1. Introduction
Chronic pain is a widespread problem. Between 11% and 38% of children and adolescents worldwide have been reported to experience some form of chronic pain [
1], and about 5% experience serious disability problems related to this pain [
2]. In Spain, the prevalence of pediatric chronic pain is in line with these results. For example, Huguet and Miró [
2] found that 37% of schoolchildren reported some form of chronic pain.
The biopsychosocial model of pain argues that a complex set of biological, psychological, and sociocultural variables contribute to the experience and impact of pain [
3]. A psychological variable that is receiving a growing amount of empirical attention in the study of pediatric pain is perfectionism [
4,
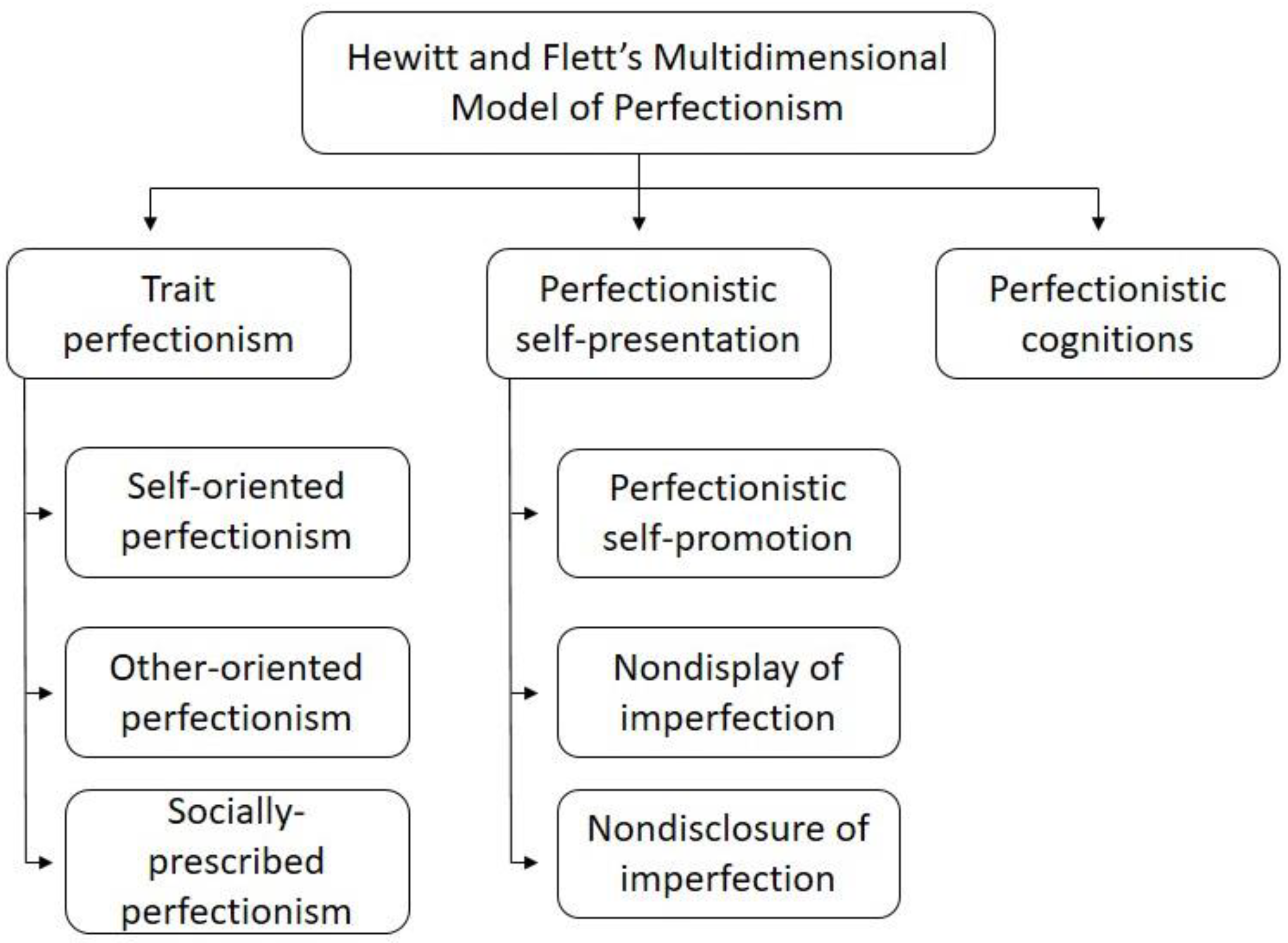
5]. Hewitt and Flett’s Multidimensional Model of Perfectionism [
6] identifies three domains of perfectionism. The first is trait perfectionism, defined as “…a personality disposition characterized by striving for flawlessness and setting exceedingly high standards of performance accompanied by overly critical evaluations of one’s behaviour” [
7] (p. 171). It consists of three subdomains: Self-oriented perfectionism, other-oriented perfectionism, and socially prescribed perfectionism. The second domain is perfectionistic self-presentation, defined as an “interpersonal expression of perfection or the drive to appear to others as perfect by either publicly promoting one’s ‘perfection’ or by concealing one’s imperfections” [
8] (p. 126). Perfectionistic self-presentation consists of the following three subdomains: Perfectionistic self-promotion, nondisplay of imperfection, and nondisclosure of imperfection. The third domain of Hewitt and Flett’s model consists of cognitive processes reflecting perfectionistic thoughts (e.g., ruminative thoughts regarding the need to be perfect).
