Obesity Prevention within the Early Childhood Education and Care Setting: A Systematic Review of Dietary Behavior and Physical Activity Policies and Guidelines in High Income Countries

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Search Strategy
2.3. Selection of Guidelines
2.4. Data Extraction
2.5. Assessment of Methodological Quality
- (1)
- Scope and Purpose: this relates to the overall aim of the guideline, and the target population (2 items).
- (2)
- Stakeholder Involvement: focuses on the extent and reporting to which appropriate stakeholders and views of its intended users were considered during the development of guidelines (3 items).
- (3)
- Rigor of Development: relates to the processes used to gather and synthesize the evidenced used to formulate the recommendations (8 items).
- (4)
- Clarity of Presentation: deals with the language structure, and format of the guideline (2 items).
- (5)
- Applicability: relates to consideration of barriers and facilitators to implementation, strategies to improve uptake, and availability of resources to apply the guidelines (4 items).
- (6)
- Editorial Independence: this considers if the formulation of the guidelines are not being unduly biased by funding agencies, and reporting of competing interests (2 items).
2.6. Data Synthesis and Analysis
3. Results
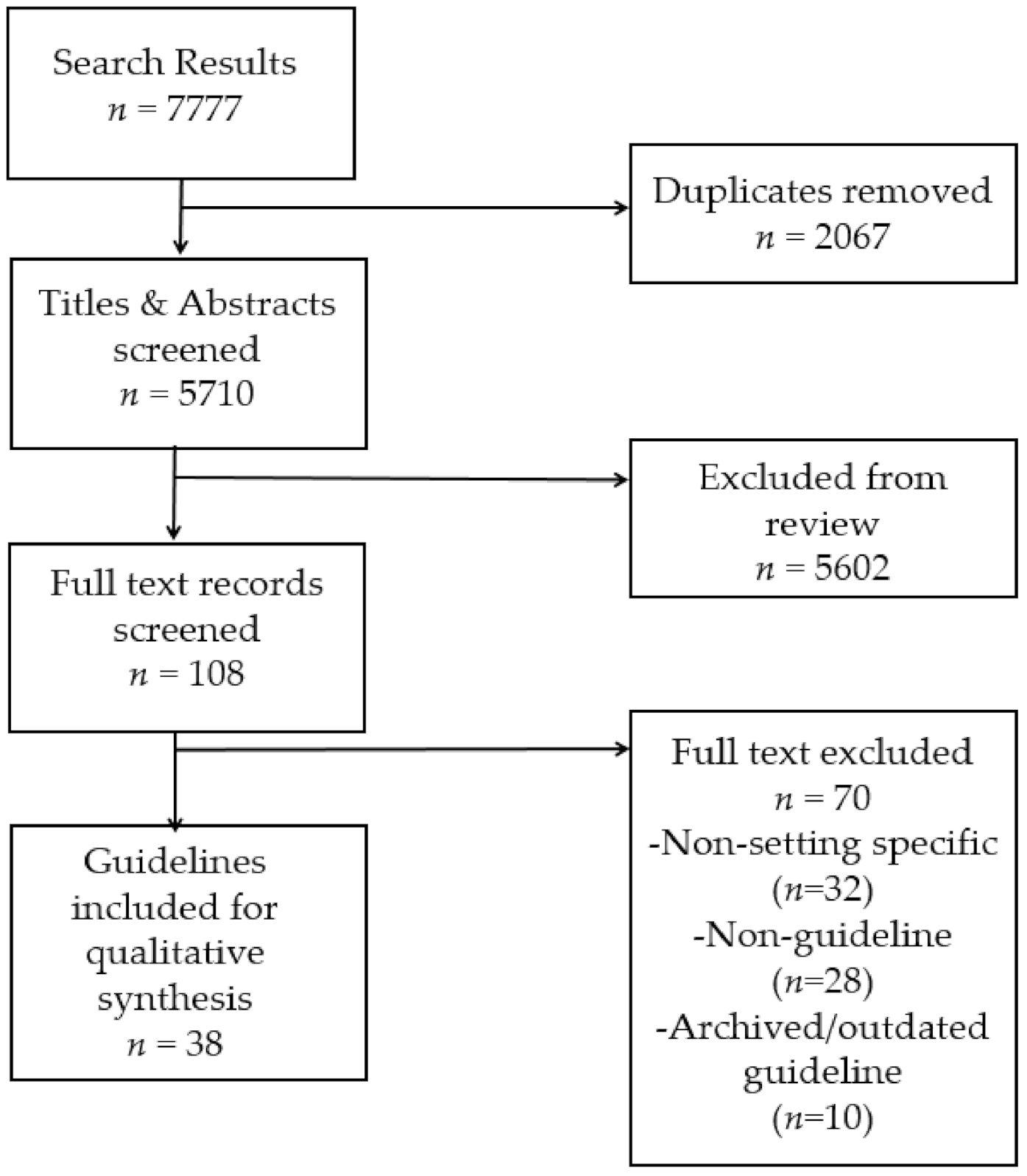
3.1. Guideline Selection
3.2. Guideline Characteristics
3.3. Quality of Guidelines
3.4. Dietary Behavior Policy and Practice Recommendations Grouped according to the ANGELO Framework
3.4.1. Dietary Behavior Recommendations addressing the Physical Environment
3.4.2. Dietary Behavior Recommendations Addressing the Sociocultural Environment
3.4.3. Dietary Behavior Recommendations Addressing the Policy Environment
3.5. Physical Activity Policy and Practice Recommendations Grouped According to the ANGELO Framework
3.5.1. Physical Activity Recommendations Addressing the Physical Environment
