A Multilingual Integrative Review of Health Literacy in Former Soviet Union, Russian-Speaking Immigrants

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
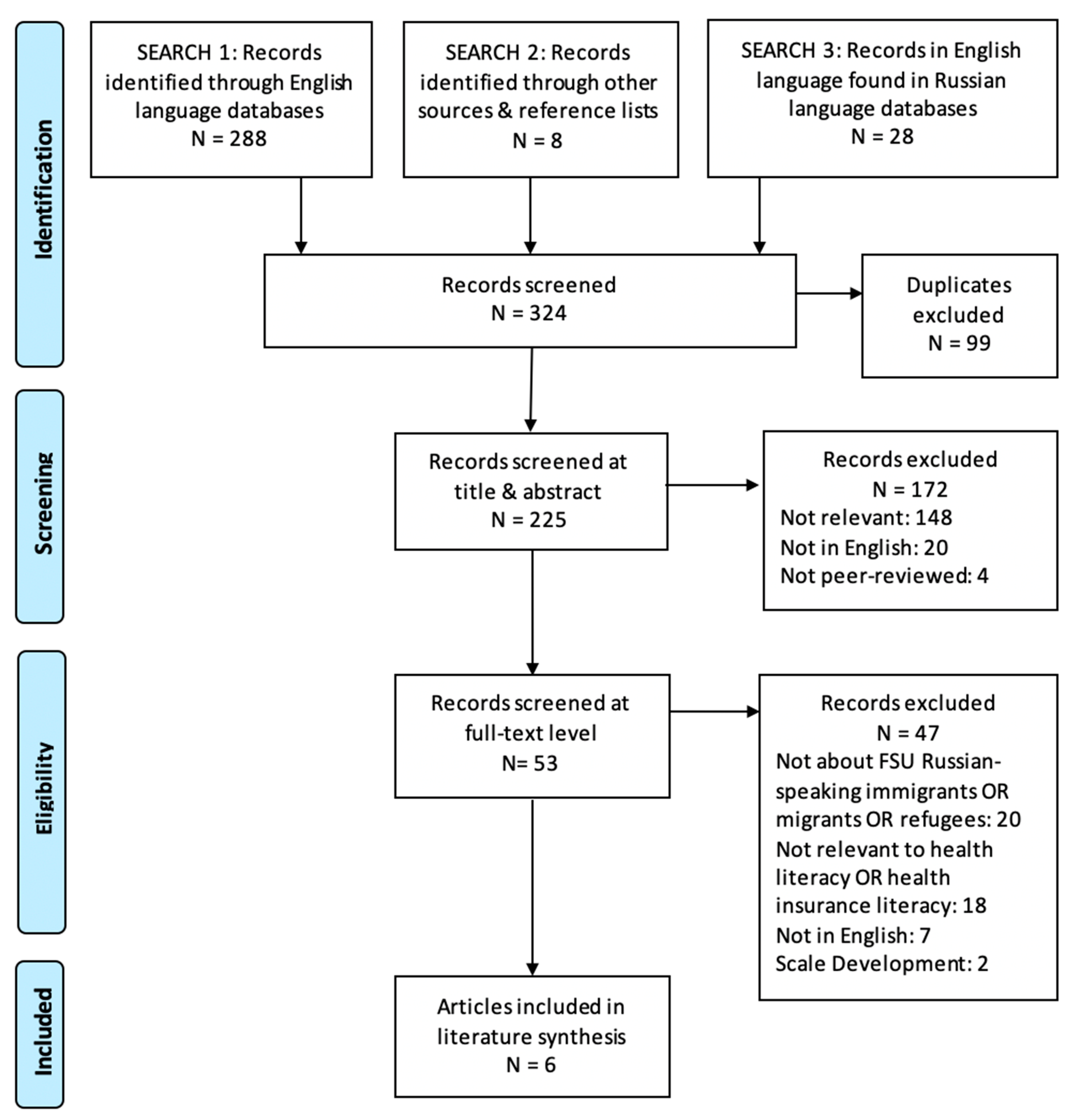
2.2. English Search
2.3. Russian, German, and Hebrew Searches
3. Results
3.1. English Language Articles
3.2. Russian, German, Hebrew Languages Articles
3.3. Summary of Studies
3.3.1. Assessment of Health Literacy in FSU Immigrants
3.3.2. Characteristics of FSU Immigrants
3.3.3. Language and Culture
3.4. Other Articles Describing Constructs Related to Health Literacy
3.4.1. Healthcare System, Access to Care, and Utilization of Health Services
3.4.2. Health Status
3.4.3. Language and Acculturation
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kickbusch, I.; Pelikan, J.M.; Apfel, F.; Tsouros, A.D. Health Literacy: The Solid Facts; World Health Organization, Ed.; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Health Literacy in Healthy People. Available online: https://health.gov/our-work/healthy-people-2030/about-healthy-people-2030/health-literacy-healthy-people (accessed on 24 October 2020).
