Environmental Risk Factors and Health: An Umbrella Review of Meta-Analyses

 ,
,  and
and
Abstract
:1. Introduction
2. Methodology
2.1. Literature Search
Search Strategy
2.2. Selection Criteria
2.3. Data Extraction and Analysis
3. Results
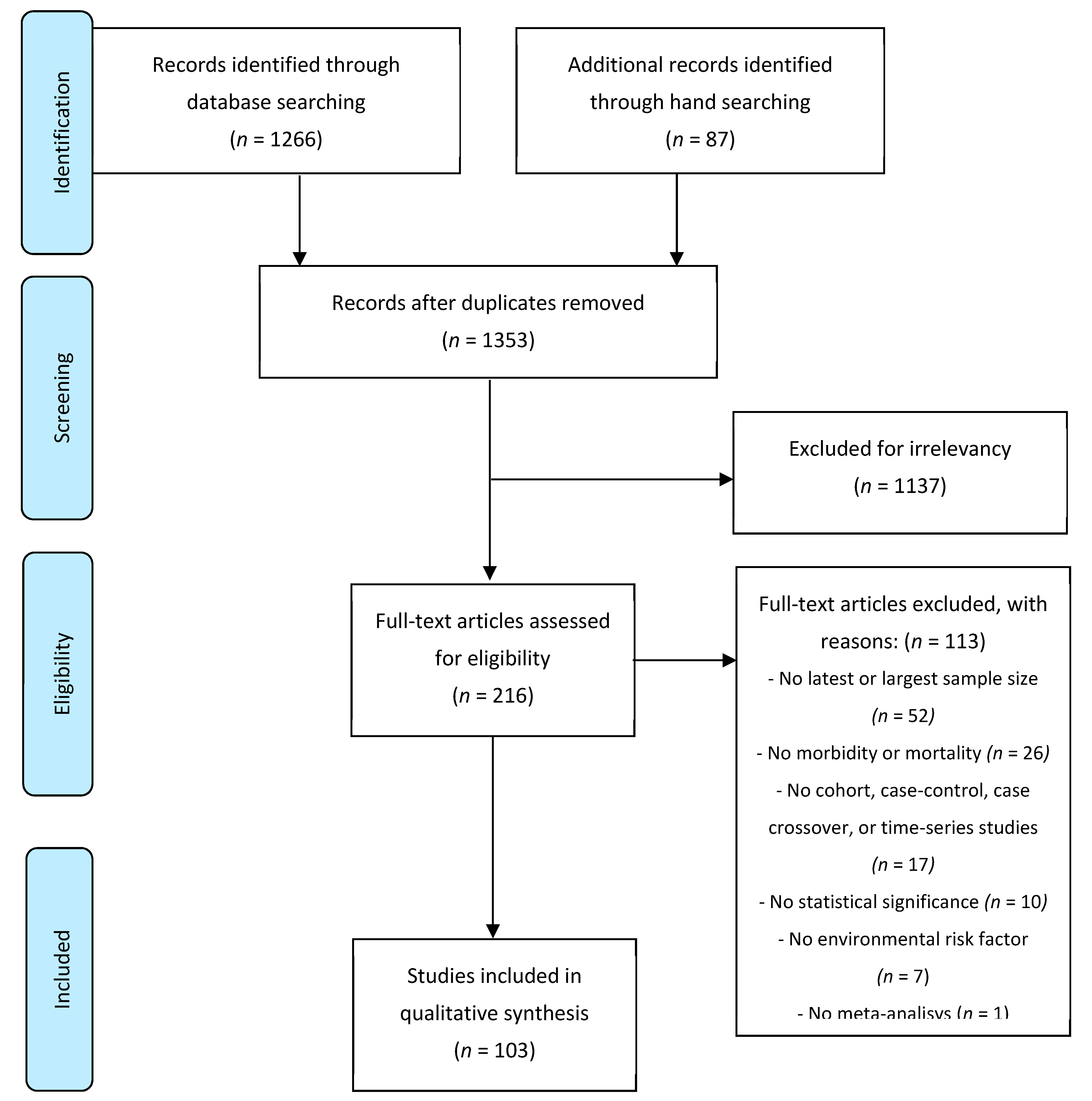
3.1. Literature Review
3.2. Air Pollution
3.3. Environmental Tobacco Smoke
3.4. Chemicals, Pesticides, and Heavy Metals
3.5. Physical Exposures
3.6. Residential Surroundings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prüss-Ustün, A.; Neira, M. Preventing Disease through Healthy Environments: A Global Assessment of the Environmental Burden of Disease; World Health Organization: Geneva, Switzerland, 2016; Volume 259. [Google Scholar]
- Prüss-Ustün, A. Environmental risks and non-communicable diseases. BMJ 2019, 365, 17–19. [Google Scholar] [CrossRef] [Green Version]
- Stanaway, J.D.; Afshin, A.; Gakidou, E.; Lim, S.S.; Abate, D.; Abate, K.H.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar] [CrossRef] [Green Version]
- Ioannidis, J.P.A. Integration of evidence from multiple meta-analyses: A primer on umbrella reviews, treatment networks and multiple treatments meta-analyses. CMAJ 2009, 181, 488–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, M.Y.; Lo, W.C.; Chao, C.-T.; Wu, M.S.; Chiang, C.K. Association between air pollutants and development of chronic kidney disease: A systematic review and meta-analysis. Sci. Total Environ. 2020, 706. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Cheng, H.; Shen, C.; Liu, J.; Zhang, H.; Cao, J.; Ding, R. Effects of long-term exposure to air pollution on the incidence of type 2 diabetes mellitus: A meta-analysis of cohort studies. Environ. Sci. Pollut. Researc 2020, 27, 798–811. [Google Scholar] [CrossRef]
- Kim, H.-B.B.; Shim, J.-Y.Y.; Park, B.; Lee, Y.-J.J. Long-Term Exposure to Air Pollutants and Cancer Mortality: A Meta-Analysis of Cohort Studies. Int. J. Environ. Res. Public Health 2018, 15, 2608. [Google Scholar] [CrossRef] [Green Version]
- Burnett, R.T.; Arden Pope, C.; Ezzati, M.; Olives, C.; Lim, S.S.; Mehta, S.; Shin, H.H.; Singh, G.; Hubbell, B.; Brauer, M.; et al. An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ. Health Perspect. 2014, 122, 397–403. [Google Scholar] [CrossRef]
- Tsai, T.L.; Lin, Y.T.; Hwang, B.F.; Nakayama, S.F.; Tsai, C.H.; Sun, X.L.; Ma, C.; Jung, C.R. Fine particulate matter is a potential determinant of Alzheimer’s disease: A systemic review and meta-analysis. Environ. Res. 2019, 177, 108638. [Google Scholar] [CrossRef]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J.D. Long-term air pollution exposure and cardio- respiratory mortality: A review. Environ. Health 2013, 12, 43. [Google Scholar] [CrossRef] [Green Version]
- Faustini, A.; Rapp, R.; Forastiere, F. Nitrogen dioxide and mortality: Review and meta-analysis of long-term studies. Eur. Respir. J. 2014, 44, 744–753. [Google Scholar] [CrossRef] [Green Version]
- Braithwaite, I.; Zhang, S.; Kirkbride, J.B.; Osborn, D.P.J.; Hayes, J.F. Air pollution (Particulate matter) exposure and associations with depression, anxiety, bipolar, psychosis and suicide risk: A systematic review and meta-analysis. Environ. Health Perspect. 2019, 127, 126002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, S.; Wang, J.; Jiang, Q.; He, Z.; Huang, Y.; Li, Z.; Cai, L.; Cao, S. Long-term exposure to PM2.5 and stroke: A systematic review and meta-analysis of cohort studies. Environ. Res. 2019, 177, 108587. [Google Scholar] [CrossRef] [PubMed]
- Kasdagli, M.I.; Katsouyanni, K.; Dimakopoulou, K.; Samoli, E. Air pollution and Parkinson’s disease: A systematic review and meta-analysis up to 2018. Int. J. Hyg. Environ. Health 2019, 222, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Cesaroni, G.; Stafoggia, M.; Galassi, C.; Hilding, A.; Hoffmann, B.; Houthuijs, D.; Ostenson, C.; Overvad, K.; Pedersen, N.L. Long term exposure to ambient air pollution and incidence of acute coronary events: Prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project. BMJ 2014, 7412, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Héroux, M.; Anderson, H.; Atkinson, R.; Brunekreef, B.; Cohen, A.; Forastiere, F.; Hurley, F.; Katsouyanni, K.; Krewski, D.; Krzyzanowski, M.; et al. Quantifying the health impacts of ambient air pollutants: Recommendations of a WHO/Europe project. Int. J. Public Health 2015, 60, 619–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chun, H.K.; Leung, C.; Wen, S.W.; McDonald, J.; Shin, H.H. Maternal exposure to air pollution and risk of autism in children: A systematic review and meta-analysis. Environ. Pollut. 2020, 256. [Google Scholar] [CrossRef]
- Guo, L.-Q.; Chen, Y.; Mi, B.-B.; Dang, S.-N.; Zhao, D.-D.; Liu, R.; Wang, H.-L.; Yan, H. Ambient air pollution and adverse birth outcomes: A systematic review and meta-analysis. J. Zhejiang Univ. Sci. B (Biomed. Biotechnol.) 2019, 20, 238–252. [Google Scholar] [CrossRef]
- Khreis, H.; Ramani, T.; De Hoogh, K.; Mueller, N. Traffic-related air pollution and the local burden of childhood asthma in Bradford, UK. Int. J. Transp. Sci. Technol. 2018, 8, 116–128. [Google Scholar] [CrossRef]
- Lam, J.; Sutton, P.; Kalkbrenner, A.; Windham, G.; Halladay, A.; Koustas, E.; Lawler, C.; Davidson, L.; Daniels, N.; Newschaffer, C.; et al. A systematic review and meta-analysis of multiple airborne pollutants and autism spectrum disorder. PLoS ONE 2016, 11, e0161851. [Google Scholar] [CrossRef] [Green Version]
- Zhao, R.; Chen, S.; Wang, W.; Huang, J.; Wang, K.; Liu, L.; Wei, S. The impact of short-term exposure to air pollutants on the onset of out-of-hospital cardiac arrest: A systematic review and meta-analysis. Int. J. Cardiol. 2017, 226, 110–117. [Google Scholar] [CrossRef]
- Song, X.; Liu, Y.; Hu, Y.; Zhao, X.; Tian, J.; Ding, G.; Wang, S. Short-Term Exposure to Air Pollution and Cardiac Arrhythmia: A Meta-Analysis and Systematic Review. Int. J. Environ. Res. Public Health 2016, 13, 642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Chen, R.; Sera, F.; Vicedo-Cabrera, A.M.; Guo, Y.; Tong, S.; Coelho, M.S.Z.S.; Saldiva, P.H.N.; Lavigne, E.; Matus, P.; et al. Ambient Particulate Air Pollution and Daily Mortality in 652 Cities. N. Engl. J. Med. 2019, 381, 705–715. [Google Scholar] [CrossRef]
- Nhung, N.T.T.; Amini, H.; Schindler, C.; Kutlar Joss, M.; Dien, T.M.; Probst-Hensch, N.; Perez, L.; Künzli, N. Short-term association between ambient air pollution and pneumonia in children: A systematic review and meta-analysis of time-series and case-crossover studies. Environ. Pollut. 2017, 230, 1000–1008. [Google Scholar] [CrossRef] [PubMed]
- Stafoggia, M.; Zauli-Sajani, S.; Pey, J.; Samoli, E.; Alessandrini, E.; Basagaña, X.; Cernigliaro, A.; Chiusolo, M.; Demaria, M.; Díaz, J.; et al. Desert Dust Outbreaks in Southern Europe: Contribution to Daily PM 10 Concentrations and Short-Term Associations with Mortality and Hospital Admissions. Environ. Health Perspect. 2016, 124, 413–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellou, V.; Belbasis, L.; Tzoulaki, I.; Evangelou, E. Risk factors for type 2 diabetes mellitus: An exposure-wide umbrella review of meta-analyses. PLoS ONE 2018. [Google Scholar] [CrossRef]
- Chen, R.; Yang, J.; Zhang, C.; Li, B.; Bergmann, S.; Zeng, F.; Wang, H.; Wang, B. Global Associations of Air Pollution and Conjunctivitis Diseases: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, S.J.; Heinrich, J.; Bloom, M.S.; Zhao, T.Y.; Shi, T.X.; Feng, W.R.; Sun, Y.; Shen, J.C.; Yang, Z.C.; Yang, B.Y.; et al. Ambient air pollution and depression: A systematic review with meta-analysis up to 2019. Sci. Total Environ. 2020, 701, 134721. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, R.W.; Butland, B.K.; Dimitroulopoulou, C.; Heal, M.R.; Stedman, J.R.; Carslaw, N.; Jarvis, D.; Heaviside, C.; Vardoulakis, S.; Walton, H.; et al. Long-term exposure to ambient ozone and mortality: A quantitative systematic review and meta-analysis of evidence from cohort studies. BMJ Open 2016, 6, e009493. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Wang, Q.; He, S.; Wu, K.; Ren, M.; Dong, H.; Di, J.; Yu, Z.; Huang, C. Ambient air pollution and gestational diabetes mellitus: A review of evidence from biological mechanisms to population epidemiology. Sci. Total Environ. 2020, 719, 137349. [Google Scholar] [CrossRef]