3.5.2. Physical Activity Recommendations Addressing the Sociocultural Environment
3.5.3. Physical Activity Recommendations Addressing the Policy Environment
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Commission on Ending Childhood Obesity. Facts and Figures on Childhood Obesity. 2017. Available online: https://www.who.int/end-childhood-obesity/facts/en/. (accessed on 6 September 2019).
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240. [Google Scholar] [CrossRef] [Green Version]
- Herman, K.M.; Cora, C.L.; Lise, G.; Katzmarzyk, P.T. Tracking of obesity and physical activity from childhood to adulthood: The Physical Activity Longitudinal Study. Int. J. Pediatric Obes. 2009, 4, 281–288. [Google Scholar] [CrossRef]
- World Health Organization. Population-Based Approaches to Childhood Obesity Prevention. 2012. Available online: https://www.who.int/dietphysicalactivity/childhood/WHO_new_childhoodobesity_PREVENTION_27nov_HR_PRINT_OK.pdf (accessed on 6 September 2019).
- Bakken, L.; Brown, N.; Downing, B. Early Childhood Education: The Long-Term Benefits. J. Res. Child. Educ. 2017, 31, 255–269. [Google Scholar] [CrossRef] [Green Version]
- Sheppard, M. Child Care in Australia: A Quick Guide; Parliament of Australia: Canberra, Australia, 2015. [Google Scholar]
- OECD-Social Policy Division—Directorate of Employment Labour and Soical Affairs. PF3.2: Enrolement in Childcare and Pre-School, in Public Policies for Families and Children; OECD Family Database: Paris, France, 2019; Available online: https://www.oecd.org/els/soc/PF3_2_Enrolment_childcare_preschool.pdf (accessed on 12 December 2019).
- Division of Nutrition Physical Activity and Obesity National Centre for Disease Control and Prevention and Health Promotion. Overweight & Obesity.Strategies to Prevent and Manage Obesity: Early Care and Education. 2020. Available online: https://www.cdc.gov/obesity/strategies/childcareece.html. (accessed on 9 October 2020).