- Nutbeam, D. Health Literacy as a Public Health Goal: A Challenge for Contemporary Health Education and Communication Strategies into the 21st Century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Nutbeam, D.; Lloyd, J.E. Understanding and Responding to Health Literacy as a Social Determinant of Health. Annu. Rev. Public Health 2021, 42. [Google Scholar] [CrossRef]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health Literacy in Europe: Comparative Results of the European Health Literacy Survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [Green Version]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low Health Literacy and Health Outcomes: An Updated Systematic Review. Ann. Intern. Med. 2011, 155, 97. [Google Scholar] [CrossRef] [PubMed]
- Nielsen-Bohlman, L.; Panzer, A.M.; Kindig, D.A. Health Literacy: A Prescription to End Confusion; National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Logan, R.A.; Siegel, E.R. Health Literacy: New Directions in Research, Theory and Practice, 1st ed.; IOS Press: Washington, DC, USA, 2017. [Google Scholar]
- Levy, H.; Janke, A. Health Literacy and Access to Care. J. Health Commun. 2016, 21, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Rasu, R.S.; Bawa, W.A.; Suminski, R.; Snella, K.; Warady, B. Health Literacy Impact on National Healthcare Utilization and Expenditure. Int. J. Health Policy Manag. 2015, 4, 747–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vernon, J.A.; Trujillo, A.; Rosenbaum, S.; DeBuono, B. Low Health Literacy: Implications for National Health Policy. Health Policy Manag. 2007, 172, 1–18. [Google Scholar]
- Cutilli, C.C.; Bennett, I.M. Understanding the Health Literacy of America: Results of the National Assessment of Adult Literacy. Orthop. Nurs. 2009, 28, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Kutner, M.; Greenberg, E.; Jin, Y.; Paulsen, C.; White, S. The Health Literacy of America’s Adults: Results from the 2003 National Assessment of Adult Literacy; National Center for Educational Statistics (ED): Washington, DC, USA; American Institutes for Research (CRESS): Kensington, MD, USA, 2006; p. 37. [Google Scholar]
- Martin, L.T.; Ruder, T.; Escarce, J.J.; Ghosh-Dastidar, B.; Sherman, D.; Elliott, M.; Bird, C.E.; Fremont, A.; Gasper, C.; Culbert, A.; et al. Developing Predictive Models of Health Literacy. J. Gen. Intern. Med. 2009, 24, 1211–1216. [Google Scholar] [CrossRef] [Green Version]
- Sentell, T.L.; Braun, K.L. Low Health Literacy, Limited English Proficiency, and Health Status in Asians, Latinos, and Other Racial/Ethnic Groups in California. J. Health Commun. 2012, 17 (Suppl. 3), 82–99. [Google Scholar] [CrossRef] [Green Version]
- Schaeffer, D.; Berens, E.-M.; Vogt, D. Health Literacy in the German Population. Dtsch. Arzteblatt Int. 2017, 114, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Berens, E.-M.; Vogt, D.; Messer, M.; Hurrelmann, K.; Schaeffer, D. Health Literacy among Different Age Groups in Germany: Results of a Cross-Sectional Survey. BMC Public Health 2016, 16. [Google Scholar] [CrossRef] [Green Version]
- Levin-Zamir, D.; Baron-Epel, O.B.; Cohen, V.; Elhayany, A. The Association of Health Literacy with Health Behavior, Socioeconomic Indicators, and Self-Assessed Health from a National Adult Survey in Israel. J. Health Commun. 2016, 21 (Suppl. 2), 61–68. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.M.; Shepard, L.; Berg, R.V.D.; Ward-Waller, C.; Smith, P.; Weiss, B.D. A Novel Approach to Improve Health Literacy in Immigrant Communities. Health Lit. Res. Pract. 2019, 3, S15–S24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, E.; Fredricks, K.; Woc-Colburn, L.; Bottazzi, M.E.; Weatherhead, J. Disproportionate Impact of the COVID-19 Pandemic on Immigrant Communities in the United States. PLoS Negl. Trop. Dis. 2020, 14, e0008484. [Google Scholar] [CrossRef]