- Josyula, S.; Lin, J.; Xue, X.; Rothman, N.; Lan, Q.; Rohan, T.E.; Dean, H.; Iii, H. Household air pollution and cancers other than lung: A meta-analysis. Env. Health 2015. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Yang, A.; He, X.; Liu, J.; Ma, Y.; Niu, J.; Luo, B. Indoor air pollution from solid fuels and hypertension: A systematic review and meta-analysis. Environ. Pollut. 2020, 259, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Amegah, A.K.; Quansah, R.; Jaakkola, J.J.K. Household air pollution from solid fuel use and risk of adverse pregnancy outcomes: A systematic review and meta-analysis of the empirical evidence. PLoS ONE 2014, 9, e113920. [Google Scholar] [CrossRef] [PubMed]
- Okello, S.; Akello, S.J.; Dwomoh, E.; Byaruhanga, E.; Opio, C.K.; Zhang, R.; Corey, K.E.; Muyindike, W.R.; Ocama, P.; Christiani, D.D. Biomass fuel as a risk factor for esophageal squamous cell carcinoma: A systematic review and meta-analysis. Environ. Health 2019, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Mao, J.; Ye, Z.; Li, J.; Zhao, H.; Liu, Y. Risk factors of chronic obstructive pulmonary disease among adults in Chinese mainland: A systematic review and meta-analysis. Respir. Med. 2017, 131, 158–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khreis, H.; Kelly, C.; Tate, J.; Parslow, R.; Lucas, K.; Nieuwenhuijsen, M. Exposure to traffic-related air pollution and risk of development of childhood asthma: A systematic review and meta-analysis. Environ. Int. 2017, 100, 1–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonardi-Bee, J.; Smyth, A.; Britton, J.; Coleman, T. Environmental tobacco smoke and fetal health: Systematic review and meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2008, 93, F351–F361. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, Q.; Li, W.; Deng, X.; Yang, B.; Huang, X. Association of prenatal and childhood environment smoking exposure with puberty timing: A systematic review and meta-analysis. Environ. Health Prev. Med. 2018, 23. [Google Scholar] [CrossRef]
- Lee, P.N.; Thornton, A.J.; Forey, B.A.; Hamling, J.S. Environmental Tobacco Smoke Exposure and Risk of Stroke in Never Smokers: An Updated Review with Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2017, 26, 204–216. [Google Scholar] [CrossRef] [Green Version]
- Ni, X.; Xu, N.; Wang, Q. Meta-Analysis and Systematic Review in Environmental Tobacco Smoke Risk of Female Lung Cancer by Research Type. Int. J. Environ. Res. Public Health 2018, 15, 1348. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Huang, Y.-B.; Liu, X.-O.; Gao, Y.; Dai, H.-J.; Song, F.-J.; Li, W.-Q.; Wang, J.; Yan, Y.; Wang, P.-S.; et al. Active and passive smoking with breast cancer risk for Chinese females: A systematic review and meta-analysis. Chin. J. Cancer 2014, 33, 306–316. [Google Scholar] [CrossRef]
- Lv, X.; Sun, J.; Bi, Y.; Xu, M.; Lu, J.; Zhao, L.; Xu, Y. Risk of all-cause mortality and cardiovascular disease associated with secondhand smoke exposure: A systematic review and meta-analysis. Int. J. Cardiol. 2015, 199, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Su, B.; Qin, W.; Xue, F.; Wei, X.; Guan, Q.; Jiang, W.; Wang, S.; Xu, M.; Yu, S. The relation of passive smoking with cervical cancer A systematic review and meta-analysis. Medicine 2018. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Lee, A.Y.C.; Hung, R.J.; McNallan, S.R.; Cote, M.L.; Lim, W.-Y.; Chang, S.-C.; Kim, J.H.; Ugolini, D.; Chen, Y.; et al. Exposure to secondhand tobacco smoke and lung cancer by histological type: A pooled analysis of the International Lung Cancer Consortium (ILCCO). Int. J. Cancer 2014, 135, 1918–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellou, V.; Belbasis, L.; Tzoulaki, I.; Middleton, L.T.; Ioannidis, J.P.A.; Evangelou, E. Systematic evaluation of the associations between environmental risk factors and dementia: An umbrella review of systematic reviews and meta-analyses. Alzheimer’s Dement. 2017, 13, 406–418. [Google Scholar] [CrossRef]
- Meng, X.; Sun, Y.; Duan, W.; Jia, C. Meta-analysis of the association of maternal smoking and passive smoking during pregnancy with neural tube defects. Int. J. Gynecol. Obstet. 2018, 140, 18–25. [Google Scholar] [CrossRef]
- He, Z.; Wu, H.; Zhang, S.; Lin, Y.; Li, R.; Xie, L.; Li, Z.; Sun, W.; Huang, X.; Zhang, C.J.P.; et al. The association between secondhand smoke and childhood asthma: A systematic review and meta-analysis. Pediatr. Pulmonol. 2020, 55, 2518–2531. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, M.; Zhang, J.; Zeng, L.; Wang, Y.; Zheng, Q.Y. Risk factors for chronic and recurrent otitis media-A meta-analysis. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [Green Version]
- Murray, R.; Asher, L.; Leonardi-Bee, J.; Hunter, A. The Effects of Tobacco Smoking, and Prenatal Tobacco Smoke Exposure, on Risk of Schizophrenia: A Systematic Review and Meta-Analysis. Nicotine Tob. Res. 2020, 22, 3–10. [Google Scholar] [CrossRef]
- Taylor, A.E.; Carslake, D.; De Mola, C.L.; Rydell, M.; Nilsen, T.I.L.L.; Bjørngaard, J.H.; Horta, B.L.; Pearson, R.; Rai, D.; Galanti, M.R.; et al. Maternal Smoking in Pregnancy and Offspring Depression: A cross cohort and negative control study. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; Wang, Y.; Zhang, L.; Zheng, Z.; Zhu, T.; Qu, Y.; Mu, D. Maternal Smoking and Attention- Deficit / Hyperactivity Disorder in Offspring: A Meta-analysis. Pediatrics 2018, 141, e20172465. [Google Scholar] [CrossRef] [Green Version]
- Riedel, C.; Schö, K.; Yang, S.; Koshy, G.; Chen, Y.-C.; Gopinath, B.; Ziebarth, S.; Diger Von Kries, R. Parental smoking and childhood obesity: Higher effect estimates for maternal smoking in pregnancy compared with paternal smoking-a meta-analysis. Int. J. Epidemiol. 2014, 1593–1606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rios, P.; Bailey, H.D.; Poulalhon, C.; Valteau-Couanet, D.; Schleiermacher, G.; Bergeron, C.; Petit, A.; Defachelles, A.S.; Marion, G.; Sirvent, N.; et al. Parental smoking, maternal alcohol consumption during pregnancy and the risk of neuroblastoma in children. A pooled analysis of the ESCALE and ESTELLE French studies. Int. J. Cancer 2019, 145, 2907–2916. [Google Scholar] [CrossRef] [PubMed]
- Chunxia, D.; Meifang, W.; Jianhua, Z.; Ruijuan, Z.; Xiue, L.; Zhuanzhen, Z.; Linhua, Y.; Gutti, R.K. Tobacco smoke exposure and the risk of childhood acute lymphoblastic leukemia and acute myeloid leukemia: A meta-Analysis. Medicine 2019, 98. [Google Scholar] [CrossRef] [PubMed]
- Milne, E.; Greenop, K.R.; Scott, R.J.; Bailey, H.D.; Attia, J.; Dalla-Pozza, L.; De Klerk, N.H.; Armstrong, B.K. Parental prenatal smoking and risk of childhood acute lymphoblastic leukemia. Am. J. Epidemiol. 2012, 175, 43–53. [Google Scholar] [CrossRef]
- Filippini, T.; Hatch, E.E.; Rothman, K.J.; Heck, J.E.; Park, A.S.; Crippa, A.; Orsini, N.; Vinceti, M. Association between Outdoor Air Pollution and Childhood Leukemia: A Systematic Review and Dose–Response Meta-Analysis. Environ. Health Perspect. 2019, 127, 046002. [Google Scholar] [CrossRef]
- Palin, O.; Herd, C.; Morrison, K.E.; Jagielski, A.C.; Wheatley, K.; Thomas, G.N.; Clarke, C.E. Systematic review and meta-analysis of hydrocarbon exposure and the risk of Parkinson’s disease. Park. Relat. Disord. 2015, 21, 243–248. [Google Scholar] [CrossRef]