- World Health Organization. Ottawa charter for health promotion. In Proceedings of the 1st International Conference on Health Promotion, Ottawa, ON, Canada, 21 November 1986. [Google Scholar]
- Stokols, D. Translating social ecological theory into guidelines for community health promotion. Am. J. Health Promot. 1996, 10, 282–298. [Google Scholar] [CrossRef] [Green Version]
- Swinburn, B.; Egger, G.; Raza, F. Dissecting obesogenic environments: The development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev. Med. 1999, 29, 563–570. [Google Scholar] [CrossRef]
- Browman, G.P.; Levine, M.N.; Mohide, E.A.; Hayward, R.S.; Pritchard, K.I.; Gafni, A.; Laupacis, A. The practice guidelines development cycle: A conceptual tool for practice guidelines development and implementation. J. Clin. Oncol. 1995, 13, 502–512. [Google Scholar] [CrossRef]
- Brennan, L.K.; Brownson, R.C.; Orleans, C.T. Childhood obesity policy research and practice: Evidence for policy and environmental strategies. Am. J. Prev. Med. 2014, 46, e1–e16. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Foltz, J.L.; May, A.L.; Belay, B.; Nihiser, A.J.; Dooyema, C.A.; Blanck, H.M. Population-level intervention strategies and examples for obesity prevention in children. Annu. Rev. Nutr. 2012, 32, 391–415. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Report of the Commission on Ending Childhood Obesity. Implementation Plan: Executive Summary. 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/259349/WHO-NMH-PND-ECHO-17.1-eng.pdf?sequence=1 (accessed on 6 September 2019).
- Ministry of Health. Sit Less. Move More, Sleep Well: Active Play Guidelines for Under-Fives; Ministry of Health: Wellington, New Zealand, 2017. [Google Scholar]
- Tremblay, M.S.; Warburton, D.E.R.; Janssen, I.; Paterson, D.H.; Latimer, A.E.; Rhodes, R.E.; Kho, M.E.; Hicks, A.; LeBlanc, A.G.; Zehr, L.; et al. New Canadian Physical Activity Guidelines. Appl. Physiol. Nutr. Metab. 2011, 36, 36–46. [Google Scholar] [CrossRef]
- Green, A.M.; Mihrshahi, S.; Innes-Hughes, C.; O’Hara, B.J.; McGill, B.; Rissel, C. Implementation of an Early Childhood Healthy Eating and Physical Activity Program in New South Wales, Australia: Munch & Move. Front. Public Health 2020, 8. [Google Scholar] [CrossRef]
- Neuman, M.J.; Okeng’o, L. Early childhood policies in low- and middle-income countries. Early Years 2019, 39, 223–228. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stok, F.M.; Renner, B.; Allan, J.; Boeing, H.; Ensenauer, R.; Issanchou, S.; Kiesswetter, E.; Lien, N.; Mazzocchi, M.; Monsivais, P.; et al. Dietary Behavior: An Interdisciplinary Conceptual Analysis and Taxonomy. Front. Psychol. 2018, 9, 1689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makanjana, O.; Naicker, A. Nutritional Status of Children 24–60 Months Attending Early Child Development Centres in a Semi-Rural Community in South Africa. Int. J. Environ. Res. Public Health 2021, 18, 261. [Google Scholar] [CrossRef] [PubMed]
- OCED Data. Average Wages. 2019. Available online: https://data.oecd.org/earnwage/average-wages.htm (accessed on 8 September 2020).
