Neurodevelopmental Outcomes at 18 Months of Corrected Age for Late Preterm Infants Born at 34 and 35 Gestational Weeks

 , , , and
, , , and
Abstract
:1. Introduction
2. Patients and Methods
3. Results
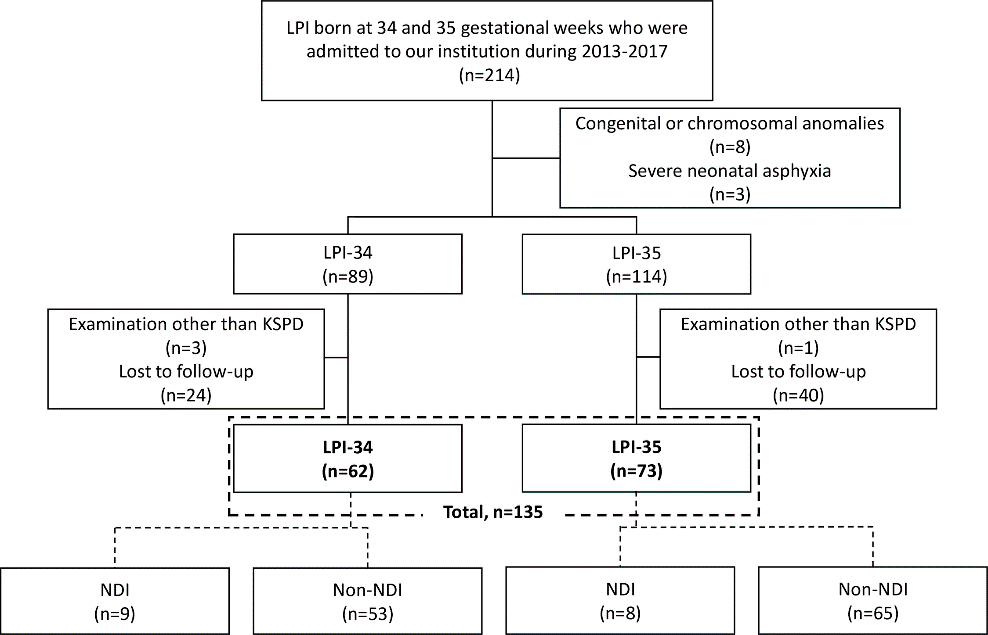
3.1. Patient Characteristics
3.2. Clinical Characteristics in LPI-34 and LPI-35 Infants
3.3. Clinical Characteristics in NDI and Non-NDI Infants
3.4. Sensitivity, Specificity, and Youden Index for Predicting NDI at 18 Months of Corrected Age
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gyamfi-Bannerman, C. The scope of the problem: The epidemiology of late preterm and early-term birth. Semin. Perinatol. 2011, 35, 246–248. [Google Scholar] [CrossRef]
- Davidoff, M.J.; Dias, T.; Damus, K.; Russell, R.; Bettegowda, V.R.; Dolan, S.; Schwarz, R.H.; Green, N.S.; Petrini, J. Changes in the gestational age distribution among U.S. singleton births: Impact on rates of late preterm birth, 1992 to 2002. Semin. Perinatol. 2006, 30, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Engle, W.A.; Tomashek, K.M.; Wallman, C.; Committee on, F.; Newborn, A.A.O.P. “Late-preterm” infants: A population at risk. Pediatrics 2007, 120, 1390–1401. [Google Scholar] [CrossRef] [Green Version]
- Nagasaka, M.; Morioka, I.; Yokota, T.; Fujita, K.; Kurokawa, D.; Koda, T.; Shibata, A.; Yamada, H.; Ito, Y.; Uchino, E.; et al. Incidence of short stature at 3 years of age in late preterm infants: A population-based study. Arch. Dis. Child. 2015, 100, 250–254. [Google Scholar] [CrossRef]
- Kugelman, A.; Colin, A.A. Late preterm infants: Near term but still in a critical developmental time period. Pediatrics 2013, 132, 741–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrini, J.R.; Dias, T.; McCormick, M.C.; Massolo, M.L.; Green, N.S.; Escobar, G.J. Increased risk of adverse neurological development for late preterm infants. J. Pediatr. 2009, 154, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Morse, S.B.; Zheng, H.; Tang, Y.; Roth, J. Early school-age outcomes of late preterm infants. Pediatrics 2009, 123, e622–e629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moster, D.; Lie, R.T.; Markestad, T. Long-term medical and social consequences of preterm birth. N. Engl. J. Med. 2008, 359, 262–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumert, M.; Surmiak, P.; Walencka, Z.; Mrowiec, E.; Sodowska, P. Can neonates born at 34 weeks be classified as late preterm? Ginekol. Pol. 2016, 87, 805–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srinivasjois, R.; Nembhard, W.; Wong, K.; Bourke, J.; Pereira, G.; Leonard, H. Risk of Mortality into Adulthood According to Gestational Age at Birth. J. Pediatr. 2017, 190, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Ancel, P.Y.; Goffinet, F.; Group, E.-W.; Kuhn, P.; Langer, B.; Matis, J.; Hernandorena, X.; Chabanier, P.; Joly-Pedespan, L.; Lecomte, B.; et al. Survival and morbidity of preterm children born at 22 through 34 weeks’ gestation in France in 2011: Results of the EPIPAGE-2 cohort study. JAMA Pediatr. 