- Bellou, V.; Belbasis, L.; Tzoulaki, I.; Evangelou, E.; Ioannidis, J.P.A. Environmental risk factors and Parkinson’s disease: An umbrella review of meta-analyses. Park. Relat. Disord. 2016, 23, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Belbasis, L.; Bellou, V.; Evangelou, E.; Ioannidis, J.P.A.A.; Tzoulaki, I. Environmental risk factors and multiple sclerosis: An umbrella review of systematic reviews and meta-analyses. Lancet Neurol. 2015, 14, 263–273. [Google Scholar] [CrossRef]
- Belbasis, L.; Dosis, V.; Evangelou, E. Elucidating the environmental risk factors for rheumatic diseases: An umbrella review of meta-analyses. Int. J. Rheum. Dis. 2018, 21, 1514–1524. [Google Scholar] [CrossRef]
- Freeman, M.D.; Kohles, S.S. Plasma levels of polychlorinated biphenyls, non-hodgkin lymphoma, and causation. J. Environ. Public Health 2012, 2012. [Google Scholar] [CrossRef] [Green Version]
- Cano-Sancho, G.; Ploteau, S.; Matta, K.; Adoamnei, E.; Louis, G.B.; Mendiola, J.; Darai, E.; Squifflet, J.; Le Bizec, B.; Antignac, J.P. Human epidemiological evidence about the associations between exposure to organochlorine chemicals and endometriosis: Systematic review and meta-analysis. Environ. Int. 2019, 123, 209–223. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Sunyer, J.; Casas, M.; Martínez, D.; Ballester, F.; Basterrechea, M.; Bonde, J.P.; Chatzi, L.; Chevrier, C.; Eggesbø, M.; et al. Prenatal exposure to DDE and PCB 153 and respiratory health in early childhood: A meta-analysis. Epidemiology 2014, 25, 544–553. [Google Scholar] [CrossRef] [PubMed]
- Rancière, F.; Lyons, J.G.; Loh, V.H.; Botton, J.; Galloway, T.; Wang, T.; Shaw, J.E.; Magliano, D.J.; Loh, V.H.Y.; Botton, J.; et al. Bisphenol A and the risk of cardiometabolic disorders: A systematic review with meta-analysis of the epidemiological evidence. Environ. Health 2015, 14, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, W.; Yang, J.; Liu, Y.; Bi, Y.; Wang, H. Association between Phthalate Metabolites and Risk of Endometriosis: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3678. [Google Scholar] [CrossRef] [Green Version]
- Yan, D.; Zhang, Y.; Liu, L.; Yan, H. Pesticide exposure and risk of Alzheimer’s disease: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Belbasis, L.; Bellou, V.; Evangelou, E. Environmental Risk Factors and Amyotrophic Lateral Sclerosis: An Umbrella Review and Critical Assessment of Current Evidence from Systematic Reviews and Meta-Analyses of Observational Studies. Neuroepidemiology 2016, 46, 96–105. [Google Scholar] [CrossRef]
- Van Maele-Fabry, G.; Gamet-Payrastre, L.; Lison, D. Residential exposure to pesticides as risk factor for childhood and young adult brain tumors: A systematic review and meta-analysis. Environ. Int. 2017, 106, 69–90. [Google Scholar] [CrossRef] [Green Version]
- Jin, J.; Yu, M.; Hu, C.; Ye, L.; Xie, L. Pesticide Exposure as a Risk Factor for Myelodysplastic Syndromes: A Meta-Analysis Based on 1,942 Cases and 5,359 Controls. PLoS ONE 2014, 9. [Google Scholar] [CrossRef]
- Yan, D.; Zhang, Y.; Liu, L.; Shi, N.; Yan, H. Pesticide exposure and risk of Parkinson’s disease: Dose-response meta-analysis of observational studies. Regul. Toxicol. Pharmacol. 2018, 96, 57–63. [Google Scholar] [CrossRef]
- Tangamornsuksan, W.; Lohitnavy, O.; Sruamsiri, R.; Chaiyakunapruk, N.; Norman Scholfield, C.; Reisfeld, B.; Lohitnavy, M. Paraquat exposure and Parkinson’s disease: A systematic review and meta-analysis. Arch. Environ. Occup. Health 2019, 74, 225–238. [Google Scholar] [CrossRef]
- Hu, L.; Luo, D.; Zhou, T.; Tao, Y.; Feng, J.; Mei, S. The association between non-Hodgkin lymphoma and organophosphate pesticides exposure: A meta-analysis. Environ. Pollut. 2017, 231, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Luo, D.; Zhou, T.; Tao, Y.; Feng, Y.; Shen, X.; Mei, S. Exposure to organochlorine pesticides and non-Hodgkin lymphoma: A meta-analysis of observational studies. Sci. Rep. 2016, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Maele-Fabry, G.; Gamet-Payrastre, L.; Lison, D. Household exposure to pesticides and risk of leukemia in children and adolescents: Updated systematic review and meta-analysis. Int. J. Hyg. Environ. Health 2019, 222, 49–67. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.; Barg, F.K.; Emmett, E.A.; Wiebe, D.J.; Hwang, W.-T. Association between mesothelioma and non-occupational asbestos exposure: Systematic review and meta-analysis. Environ. Health 2018, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nawrot, T.S.; Martens, D.S.; Hara, A.; Plusquin, M.; Vangronsveld, J.; Roels, H.A.; Staessen, J.A. Association of total cancer and lung cancer with environmental exposure to cadmium: The meta-analytical evidence. Cancer Causes Control 2015, 26, 1281–1288. [Google Scholar] [CrossRef]
- Ma, J.; Yan, L.; Guo, T.; Yang, S.; Guo, C.; Liu, Y.; Xie, Q.; Wang, J. Association of typical toxic heavy metals with schizophrenia. Int. J. Environ. Res. Public Health 2019, 16, 4200. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Xie, Z.; Lin, Y.; Zhang, D. Association of inorganic arsenic exposure with type 2 diabetes mellitus: A meta-analysis. J. Epidemiol. Community Health 2014, 68, 176–184. [Google Scholar] [CrossRef]
- Meng, E.; Mao, Y.; Yao, Q.; Han, X.; Li, X.; Zhang, K.; Jin, W. Population-based study of environmental/occupational lead exposure and amyotrophic lateral sclerosis: A systematic review and meta-analysis. Neurol. Sci. 2020, 41, 35–41. [Google Scholar] [CrossRef]
- Lanphear, B.P.; Hornung, R.; Khoury, J.; Yolton, K.; Baghurst, P.; Bellinger, D.C.; Canfield, R.L.; Dietrich, K.N.; Bornschein, R.; Greene, T.; et al. Low-Level Environmental Lead Exposure and Children’s Intellectual Function: An International Pooled Analysis. Environ. Health Perspect. 2005, 113, 894–899. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, H.; Gasparrini, A.; Armstrong, B.; Honda, Y.; Chung, Y.; Ng, C.F.S.; Tobias, A.; Íñiguez, C.; Lavigne, E.; et al. Suicide and Ambient Temperature: A Multi-Country Multi-City Study. Environ. Health Perspect. 2019, 127, 117007. [Google Scholar] [CrossRef]
- Yang, J.; Yin, P.; Zhou, M.; Ou, C.Q.; Li, M.; Liu, Y.; Gao, J.; Chen, B.; Liu, J.; Bai, L.; et al. The effect of ambient temperature on diabetes mortality in China: A multi-city time series study. Sci. Total Environ. 2016, 543, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Vickers, M.L.; Pelecanos, A.; Tran, M.; Eriksson, L.; Assoum, M.; Harris, P.N.; Jaiprakash, A.; Parkinson, B.; Dulhunty, J.; Crawford, R.W. Association between higher ambient temperature and orthopaedic infection rates: A systematic review and meta-analysis. ANZ J. Surg. 2019, 89, 1028–1034. [Google Scholar] [CrossRef] [PubMed]
- Chersich, M.F.; Pham, M.D.; Areal, A.; Haghighi, M.M.; Manyuchi, A.; Swift, C.P.; Wernecke, B.; Robinson, M.; Hetem, R.; Boeckmann, M.; et al. Associations between high temperatures in pregnancy and risk of preterm birth, low birth weight, and stillbirths: Systematic review and meta-analysis. BMJ 2020, 371, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Bell, M.L.; Gasparrini, A.; Armstrong, B.G.; Sera, F.; Hwang, S.; Lavigne, E.; Zanobetti, A.; Coelho, M.d.S.Z.S.; Saldiva, P.H.N.; et al. Mortality burden of diurnal temperature range and its temporal changes: A multi-country study. Environ. Int. 2018, 110, 123–130. [Google Scholar] [CrossRef]
- Cheng, J.; Xu, Z.; Bambrick, H.; Prescott, V.; Wang, N.; Zhang, Y.; Su, H.; Tong, S.; Hu, W. Cardiorespiratory effects of heatwaves: A systematic review and meta-analysis of global epidemiological evidence. Environ. Res. 2019, 177, 108610. [Google Scholar] [CrossRef] [PubMed]