Figure 1 shows a schema of the Hewitt and Flett’s Multidimensional Model of Perfectionism.
Perfectionism has been shown to be positively associated with psychological inflexibility, that is, the inability to adapt our responses to the demands of the situation [
9,
10]. In fact, psychological inflexibility is considered as a core element of perfectionism, and has been shown to be related to avoidance behavior and psychological distress [
11,
12]. The associations between measures of trait perfectionism and psychological inflexibility with measures of function have been studied in a number of clinical populations and community samples. For example, trait perfectionism has been shown to be consistently related with measures of psychological dysfunction such as anxiety and depressive symptoms (including suicidal behaviors) in studies with adults [
13,
14] and children [
15,
16,
17]. Perfectionistic self-presentation, although less studied in pediatric populations, has also shown to be significantly related to psychological distress. For example, Hewitt and colleagues [
8] found that measures of the three domains of perfectionistic self-presentation were significantly associated with measures of depressive symptoms in adolescents with anxiety and depression disorders. They also found that their measure of nondisplay of imperfections was associated significantly with measures of depression, anxiety, and worry beyond the effects of perfectionism traits, and that nondisclosure of imperfection predicted depression, social anxiety, and anger beyond the effects of perfectionistic traits. Along these lines, Flett and colleagues [
18] found that a measure of perfectionistic self-presentation in early adolescents (12 to 13 years old) from the community was significantly associated with social anxiety, even when controlling for measures of trait perfectionism.
Overall, then, both perfectionism as a trait and perfectionistic self-presentation have been consistently associated with a variety of psychological dysfunction domains (e.g., anxiety, depression, worry) [
19], all of which have also been shown to play a role in the experience of pain (e.g., [
20,
21]). However, the study of perfectionism in samples of individuals with pain is very limited. The research that has been conducted suggests that perfectionism might play an important role in the experience of pain in both adult [
14,
22] and pediatric populations [
4]. For example, Kempke and colleagues [
23] found that measures of perfectionistic traits were significantly associated with the frequency and intensity of pain and fatigue in a sample of adult patients with chronic fatigue syndrome. In a subsequent study [
22], these investigators found that self-critical perfectionism was significantly associated with poor treatment outcomes in a sample of adults with chronic pain.
Focusing in pediatric populations, Bonvanie and colleagues [
24] found, in a longitudinal study carried out with adolescents, that trait perfectionism was associated with functional somatic symptoms (i.e., pain, headache, stomachache, nausea, vomiting, dizziness, and fatigue without an identified organic cause). Furthermore, a recent study by Randall and colleagues [
5], carried out with children with chronic pain, showed that measures of trait perfectionism were significantly associated with physical disability through its relationship with the fear of pain and pain catastrophizing, and that parent’s perfectionism also played a role in their children’s pain experience.
Although these studies support the premise that perfectionism may play an important role in the adjustment to chronic pain, further studies are needed to determine the reliability and generalizability of these preliminary findings. Furthermore, to the best of our knowledge, no studies have yet explored the role that perfectionistic self-presentation could play in the experience of pain in children and adolescents.
Given these considerations, the primary aim of the current study was to better understand the relationships between perfectionistic self-presentation and measures of pain intensity, pain catastrophizing, pain interference, and fatigue in children and adolescents with pain. We hypothesized that the three domains of perfectionistic self-presentation (i.e., perfectionistic self-promotion, nondisplay of imperfection, and nondisclosure of imperfection) would evidence significant concurrent positive associations with measures of pain intensity, pain catastrophizing, pain interference, and fatigue. Furthermore, we sought to understand the potential moderating role of perfectionism in the associations between pain intensity and the other three pain-related criterion variables (i.e., pain catastrophizing, pain interference, and fatigue). We hypothesized that, if a significant moderating effect emerged, the association between pain intensity and the criterion variables would be stronger among children with higher levels of perfectionistic self-presentation than children with lower levels of perfectionistic self-presentation. Finally, we sought to determine if the mediating effects of pain catastrophizing on the association between perfectionism and pain interference found in previous studies [
5] would be replicated in the current nonclinical sample of schoolchildren with pain.
2. Materials and Methods
2.1. Participants
We invited children enrolled in grades 7 to 12 in 3 schools of the province of Tarragona (Catalonia, Spain) to participate in the study. We included schoolchildren who: (1) Were able to read and write Spanish; (2) were between 12 and 18 years old; (3) had experienced pain during the last 3 months, and (3) provided complete responses to all the questionnaires used in this study. Exclusion criteria were: (1) Failing to return the informed consent signed by their parents and (2) having any cognitive impairment that would interfere with the ability to understand and complete the questionnaires.