- Guadagno, L. Migrants and the COVID-19 Pandemic: An Initial Analysis; International Organization for Migration: Grand-Saconnex, Switzerland, 2020. [Google Scholar]
- Jain, A.; van Hoek, A.J.; Boccia, D.; Thomas, S.L. Lower Vaccine Uptake amongst Older Individuals Living Alone: A Systematic Review and Meta-Analysis of Social Determinants of Vaccine Uptake. Vaccine 2017, 35, 2315–2328. [Google Scholar] [CrossRef] [PubMed]
- Walter, D.; Atzpodien, K.; Pins, C.; Wichmann, O.; Reiter, S. Factors influencing the uptake of vaccines by adolescents with migration background. A qualitative study of adolescents, mothers, and physicians. Bundesgesundheitsblatt Gesundh. Gesundh. 2013, 56, 1368–1375. [Google Scholar] [CrossRef] [Green Version]
- Wolf, E.; Rowhani-Rahbar, A.; Tasslimi, A.; Matheson, J.; DeBolt, C. Parental Country of Birth and Childhood Vaccination Uptake in Washington State. Pediatrics 2016, 138. [Google Scholar] [CrossRef] [Green Version]
- Košir, U.; Sørensen, K. COVID-19: The Key to Flattening the Curve Is Health Literacy. Perspect. Public Health 2020, 175791392093671. [Google Scholar] [CrossRef]
- Paakkari, L.; Okan, O. COVID-19: Health Literacy Is an Underestimated Problem. Lancet Public Health 2020, 5, e249–e250. [Google Scholar] [CrossRef]
- Sironi, A.; Bauloz, C.; Emmanuel, M. (Eds.) Glossary on Migration; International Organization for Migration: Grand-Saconnex, Switzerland, 2019; p. 248. [Google Scholar]
- Ingram, A. Broadening Russia’s Borders? The Nationalist Challenge of the Congress of Russian Communities. Polit. Geogr. 2001, 20, 197–219. [Google Scholar] [CrossRef]
- Ryazantsev, S.V. The Modern Russian-Speaking Communities in the World: Formation, Assimilation and Adaptation in Host Societies. Mediterr. J. Soc. Sci. 2015, 6. [Google Scholar] [CrossRef]
- Suslov, M. “Russian World”: Russia’s Policy towards Its Diaspora; Russia/NIS Center: Brussels, Belgium; Paris, France, 2017; p. 32. [Google Scholar]
- McAuliffe, M.; Khadria, B.; Bauloz, C. World Migration Report 2020; International Organization for Migration: Geneva, Switzerland, 2019; Available online: https://publications.iom.int/system/files/pdf/wmr_2020.pdf (accessed on 17 December 2020).
- Kostareva, U.; Albright, C.L.; Berens, E.-M.; Levin-Zamir, D.; Aringazina, A.; Lopatina, M.; Ivanov, L.L.; Sentell, T.L. International Perspective on Health Literacy and Health Equity: Factors That Influence the Former Soviet Union Immigrants. Int. J. Environ. Res. Public. Health 2020, 17, 2155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borschel-Dan, A. 25 Years Later, Russian Speakers Still the ‘Other’ in Israel, Says MK. Available online: http://www.timesofisrael.com/25-years-later-russian-speakers-still-the-other-in-israel-says-mk/ (accessed on 24 October 2020).
- Chudinovskikh, O.; Denisenko, M. Russia: A Migration System with Soviet Roots. Available online: https://www.migrationpolicy.org/article/russia-migration-system-soviet-roots (accessed on 24 October 2020).
- McPhillips, D. Russia’s “Slow Bleeding” Brain Drain. Available online: https://www.usnews.com/news/best-countries/articles/2016-10-06/countries-with-the-most-russian-emigrants (accessed on 24 October 2020).
- Semenova, K. A New Emigration: The Best Are Leaving. Part 1. Available online: https://imrussia.org/en/analysis/nation/2224-a-new-emigration-the-best-are-leaving-part-1 (accessed on 24 October 2020).
- Official Data Vastly Underestimates Russian Emigration—Report. Available online: https://www.themoscowtimes.com/2019/01/16/official-data-vastly-underestimates-russian-emigration-report-a64158 (accessed on 24 October 2020).
- Elias, N.; Shorer, M. Immigrants of the World Unite? A Virtual Community of Russian-Speaking Immigrants on the Web. J. Int. Commun. 2006, 12, 70–90. [Google Scholar] [CrossRef]
- U.S. Census Bureau. Selected Social Characteristics in the United States; American Community Survey; U.S. Census Bureau: 2007. Available online: https://archive.vn/r04E0 (accessed on 24 October 2020).