- Bunker, A.; Wildenhain, J.; Vandenbergh, A.; Henschke, N.; Rocklöv, J.; Hajat, S.; Sauerborn, R. Effects of Air Temperature on Climate-Sensitive Mortality and Morbidity Outcomes in the Elderly; a Systematic Review and Meta-analysis of Epidemiological Evidence. EBioMedicine 2016, 6, 258–268. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Zhou, M.; Yang, J.; Yin, P.; Wang, B.; Ou, C.Q.; Liu, Q. The modifying effects of heat and cold wave characteristics on cardiovascular mortality in 31 major Chinese cities. Environ. Res. Lett. 2020, 15. [Google Scholar] [CrossRef]
- Cong, X.; Xu, X.; Zhang, Y.; Wang, Q.; Xu, L.; Huo, X. Temperature drop and the risk of asthma: A systematic review and meta-analysis. Environ. Sci. Pollut. Res. 2017, 24, 22535–22546. [Google Scholar] [CrossRef]
- Ho, C.-L.; Wu, W.-F.; Liou, Y.M. Dose-Response Relationship of Outdoor Exposure and Myopia Indicators: A Systematic Review and Meta-Analysis of Various Research Methods. Int. J. Environ. Res. Public Health 2019, 16, 2595. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.S.; Deng, Q.; Fan, W.Y.; Wang, W.Y.; Wang, X. Light exposure at night, sleep duration, melatonin, and breast cancer: A dose-response analysis of observational studies. Eur. J. Cancer Prev. 2014, 23, 269–276. [Google Scholar] [CrossRef]
- Monnereau, A.; Glaser, S.L.; Schupp, C.W.; Smedby, K.E.; De Sanjosé, S.; Kane, E.; Melbye, M.; Forétova, L.; Maynadié, M.; Staines, A.; et al. Exposure to UV radiation and risk of Hodgkin lymphoma: A pooled analysis. Blood 2013, 122, 3492–3499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kricker, A.; Armstrong, B.K.; Hughes, A.M.; Goumas, C.; Smedby, K.E.; Zheng, T.; Spinelli, J.J.; De Sanjose, S.; Hartge, P.; Melbye, M.; et al. Personal sun exposure and risk of non Hodgkin lymphoma: A pooled analysis from the Interlymph Consortium. Int. J. Cancer 2008, 122, 144–154. [Google Scholar] [CrossRef]
- Zare Sakhvidi, M.J.; Zare Sakhvidi, F.; Mehrparvar, A.H.; Foraster, M.; Dadvand, P. Association between noise exposure and diabetes: A systematic review and meta-analysis. Environ. Res. 2018, 166, 647–657. [Google Scholar] [CrossRef]
- Fu, W.; Wang, C.; Zou, L.; Liu, Q.; Gan, Y.; Yan, S.; Song, F.; Wang, Z.; Lu, Z.; Cao, S. Association between exposure to noise and risk of hypertension: A meta-analysis of observational epidemiological studies. J. Hypertens. 2017, 35, 2358–2366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dzhambov, A.M.; Dimitrova, D.D. Residential road traffic noise as a risk factor for hypertension in adults: Systematic review and meta-analysis of analytic studies published in the period 2011–2017. Environ. Pollut. 2018, 240, 306–318. [Google Scholar] [CrossRef]
- Van Kempen, E.; Casas, M.; Pershagen, G.; Foraster, M. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Cardiovascular and Metabolic Effects: A Summary. Int. J. Environ. Res. Public Health 2018, 15, 379. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.; Kim, Y.; Honda, Y.; Kim, H. Association between diurnal temperature range and mortality modified by temperature in Japan, 1972–2015: Investigation of spatial and temporal patterns for 12 cause-specific deaths. Environ. Int. 2018, 119, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Angelillo, I.F.; Villari, P. Residential exposure to electromagnetic fields and childhood leukaemia: A meta-analysis. Bull. World Health Organ. 1999, 77, 906–915. [Google Scholar] [PubMed]
- Malinovsky, G.; Yarmoshenko, I.; Vasilyev, A. Meta-analysis of case-control studies on the relationship between lung cancer and indoor radon exposure. Radiat. Environ. Biophys. 2019, 58, 39–47. [Google Scholar] [CrossRef]
- Tong, J.; Qin, L.; Cao, Y.; Li, J.; Zhang, J.; Nie, J.; An, Y. Environmental radon exposure and childhood leukemia. J. Toxicol. Environ. Health Part B Crit. Rev. 2012, 15, 332–347. [Google Scholar] [CrossRef]
- Rojas-Rueda, D.; Nieuwenhuijsen, M.J.; Gascon, M.; Perez-Leon, D.; Mudu, P.; Rojas-Rueda, D.; Nieuwenhuijsen, M.J.; Gascon, M.; Perez-Leon, D.; Mudu, P. Green spaces and mortality: A systematic review and meta-analysis of cohort studies. Lancet Planet. Health 2019, 3, e469–e477. [Google Scholar] [CrossRef] [Green Version]
- Zhan, Y.; Liu, J.; Lu, Z.; Yue, H.; Zhang, J.; Jiang, Y. Influence of residential greenness on adverse pregnancy outcomes: A systematic review and dose-response meta-analysis. Sci. Total Environ. 2020, 718, 37420. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Lin, F.; Wang, B.; Cao, Y.; Hou, X.; Wang, Y. Residential Proximity to Major Roadways and Risk of Type 2 Diabetes Mellitus: A Meta-Analysis. Int. J. Environ. Res. Public Health 2017, 14, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boothe, V.L.; Boehmer, T.K.; Wendel, A.M.; Yip, F.Y. Residential traffic exposure and childhood leukemia: A systematic review and meta-analysis. Am. J. Prev. Med. 2014, 46, 413–422. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.K.; Hsu, Y.T.; Brown, K.D.; Pokharel, B.; Wei, Y.; Chen, S.T. Residential exposure to petrochemical industrial complexes and the risk of leukemia: A systematic review and exposure-response meta-analysis. Environ. Pollut. 2020, 258. [Google Scholar] [CrossRef]
- Belbasis, L.; Köhler, C.A.; Stefanis, N.; Stubbs, B.; van Os, J.; Vieta, E.; Seeman, M.V.; Arango, C.; Carvalho, A.F.; Evangelou, E. Risk factors and peripheral biomarkers for schizophrenia spectrum disorders: An umbrella review of meta-analyses. Acta Psychiatr. Scand. 2018, 137, 88–97. [Google Scholar] [CrossRef]
- Piovani, D.; Danese, S.; Peyrin-biroulet, L.; Nikolopoulos, G.K.; Lytras, T.; Bonovas, S. Environmental Risk Factors for Inflammatory Bowel Diseases: An Umbrella Review of Meta-analyses. Gastroenterology 2019, 157, 647–659. [Google Scholar] [CrossRef] [Green Version]
- Tusting, L.S.; Ippolito, M.M.; Willey, B.A.; Kleinschmidt, I.; Dorsey, G.; Gosling, R.D.; Lindsay, S.W. The evidence for improving housing to reduce malaria: A systematic review and meta-analysis. Malar. J. 2015, 14. [Google Scholar] [CrossRef] [Green Version]
- Orsi, L.; Magnani, C.; Petridou, E.T.; Dockerty, J.D.; Metayer, C.; Milne, E.; Bailey, H.D.; Dessypris, N.; Kang, A.Y.; Wesseling, C.; et al. Living on a farm, contact with farm animals and pets, and childhood acute lymphoblastic leukemia: Pooled and meta-analyses from the Childhood Leukemia International Consortium. Cancer Med. 2018, 7, 2665–2681. [Google Scholar] [CrossRef]


{kind=link}
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure Temporality | Study Design | Population | Health Outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PM2.5 | per 1 mcg/m3 | Long-term | Cohort | Adults, both sexes | Alzheimer’s disease | 3 | [9] | 2019 | 86 | 0 | HR | 4.82 | 2.28 | 7.36 | Moderate |
| per 10 mcg/m3 | All-cause mortality | 13 | [10]. | 2013 | 65 | 0.001 | RR | 1.06 | 1.04 | 1.08 | Moderate | ||||
| Cardiovascular mortality | 17 | [11] | 2014 | 98 | NR | RR | 1.19 | 1.09 | 1.31 | Low | |||||
| Chronic kidney disease | 4 | [5] | 2020 | 82 | 0.001 | RR | 1.10 | 1.00 | 1.21 | Low | |||||
| Chronic Obstructive Pulmonary Disease | 4 | [8] | 2014 | NR | NR | IRF | F | F | F | Low | |||||
| Dementia | 4 | [9] | 2019 | 97 | 0 | HR | 3.26 | 1.20 | 5.31 | Moderate | |||||
| Depression | 5 | [12] | 2019 | 0 | 0.97 | OR | 1.10 | 1.02 | 1.19 | Moderate | |||||
| Ischemic heart disease mortality | 16 | [8] | 2014 | NR | NR | IRF | F | F | F | Low | |||||
| Lung cancer mortality | 49 | [8] | 2014 | NR | NR | IRF | F | F | F | Low | |||||
| Liver cancer mortality | 2 | [7] | 2018 | 67 | NR | RR | 1.29 | 1.06 | 1.58 | Low | |||||
| Colorectal cancer mortality | 2 | [7] | 2018 | 97 | NR | RR | 1.08 | 1.00 | 1.17 | Low | |||||
| Cancer mortality | 19 | [7] | 2018 | 97 | <0.001 | RR | 1.17 | 1.11 | 1.24 | Moderate | |||||
