurobiol. 2012, 96, 46–68. [Google Scholar] [CrossRef]
- Rezaie, L.; Shafaroodi, N.; Philips, D. The barriers to participation in leisure time physical activities among Iranian women with severe mental illness: A qualitative study. Mental Health Phys. Act. 2017, 13, 171–177. [Google Scholar] [CrossRef]
- Rosenbaum, S.; Tiedemann, A.; Stanton, R.; Parker, A.; Waterreus, A.; Curtis, J.; Ward, P.B. Implementing evidence-based physical activity interventions for people with mental illness: An Australian perspective. Australas Psychiatry 2015. [Google Scholar] [CrossRef]
- Stubbs, B.; Vancampfort, D.; Firth, J.; Hallgren, M.; Schuch, F.; Veronese, N.; Solmi, M.; Gaughran, F.; Kahl, K.G.; Rosenbaum, S.; et al. Physical activity correlates among people with psychosis: Data from 47 low- and middle-income countries. Schizophr. Res. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vancampfort, D.; Firth, J.; Schuch, F.B.; Rosenbaum, S.; Mugisha, J.; Hallgren, M.; Probst, M.; Ward, P.B.; Gaughran, F.; De Hert, M.; et al. Sedentary behavior and physical activity levels in people with schizophrenia, bipolar disorder and major depressive disorder: A global systematic review and meta-analysis. World Psychiatry 2017, 16, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Watson, P.; Zhang, J.P.; Rizvi, A.; Tamaiev, J.; Birnbaum, M.L.; Kane, J. A meta-analysis of factors associated with quality of life in first episode psychosis. Schizophr. Res. 2018, 202, 26–36. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Total | Male | Female | |
|---|---|---|---|---|
| N (%) | 401 (100) | 255 (63.59) | 146 (36.40) | |
| M (SD) | M (SD) | M (SD) | ||
| Age | 37.81 (9.90) | 37.56 (10.06) | 38.33 (9.62) | |
| Age at onset of SSD (years) | 26.24 (9.05) | 25.64 (8.70) | 27.29 (9.56) | |
| Frequency (%) | Frequency (%) | Frequency (%) | ||
| Marital status | Married | 104 (25.9) | 63 (24.7) | 41 (28.1) |
| Single | 250 (62.3) | 167 (65.5) | 83 (56.8) | |
| Divorced/widowed | 47 (11.7) | 25 (9.8) | 22 (15.1) | |