A total of 500 adolescents from 12 to 18 years old were invited to participate in this study. Of these, 333 (67%) assented to participate and returned the informed consent signed by their parents and participated in the study. Of the participants, 26 (8%) reported not having experienced pain in the last 3 months and 89 (27%) did not complete all the measures and were excluded from final analyses. Thus, the final sample of the participants was made up of 218 adolescents (44% of the initially invited) that experienced pain in the 3 months preceding the study. The average age was 14.39 years old (SD = 1.79; range = 12 to 18 years). There were no statistically significant differences in the average age associated to sex.
Table 1 provides additional descriptive information about the study sample.
2.2. Measures
Sociodemographic and pain information. Participants were asked to provide information about their age, sex, presence or absence of pain in the last 3 months, and pain location using a pain site checklist based on the site classification recommended by the International Association of Pain [
25]. In addition, for each pain location, they were asked to rate the average intensity of that pain in the last 7 days using a 0–10 Numerical Rating Scale (NRS-11) where 0 represents “No pain” and 10 represents “Very much pain.” For participants who had multiple pain locations, we selected the highest average pain intensity rating (among those provided for each site) for data analyses. The NRS-11 has been shown to provide valid and reliable data in children as young as 6 years old [
26,
27].
Perfectionistic self-presentation. We assessed perfectionistic self-presentation using a Spanish version of the Perfectionistic Self-Presentation Scale–Junior Form (PSPS–Jr; [
8]). With the PSPS–Jr, respondents are asked to rate the degree of agreement with each of the 18 statements included in the questionnaire using a 5-point Likert scale from 1 (“Strongly disagree”) to 5 (“Strongly agree”). The PSPS–Jr assesses 3 different domains of perfectionistic self-presentation: (1) Perfectionistic Self-Promotion (8 items, e.g., “I always have to look perfect”); (2) Nondisplay of Imperfection (P-ND; 6 items, e.g., “I feel bad about myself when I make mistakes in front of other people”), and (3) Nondisclosure of Imperfection (4 items, e.g., “I should always keep my problems secret”). The PSPS–Jr scales have shown to provide valid and reliable scores in several samples of children and adolescents [
8,
18]. Higher scores on each scale reflect a greater endorsement of each domain. In order to develop a translated version of the PSPS–Jr to use for this study, we conducted a back-translation process from English to Spanish following international guidelines [
28]. First, 2 bilingual authors (ESR and JM) translated the original version into Spanish and agreed on a single translation. Next, a professional translator (a native English speaker and a linguist) back-translated the Spanish version into English. Then, the back-translated instructions and items were reviewed by the authors of the translated version (ESR and JM) with the professional translator to determine if any additional changes in the Spanish version were needed. At this stage, no changes were deemed necessary. The internal consistency (Cronbach’s alphas) of the 3 scales of the PSPS–Jr in our sample was excellent for the Perfectionistic Self-Promotion scale (α = 0.90) and borderline for Nondisplay of Imperfection and Nondisclosure of Imperfection scales (αs = 0.67 and 0.60, respectively).
Pain catastrophizing. Participants were asked to indicate the frequency with which they thought or felt 13 different catastrophizing responses to pain using the Spanish version of the Pain Catastrophizing Scale (PCS-C; [
29,
30]). Responses to each item can vary from 0 (“Not at all”) to 4 (“Always”). The PCS-C can be scored as a total score of pain catastrophizing or as 3 subscales assessing rumination, magnification, and helplessness. Higher scores on the PCS-C reflect higher levels of pain catastrophizing. In this study, we used the total score of the PCS-C. Reports from the PCS-C have been shown to be valid and reliable when used with children and adolescents [
29,
30]. The internal consistency (Cronbach’s alpha) of the PCS-C total scale score was good (
α = 0.89) in our sample.
Pain interference. Pain interference was assessed using the 8-item pediatric PROMIS Pain Interference scale v.2.0 (PROMIS-PI; [
31]). With this measure, respondents are asked to indicate the frequency with which pain has interfered with 8 different daily activities during the last 7 days using a 5-point Likert scale ranging from 1 (“Never”) to 5 (“Almost always”). Higher scores reflect higher pain interference. The pediatric version of the PROMIS-PI has been shown to provide a valid and reliable measure of pain interference in children and adolescents [
32]. The internal consistency (Cronbach’s alpha) of the pediatric PROMIS-PI was good (α = 0.89) in our sample.
Fatigue. We used the Spanish version of the 4-item fatigue short form from the PROMIS Pediatric-25 Profile Form v.2. With these items, respondents are asked to rate how often they experience each fatigue response using a 5-point Likert scale from 1 (“Never”) to 5 (“Almost always”). Higher scores in the fatigue scale reflect greater fatigue. Previous work has shown that these PROMIS items are able to provide valid and reliable data for assessing fatigue in children and adolescents [
33]. The internal consistency (Cronbach’s alpha) of the measure was good (α = 0.85) in our sample.