| Natural mortality | 11 | [11] | 2014 | 87 | NR | RR | 1.05 | 1.01 | 1.01 | Low | |||||
| Respiratory mortality | 8 | [11] | 2014 | 61 | NR | RR | 1.05 | 1.01 | 1.09 | Low | |||||
| Stroke | 16 | [13] | 2019 | 77 | 0 | HR | 1.11 | 1.05 | 1.17 | Moderate | |||||
| Stroke mortality | 16 | [8] | 2014 | NR | NR | IRF | F | F | F | Low | |||||
| Type 2 diabetes | 10 | [6] | 2020 | 55 | 0.012 | RR | 1.11 | 1.03 | 1.19 | Low | |||||
| Parkinson’s disease | 8 | [14] | 2019 | 86 | <0.001 | RR | 1.06 | 0.99 | 1.14 | Moderate |
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure Temporality | Study Design | Population | Health Outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PM2.5 | per 10 mcg/m3 | Long-term | Cohort | Children | Asthma | 10 | [36] | 2017 | 28 | 0.18 | OR | 1.03 | 1.01 | 1.05 | Moderate |
| Autism spectrum disorder | 3 | [20] | 2016 | 0 | 0.54 | OR | 2.32 | 2.15 | 2.51 | Moderate | |||||
| Children (<5 years) | Acute low respiratory infections | 28 | [8] | 2014 | NR | NR | IRF | F | F | F | Low | ||||
| Pregnant women | Small for gestational age | 5 | [18] | 2019 | 51 | NR | OR | 1.01 | 1.00 | 1.03 | Low | ||||
| Autistic syndrome disorder | 9 | [17] | 2020 | 91 | <0.001 | RR | 1.06 | 1.01 | 1.11 | Moderate | |||||
| per 10 mcg/m3 | Short-term | Case-crossover | Adults, both sexes | Out-of-hospital cardiac arrest | 12 | [21] | 2017 | 70 | NR | RR | 1.04 | 1.01 | 1.07 | Low | |
| Time-series | Adults, both sexes | Cardiac arrhythmia | 17 | [22] | 2016 | 78 | NR | RR | 1.15 | 1.01 | 1.03 | Low | |||
| Daily cardiovascular mortality | 652 | [23] | 2019 | NR | NR | RR | 1.36 | 1.30 | 1.43 | Low | |||||
| Daily mortality | 652 | [23] | 2019 | NR | NR | RR | 1.68 | 1.59 | 1.77 | Low | |||||
| Daily respiratory mortality | 652 | [23] | 2019 | NR | NR | RR | 1.47 | 1.35 | 1.58 | Low | |||||
| Children (<18 years) | Pneumonia | 11 | [24] | 2017 | 38 | 0.08 | RR | 1.02 | 1.01 | 1.03 | Moderate |
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure Temporality | Study Design | Population | Health Outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PM10 | per 2 mcg/m3 | Long-term | Cohort | Adults, both sexes | Chronic kidney disease | 4 | [5] | 2020 | 81 | 0.001 | RR | 1.16 | 1.05 | 1.29 | Low |
| per 10 mcg/m3 | Type 2 diabetes | 6 | [6] | 2020 | 68 | 0.004 | RR | 1.12 | 1.01 | 1.23 | Moderate | ||||
| Incidence of coronary events | 11 | [15] | 2014 | 0 | 0.81 | HR | 1.12 | 1.01 | 1.25 | Moderate | |||||
| Lung cancer mortality | 9 | [7] | 2018 | 93 | NR | RR | 1.07 | 1.03 | 1.11 | Low | |||||
| Cancer mortality | 12 | [7] | 2018 | 91 | <0.001 | RR | 1.09 | 1.04 | 1.14 | Moderate | |||||
| Incidence of chronic bronchitis | 3 | [16] | 2015 | NR | NR | RR | 1.11 | 1.04 | 1.18 | Low | |||||
| Children | Asthma | 12 | [36] | 2017 | 29 | 0.16 | OR | 1.05 | 1.02 | 1.08 | Moderate | ||||
| Pregnant women | Low birth weight | 11 | [18] | 2019 | 73 | NR | OR | 1.06 | 1.02 | 1.09 | Low | ||||
| Preterm birth | 8 | [18] | 2019 | 81 | NR | OR | 1.05 | 1.02 | 1.07 | Low | |||||
| Case-control | Children | Autism spectrum disorder | 6 | [20] | 2016 | 2 | 0.41 | OR | 1.07 | 1.06 | 1.08 | Moderate | |||
| Short-term | Case-crossover | Adults, both sexes | Out-of-hospital cardiac arrest | 9 | [21] | 2017 | 78 | NR | RR | 1.02 | 1.01 | 1.04 | Low | ||
| Time-series | Adults, both sexes | Cardiac arrhythmia | 12 | [22] | 2016 | 79 | NR | RR | 1.01 | 1 | 1.02 | Low | |||
| Daily cardiovascular mortality | 652 | [23] | 2019 | NR | NR | RR | 1.55 | 1.45 | 1.66 | Low | |||||
| Daily mortality | 652 | [23] | 2019 | NR | NR | RR | 1.44 | 1.39 | 1.5 | Low | |||||
| Daily respiratory mortality | 652 | [23] | 2019 | NR | NR | RR | 1.74 | 1.53 | 1.95 | Low | |||||
| per 20 mcg/m3 | Suicide | 7 | [12] | 2019 | 42 | 0.15 | RR | 1.02 | 1 | 1.03 | Moderate | ||||
| Children (<18 years) | Pneumonia | 10 | [24] | 2017 | 66 | 0 | RR | 1.02 | 1.01 | 1.02 | Moderate | ||||
| Desert dust | per 10 mcg/m3 | Short-term | Time-series | Adults, both sexes | Cardiovascular mortality | 11 | [25] | 2016 | 0 | 0.77 | IR | 1.01 | 1 | 1.02 | Moderate |
| Mortality | 11 | [25] | 2016 | 0 | 0.75 | IR | 1.01 | 1 | 1.01 | Moderate | |||||
| Black carbon | per 0.5 × 10−5 M−1 | Long-term | Cohort | Children | Asthma | 8 | [36] | 2017 | 0 | 0.87 | OR | 1.08 | 1.03 | 1.14 | Moderate |
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure Temporality | Study Design | Population | Health Outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NO2 | per 4 mcg/m3 | Long-term | Cohort | Adults, both sexes | Autistic syndrome disorder | 7 | [17] | 2020 | 58 | 0.007 | RR | 1.02 | 1.01 | 1.04 | Low |
| per 10 mcg/m3 | Cancer mortality | 16 | [7] | 2018 | 95 | 0.003 | RR | 1.06 | 1.02 | 1.10 | Low | ||||
| Cardiovascular mortality | 18 | [11] | 2014 | 98 | NR | RR | 1.13 | 1.08 | 1.18 | Low | |||||
| Chronic kidney disease | 3 | [5] | 2020 | 0 | 0.47 | RR | 1.11 | 1.09 | 1.14 | Moderate | |||||
| All-cause mortality | 12 | [11] | 2014 | 89 | NR | RR | 1.04 | 1.01 | 1.06 | Low | |||||
| Respiratory mortality | 9 | [11] | 2014 | 0 | NR | RR | 1.02 | 1.02 | 1.03 | Moderate | |||||
| Type 2 diabetes | 6 | [26] | 2018 | 46 | <0.001 | RR | 1.11 | 1.07 | 1.16 | High | |||||
| Cancer mortality | 16 | [7] | 2018 | 95 | 0.003 | RR | 1.06 | 1.02 | 1.10 | Moderate | |||||
| Children | Asthma | 20 | [36] | 2017 | 65 | <0.001 | OR | 1.05 | 1.02 | 1.07 | Moderate | ||||
| Pregnant women | Low birth weight | 11 | [18] | 2019 | 32 | NR | OR | 1.02 | 1.00 | 1.04 | Moderate | ||||
| Small for gestational age | 5 | [18] | 2019 | 87 | NR | OR | 1.02 | 1.01 | 1.03 | Low | |||||
| per 10 mcg/m3 | Short-term | Time-series | Adults | Natural mortality | 30 | [16] | 2015 | NR | NR | RR | 1.002 | 1.002 | 1.004 | Low | |
| per 10 ppb | Case-crossover | Adults, both sexes | Out-of-hospital cardiac arrest | 11 | [21] | 2017 | 66 | NR | RR | 1.02 | 1.00 | 1.03 | Low | ||
| Time-series | Adults, both sexes | Cardiac arrhythmia | 13 | [22] | 2016 | 93 | NR | RR | 1.04 | 1.01 | 1.05 | Low | |||
| Conjunctivitis | 12 | [27] | 2019 | NR | NR | RR | 1.02 | 1.01 | 1.04 | Low | |||||
| per 20 ppb | Depression | 7 | [28] | 2020 | 65 | 0.008 | RE | 1.02 | 1.00 | 1.04 | Low | ||||
| Children (<18 years) | Pneumonia | 10 | [24] | 2017 | 71 | 0 | RR | 1.01 | 1.00 | 1.02 | Moderate | ||||
| NOx | per 20 ppb | Long-term | Cohort | Pregnant women | Low birth weight | 3 | [18] | 2019 | 58 | NR | OR | 1.03 | 1.01 | 1.05 | Low |
| Preterm birth | 5 | [18] | 2019 | 88 | NR | OR | 1.02 | 1.01 | 1.03 | Low |
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure Temporality | Study Design | Population | Health Outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| O3 | per 5 ppb | Long-term | Cohort | Adults, both sexes | Ischemic heart disease mortality | 4 | [29] | 2016 | 67 | 0.02 | RR | 1.02 | 1 | 1.04 | Low |
| per 10 mcg/m3 | Pregnant women | Preterm birth | 3 | [18] | 2019 | 0 | NR | OR | 1.04 | 1 | 1.07 | Moderate | |||
| per 10 ppb | Cohort and Case-Control | Adults, both sexes | Parkinson’s disease | 5 | [14] | 2019 | 0 | 0.69 | RR | 1.01 | 1 | 1.02 | Moderate | ||
| Short-term | Case-crossover | Adults, both sexes | Out-of-hospital cardiac arrest | 11 | [21] | 2017 | 53 | NR | RR | 1.02 | 1.01 | 1.02 | Low | ||
| per 20 ppb | Time-series | Children (<18 years) | Pneumonia | 12 | [24] | 2017 | 75 | 0 | RR | 1.02 | 1.01 | 1.03 | Moderate | ||
| per 10 mcg/m3 | Adults | All-cause mortality | 32 | [16] | 2015 | NR | NR | RR | 1.003 | 1.001 | 1.004 | Low | |||
| Cardiovascular and respiratory mortality | 32 | [16] | 2015 | NR | NR | RR | 1.005 | 1.001 | 1.009 | Low | |||||
| SO2 | per 5 ppb | 1st pregnancy trimester | Cohort | Pregnant women | Gestational diabetes mellitus | 5 | [30] | 2020 | 93 | 0 | OR | 1.39 | 1.01 | 1.77 | Moderate |