| Place of birth | Urban | 279 (69.6) | 186 (72.9) | 93 (63.7) |
| Rural | 122 (30.4) | 69 (27.1) | 53 (36.3) | |
| Employment status | Employee | 98 (24.4) | 92 (36.1) | 6 (4.1) |
| Unemployed | 303 (75.6) | 163 (63.9) | 140 (95.9) | |
| Substance Abuse | No | 306 (76.3) | 170 (66.7) | 136 (93.2) |
| Yes | 95 (23.7) | 85 (33.3) | 10 (6.8) | |
| History of head trauma | No | 380 (94.8) | 239 (93.7) | 141 (96.6) |
| Yes | 21 (5.2) | 16 (6.3) | 5 (3.4) | |
| Family history of schizophrenia | No | 372 (92.8) | 236 (92.5) | 136 (93.2) |
| Yes | 29 (7.2) | 19 (7.5) | 10 (6.8) | |
| Mode of Onset | Acute | 41 (10.2) | 28 (11) | 13 (8.9) |
| Gradual | 360 (89.8) | 227 (89) | 133 (91.1) | |
| Medication Adherence | Non-Adherence | 234 (58.4) | 149 (58.4) | 85 (58.2) |
| Adherence | 167 (41.6) | 106 (41.6) | 61 (41.8) | |
| Season of Birth | Spring | 120 (29.9) | 74 (29) | 46 (31.5) |
| Summer | 123 (30.7) | 79 (31) | 44 (30.1) | |
| Autumn | 69 (17.2) | 47 (18.4) | 22 (15.1) | |
| Winter | 89 (22.2) | 55 (21.6) | 34 (23.3) | |
| History of suicide attempt | No | 325 (81.0) | 203 (79.6) | 122 (83.6) |
| Yes | 76 (19.0) | 52 (20.4) | 24 (16.4) | |
| Number of relapses | One to two relapses | 222 (55.4) | 144 (56.5) | 78 (53.4) |
| Three to four relapses | 114 (28.4) | 70 (27.5) | 44 (30.1) | |
| Five to eleven relapses | 65 (16.2) | 41 (16.1) | 24 (16.4) | |
| Variable | Categories | Crude HR * (95% CI) | Adjusted HR (95% CI) | p-Value |
|---|---|---|---|---|
| Age of onset of schizophrenia | 0.99 (0.98–1.00) | 0.99(0.98–1.00) | 0.044 | |
| Gender | (male) * | |||
| female | 1.00 (0.85–1.18) | |||
| Marital Status | (married) | |||
| single | 1.15 (0.94–1.41) | |||
| divorced or widowed | 1.12 (0.84–1.50) | |||
| Place of Birth | (urban) | |||
| rural | 0.91 (0.75–1.09) | |||
| Employment status | unemployed | |||
| employed | 0.91 (0.74–1.12) | |||
| Substance Abuse | (no) | |||
| yes | 1.08 (0.90–1.31) | |||
| History of head trauma | (no) | |||
| yes | 1.12 (0.79–1.60) | |||