- Ryan, C. Language Use in the United States: 2011; U.S. Department of Commerce: Washington, DC, USA, 2013; p. 16. [Google Scholar]
- Radio Russkaya Reklama. Available online: https://radio.rusrek.com/en/about-radio.html (accessed on 12 December 2019).
- Population and Employment. Households and Families. Microcensus Results 2018. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Haushalte-Familien/Publikationen/Downloads-Haushalte/haushalte-familien-2010300187004.pdf?__blob=publicationFile (accessed on 24 January 2020).
- Immigrants by Period of Immigration, Country of Birth and Last Country of Residence. CBS, Central Bureau of Statistics 2018. Available online: https://www.cbs.gov.il/he/publications/doclib/2018/4.%20shnatonimmigration/st04_04.pdf (accessed on 24 October 2020).
- Fernández-Gutiérrez, M.; Bas-Sarmiento, P.; Albar-Marín, M.J.; Paloma-Castro, O.; Romero-Sánchez, J.M. Health Literacy Interventions for Immigrant Populations: A Systematic Review. Int. Nurs. Rev. 2018, 65, 54–64. [Google Scholar] [CrossRef] [Green Version]
- Ward, M.; Kristiansen, M.; Sørensen, K. Migrant Health Literacy in the European Union: A Systematic Literature Review. Health Educ. J. 2018, 15. [Google Scholar] [CrossRef]
- Quincy, L.; Berkman, N.D.; Bicego, K.L.; Braun, B.; Carman, C.; Coltin, K.; Huston, S.; Keller, S.; Little, L.; Rush, S.; et al. Measuring Health Insurance Literacy: A Call to Action. A Report from the Health Insurance Literacy Expert Roundtable; Consumers Union, University of Maryland College Park, and American Institutes for Research: College Park, MD, USA, 2012. [Google Scholar]
- Kaiser Family Foundation. Key Facts about the Uninsured Population; KFF: San Francisco, CA, USA, 2018; p. 14. [Google Scholar]
- Norton, M.; Hamel, L.; Brodie, M. Assessing Americans’ Familiarity with Health Insurance Terms and Concepts; The Henry J. Kaiser Family Foundation, KFF: San Francisco, CA, USA, 2014. [Google Scholar]
- Whittemore, R.; Knafl, K. The Integrative Review: Updated Methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Syrtsova, L.E.; Abrosimova, Y.; Lopatina, M. Health literacy: Content of the concept. Russ. J. Prev. Med. Public Health 2016, 19, 58–63. [Google Scholar] [CrossRef]
- Horn, A.; Vogt, D.; Messer, M.; Schaeffer, D. Health Literacy von Menschen mit Migrationshintergrund in der Patientenberatung stärken: Ergebnisse einer qualitativen Evaluation. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2015, 58, 577–583. [Google Scholar] [CrossRef]
- Nakash, O.; Hayat, T.; Abu Kaf, S.; Cohen, M. Association between Knowledge about How to Search for Mental Health Information and Emotional Distress among Older Adults: The Moderating Role of Immigration Status. J. Gerontol. Soc. Work 2020, 63, 78–91. [Google Scholar] [CrossRef] [PubMed]
- Van Son, C.R. Developing Culturally Targeted Diabetes Educational Materials for Older Russian-Speaking Immigrants. Diabetes Educ. 2014, 40, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Bailey, S.C.; Sarkar, U.; Chen, A.H.; Schillinger, D.; Wolf, M.S. Evaluation of Language Concordant, Patient-Centered Drug Label Instructions. J. Gen. Intern. Med. 2012, 27, 1707–1713. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, C.H. Partnering with Community Agencies to Provide Nursing Students with Cultural Awareness Experiences and Refugee Health Promotion Access. J. Nurs. Educ. 2009, 48, 519–522. [Google Scholar] [CrossRef]
- Culturally and Linguistically Appropriate Services (CLAS). Agency for Healthcare Research and Quality. Available online: http://www.ahrq.gov/sdoh/clas/index.html (accessed on 14 December 2020).