- Benjamin, S.E.; Ammerman, A.; Sommers, J.; Dodds, J.; Neelon, B.; Ward, D.S. Nutrition and physical activity self-assessment for child care (NAP SACC): Results from a pilot intervention. J. Nutr. Educ. Behav. 2007, 39, 142–149. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children Under 5 Years of Age: Web Annex: Evidence Profiles; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E. AGREE II: Advancing guideline development, reporting and evaluation in health care. CMAJ 2010, 182, E839–E842. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann-Eßer, W.; Siering, U.; Neugebauer, E.A.M.; Brockhaus, A.C.; McGauran, N.; Eikermann, M. Guideline appraisal with AGREE II: Online survey of the potential influence of AGREE II items on overall assessment of guideline quality and recommendation for use. BMC Health Ser. Res. 2018, 18, 143. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.A.; Toupin-April, K.; Jutai, J.W.; Duffy, C.M.; Rahman, P.; Cavallo, S.; Brosseau, L. A systematic critical appraisal of clinical practice guidelines in juvenile idiopathic arthritis using the appraisal of guidelines for research and evaluation II (AGREE II) instrument. PLoS ONE 2015, 10, e0137180. [Google Scholar] [CrossRef]
- Matwiejczyk, L.; Mehta, K.; Scott, J.; Tonkin, E.; Coveney, J. Characteristics of effective interventions promoting healthy eating for pre-schoolers in childcare settings: An umbrella review. Nutrients 2018, 10, 293. [Google Scholar] [CrossRef] [Green Version]
- Stacey, F.G.; Finch, M.; Wolfenden, L.; Grady, A.; Jessop, K.; Wedeswiler, T.; Bartlem, K.; Jones, J.; Sutherland, R.; Vandevijvere, S. Evidence of the potential effectiveness of centre-based childcare policies and practices on child diet and physical activity: Consolidating evidence from systematic reviews of intervention trials and observational studies. Curr. Nutr. Rep. 2017, 6, 228–246. [Google Scholar] [CrossRef]
- Finch, M.; Jones, J.; Yoong, S.; Wiggers, J.; Wolfenden, L. Effectiveness of centre-based childcare interventions in increasing child physical activity: A systematic review and meta-analysis of policymakers and practitioners. Obes. Rev. 2016, 17, 412–428. [Google Scholar] [CrossRef]
- Winconsin Department of Health Services. Healthy Bites: A Winconsin Guide for Improving Childhood Nutrition; Winconsin Department of Health Services: Madison, WI, USA, 2019. Available online: https://dpi.wi.gov/sites/default/files/imce/community-nutrition/pdf/HealthyBites.pdf (accessed on 2 November 2020).
- Nemours Health & Prevention Services. Best Practices for Healthy Eating: A Guide to Help Children Grow up Healthy. 2008. Available online: https://www.nemours.org/content/dam/nemours/www/filebox/service/preventive/nhps/heguide.pdf (accessed on 2 November 2020).
- NSW Ministry of Health. Caring for Children. 2014. Available online: https://www.health.nsw.gov.au/heal/Publications/caring-for-children-manual.pdf (accessed on 2 November 2020).
- Action for Children. Eat better, start better. In A Practical Guide: Voluntary Food and Drink Guidelines for Early Years Settings in England; Food Trust, Ed.; Action for Children, 2017; Available online: https://www.foundationyears.org.uk/wp-content/uploads/2017/11/Eat-Better-Start-Better1.pdf (accessed on 2 November 2020).
- ACT Nutrition Support Service. Menu Planning in Childcare. 2016. Available online: https://www.actnss.org.assets/Menu-planning-guidelies-and-template.pdf (accessed on 2 November 2020).
- Northern Territory Government. Long Day Care Menu Planner. 2016. Available online: https://digitallibrary.health.nt.gov.au/prodjspui/bitstream/10137/665/1/Child%20Care%20Centre%20Menu%20Planner.pdf (accessed on 2 November 2020).
- Pollard, C.; Lewis, J.; Miller, M. Start right-eat right award scheme: Implementing food and nutrition policy in child care centers. Health Educ. Behav. 2001, 28, 320–330. [Google Scholar] [CrossRef]
- Ministry of Health. Healthy Food and Drink Guidance- Early Learning Services; Ministry of Health: Wellington, New Zealand, 2020. Available online: https://www.health.govy.nz/system/files/documents/publications/healthy-food-and-drink-guidance-early-learning-services-mar20.pdf (accessed on 2 November 2020).
- Healthy Eating Advisory Service. Menu Planning Guidelines for Long Day Care. 2020. Available online: https://live-heas-ca49051.pantheonsite.io/sites/default/files/ECS-Menu-planning-guidelines-LDC-2020.pdf (accessed on 2 November 2020).