| Family history of schizophrenia | (no) | |||
| yes | 1.23 (0.92–1.65) | |||
| Mode of Onset | (acute) | 1 | ||
| gradual | 1.48 (1.05–2.08) | 1.45 (1.02–2.05) | 0.0384 | |
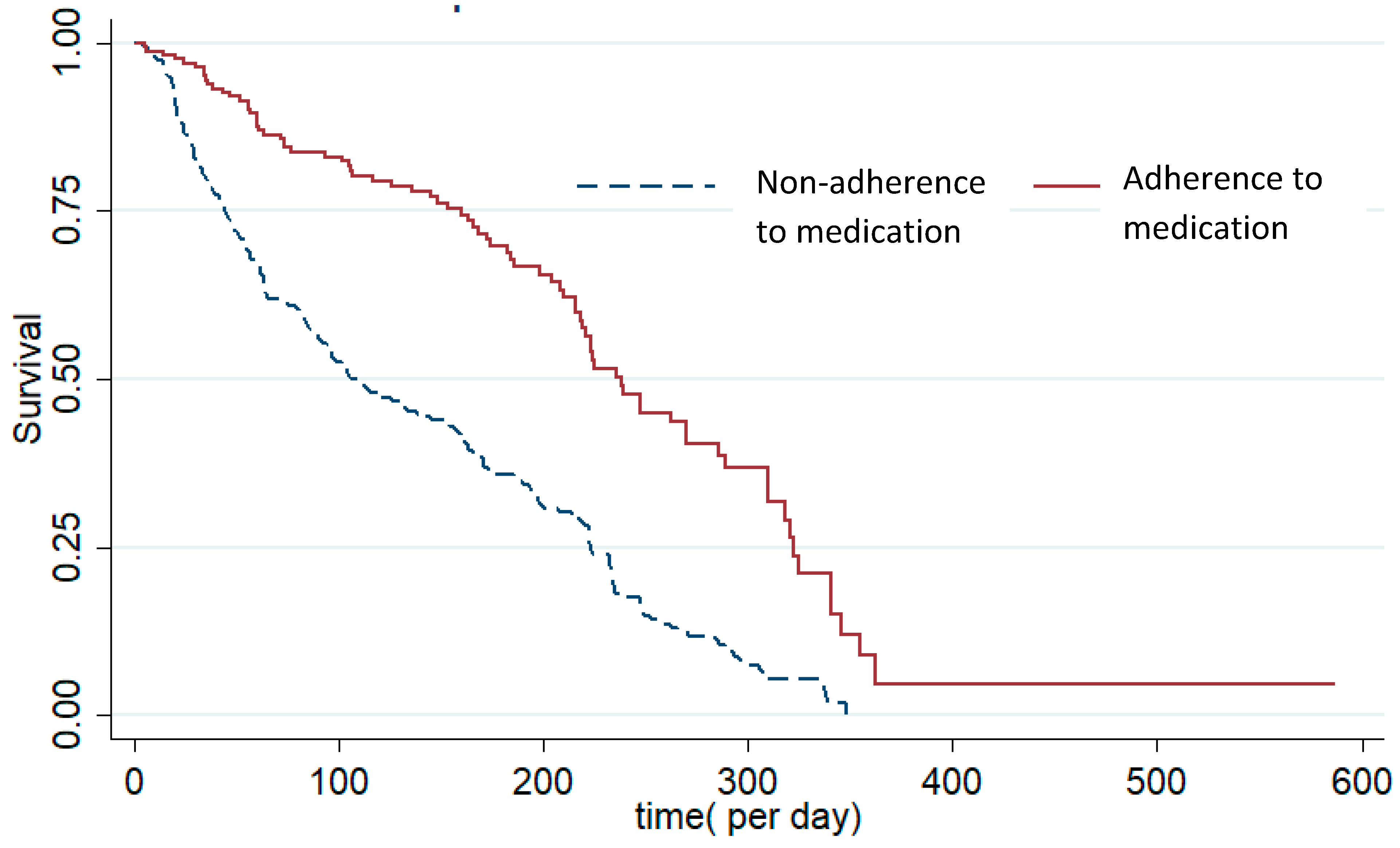
| Medication Adherence | (non-adherence) | 1 | ||
| adherence | 0.68 (0.56–0.83) | 0.71(0.58–0.86) | p < 0.001 | |
| Season of Birth | (spring) | |||
| summer | 1.03 (0.82–1.28) | |||
| autumn | 1.19 (0.94–1.51) | |||
| winter | 1.16 (0.92–1.46) | |||
| History of suicide attempt | (no) | 1 | ||
| Yes | 1.49 (1.05–2.11) | 1.32 (1.09–1.60) | 0.0314 | |
| Frailty parameter | Sigma Square = 0.08 SE = 0.01 p < 0.001 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davarinejad, O.; Mohammadi Majd, T.; Golmohammadi, F.; Mohammadi, P.; Radmehr, F.; Alikhani, M.; Motaei, T.; Moradinazar, M.; Brühl, A.; Sadeghi Bahmani, D.; et al. Identification of Risk Factors to Predict the Occurrences of Relapses in Individuals with Schizophrenia Spectrum Disorder in Iran. Int. J. Environ. Res. Public Health 2021, 18, 546. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020546
Davarinejad O, Mohammadi Majd T, Golmohammadi F, Mohammadi P, Radmehr F, Alikhani M, Motaei T, Moradinazar M, Brühl A, Sadeghi Bahmani D, et al. Identification of Risk Factors to Predict the Occurrences of Relapses in Individuals with Schizophrenia Spectrum Disorder in Iran. International Journal of Environmental Research and Public Health. 2021; 18(2):546. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020546
Chicago/Turabian StyleDavarinejad, Omran, Tahereh Mohammadi Majd, Farzaneh Golmohammadi, Payam Mohammadi, Farnaz Radmehr, Mostafa Alikhani, Tayebeh Motaei, Mehdi Moradinazar, Annette Brühl, Dena Sadeghi Bahmani, and et al. 2021. "Identification of Risk Factors to Predict the Occurrences of Relapses in Individuals with Schizophrenia Spectrum Disorder in Iran" International Journal of Environmental Research and Public Health 18, no. 2: 546. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020546