2015, 169, 230–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotecha, S.J.; Watkins, W.J.; Paranjothy, S.; Dunstan, F.D.; Henderson, A.J.; Kotecha, S. Effect of late preterm birth on longitudinal lung spirometry in school age children and adolescents. Thorax 2012, 67, 54–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddy, U.M.; Ko, C.W.; Raju, T.N.; Willinger, M. Delivery indications at late-preterm gestations and infant mortality rates in the United States. Pediatrics 2009, 124, 234–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kono, Y.; Yonemoto, N.; Kusuda, S.; Hirano, S.; Iwata, O.; Tanaka, K.; Nakazawa, J. Developmental assessment of VLBW infants at 18 months of age: A comparison study between KSPD and Bayley III. Brain Dev. 2016, 38, 377–385. [Google Scholar] [CrossRef]
- Fukushima, S.; Morioka, I.; Ohyama, S.; Nishida, K.; Iwatani, S.; Fujioka, K.; Mandai, T.; Matsumoto, H.; Nakamachi, Y.; Deguchi, M.; et al. Prediction of poor neurological development in patients with symptomatic congenital cytomegalovirus diseases after oral valganciclovir treatment. Brain Dev. 2019, 41, 743–750. [Google Scholar] [CrossRef]
- Uchida, A.; Tanimura, K.; Morizane, M.; Fujioka, K.; Morioka, I.; Oohashi, M.; Minematsu, T.; Yamada, H. Clinical factors associated with congenital cytomegalovirus infection: A cohort study of pregnant women and newborns. Clin. Infect. Dis. 2019, 71, 2833–2839. [Google Scholar] [CrossRef]
- Fujioka, K.; Shibata, A.; Yokota, T.; Koda, T.; Nagasaka, M.; Yagi, M.; Takeshima, Y.; Yamada, H.; Iijima, K.; Morioka, I. Association of a vascular endothelial growth factor polymorphism with the development of bronchopulmonary dysplasia in Japanese premature newborns. Sci. Rep. 2014, 4, 4459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huhn, E.A.; Fischer, T.; Gobl, C.S.; Todesco Bernasconi, M.; Kreft, M.; Kunze, M.; Schoetzau, A.; Dolzlmuller, E.; Eppel, W.; Husslein, P.; et al. Screening of gestational diabetes mellitus in early pregnancy by oral glucose tolerance test and glycosylated fibronectin: Study protocol for an international, prospective, multicentre cohort trial. BMJ Open 2016, 6, e012115. [Google Scholar] [CrossRef] [Green Version]
- Morioka, I. Hyperbilirubinemia in preterm infants in Japan: New treatment criteria. Pediatr. Int. 2018, 60, 684–690. [Google Scholar] [CrossRef] [PubMed]
- Rovira, N.; Alarcon, A.; Iriondo, M.; Ibanez, M.; Poo, P.; Cusi, V.; Agut, T.; Pertierra, A.; Krauel, X. Impact of histological chorioamnionitis, funisitis and clinical chorioamnionitis on neurodevelopmental outcome of preterm infants. Early Hum. Dev. 2011, 87, 253–257. [Google Scholar] [CrossRef]
- Kato, T.; Mandai, T.; Iwatani, S.; Koda, T.; Nagasaka, M.; Fujita, K.; Kurokawa, D.; Yamana, K.; Nishida, K.; Taniguchi-Ikeda, M.; et al. Extremely preterm infants small for gestational age are at risk for motor impairment at 3 years corrected age. Brain Dev. 2016, 38, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Fluss, R.; Faraggi, D.; Reiser, B. Estimation of the Youden Index and its associated cutoff point. Biom. J. 2005, 47, 458–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastek, J.A.; Sammel, M.D.; Pare, E.; Srinivas, S.K.; Posencheg, M.A.; Elovitz, M.A. Adverse neonatal outcomes: Examining the risks between preterm, late preterm, and term infants. Am. J. Obstet. Gynecol. 2008, 199, 367.e1–367.e8. [Google Scholar] [CrossRef] [PubMed]