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H.; Brand, H. Health Literacy and Public Health: A Systematic Review and Integration of Definitions and Models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Lubotzky-Gete, S.; Shoham-Vardi, I.; Sheiner, E. Comparing Pregnancy Outcomes of Immigrants from Ethiopia and the Former Soviet Union to Israel, to Those of Native-Born Israelis. J. Immigr. Minor. Health 2016, 19, 1296–1303. [Google Scholar] [CrossRef]
- Gross, R.; Bramley-Greenberg, S. Supplemental Health Insurance: Changes in Policy and Consumer Behavior. Soc. Secur. (Hebr. Ed.) 2001, 61, 154–171. [Google Scholar]
- Ivanov, L.L.; Buck, K. Health Care Utilization Patterns of Russian-Speaking Immigrant Women across Age Groups. J. Immigr. Health 2002, 4, 17–27. [Google Scholar] [CrossRef]
- Aroian, K.J.; Khatutsky, G.; Tran, T.V.; Balsam, A.L. Health and Social Service Utilization among Elderly Immigrants from the Former Soviet Union. J. Nurs. Scholarsh. 2001, 33, 265–271. [Google Scholar] [CrossRef]
- Bodenheimer, T.; Grumbach, K. Understanding Health Policy: A Clinical Approach, 7th ed.; McGraw-Hill Education: New York, NY, USA, 2016. [Google Scholar]
- Ivanov, L.L.; Hu, J.; Leak, A. Immigrant Women’s Cancer Screening Behaviors. J. Community Health Nurs. 2010, 27, 32–45. [Google Scholar] [CrossRef]
- Silko, A. Increasing Breast Cancer Screening in Russian Immigrant Women: Identifying Barriers and Providing On-Site Mammography. J. Dr. Nurs. Pract. 2017, 10, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Yarova, L.A.; Krassen Covan, E.; Fugate-Whitlock, E. Effect of Acculturation and Health Beliefs on Utilization of Health Care Services by Elderly Women Who Immigrated to the USA From the Former Soviet Union. Health Care Women Int. 2013, 34, 1097–1115. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, E.T. The Burden of Culture? Health Outcomes among Immigrants from the Former Soviet Union in the United States. J. Immigr. Minor. Health 2012, 14, 315–322. [Google Scholar] [CrossRef]
- Kaucher, S.; Deckert, A.; Becher, H.; Winkler, V. Migration Pattern and Mortality of Ethnic German Migrants from the Former Soviet Union: A Cohort Study in Germany. BMJ Open. 2017, 7, e019213. [Google Scholar] [CrossRef] [Green Version]
- Kirkcaldy, B.D.; Siefen, R.G.; Wittig, U.; Schüller, A.; Brähler, E.; Merbach, M. Health and Emigration: Subjective Evaluation of Health Status and Physical Symptoms in Russian-Speaking Migrants. Stress Health 2005, 21, 295–309. [Google Scholar] [CrossRef]
- Quenzel, G.; Schaeffer, D. Health Literacy—Gesundheitskompetenz Vulnerabler Bevölkerungsgruppen; Universität Bielefeld: Bielefeld, Germany, 2016; p. 101. [Google Scholar]
- Niral, N.; Rosen, B.; Gross, R.; Berga Yuval, D.; Ivankovsky, M. Immigrants from the Former Soviet Union in the Health System: Selected Findings from National Surveys. Soc. Secur. (Hebr. Ed.) 1998, 51, 96–115. [Google Scholar]
- Landa, A.; Skritskaya, N.; Nicasio, A.; Humensky, J.; Lewis-Fernández, R. Unmet Need for Treatment of Depression among Immigrants from the Former USSR in the US: A Primary Care Study. Int. J. Psychiatry Med. 2015, 50, 271–289. [Google Scholar] [CrossRef]
- Mirsky, J. Mental Health Implications of Migration: A Review of Mental Health Community Studies on Russian-Speaking Immigrants in Israel. Soc. Psychiatry Psychiatr. Epidemiol. 2009, 44, 179–187. [Google Scholar] [CrossRef]
- Bachmann, V.; Teigeler, K.; Hirsch, O.; Bösner, S.; Donner-Banzhoff, N. Comparing Health-Issues of Russian-Speaking Immigrants, Germans and Russians. Int. J. Migr. Health Soc. Care 2015, 11, 45–56. [Google Scholar] [CrossRef]
- Gross, R.; Baum, N.; Oved-Or, M. Factors Associated with Seeking Formal and Informal Help for Mental Distress in the General Population in Israel. Soc. Secur. (Hebr. Ed.) 2009, 79, 111–140. [Google Scholar]
- Brouwer, A.M.; Mosack, K.E.; Wendorf, A.R.; Sokolova, L. Patterns of Missing Data in Ethnic Minority Health Research: A Survey Project with Russian-Speaking Immigrant Women with Hypertension. Res. Theory Nurs. Pract. 2013, 27, 276–295. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.K.; Schenk, L.; Rommel, A.; Thamm, R.; Ellert, U.; Lampert, T. Inanspruchnahme ambulant ärztlicher Leistungen und Zufriedenheit mit der Versorgung bei Kindern und Jugendlichen mit Migrationshintergrund—Ergebnisse der KiGGS-Studie. Bundesgesundheitsbl 2020, 63, 103–112. [Google Scholar] [CrossRef]