2.3. Procedure
We first contacted 4 secondary schools in the province of Tarragona (Catalonia, Spain) to inform them about the study, and 3 of them were willing to consider participation. We then met the principals of these 3 schools to describe the study procedures and goals and they consented for data collection. Next, we sent a letter to the parents of the children enrolled in grades 7 to 12 in these schools, explaining the study objectives and procedures and requesting permission for their children to participate in the study. Parents were requested to indicate their approval by signing an informed consent form and returning it to the researchers. Research staff then went to the participating schools and administered the questionnaires (self-reports) to the participants who had assented and whose parents provided consent. In order to foster truthfully responses, participants were told that there were no correct or incorrect answers and that all the answers would be anonymized. The study procedures were approved by the Ethics Committee of the Institut d’Investigació Sanitària Pere i Virgili.
2.4. Data Analysis
We first computed descriptive statistics (means and standard deviations for continuous variables and number and percentages for dichotomous variables) for the demographic and study variables and computed zero-order correlation coefficients among the study variables for descriptive purposes. Next, we examined the distributions (skewness and kurtosis) and the multicollinearity (by computing variance inflation factors and tolerance) of the predictor and criteria variables to ensure that they met the assumptions for the planned analyses (i.e., normal distribution and no multicollinearity). Then, in order to test the first and second hypotheses (i.e., that the 3 domains of perfectionistic self-presentation would evidence significant concurrent positive association with measures of pain intensity, pain catastrophizing, pain interference, and fatigue and that perfectionistic self-presentation could act as moderator in the associations between pain intensity and the other three pain-related criterion variables), we computed 4 hierarchical regression analyses, with the measures of pain intensity, pain interference, pain catastrophizing, and fatigue as the criterion variables. We entered demographic variables (sex and age) in step 1 as control variables. In step 2, we entered pain intensity (only when the criterion variable was pain catastrophizing, pain interference, or fatigue). In step 3, we entered the 3 domains of perfectionistic self-presentation (i.e., perfectionistic self-promotion, nondisplay of imperfection, and nondisclosure of imperfection). Finally, in step 4, we entered the 3 interaction terms (Pain Intensity x Perfectionistic Self-Promotion, Pain Intensity x Nondisplay of Imperfection, and Pain Intensity x Nondisclosure of Imperfection) when the criterion variables were pain catastrophizing, pain interference, or fatigue. If an interaction term emerged as significant, we planned to evaluate the moderating effects using the visualization strategy recommended by Hayes and Rockwood using PROCESS macro for SPSS [
34].
Finally, in order to evaluate the potential mediating role of pain catastrophizing in the association between the 3 domains of perfectionistic self-presentation and pain interference, we performed 3 mediation analyses using PROCESS macro, with the 3 domains of perfectionistic self-presentation as predictors; pain interference as the criterion; pain catastrophizing as potential mediators; and sex, age, and pain intensity as covariates.
All data analyses were performed using the Statistical Package for Social Sciences (Windows version 25.0, SPSS Inc., Chicago, IL, USA). The sample size needed in the regression analyses was calculated using G*Power software v.3.1.9.4. (HHU, Heinrich Heine Universität Düsseldorf, Düsseldorf, North Rhine-Westphalia, Germany) Assuming 9 predictors and an alpha of 0.05, we needed a minimum of 166 participants to detect a medium effect (f2 = 0.15).
4. Discussion
The primary objective of this study was to better understand the role that perfectionistic self-presentation plays in explaining the pain experience of children and adolescents with pain recruited from the community. We hypothesized that the three domains of perfectionistic self-presentation would evidence significant concurrent positive associations with measures of pain intensity, pain catastrophizing, pain interference, and fatigue in this sample. We also hypothesized that, if a significant moderating effect of perfectionism was found, then the association between pain intensity and the criterion variables would be stronger among children with higher levels of perfectionistic self-presentation than children with lower levels of perfectionistic self-presentation. Finally, we sought to determine if the mediating effect of pain catastrophizing on the association between perfectionistic self-presentation and pain interference found in prior research would be replicated.
The study hypothesis regarding the prediction of pain-related criterion variables from measures of perfectionism was partially supported. Some, but not all, of the domains of perfectionism showed significant associations with some criterion measures (see
Figure 5).
This result is consistent with previous research indicating that different domains of perfectionistic self-presentation might be distinctly associated with different outcomes [
8,
18]. Specifically, the findings suggest that nondisplay of imperfection could play a larger role in the adolescents’ experience of pain than either perfectionistic self-promotion or nondisclosure of imperfection. If this finding is replicated in future studies, including longitudinal studies supporting a causal influence of nondisplay of imperfection on pain, this would support the potential importance of targeting this component of perfectionism in pain management programs. Such programs might include Acceptance and Commitment Therapy to help develop or reinforce psychological flexibility (i.e., acceptance, cognitive defusion, contact with the present moment, self-as-context, committed action, values orientation) [
35], or cognitive-behavioral therapy [
36], with the objective of encouraging adolescents to participate in activities with which they might not evidence perfection while, at the same time, practicing self-acceptance. Research to evaluate the potential benefits of such programs, as well as the potential mediation role of reductions in nondisplay of imperfection in those benefits, is warranted.