- Lipkind, H.S.; Slopen, M.E.; Pfeiffer, M.R.; McVeigh, K.H. School-age outcomes of late preterm infants in New York City. Am. J. Obstet. Gynecol. 2012, 206, 222.e1–222.e6. [Google Scholar] [CrossRef] [PubMed]
- Huddy, C.L.; Johnson, A.; Hope, P.L. Educational and behavioural problems in babies of 32–35 weeks gestation. Arch. Dis. Child. Fetal Neonatal Ed. 2001, 85, F23–F28. [Google Scholar] [CrossRef] [Green Version]
- Teune, M.J.; Bakhuizen, S.; Gyamfi Bannerman, C.; Opmeer, B.C.; van Kaam, A.H.; van Wassenaer, A.G.; Morris, J.M.; Mol, B.W. A systematic review of severe morbidity in infants born late preterm. Am. J. Obstet. Gynecol. 2011, 205, 374.e1–374.e9. [Google Scholar] [CrossRef]
- Melamed, N.; Klinger, G.; Tenenbaum-Gavish, K.; Herscovici, T.; Linder, N.; Hod, M.; Yogev, Y. Short-term neonatal outcome in low-risk, spontaneous, singleton, late preterm deliveries. Obstet. Gynecol. 2009, 114 (2 Pt 1), 253–260. [Google Scholar] [CrossRef]
- Bolisetty, S.; Dhawan, A.; Abdel-Latif, M.; Bajuk, B.; Stack, J.; Oei, J.L.; Lui, K. Intraventricular hemorrhage and neurodevelopmental outcomes in extreme preterm infants. Pediatrics 2014, 133, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Maimburg, R.D.; Bech, B.H.; Vaeth, M.; Moller-Madsen, B.; Olsen, J. Neonatal jaundice, autism, and other disorders of psychological development. Pediatrics 2010, 126, 872–878. [Google Scholar] [CrossRef]
- Jangaard, K.A.; Fell, D.B.; Dodds, L.; Allen, A.C. Outcomes in a population of healthy term and near-term infants with serum bilirubin levels of > or = 325 micromol/L (> or = 19 mg/dL) who were born in Nova Scotia, Canada, between 1994 and 2000. Pediatrics 2008, 122, 119–124. [Google Scholar] [CrossRef]
- Wusthoff, C.J.; Loe, I.M. Impact of bilirubin-induced neurologic dysfunction on neurodevelopmental outcomes. Semin. Fetal Neonatal Med. 2015, 20, 52–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.W.; Colford, J.M., Jr. Chorioamnionitis as a risk factor for cerebral palsy: A meta-analysis. JAMA 2000, 284, 1417–1424. [Google Scholar] [CrossRef] [PubMed]
- Salas, A.A.; Faye-Petersen, O.M.; Sims, B.; Peralta-Carcelen, M.; Reilly, S.D.; McGwin, G., Jr.; Carlo, W.A.; Ambalavanan, N. Histological characteristics of the fetal inflammatory response associated with neurodevelopmental impairment and death in extremely preterm infants. J. Pediatr. 2013, 163, 652–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soraisham, A.S.; Trevenen, C.; Wood, S.; Singhal, N.; Sauve, R. Histological chorioamnionitis and neurodevelopmental outcome in preterm infants. J. Perinatol. 2013, 33, 70–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ylijoki, M.; Lehtonen, L.; Lind, A.; Ekholm, E.; Lapinleimu, H.; Kujari, H.; Haataja, L.; Group, P.S. Chorioamnionitis and Five-Year Neurodevelopmental Outcome in Preterm Infants. Neonatology 2016, 110, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Torrance, H.L.; Bloemen, M.C.; Mulder, E.J.; Nikkels, P.G.; Derks, J.B.; de Vries, L.S.; Visser, G.H. Predictors of outcome at 2 years of age after early intrauterine growth restriction. Ultrasound Obstet. Gynecol. 2010, 36, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Chevallier, M.; Debillon, T.; Pierrat, V.; Delorme, P.; Kayem, G.; Durox, M.; Goffinet, F.; Marret, S.; Ancel, P.Y.; Arnaud, C.; et al. Leading causes of preterm delivery as risk factors for intraventricular hemorrhage in very preterm infants: Results of the EPIPAGE 2 cohort study. Am. J. Obstet. Gynecol. 2017, 216, 518.e1–518.e12. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| LPI-34 n = 62 | LPI-35 n = 73 | p Value | |