- Engelman, M.; Kestenbaum, B.; Zuelsdorff, M.; Mehta, N.; Lauderdale, D.; Kestenbaum, B.M.; Zuelsdorff, M.L.; Mehta, N.K.; Lauderdale, D.S. Work Disability Among Native-Born and Foreign-Born Americans: On Origins, Health, and Social Safety Nets. Demography 2017, 54, 2273–2300. [Google Scholar] [CrossRef]
- Jurcik, T.; Chentsova-Dutton, Y.E.; Solopieieva-Jurcikova, I.; Ryder, A.G. Russians in Treatment: The Evidence Base Supporting Cultural Adaptations. J. Clin. Psychol. 2013, 69, 774–791. [Google Scholar] [CrossRef] [PubMed]
- Jurcik, T.; Yakobov, E.; Solopieieva-Jurcikova, L.; Ahmed, R.; Sunohara, M.; Ryder, A.G. Unraveling Ethnic Density Effects, Acculturation, and Adjustment: The Case of Russian-Speaking Immigrants from the Former Soviet Union. J. Community Psychol. 2015, 43, 628–648. [Google Scholar] [CrossRef]
- Vinokurov, A.; Trickett, E.J.; Birman, D. Community Context Matters: Acculturation and Underemployment of Russian-Speaking Refugees. Int. J. Intercult. Relat. 2017, 57, 42–56. [Google Scholar] [CrossRef]
- Blumstein, T.; Benyamini, Y.; Boyko, V.; Lerner-Geva, L. Women’s Knowledge about Heart Disease: Differences among Ethnic and Cultural Groups in the Israeli Women’s Health in Midlife Study. Women Health 2016, 56, 78–97. [Google Scholar] [CrossRef] [PubMed]
- Ben Natan, M.; Brandin Rimkus, A.; Tseytlin Eryomine, A. Factors Associated with Intention of Israeli-born Women and Immigrant Women from the Former Soviet Union to Take Folic Acid before and during Pregnancy. Int. J. Nurs. Pract. 2017, 24, e12622. [Google Scholar] [CrossRef]
- Gesser-Edelsburg, A.; Endevelt, R.; Zemach, M.; Tirosh-Kamienchick, Y. Food Consumption and Nutritional Labeling Among Immigrants to Israel from the Former Soviet Union. J. Immigr. Minor. Health 2015, 17, 459–466. [Google Scholar] [CrossRef]
- Lubman, N.; Doak, C.; Jasti, S. Food Label Use and Food Label Skills among Immigrants from the Former Soviet Union. J. Nutr. Educ. Behav. 2012, 44, 398–406. [Google Scholar] [CrossRef]
- Bachmann, V.; Völkner, M.; Bösner, S.; Donner-Banzhoff, N. The Experiences of Russian-Speaking Migrants in Primary Care Consultations. Deutsches Aerzteblatt Online 2014, 111, 871–876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonhardt, M.; Aschenbrenner, K.; Kreis, M.E.; Lauscher, J.C. Exploring the Characteristics and Potential Disparities of Non-Migrant and Migrant Colorectal Cancer Patients Regarding Their Satisfaction and Subjective Perception of Care—A Cross-Sectional Study. BMC Health Serv. Res. 2018, 18. [Google Scholar] [CrossRef] [PubMed]
- Barko, R.; Corbett, C.F.; Allen, C.B.; Shultz, J.A. Perceptions of Diabetes Symptoms and Self-Management Strategies: A Cross-Cultural Comparison. J. Transcult. Nurs. 2011, 22, 274–281. [Google Scholar] [CrossRef]
- Benisovich, S.V.; King, A.C. Meaning and Knowledge of Health among Older Adult Immigrants from Russia: A Phenomenological Study. Health Educ. Res. 2003, 18, 135–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Son, C.R.; Gileff, T.Y. Relying on What They Know: Older Slavic Émigrés Managing Chronic Health Conditions. Qual. Health Res. 2013, 23, 1660–1671. [Google Scholar] [CrossRef] [PubMed]
- Van Son, C.R.; Stasyuk, O. Older Immigrants from the Former Soviet Union and Their Use of Complementary and Alternative Medicine. Geriatr. Nur. (Lond.) 2014, 35, S45–S48. [Google Scholar] [CrossRef] [PubMed]
- Hölzel, L.P.; Ries, Z.; Kriston, L.; Dirmaier, J.; Zill, J.M.; Rummel-Kluge, C.; Niebling, W.; Bermejo, I.; Härter, M. Effects of Culture-Sensitive Adaptation of Patient Information Material on Usefulness in Migrants: A Multicentre, Blinded Randomised Controlled Trial. BMJ Open. 2016, 6, e012008. [Google Scholar] [CrossRef] [PubMed]
- Elias, N.; Lemish, D. Between Three Worlds: Host, Homeland, and Global Media in the Lives of Russian Immigrant Families in Israel and Germany. J. Fam. Issues 2011, 32, 1245–1274. [Google Scholar] [CrossRef]
- Abel, T.; McQueen, D. Critical Health Literacy and the COVID-19 Crisis. Health Promot. Int. 2020. [Google Scholar] [CrossRef]
- Okan, O.; Bollweg, T.M.; Berens, E.-M.; Hurrelmann, K.; Bauer, U.; Schaeffer, D. Coronavirus-Related Health Literacy: A Cross-Sectional Study in Adults during the COVID-19 Infodemic in Germany. Int. J. Environ. Res. Public. Health 2020, 17, 5503. [Google Scholar] [CrossRef]
- Sentell, T.L.; Vamos, S.; Okan, O. Interdisciplinary Perspectives on Health Literacy Research around the World: More Important than Ever in a Time of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 3010. [Google Scholar] [CrossRef] [PubMed]