- Winconsin Department of Health Services. Active Early: A Winconsin Guide for Improving Childhood Physical Activity; Winconsin Department of Health Services: Madison, WI, USA, 2018. Available online: https://www.dhs.winsonsin.gov/publications/p0/p00280.pdf (accessed on 2 November 2020).
- The Department of Health. Australian 24-Hour Movement Guidelines for the Early Years (Birth to 5 years). 2019. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/health-pubhlth-strateg-phys-act-guidelines#npa05 (accessed on 2 November 2020).
- Nemours Health & Prevention Services. Best Practices for Physical Activity: A Guide to Help Children Grow up Healthy. 2009. Available online: https://www.nemours.org/content/dam/nemours/www/filebox/service/preventive/nhps/paguidelines.pdf (accessed on 2 November 2020).
- Tremblay, M.S.; Chaput, J.-P.; Adamo, K.B.; Aubert, S.; Barnes, J.D.; Choquette, L.; Duggan, M.; Faulkner, G.; Goldfield, G.S.; Gray, C.E. Canadian 24-hour movement guidelines for the early years (0–4 years): An integration of physical activity, sedentary behaviour, and sleep. BMC Public Health 2017, 17, 874. [Google Scholar] [CrossRef]
- Pennington Biomedical Research Center. Policy Intervention Briefs: Enacting Eight Policies To Prevent Childhood Obesity: Projected Outcomes For Louisiana; Pennington Biomedical Research Center: Lousiana, LA, USA, 2006; Available online: https://www.pbrc.edu/prism/docs/PRISM_PolicyInterventionBriefs.pdf (accessed on 2 November 2020).
- Missouri Department of Health and Senior Services. Missouri Move Smart Child Care. 2018. Available online: https://health.mo.gov/living/wellness/nutrition/movesmartguidelines/pdf/MOveSmartWorkbook.pdf (accessed on 2 November 2020).
- Arizona Department of Health Services. Empower Guidebook. Ten Ways to Empower Children to Live Healthy Lives: Standards for Empower Child Care Facilities in Arizona. 2016. Available online: https://www.azdhs.gov/documents/prevention/nutrition-physical-activity/empower/resources-policies/empower-guidebook.pdf (accessed on 2 November 2020).
- The Child and Adolescent Obesity Task Force. Action Plan for Preventing Child and Adolescent Obesity. Promoting Healthy Lifestyles and Preventing Obesity In the Child Care Setting. 1999. Available online: www.iowa.gov/iowansfitforlife/docs/The_Prevention_of_Child_and_Adolescent_Obesity_in_Iowa.doc+&cd=1&hl=en&ct=clnk&gl=au (accessed on 2 November 2020).
- Benjamin-Neelon, S.E. Position of the Academy of Nutrition and Dietetics: Benchmarks for nutrition in child care. J. Acad. Nutr. Diet. 2018, 118, 1291–1300. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Pediatrics; American Public Health Association; National Resource Center for Health and Safety in Child Care and Early Education. Preventing Childhood Obesity in Early Care and Education: Selected Standards from Caring for Our Children: National Health and Safety Performance Standards, Guidelines for Early Care and Education Programs. 3rd ed. 2012. Available online: https://nrckids.org/CFOC/Childhood_Obesity (accessed on 2 November 2020).
- Harvard, T.H.; Chan School of Public Health. Early Child Care Obesity Prevention Recommendations: Complete List. Available online: https://www.hsph.harvard.edu/obesity-prevention-source/obesity-prevention/early-child-care/early-child-care-obesity-prevention-recommendation-complete-list/ (accessed on 2 November 2020).
- McGuire, S. Institute of Medicine (IOM) Early Childhood Obesity Prevention Policies; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Crawley, H. Eating Well for Under-5s in Child Care: Practical and Nutritional Guidelines. 2006. Available online: https://cwt.org.uk/wp-content/uploads/2014/07/Under5s.pdf (accessed on 2 November 2020).
- Health Promotion Unit Department of Health and Children. Food and Nutrition Guidelines for Pre-School Services. 2004. Available online: https://assets.gov.ie/18832/6406be0488a643e88f6d512856a7b573.pdf (accessed on 2 November 2020).