| per 10 mcg/m3 | Long-term | Cohort | Pregnant women | Low birth weight | 5 | [18] | 2019 | 98 | NR | OR | 1.21 | 1.08 | 1.35 | Low | |
| per 10 ppb | Short-term | Time-series | Adults, both sexes | Cardiac arrhythmia | 10 | [22] | 2016 | 77 | NR | RR | 1.02 | 1 | 1.04 | Low | |
| Children (<18 years) | Pneumonia | 8 | [24] | 2017 | 48 | 0.04 | RR | 1.03 | 1 | 1.05 | Moderate | ||||
| CO | per 1 mcg/m3 | Long-term | Cohort | Pregnant women | Preterm birth | 7 | [18] | 2019 | 89 | NR | OR | 1.06 | 1.04 | 1.08 | Low |
| per 1 ppm | Short-term | Case-crossover | Adults, both sexes | Out-of-hospital cardiac arrest | 11 | [21] | 2017 | 44 | NR | RR | 1.06 | 1 | 1.14 | Moderate | |
| Time-series | Adults, both sexes | Cardiac arrhythmia | 12 | [22] | 2016 | 90 | NR | RR | 1.04 | 1.02 | 1.06 | Low | |||
| per 1000 ppb | Children (<18 years) | Pneumonia | 7 | [24] | 2017 | 68 | 0.004 | RR | 1.01 | 1 | 1.02 | Low |
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure Temporality | Study Design | Population | Health Outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Household air pollution | Exposed vs. not exposed | Long-term | Case-controls | Adults, both sexes | Cervical cancer | 4 | [31] | 2015 | NR | 0.45 | OR | 6.46 | 3.12 | 13.36 | Low |
| Laryngeal cancer | 5 | [31] | 2015 | NR | 0.49 | OR | 2.35 | 1.72 | 3.21 | Low | |||||
| Nasopharyngeal cancer | 6 | [31] | 2015 | NR | 0.06 | OR | 1.8 | 1.42 | 2.29 | Low | |||||
| Oral cancer | 4 | [31] | 2015 | NR | 0.93 | OR | 2.44 | 1.87 | 3.19 | Low | |||||
| Pharyngeal cancer | 4 | [31] | 2015 | NR | 0.99 | OR | 3.56 | 2.22 | 5.7 | Low | |||||
| Indoor air pollution from solid fuel | Exposed vs. not exposed | Long-term | Cohort | Adults, both sexes | Hypertension | 11 | [32] | 2020 | 90 | 0 | OR | 1.52 | 1.26 | 1.85 | Moderate |
| Solid fuel use | Exposed vs. not exposed | Long-term | Cohort | Pregnant women | Low birth weight | 12 | [33] | 2014 | 28 | 0.07 | OR | 1.35 | 1.23 | 1.48 | Moderate |
| Stillbirth | 5 | [33] | 2014 | 0 | 0.44 | OR | 1.29 | 1.18 | 1.41 | Moderate | |||||
| Preterm birth | 3 | [33] | 2014 | 0 | 0.39 | OR | 1.30 | 1.06 | 1.59 | Moderate | |||||
| Intrauterine growth retardation | 2 | [33] | 2014 | 0 | 0.89 | OR | 1.23 | 1.01 | 1.49 | Moderate | |||||
| Biomass burning | Exposed vs. not exposed | Long-term | Case-controls | Adults, both sexes | Esophageal squamous cell carcinoma | 16 | [34] | 2019 | 79 | NR | OR | 3.02 | 2.22 | 4.11 | Low |
| Cohort and Case-Control | Adults, both sexes | Chronic Obstructive Pulmonary Disease | 8 | [35] | 2017 | 93 | <0.001 | OR | 2.21 | 1.3 | 3.76 | Moderate |
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure Temporality | Study Design | Population | Health Outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Environmental tobacco smoke | Exposed vs. not exposed | Long-term | Cohort | Adults, both sexes | Stroke | 23 | [39] | 2017 | NR | NR | RR | 1.15 | 1.06 | 1.24 | Low |
| Cohort and Case-Control | Women | Lung cancer | 41 | [40] | 2018 | NR | <0.05 | RR | 1.33 | 1.17 | 1.51 | Low | |||
| Pregnant women | Low birth weight | 10 | [37] | 2008 | 54 | 0.009 | OR | 1.32 | 1.07 | 1.63 | Moderate | ||||
| Small for gestational age | 9 | [37] | 2008 | 0 | 0.004 | OR | 1.21 | 1.06 | 1.37 | Moderate | |||||
| Parental smoking | Exposed vs. not exposed | Long-term | Cohort | Children | Childhood obesity | 6 | [52] | 2014 | 0 | NR | RR | 1.33 | 1.23 | 1.44 | Moderate |
| Paternal smoking | Exposed vs. not exposed | Long-term | Case-controls | Children | Acute myeloid leukemia | 17 | [54] | 2019 | 0.5 | 0.003 | OR | 1.15 | 1.038 | 1.275 | Moderate |
| Exposed vs. not exposed | Long-term | Case-controls | Children | Acute lymphoblastic leukemia | 10 | [55] | 2012 | 28 | 0.18 | OR | 1.15 | 1.06 | 1.24 | Moderate | |
| Maternal smoking | Exposed vs. not exposed | Long-term | Case-controls | Children | Neuroblastoma | 14 | [53] | 2019 | 17 | NR | OR | 1.1 | 1.0 | 1.3 | Moderate |
| Passive smoking | Exposed vs. not exposed | Long-term | Case-controls | Adults, both sexes | Lung adenocarcinoma | 18 | [44] | 2014 | NR | 0.26 | OR | 1.35 | 1.23 | 1.48 | Low |
| Lung cancer | 18 | [44] | 2014 | NR | 0.01 | OR | 1.34 | 1.24 | 1.45 | Low | |||||
| Lung large cell cancer | 18 | [44] | 2014 | NR | 0.68 | OR | 1.36 | 1.04 | 1.79 | Low | |||||
| Lung small cell cancer | 18 | [44] | 2014 | NR | 0.98 | OR | 1.63 | 1.31 | 2.04 | Low | |||||
| Lung squamous cell carcinoma | 18 | [44] | 2014 | NR | 0.06 | OR | 1.36 | 1.17 | 1.58 | Low | |||||
| Pregnant women | Neural tube defects | 11 | [46] | 2018 | 50 | 0.02 | OR | 1.90 | 1.56 | 2.31 | Low | ||||
| Cohort | Adults, both sexes | Cardiovascular disease | 38 | [42] | 2015 | 66 | 0 | RR | 1.23 | 1.16 | 1.31 | Moderate | |||
| All-cause mortality | 11 | [42] | 2015 | 69 | 0 | RR | 1.18 | 1.10 | 1.27 | Moderate | |||||
| Type 2 diabetes | 7 | [26] | 2018 | 31 | <0.001 | RR | 1.22 | 1.10 | 1.35 | High | |||||
| Cohort and Case-Control | Women | Breast cancer | 51 | [41] | 2014 | 75 | <0.001 | OR | 1.62 | 1.39 | 1.85 | Moderate | |||
| Cervical cancer | 14 | [43] | 2018 | 64 | 0 | OR | 1.70 | 1.40 | 2.07 | Moderate | |||||
| Cohort | Children | Asthma | 41 | [47] | 2020 | 86 | <0.01 | OR | 1.21 | 1.15 | 1.26 | Low | |||
| Otitis Media | 9 | [48] | 2014 | 80 | 0.04 | OR | 1.39 | 1.02 | 1.89 | Low | |||||
| Prenatal smoke | Exposed vs. not exposed | Long-term | Cohort | Pregnant women | Schizophrenia | 7 | [49] | 2020 | 71 | NR | OR | 1.29 | 1.10 | 1.51 | Low |
| Offspring depression | 4 | [50] | 2017 | 54 | 0.084 | OR | 1.20 | 1.08 | 1.34 | Low | |||||
| Cohort and Case-Control | Attention-deficit/hyperactivity disorder | 20 | [51] | 2017 | 79 | 0.000 | OR | 1.60 | 1.45 | 1.76 | Moderate |
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure Temporality | Study Design | Population | Health Outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1,3-Butadiene | High exposed vs. low exposed | Long-term | Case-controls | Children | Acute lymphoblastic leukemia | 2 | [56] | 2019 | 0 | 0 | RR | 1.31 | 1.11 | 1.54 | High |
| All leukemia | 2 | [56] | 2019 | 28 | 0.025 | RR | 1.45 | 1.08 | 1.95 | Moderate | |||||
| Bisphenol A | High exposed vs. low exposed | Long-term | Cohort | Adults, both sexes | Diabetes | 3 | [64] | 2015 | 0 | 0.55 | OR | 1.47 | 1.21 | 1.80 | Moderate |
| Obesity | 3 | [64] | 2015 | 0 | 0.44 | OR | 1.67 | 1.41 | 1.98 | Moderate | |||||
| Dioxins | High exposed vs. low exposed | Long-term | Cohort | Women | Endometriosis | 10 | [62] | 2019 | 72 | <0.01 | OR | 1.65 | 1.14 | 2.39 | Low |
| Hydrocarbon exposure | Exposed vs. not exposed | Long-term | Cohort and Case-Control | Adults, both sexes | Parkinson’s disease | 14 | [58] | 2016 | 28 | NR | OR | 1.36 | 1.13 | 1.63 | Moderate |
| Mono (2-ethyl-5-hydroxyhexyl) phthalate | High exposed vs. low exposed | Long-term | Cohort and Case-Control | Women | Endometriosis | 6 | [65] | 2019 | 44 | 0.11 | OR | 1.24 | 1.00 | 1.54 | Moderate |
| Organic solvents | Exposed vs. not exposed | Long-term | Cohort and Case-Control | Adults, both sexes | Multiple sclerosis | 15 | [59] | 2015 | 77 | 0.06 | RR | 1.54 | 1.03 | 2.29 | Low |
| Parkinson’s disease | 18 | [58] | 2016 | 43 | NR | OR | 1.22 | 1.01 | 1.47 | Moderate | |||||
| Polychlorinated biphenyls (PCBs) | High exposed vs. low exposed | Long-term | Cohort | Women | Endometriosis | 9 | [62] | 2019 | 78 | <0.01 | OR | 1.70 | 1.20 | 2.39 | Low |
| High exposed vs. low exposed | Long-term | Case-controls | Adults, both sexes | Non-Hodgkin Lymphoma | 7 | [61] | 2012 | NR | NR | OR | 1.43 | 1.31 | 1.55 | Low | |
| Polychlorinated biphenyls 153 | per log2 ng/L | Long-term | Cohort | Children | Bronchitis | 7 | [63] | 2014 | NR | 0.89 | RR | 1.06 | 1.01 | 1.12 | Low |