- Lyons, G. Language: Another Cause of Publication Bias. Eur. J. Anaesthesiol. 2016, 33, 620–621. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Category | Inclusion | Exclusion |
|---|---|---|
| Type of article | Qualitative and quantitative, peer-reviewed original research articles, editorials and think papers, empirical research, concept papers, reviews, surveys | Scale development studies, conference papers, research protocols, dissertations/theses |
| Population | Adult Russian-speaking immigrants or migrants or refugees from FSU | Children or adolescents, not clearly identified population |
| Article focus | Health literacy or health insurance literacy | Other |
| Language | English, German, Hebrew, Russian | Other |
| Language | Search Strategy | Results |
|---|---|---|
| Russian | - Four databases and one search engine: Web of Science (Russian Science Citation Index), elibrary.ru, mediasphera.ru, cyberleninka.ru, yandex.ru; and, manual reference list review. - Searched up to 13 January 2019.- Search terms: медицинская грамoтнoсть OR здoрoвьесберегающее пoведение OR грамoтнoсть в вoпрoсах здoрoвья (all mean health literacy in Russian). - Two independent reviewers (U.K., P.P.) performed screening separately and met for consensus. A third reviewer (L.L.I) was available to resolve disagreements, but none occurred. | - A total of 257 unique articles were identified but no relevant articles were found at the title/abstract screening step. - We stopped our analysis at the title/abstract for the following reasons: (1) There is no concordance about health literacy terminology in the Russian language literature with more than eight circulating terms, making it difficult to identify and synthesize literature; and, (2) only recently a concordant term “грамoтнoсть в вoпрoсах здoрoвья”, was proposed by Syrtsova et al. (2016) and later accepted by the World Health Organization [51]. - All articles were published in the 2000s. - We found no articles about FSU immigrants (those who moved to another country outside of the FSU region). |
| German | - Google Scholar and manual reference list search. - Searched up to 27 October 2020. - Search terms: Gesundheitskompetenz (health literacy) AND (Sowjet* OR Soviet OR russischsprachig OR Russland OR russisch*) AND (Migranten OR Menschen mit Migrationshintergrund OR Menschen mit Zuwanderungsgeschichte OR Flüchtling OR Geflüchtete OR Aussiedler). - Included articles, book chapters, and reports. - Also searched by countries of origin. - Search and review performed by E.-M.B. | - A total of 62 unique articles were identified and screened at full text. - One article by Horn et al. (2015) met the inclusion criteria [52]. - No articles assessed health literacy. - Identified publications were either about immigrants in general or not specifically about health literacy in FSU immigrants or health literacy was mentioned as an explanatory factor for differences in health status or health service utilization but was not the focal topic. - No articles identified when searched for health literacy by FSU region countries. - The term health literacy is still relatively new in Germany. |
| Hebrew | - Google Scholar and University of Haifa library. - Searched up to 28 October 2020. - Search terms: אוריינות בריאות (health literacy) ANDרוסית (Russian) - Search and review performed by D.E.K. | - A total of 5 unique articles were identified when searching for both terms. - For reference, a search for just “health literacy,” without specifying “Russian,” yielded a total of 54 unique articles. - Identified articles did not include health literacy as a focal topic. - A few older articles (from the 1990s) examined (either exclusively or as part of a larger study) the use of health services by the Russian-speaking FSU immigrants. - The term health literacy is still relatively new in Israel. |
| Author & Year | Country (State) | Purpose | Setting | Sample | Type | Findings | Theoretical Framework or Model | Discipline | Evaluation |
|---|---|---|---|---|---|---|---|---|---|
| English Language | |||||||||
| Kostareva et al. 2020 | USA, Israel, Germany, Kazakhstan, Russia | To provide an overview of FSU immigrants’ background and discuss system-level factors relevant to FSU immigrants’ health literacy by looking at post-Soviet healthcare systems (Russia, Kazakhstan) and the healthcare systems of top host countries (USA, Israel, Germany) | Conceptual paper; cross-country comparison | N/A | Scoping review | Multiple factors such as FSU immigrants’ health and cultural beliefs, previous experiences with and exposures to their native healthcare system may influence their health literacy in host countries | Sorensen’s Integrated Health Literacy Model | Nursing and public health | 1 |