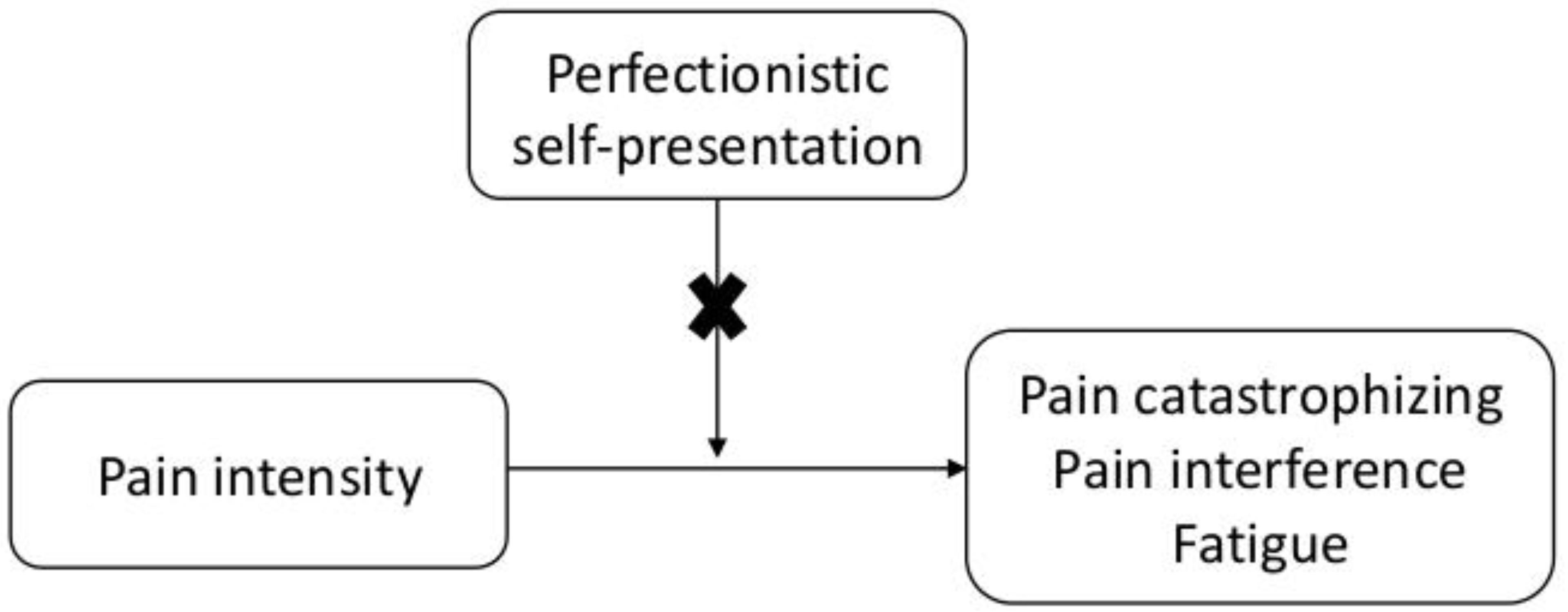
The findings did not support a moderating role for perfectionistic self-presentation in the association between pain intensity and pain catastrophizing, pain interference, and fatigue. Thus, higher levels in perfectionistic self-presentation domains do not appear to make adolescents more vulnerable to the negative effects of pain intensity on function (see
Figure 6).
This is, to the best of our knowledge, the first study that tested the potential moderating role of perfectionistic self-presentation in the associations between pain intensity and the three pain-related criterion variables studied here (i.e., pain catastrophizing, pain interference, and fatigue). If these findings are replicated in other samples, they would suggest that teaching adolescents skills to reduce perfectionistic self-presentation, while possibly having some positive effects on some outcomes (e.g., increasing self-esteem, decreasing fear and intolerance of uncertainty; [
37]), would not necessarily buffer the negative effects of pain on function.