- Llywodraeth Cymru Welsh Government. Food & Nutrition for Childcare Settings: Best Practice Guidance. 2018. Available online: https://gov.wales/sites/default/files/publications/2019-03/190313-nutrition-guidance-complete.pdf (accessed on 2 November 2020).
- Australian Government Department of Health and Ageing. Get Up & Grow: Healthy Eating and Physical Activity for Early Childhood. 2009. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/2CDB3A000FE57A4ECA257BF0001916EC/$File/HEPA%20-%20B5%20Book%20-%20Staff%20and%20Carer%20Book_LR.pdf (accessed on 2 November 2020).
- Nemours Children’s Health System. Healthy Kids, Healthy Future. Available online: https://healthykidshealthyfuture.org/5-healthy-goals/nurture-healthy-eaters/ (accessed on 2 November 2020).
- Washington State Department of Health. Improving Healthy Weight in Children: The Healthiest Next Generation Initiative; Division of Prevention and Community Health: Washington, DC, USA, 2014. Available online: https://www.doh.wa.gov/Portals/1/Documents/Pubs/120-037-HNGMidYearLegReportDec2014.pdf (accessed on 2 November 2020).
- Maine Health. Let’s Go! Health Care Toolkit; Maine Health: Portland, OR, USA, 2014; Available online: https://www.mainehealth.org/-/media/lets-go/files/childrens-program/pediatric-family-practices/full-healthcare-toolkit.pdf (accessed on 2 November 2020).
- Early Childhood Education Linkage System and Healthy Child Care Pennsylvania. Model Child Care Health. 2014. Available online: http://ecels-healthychildcarepa.org/publications/manuals-pamphlets-policies/item/248-model-child-care-health-policies.html (accessed on 2 November 2020).
- NSW Ministry of Health. Munch & Move: Resource Manual Birth to Five Years; NSW Ministry of Health: North Sydney, Australia, 2017. Available online: https://www.healthykids.nsw.gov.au/downloads/file/campaignsprograms/MMManualPart1-Introduction.pdf (accessed on 2 November 2020).
- NYC Health. Nutriton and Physical Activity Best Practices for Child Care Centers. 2015. Available online: https://www1.nyc.gov/assets/doh/downloads/pdf/dc/childcare-phys-best.pdf (accessed on 2 November 2020).
- Scottish Executive. Nutritional Guidance for Early Years: Food Choices for Children Aged 1-5 Years in Early Education and Child Care Setting. 2006. Available online: https://www.gov.scot/binaries/content/documents/govscot/publications/advice-and-guidance/2006/01/nutritional-guidance-early-years-food-choices-children-aged-1-5-years-early-education-childcare-settings/documents/0021563-pdf/0021563-pdf/govscot%3Adocument/0021563.pdf (accessed on 2 November 2020).
- U. S. Department of Agriculture and U.S. Department of Health and Human Services. Nutrition and Wellness Tips for Young Children: Provider Handbook for the Child and Adult Care Food Program; USDA Food and Nutrition Service: Alexandria, VA, USA, 2013. Available online: http://www.yoursforchildren.com/nutrition-resources/TeamNutrition/Nutrition%20&%20Wellness%20Tips%20for%20Young%20Children%20--%20English.pdf (accessed on 2 November 2020).
- South Australian Department of Education and Children’s Services and SA Health. Right Bite: Healthy Food and Drink Supply Strategy for South Australian Schools and Preschools. 2008. Available online: https://www.education.sa.gov.au/sites/default/files/right_bite_manual_colour.pdf?acsf_files_redirect (accessed on 2 November 2020).
- NHS Health Scotland. Setting the Table: Nutritional Guidance and Food Standards for Early Years Childcare Providers in Scotland. 2018. Available online: http://www.healthscotland.com/uploads/documents/30341-Setting%20the%20Table.pdf (accessed on 2 November 2020).
- The Food Trust. The Preschool Initiative: Building A Healthy Foundation For Life. 2011. Available online: http://thefoodtrust.org/uploads/media_items/the-preschool-initiative.original.pdf (accessed on 2 November 2020).