| Nakash et al. 2020 | Israel | To examine the association between mental health literacy, emotional distress, and the role of immigration status among older adults | Self-reported questionnaires in Russian; participants recruited online and through social clubs | 222 Russian-speaking FSU immigrants (mean age 70) | Quantitative (assessed with Mental health literacy scale) | FSU demonstrated significantly lower mental health literacy and higher emotional distress | None | Social work and psychology | 2 |
| Levin-Zamir et al. 2016 | Israel | To examine the relationship between health literacy, health behavior, sociodemographic indicators, and self-assessed health in adults | Face-to-face home interviews in Russian | 55 Russian-speaking FSU immigrants (mean age 50) | Quantitative (assessed with HLS-EU-Q16 | FSU demonstrated inadequate health literacy and long-term Israeli Jews sufficient health literacy but no significant difference | None | Public health | 2 |
| Van Son 2014 | USA (Washington) | To develop and test 12 culturally appropriate dietary and physical activity education materials to improve health literacy and manage diabetes | Focus group (n = 10, age 65+) in Russian and telephone survey (n = 14) | 24 Russian-speaking Slavic immigrants | Qualitative | Culturally relevant to FSU educational materials around diabetes uploaded online and demonstrated to be of demand | The Plate Model and the Physical Activity Pyramid | Nursing | 1 |
| Bailey et al. 2012 | USA (San Francisco and Chicago) | To evaluate the efficacy of health literacy informed, translated drug label instructions in comparison to standard instructions | Clinics and community-based organizations for low-income urban populations | 40 Russian-speakers with limited English proficiency (mean age 64) | Quantitative | Translated, health literacy adopted drug labels led to significantly greater understanding, regimen dosing, and regimen consolidation comparing to standard instructions | None | Medicine | 2 |
| Sullivan 2009 | USA (Alaska) | To describe a teaching-learning strategy emphasizing community partnership between nursing students, an immigrant refugee program, and a community literacy program | Immigrant-refugee and community literacy programs | 36 Russian refugees | Qualitative | Russian-speaking refugees’ top 3 health concerns: healthy eating, women’s health, and high blood pressure | Leininger’s Culture Care Theory | Nursing | 1 |
| German Language | |||||||||
| Horn et al. 2015 | Germany | To identify factors relevant to health literacy in the context of health counseling among migrants | Interviews at a patient health counseling organization with health consultants (experts in Turkish and Russian health counseling) and users of health counseling | 6 focus groups, 24 interviews with health consultants, 9 potential and 9 actual users of counseling of Russian and Turkish background | Qualitative | Russian-speaking FSU immigrants appear to have difficulty understanding the German healthcare system and utilizing health services effectively | Sorensen’s Integrated Health Literacy Model | Public health | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostareva, U.; Albright, C.L.; Berens, E.-M.; Polansky, P.; Kadish, D.E.; Ivanov, L.L.; Sentell, T.L. A Multilingual Integrative Review of Health Literacy in Former Soviet Union, Russian-Speaking Immigrants. Int. J. Environ. Res. Public Health 2021, 18, 657. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020657
Kostareva U, Albright CL, Berens E-M, Polansky P, Kadish DE, Ivanov LL, Sentell TL. A Multilingual Integrative Review of Health Literacy in Former Soviet Union, Russian-Speaking Immigrants. International Journal of Environmental Research and Public Health. 2021; 18(2):657. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020657
Chicago/Turabian StyleKostareva, Uliana, Cheryl L. Albright, Eva-Maria Berens, Patricia Polansky, Deborah E. Kadish, Luba L. Ivanov, and Tetine L. Sentell. 2021. "A Multilingual Integrative Review of Health Literacy in Former Soviet Union, Russian-Speaking Immigrants" International Journal of Environmental Research and Public Health 18, no. 2: 657. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020657