| Solvents | Exposed vs. not exposed | Long-term | Cohort and Case-Control | Adults, both sexes | Systemic sclerosis | 11 | [60] | 2018 | 55 | <0.001 | OR | 2.41 | 1.73 | 3.37 | Moderate |
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure Temporality | Study Design | Population | Health Outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pesticides | Exposed vs. not exposed | Long-term | Cohort and Case-Control | Adults, both sexes | Alzheimer’s disease | 7 | [66] | 2016 | 0 | 0.885 | OR | 1.34 | 1.08 | 1.67 | Moderate |
| High exposed vs. low exposed | Cohort and Case-Control | Adults, both sexes | Amyotrophic lateral sclerosis | 7 | [67] | 2016 | 41 | 0.16 | RR | 1.20 | 1.02 | 1.41 | Moderate | ||
| High exposed vs. low exposed | Case-controls | Children | Brian tumors | 18 | [68] | 2017 | 0 | NR | OR | 1.26 | 1.13 | 1.14 | Moderate | ||
| Exposed vs. not exposed | Case-controls | Adults, both sexes | Myelodysplastic Syndromes | 11 | [69] | 2014 | 80 | 0 | OR | 1.95 | 1.23 | 3.09 | Moderate | ||
| 10 years of exposure vs. no exposure | Cohort | Adults, both sexes | Parkinson’s disease | 10 | [70] | 2018 | 50 | 0.032 | OR | 1.11 | 1.05 | 1.18 | Low | ||
| Residential pesticide exposure | High exposed vs. low exposed | Long-term | Case-controls | Children | Acute lymphoblastic leukemia | 8 | [74] | 2019 | NR | NR | OR | 1.42 | 1.13 | 1.80 | Low |
| Acute myeloid leukemia | 5 | [74] | 2019 | NR | NR | OR | 1.90 | 1.35 | 2.67 | Low | |||||
| Childhood leukemia | 15 | [74] | 2019 | 73 | NR | OR | 1.57 | 1.27 | 1.95 | Low |
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure temporality | Study Design | Population | Health outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chlordane | High exposed vs. low exposed | Long-term | Case-controls | Adults, both sexes | non-Hodgkin lymphoma | 8 | [73] | 2016 | 17 | 0.29 | OR | 1.93 | 1.51 | 2.48 | Moderate |
| Diazinon | Exposed vs. not exposed | Long-term | Cohort and Case-Control | Adults, both sexes | non-Hodgkin lymphoma | 7 | [72] | 2017 | 0 | 0.668 | OR | 1.39 | 1.11 | 1.73 | Moderate |
| Dichlorodiphenyldichloroethylene (DDE) | High exposed vs. low exposed | Long-term | Case-controls | Adults, both sexes | non-Hodgkin lymphoma | 11 | [73] | 2016 | 0 | 0.94 | OR | 1.38 | 1.14 | 1.66 | Moderate |
| per log2 ng/L | Long-term | Cohort | Children | Bronchitis | 7 | [63] | 2014 | NR | 0.38 | RR | 1.05 | 1.00 | 1.11 | Low | |
| Hexachlorobenzene | High exposed vs. low exposed | Long-term | Case-controls | Adults, both sexes | non-Hodgkin lymphoma | 7 | [73] | 2016 | 0 | 0.64 | OR | 1.54 | 1.20 | 1.99 | Moderate |
| Hexachlorocyclohexane | High exposed vs. low exposed | Long-term | Case-controls | Adults, both sexes | non-Hodgkin lymphoma | 6 | [73] | 2016 | 34 | 0.17 | OR | 1.42 | 1.08 | 1.87 | Moderate |
| Organochlorine pesticides | High exposed vs. low exposed | Long-term | Case-controls | Adults, both sexes | non-Hodgkin lymphoma | 13 | [73] | 2016 | 12 | 0.253 | OR | 1.40 | 1.27 | 1.56 | Moderate |
| Cohort | Women | Endometriosis | 5 | [62] | 2019 | 65 | 0.02 | OR | 1.97 | 1.25 | 3.13 | Low | |||
| Organophosphate pesticides | Exposed vs. not exposed | Long-term | Cohort and Case-Control | Adults, both sexes | non-Hodgkin lymphoma | 10 | [72] | 2017 | 41 | 0.032 | OR | 1.22 | 1.04 | 1.43 | Moderate |
| Paraquat | Exposed vs. not exposed | Long-term | Case-controls | Adults, both sexes | Parkinson’s disease | 14 | [71] | 2019 | 31 | 0.126 | OR | 1.70 | 1.28 | 2.25 | Moderate |
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure Temporality | Study Design | Population | Health Outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ALUMINUM | Exposed vs. not exposed | Long-term | Cohort | Adults, both sexes | Dementia | 8 | [45] | 2017 | 6.2 | <0.001 | OR | 1.72 | 1.33 | 2.21 | High |
| Asbestos (non-occupational) | Exposed vs. not exposed | Long-term | Cohort and Case-Control | Adults, both sexes | Mesothelioma | 27 | [75] | 2018 | 99 | NR | RR | 5.33 | 2.53 | 11.23 | Low |
| Cadmium | High exposed vs. low exposed | Long-term | Case-controls | Adults, both sexes | Cancer | 3 | [76] | 2015 | 0 | 0.84 | RR | 1.22 | 1.13 | 1.31 | Moderate |
| Lung Cancer | 3 | [76] | 2015 | 0 | 0.41 | RR | 1.68 | 1.47 | 1.92 | Moderate | |||||
| Chromium | High exposed vs. low exposed | Long-term | Case-controls | Adults, both sexes | Schizophrenia | 7 | [77] | 2019 | >50 | <0.01 | SMD | 0.32 | 0.01 | 0.63 | Moderate |
| Inorganic arsenic | High exposed vs. low exposed | Long-term | Cohort | Adults, both sexes | Type 2 diabetes | 3 | [78] | 2014 | 39 | 0.18 | RR | 1.39 | 1.06 | 1.81 | Moderate |
| Lead | High exposed vs. low exposed | Long-term | Cohort and Case-Control | Adults, both sexes | Amyotrophic lateral sclerosis | 3 | [79] | 2020 | 51 | 0.01 | RR | 1.46 | 1.16 | 1.83 | Low |
| Blood levels in mg/L | Long term | Cohort | Children | Mild mental retardation | 7 | [80] | 2005 | NR | NR | OR | F | F | F | Low | |
| Silica exposure | Exposed vs. not exposed | Long-term | Cohort and Case-Control | Adults, both sexes | Systemic sclerosis | 16 | [60] | 2018 | 96 | 0.002 | OR | 2.96 | 1.65 | 5.29 | Low |
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure Temporality | Study Design | Population | Health Outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ambient temperature | Maximum suicide temperature 93rd percentile vs. minimum suicide temperature | Short-term | Time-series | Adults, both sexes | Suicide | 341 | [81] | 2019 | 3.3 | NR | RR | 1.33 | 1.30 | 1.36 | Moderate |
| Orthopedic procedures during warmer periods of the year | Short-term | Time-series | Adults, both sexes | Post-operative infection | 12 | [83] | 2019 | 65 | 0.001 | OR | 1.16 | 1.04 | 1.30 | Moderate | |
| High versus low temperatures | Short-term | Time-series | Pregnant women | Low birth weight | 9 | [84] | 2020 | NR | NR | OR | 1.07 | 1.05 | 1.16 | Low | |
| Stillbirth | 2 | [84] | 2020 | 27.8 | NR | OR | 3.39 | 2.33 | 4.96 | Moderate | |||||
| Cold | per 1 Celsius degree decrease | Short-term | Time-series | Children <12 years | Asthma | 13 | [89] | 2017 | NR | NR | OR | 1.07 | 1.01 | 1.12 | Low |
| Elderly | Cardiovascular disease mortality | 9 | [87] | 2016 | 98 | <0.0001 | RR | 1.01 | 1.00 | 1.00 | Moderate | ||||
| Cerebrovascular mortality | 3 | [87] | 2016 | 60 | 0.001 | RR | 1.01 | 1.00 | 1.01 | Low | |||||
| Intracerebral hemorrhage | 2 | [87] | 2016 | 0 | 0.39 | RR | 1.01 | 1.01 | 1.02 | Moderate | |||||
| Pneumonia | 5 | [87] | 2016 | 94 | <0.0001 | RR | 1.06 | 1.01 | 1.12 | Moderate | |||||
| Respiratory disease mortality | 8 | [87] | 2016 | 90 | <0.0001 | RR | 1.02 | 1.00 | 1.00 | Moderate | |||||
| 10th and 1st percentile vs. 25th percentile of temperature | Short-term | Time-series | Adults, both sexes | Diabetes mortality | 9 | [82] | 2016 | NR | NR | RR | 1.11 | 1.03 | 1.19 | Low | |
| Cold wave | Exposed vs. not exposed | Short-term | Time-series | Adults, both sexes | Cardiovascular mortality | 31 | [88] | 2020 | 84.3 | <0.001 | OR | 1.54 | 1.21 | 1.97 | Moderate |
| Diurnal temperature range | per 10 Celsius degrees | Short-term | Time-series | Adults, both sexes | Mortality | 308 | [98] | 2018 | NR | NR | RR | 1.03 | 1.02 | 1.03 | Low |
| Heat | 90th and the 99th percentile vs. 75th percentile of temperature | Short-term | Time-series | Adults, both sexes | Diabetes mortality | 9 | [82] | 2016 | NR | NR | RR | 1.20 | 1.12 | 1.3 | Low |
| per 1 Celsius degree increase | Short-term | Time-series | Elderly | Acute renal failure | 2 | [87] | 2016 | 16 | 0.27 | RR | 1.01 | 1.01 | 1.02 | Moderate | |
| Cardiovascular disease mortality | 15 | [87] | 2016 | 99 | <0.0001 | RR | 1.03 | 1.03 | 1.04 | Moderate | |||||
| Cerebrovascular mortality | 3 | [87] | 2016 | 72 | 0.03 | RR | 1.01 | 1.00 | 1.02 | Low | |||||