|---|---|---|---|
| Maternal Data | |||
| Maternal age, years | 34 (18–42) | 35 (18–41) * | 0.22 |
| Threatened preterm labor | 36 (58) | 44 (60) | 0.79 |
| Premature rupture of membrane | 16 (26) | 25 (35) | 0.29 |
| Hypertensive disorder of pregnancy | 13 (21) | 10 (14) | 0.26 |
| Gestational diabetes | 9 (15) | 15 (21) | 0.36 |
| Smoking | 0 (0) | 2 (3) | 0.19 |
| Multiple pregnancies | 24 (39) | 16 (22) | 0.03 |
| Cesarean section | 53 (85) | 45 (62) | <0.005 |
| Outborn | 3 (5) | 7 (10) | 0.29 |
| Neonatal Data | |||
| Male | 39 (63) | 42 (58) | 0.53 |
| BW, g | 2061 (1354–2798) | 2328 (1700–3562) | 0.0001 |
| Apgar score at 1 min | 8 (3–10) | 8 (2–9) | 0.46 |
| Apgar score at 5 min | 9 (6–10) | 9 (4–10) | 0.44 |
| Small for gestational age infants | 14 (23) | 10 (14) | 0.18 |
| Artificial mechanical ventilation | 44 (71) | 33 (45) | <0.005 |
| Respiratory distress syndrome | 17 (27) | 6 (8) | <0.005 |
| Hyperbilirubinemia | 47 (78) # | 40 (55) | <0.005 |
| Severe hyperbilirubinemia | 4 (7) # | 8 (11) | 0.39 |
| Hypoglycemia | 40 (67) # | 34 (47) | 0.02 |
| Intraventricular hemorrhage | 2 (3) | 1 (1) | 0.47 |
| Periventricular leukomalacia | 1 (2) | 0 (0) | 0.28 |
| Length of hospital stay, days | 29.5 (17–91) | 19 (9–60) | <0.001 |
| Placental Characteristics | |||
| Chorioamnionitis ¥ | 10 (27) | 9 (20) | 0.93 |
| Funisitis ¥ | 3 (8) | 2 (4) | 0.49 |
| Infarction ¥ | 6 (16) | 12 (27) | 0.26 |
| Calcification ¥ | 13 (35) | 19 (42) | 0.51 |
| Psychomotor Development Data | |||
| All areas $ | 92 ± 9 | 92 ± 11 | 0.74 |
| Postural-motor $ | 89 ± 13 | 90 ± 13 | 0.71 |
| Cognitive-adaptive $ | 93 ± 12 | 93 ± 13 | >0.99 |
| Language-social $ | 90 ± 11 | 88 ± 12 | 0.37 |
| Neurodevelopmental impairment (DQ <80) | 9 (15) | 8 (11) | 0.53 |
| Characteristic | NDI n = 17 | Non-NDI n = 118 | p Value |
|---|---|---|---|
| Maternal Data | |||
| Maternal age, years | 35 (29–42) | 35 (18–42) * | 0.41 |
| Threatened preterm labor | 10 (59) | 70 (59) | 0.97 |
| Premature rupture of membrane | 3 (18) | 38 (32) | 0.22 |
| Hypertensive disorder of pregnancy | 3 (18) | 21 (18) | 0.99 |
| Gestational diabetes | 4 (24) | 20 (17) | 0.51 |
| Smoking | 0 (0) | 2 (2) | 0.59 |
| Multiple pregnancies | 2 (12) | 38 (32) | 0.08 |
| Cesarean section | 12 (71) | 86 (73) | 0.84 |
| Outborn | 1 (6) | 9 (8) | 0.80 |
| Neonatal Data | |||
| LPI-34 | 9 (53) | 53 (45) | 0.53 |
| Male | 14 (82) | 67 (57) | 0.04 |
| Gestational age, weeks | 34 (34–35) | 35 (34–35) | 0.61 |
| BW, g | 2224 (1512–3562) | 2155 (1354–3540) | 0.73 |
| Apgar score at 1 min | 8 (3–10) | 8 (2–9) | 0.21 |
| Apgar score at 5 min | 9 (6–10) | 9 (4–10) | 0.97 |
| Small for gestational age infants | 3 (18) | 21 (18) | 0.99 |
| Artificial mechanical ventilation | 12 (71) | 65 (55) | 0.23 |