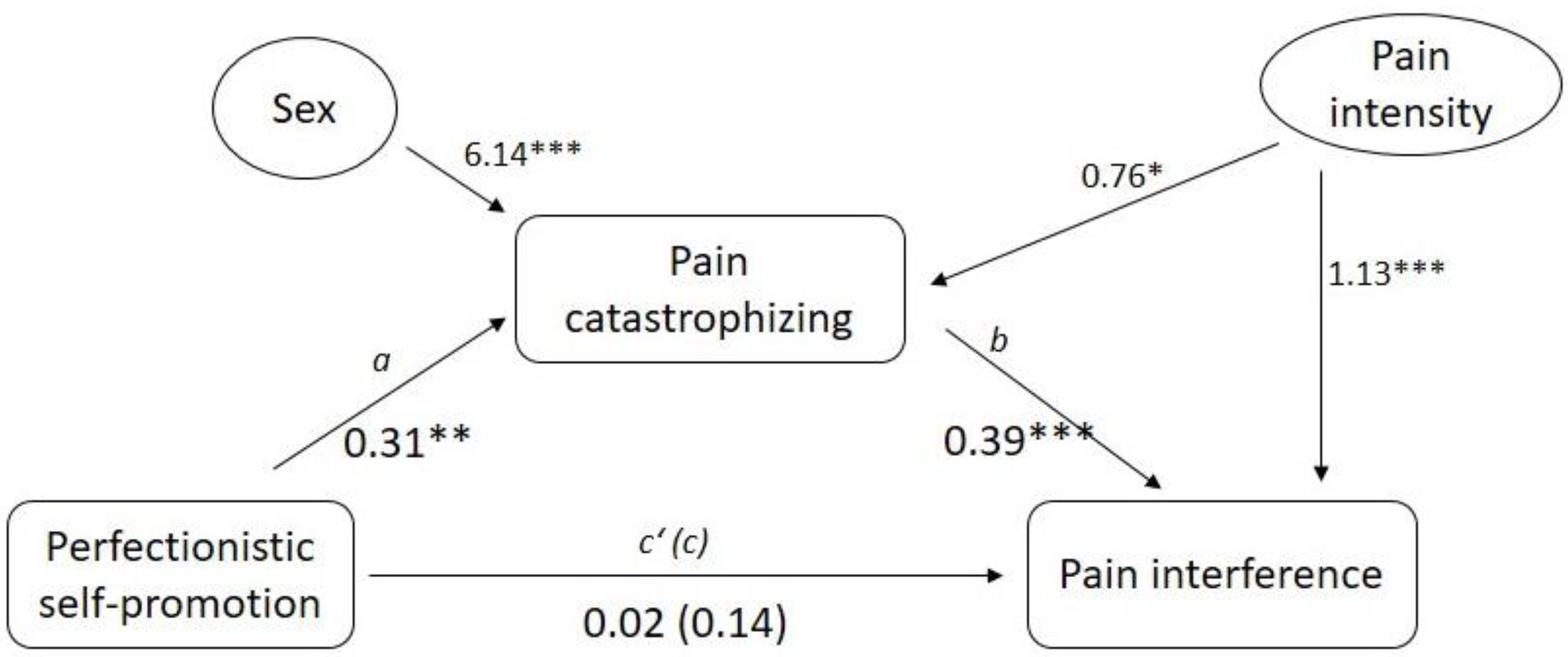
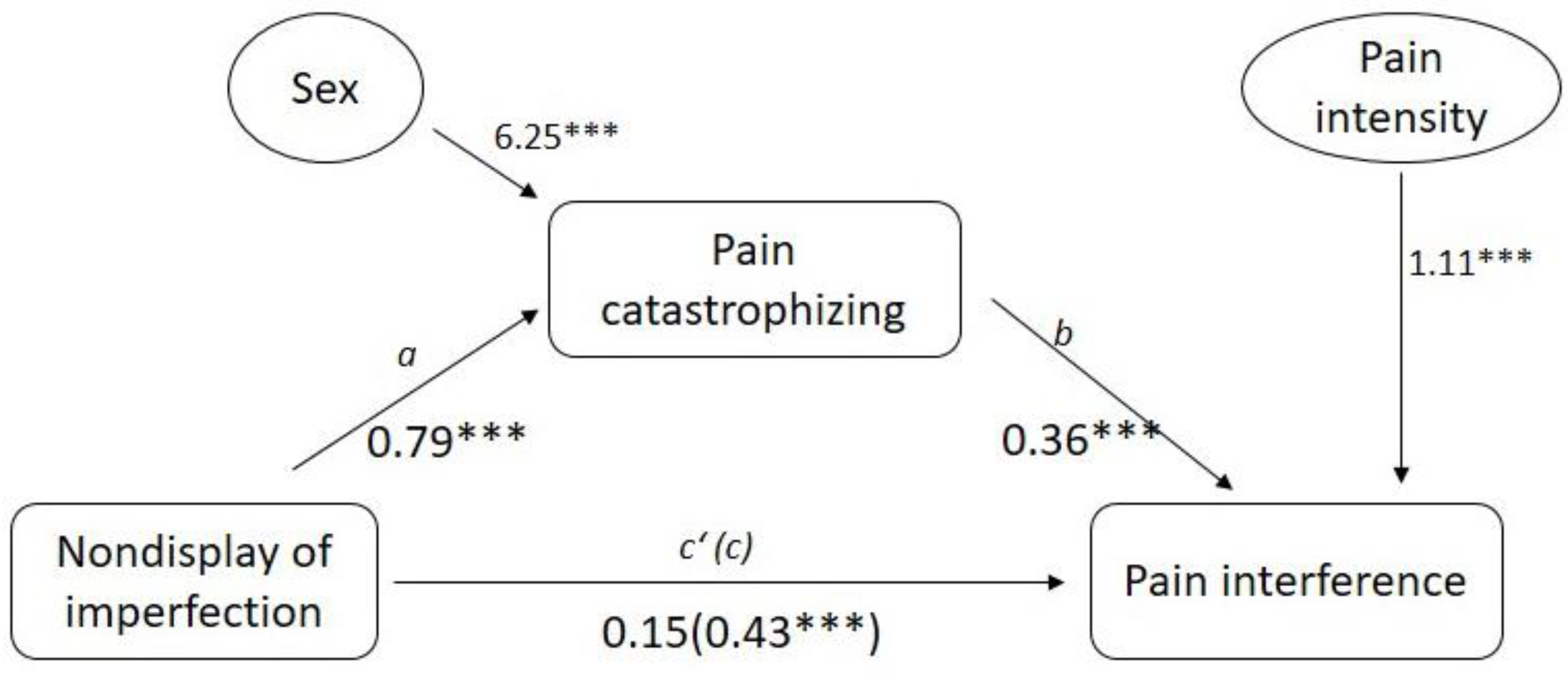
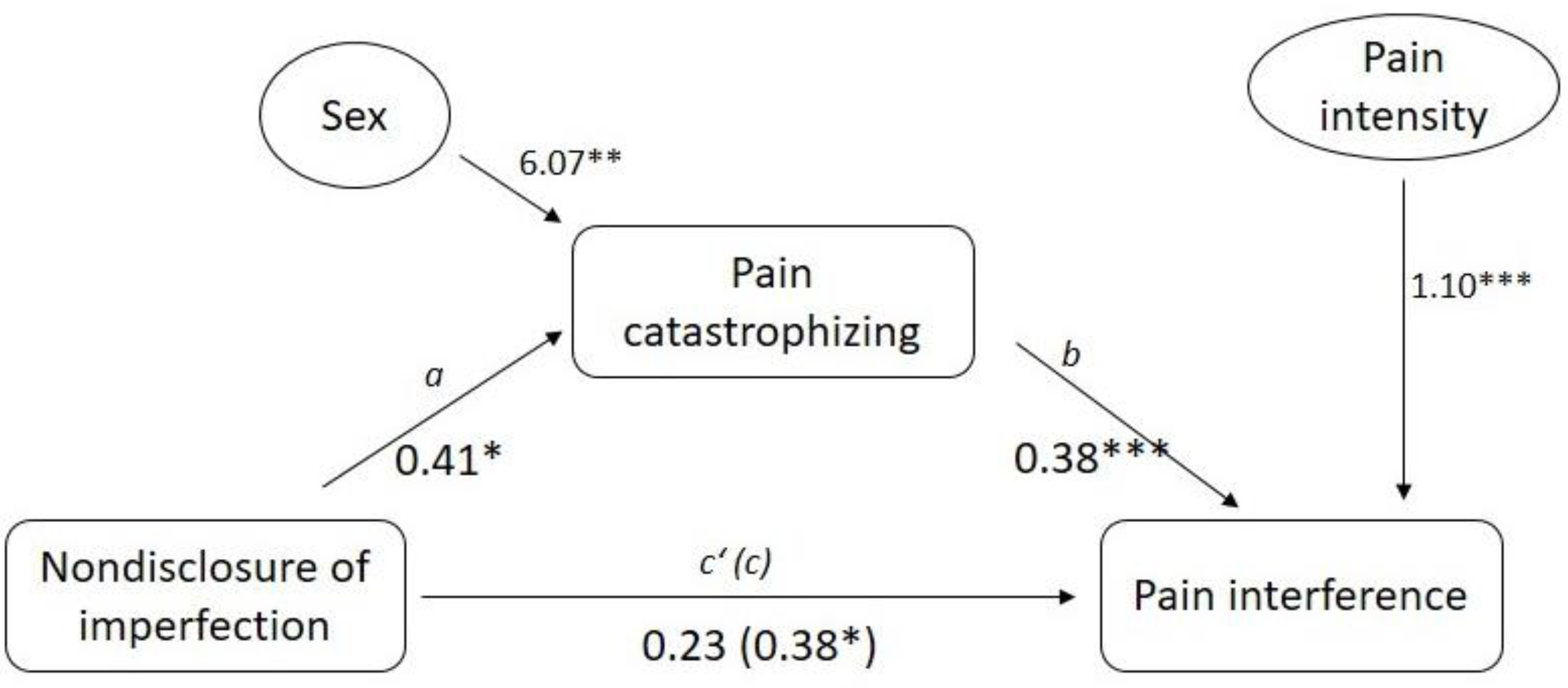
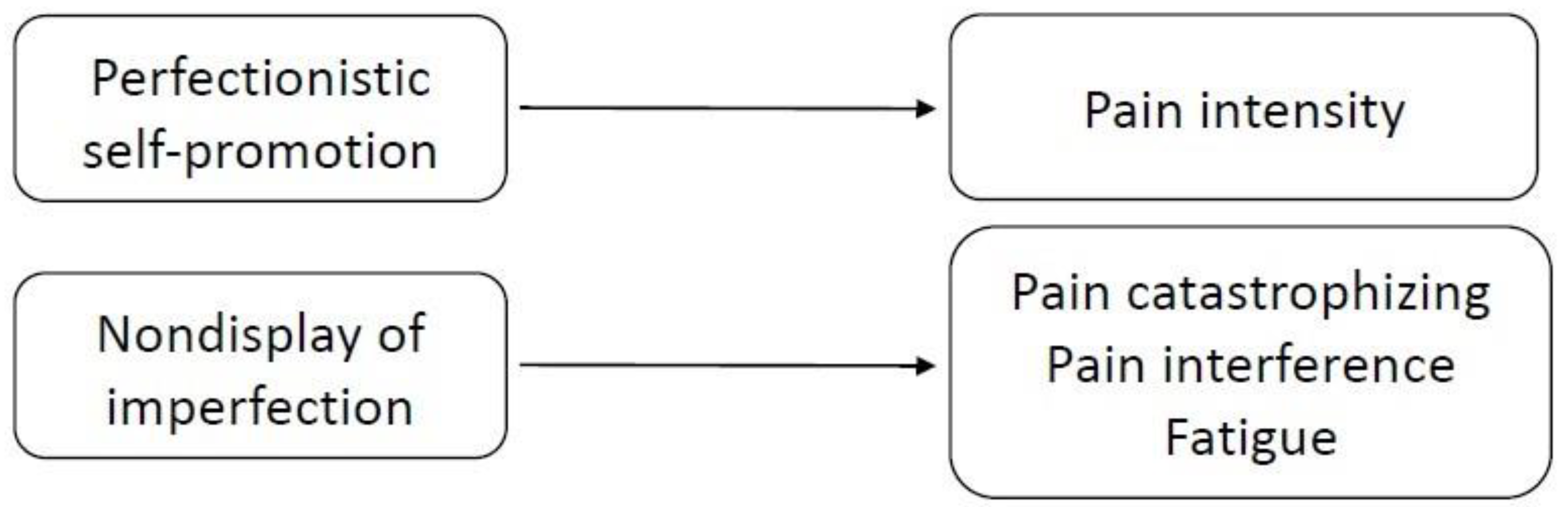
The study findings support the mediating effects of pain catastrophizing on the association between perfectionistic self-presentation and pain interference (see
Figure 1 and
Figure 2), although pain catastrophizing did not mediate the association between nondisclosure of imperfection and pain interference (see
Figure 3). Previous work with pediatric pain populations [
5] found that trait perfectionism (i.e., self-oriented, socially prescribed, and effortless perfectionism) impacts functional disability through its influence on pain catastrophizing. Our findings, in light of those reported by Randall and colleagues, suggest that trying to appear to others as perfect may contribute to increases in rumination and worry about pain, which could then lead to greater pain interference. If this finding is supported by future longitudinal research in this area, treatments which reduce perfectionism could potentially also decrease catastrophizing in adolescents, which could ultimately increase their function.