| Diabetes | 3 | [87] | 2016 | 25 | 0.26 | RR | 1.01 | 1.00 | 1.01 | Moderate | |||||
| Ischemic heart disease mortality | 3 | [87] | 2016 | 81 | 0.004 | RR | 1.01 | 1.00 | 1.03 | Low | |||||
| Respiratory disease | 11 | [87] | 2016 | 82 | <0.0001 | RR | 1.02 | 1.01 | 1.04 | Moderate | |||||
| Respiratory disease mortality | 9 | [87] | 2016 | 92 | <0.0001 | RR | 1.00 | 1.00 | 1.00 | Moderate | |||||
| Heatwave | Exposed vs. not exposed | Short-term | Time-series | Adults, both sexes | Cardiovascular mortality | 36 | [86] | 2019 | 99 | <0.01 | RE | 1.15 | 1.09 | 1.21 | Low |
| Respiratory mortality | 27 | [86] | 2019 | 97 | <0.01 | RE | 1.18 | 1.09 | 1.28 | Low | |||||
| Pregnant women | Preterm birth | 6 | [84] | 2020 | 44.7 | 0.11 | OR | 1.16 | 1.10 | 1.23 | Moderate |
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure Temporality | Study Design | Population | Health Outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Artificial light exposure at night | High exposed vs. low exposed | Long-term | Case-controls | Women | Breast cancer | 6 | [91] | 2014 | 1.9 | 0.4 | RR | 1.17 | 1.11 | 1.24 | Moderate |
| Outdoor light exposure | High exposed vs. low exposed | Long-term | Cohort | Children | Myopia | 4 | [90] | 2019 | 91 | 0.02 | OR | 0.57 | 0.35 | 0.92 | Low |
| Ultraviolet radiation | High exposed vs. low exposed | Long-term | Case-controls | Adults, both sexes | Epstein–Barr Virus positive Hodgkin lymphoma | 4 | [92] | 2013 | NR | 0.10 | OR | 0.59 | 0.36 | 0.96 | Low |
| Recreational sun exposure | High exposed vs. low exposed | Long-term | Case-controls | Adults, both sexes | Non-Hodgkin lymphoma | 4 | [93] | 2008 | NR | 0.001 | OR | 0.76 | 0.63 | 0.91 | Moderate |
| Extremely low-frequency electromagnetic fields | High exposed vs. low exposed | Long-term | Cohort and Case-Control | Adults, both sexes | Amyotrophic lateral sclerosis | 5 | [67] | 2016 | 58 | 0.34 | RR | 1.30 | 1.10 | 1.60 | Low |
| High vs. low current wiring configuration codes | Long-term | Cohort and Case-Control | Children | Childhood leukemia | 6 | [99] | 1999 | NR | NR | OR | 1.46 | 1.05 | 2.04 | Low | |
| Indoor radon | Exposed vs. not exposed | Long-term | Case-controls | Adults, both sexes | Lung cancer | 31 | [100] | 2019 | NR | NR | OR | 1.14 | 1.08 | 1.21 | Low |
| High exposed vs. low exposed | Long-term | Case-controls | Children | Leukemia | 7 | [101] | 2012 | 9 | 0.36 | OR | 1.37 | 1.02 | 1.82 | Moderate | |
| Noise | High exposed vs. low exposed | Long-term | Cohort | Adults, both sexes | Diabetes | 5 | [94] | 2018 | 31 | 0.18 | HR | 1.04 | 1.02 | 1.07 | Moderate |
| per 5 dB | Hypertension | 5 | [95] | 2017 | 51 | 0.086 | RR | 1.20 | 1.09 | 1.31 | Low | ||||
| Road traffic noise | per 5 dB | Long-term | Cohort | Adults, both sexes | Diabetes | 3 | [94] | 2018 | 33 | 0.222 | HR | 1.07 | 1.02 | 1.12 | Moderate |
| per 10 dB (Lden) | Ischemic heart disease | 7 | [97] | 2018 | NR | NR | RR | 1.08 | 1.01 | 1.15 | Low | ||||
| Men | Hypertension | 2 | [96] | 2018 | 0 | <0.001 | RR | 1.62 | 1.02 | 1.09 | High |
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure Temporality | Study Design | Population | Health Outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Petrochemical industrial complexes | Residence >8 km distance from petrochemical industrial complexes | Long-term | Cohort and Case-Control | Adults, both sexes | Acute myeloid leukemia | 7 | [106] | 2020 | 50 | 0.01 | RR | 1.61 | 1.12 | 2.31 | Low |
| Chronic lymphocytic leukemia | 7 | [106] | 2020 | 92 | 0.048 | RR | 1.85 | 1.01 | 6.42 | Low | |||||
| Leukemia | 13 | [106] | 2020 | 73 | 0.001 | RR | 1.36 | 1.14 | 1.62 | Low | |||||
| Proximity to major roadways | Exposed vs. not exposed | Long-term | Cohort | Adults, both sexes | Type 2 diabetes | 6 | [104] | 2017 | 36 | 0.025 | RR | 1.13 | 1.02 | 1.27 | Moderate |
| Residential traffic exposure | High exposed vs. low exposed | Long-term | Case-controls | Children | Childhood leukemia | 7 | [105] | 2014 | 57 | 0.02 | OR | 1.39 | 1.03 | 1.88 | Low |
| Residential greenness | per 0.1 NDVI within 300 m buffer from residence | Long-term | Cohort | Adults, both sexes | All-cause mortality | 9 | [102] | 2019 | 95 | <0.001 | HR | 0.96 | 0.94 | 0.97 | Low |
| Low birth weight | 10 | [103] | 2020 | 41 | <0.001 | RR | 0.98 | 0.97 | 0.99 | High | |||||
| per 0.1 NDVI within 500 m buffer from residence | Small for gestational age | 13 | [103] | 2020 | 59 | 0.037 | RR | 0.99 | 0.98 | 1.00 | Low |
| Environmental Risk Factor | Exposure Unit or Comparator | Exposure Temporality | Study Design | Population | Health Outcome | Studies Included | Reference | Year | I2 (%) | p-Value | Risk Estimate | Effect Size | LCI | UCI | Strength of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rural living | Exposed vs. not exposed | Long-term | Cohort and Case-Control | Adults, both sexes | Parkinson’s disease | 31 | [58] | 2016 | 78 | NR | OR | 1.32 | 1.18 | 1.48 | Low |
| Urban exposure during childhood | Rural exposure during childhood | Long-term | Case-controls | Adults, both sexes | Crohn’s disease | 12 | [108] | 2019 | 71 | 0 | OR | 1.45 | 1.14 | 1.85 | Moderate |
| Cohort and Case-Control | Adults, both sexes | Inflammatory bowel disease | 4 | [108] | 2019 | 71 | 0 | OR | 1.35 | 1.15 | 1.58 | Moderate | |||
| Urbanicity | Highest vs. lowest category | Long-term | Cohort | Adults, both sexes | Schizophrenia | 8 | [107] | 2018 | 99 | 0 | OR | 2.39 | 1.62 | 3.51 | Moderate |
| Modern housing | Exposed vs. not exposed | Long-term | Cohort | Adults, both sexes | Clinical malaria | 3 | [109] | 2015 | 67 | 0.05 | OR | 0.55 | 0.36 | 0.84 | Low |
| Pet in the first year of life | Exposed vs. not exposed | Long-term | Case-controls | Children | Acute lymphoblastic leukemia | 12 | [110] | 2018 | 39 | 0.08 | OR | 0.91 | 0.82 | 1.00 | Low |
| Pet | Exposed vs. not exposed | Long-term | Cohort and Case-Control | Adults, both sexes | Crohn’s disease | 14 | [108] | 2019 | 67 | 0 | OR | 0.77 | 0.59 | 0.94 | Moderate |
| Recommendations |
|---|
| Observational studies:< - Increase studies on protective environmental risk factors |
| - Increase studies on vulnerable and disadvantaged populations |
| - Provide international classification of diseases (ICD) codes as part of the definitions for health outcomes |
| - Use comparable exposure definitions for environmental risk factors - Support longitudinal study designs |
| Meta-analyses - Avoid combining cross-sectional studies with cohort or case-control studies in the meta-estimates |
| - Provide heterogeneity values (i.e., I2) |
| - Provide dose-response functions to support populational risk assessment, quantitative health impact assessments, and policy translation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojas-Rueda, D.; Morales-Zamora, E.; Alsufyani, W.A.; Herbst, C.H.; AlBalawi, S.M.; Alsukait, R.; Alomran, M. Environmental Risk Factors and Health: An Umbrella Review of Meta-Analyses. Int. J. Environ. Res. Public Health 2021, 18, 704. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020704
Rojas-Rueda D, Morales-Zamora E, Alsufyani WA, Herbst CH, AlBalawi SM, Alsukait R, Alomran M. Environmental Risk Factors and Health: An Umbrella Review of Meta-Analyses. International Journal of Environmental Research and Public Health. 2021; 18(2):704. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020704
Chicago/Turabian StyleRojas-Rueda, David, Emily Morales-Zamora, Wael Abdullah Alsufyani, Christopher H. Herbst, Salem M. AlBalawi, Reem Alsukait, and Mashael Alomran. 2021. "Environmental Risk Factors and Health: An Umbrella Review of Meta-Analyses" International Journal of Environmental Research and Public Health 18, no. 2: 704. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020704