| Respiratory distress syndrome | 3 (18) | 20 (17) | 0.94 |
| Hyperbilirubinemia | 15 (88) | 72 (62) # | 0.03 |
| Severe hyperbilirubinemia | 4 (24) | 8 (7) # | 0.03 |
| Hypoglycemia | 10 (59) | 64 (55) # | 0.78 |
| Intraventricular hemorrhage | 3 (18) | 0 (0) | <0.001 |
| Periventricular leukomalacia | 0 (0) | 1 (1) | 0.70 |
| Length of hospital stay, days | 25 (10–91) | 21.5 (9–65) | 0.15 |
| Placental Characteristics | |||
| Chorioamnionitis ¥ | 2 (17) | 17 (24) | 0.56 |
| Funisitis ¥ | 1 (8) | 4 (6) | 0.73 |
| Infarction ¥ | 3 (25) | 15 (21) | 0.78 |
| Calcification ¥ | 4 (33) | 28 (40) | 0.66 |
| Psychomotor Development Data | |||
| All areas | 72 ± 5 | 94 ± 8 | <0.001 |
| Postural-motor | 76 ± 14 | 90 ± 12 | <0.001 |
| Cognitive-adaptive | 71 ± 4 | 95 ± 11 | <0.001 |
| Language-social | 75 ± 10 | 90 ± 11 | <0.001 |
| Sensitivity | Specificity | Youden Index | p Value | |
|---|---|---|---|---|
| Male | 0.824 | 0.432 | 0.256 | 0.04 |
| Hyperbilirubinemia | 0.882 | 0.379 | 0.261 | 0.03 |
| Severe hyperbilirubinemia | 0.235 | 0.931 | 0.166 | 0.03 |
| IVH | 0.177 | 1.000 | 0.177 | <0.001 |
| Male and/or IVH | 0.824 | 0.432 | 0.256 | 0.04 |
| Male and/or hyperbilirubinemia | 0.941 | 0.155 | 0.096 | 0.29 |
| Male and/or severe hyperbilirubinemia | 0.882 | 0.397 | 0.279 | 0.03 |
| Hyperbilirubinemia and/or severe hyperbilirubinemia | 0.882 | 0.379 | 0.261 | 0.03 |
| Hyperbilirubinemia and/or IVH | 0.882 | 0.379 | 0.261 | 0.03 |
| Severe hyperbilirubinemia and/or IVH | 0.353 | 0.931 | 0.284 | <0.001 |
| Male and/or hyperbilirubinemia and/or severe hyperbilirubinemia | 0.941 | 0.155 | 0.096 | 0.29 |
| Male and/or hyperbilirubinemia and/or IVH | 0.941 | 0.155 | 0.096 | 0.29 |
| Male and/or severe hyperbilirubinemia and/or IVH | 0.882 | 0.397 | 0.279 | 0.03 |
| Hyperbilirubinemia and/or severe hyperbilirubinemia and/or IVH | 0.882 | 0.379 | 0.261 | 0.03 |
| Male and/or hyperbilirubinemia and/or severe hyperbilirubinemia and/or IVH | 0.941 | 0.155 | 0.096 | 0.29 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakasone, R.; Fujioka, K.; Kyono, Y.; Yoshida, A.; Kido, T.; Suga, S.; Abe, S.; Ashina, M.; Nishida, K.; Tanimura, K.; et al. Neurodevelopmental Outcomes at 18 Months of Corrected Age for Late Preterm Infants Born at 34 and 35 Gestational Weeks. Int. J. Environ. Res. Public Health 2021, 18, 640. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020640
Nakasone R, Fujioka K, Kyono Y, Yoshida A, Kido T, Suga S, Abe S, Ashina M, Nishida K, Tanimura K, et al. Neurodevelopmental Outcomes at 18 Months of Corrected Age for Late Preterm Infants Born at 34 and 35 Gestational Weeks. International Journal of Environmental Research and Public Health. 2021; 18(2):640. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020640
Chicago/Turabian StyleNakasone, Ruka, Kazumichi Fujioka, Yuki Kyono, Asumi Yoshida, Takumi Kido, Shutaro Suga, Shinya Abe, Mariko Ashina, Kosuke Nishida, Kenji Tanimura, and et al. 2021. "Neurodevelopmental Outcomes at 18 Months of Corrected Age for Late Preterm Infants Born at 34 and 35 Gestational Weeks" International Journal of Environmental Research and Public Health 18, no. 2: 640. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020640