The study findings also suggest that not only a perceived need to be perfect (trait perfectionism) but also that a perceived need to appear perfect to the others (perfectionistic self-presentation) have an important role in how young people experience and cope with pain. As this is the first study to evaluate the role of perfectionistic self-presentation in a sample of schoolchildren with pain, additional research, especially longitudinal studies, is needed to determine which of the findings reported here could be replicated in future studies.
This study has a number of limitations that should be considered when interpreting the results. First, our sample was a convenience community sample of schoolchildren with pain who may or may not be representative of the population of young people with pain. Future research should study perfectionism on additional samples of children and adolescents with pain to determine the generalizability of the findings. Second, because this was a cross-sectional study, we were not able to draw causal conclusions regarding the influence of perfectionistic self-presentation on pain and its impact. Longitudinal studies are also needed to understand causal associations between perfectionistic self-presentation and pain experience in pediatric samples. Third, all the data were collected via self-report. As a result, some of the significant associations found could have been due to shared method bias [
38]. Future researchers should evaluate some of the domains using alternative strategies when possible (e.g., measuring function via an actigraph or using observational measures, or via parent-proxy reports) to ascertain whether the findings in this study are due to shared method bias. Fourth, the Spanish version of the PSPS–Jr used in this study had borderline levels of internal consistency for the Nondisplay of Imperfection and the Nondisclosure of Imperfection scale (αs = 0.67 and 0.60, respectively). Whereas these levels of reliability are consistent with those obtained with the original version of the questionnaire [
8,
18], it is possible that the limited reliability of these measures resulted in an underestimation of the true associations among the study variables. Given the potential relevance that trait perfectionism and perfectionistic self-presentation may have in the adjustment to pain among children and adolescents, it would be reasonable to consider revising the available measures (e.g., by adding new items) or developing more reliable measures of these domains in order to increase the reliability of the research findings.

 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}