- State of Alaska Department of Health and Social Services, Wellness Guidelines for Alaska’s Young Children: A Toolkit For Child Care Providers And Families. 2017. Available online: http://dhss.alaska.gov/dph/Chronic/Documents/Obesity/EarlyCare/AKWellnessGuidelines_YoungChildren.pdf (accessed on 2 November 2020).
- Scott-Sheldon, L.A.; Hedges, L.V.; Cyr, C.; Young-Hyman, D.; Khan, L.K.; Magnus, M.; King, H.; Arteaga, S.; Cawley, J.; Economos, C.D. Childhood Obesity Evidence Base Project: A systematic review and meta-analysis of a new taxonomy of intervention components to improve weight status in children 2–5 years of age, 2005–2019. Child. Obes. 2020, 16 (Suppl. S2), 21–48. [Google Scholar] [CrossRef]
- Narzisi, K.; Simons, J. Interventions that prevent or reduce obesity in children from birth to five years of age: A systematic review. J. Child Health Care 2020. [Google Scholar] [CrossRef] [Green Version]
- Yoong, S.L.; Grady, A.; Wiggers, J.H.; Stacey, F.G.; Rissel, C.; Flood, V.; Finch, M.; Wyse, R.; Sutherland, R.; Salajan, D. Child-level evaluation of a web-based intervention to improve dietary guideline implementation in childcare centers: A cluster-randomized controlled trial. Am. J. Clin. Nutr. 2020, 111, 854–863. [Google Scholar] [CrossRef]
- Yoong, S.L.; Grady, A.; Seward, K.; Finch, M.; Wiggers, J.; Lecathelinais, C.; Wedesweiler, T.; Wolfenden, L. The Impact of a Childcare Food Service Intervention on Child Dietary Intake in Care: An Exploratory Cluster Randomized Controlled Trial. Am. J. Health Promot. 2019, 33, 991–1001. [Google Scholar] [CrossRef]
- Seward, K.; Wolfenden, L.; Finch, M.; Wiggers, J.; Wyse, R.; Jones, J.; Yoong, S.L. Improving the implementation of nutrition guidelines in childcare centres improves child dietary intake: Findings of a randomised trial of an implementation intervention. Public Health Nutr. 2017, 21, 607–617. [Google Scholar] [CrossRef] [Green Version]
- Vercammen, K.A.; Frelier, J.M.; Lowery, C.M.; McGlone, M.E.; Ebbeling, C.B.; Bleich, S.N. A systematic review of strategies to reduce sugar-sweetened beverage consumption among 0-year to 5-year olds. Obes. Rev. 2018, 19, 1504–1524. [Google Scholar] [CrossRef] [PubMed]
- Ward, S.; Belanger, M.; Donovan, D.; Carrier, N. Systematic review of the relationship between childcare educators’ practices and preschoolers’ physical activity and eating behaviours. Obes. Rev. 2015, 16, 1055–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodder, R.K.; O’Brien, K.M.; Tzelepis, F.; Wyse, R.J.; Wolfenden, L. Interventions for increasing fruit and vegetable consumption in children aged five years and under. Cochrane Database Syst. Rev. 2020, 5. [Google Scholar] [CrossRef]
- Morgan, E.H.; Schoonees, A.; Sriram, U.; Faure, M.; Seguin-Fowler, R.A. Caregiver involvement in interventions for improving children’s dietary intake and physical activity behaviors. Cochrane Database Syst. Rev. 2020, 1. [Google Scholar] [CrossRef] [Green Version]
- van de Kolk, I.; Verjans-Janssen, S.R.B.; Gubbels, J.S.; Kremers, S.P.J.; Gerards, S.M.P.L. Systematic review of interventions in the childcare setting with direct parental involvement: Effectiveness on child weight status and energy balance-related behaviours. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 110. [Google Scholar] [CrossRef] [Green Version]
- Nathan, N.; Janssen, L.; Sutherland, R.; Hodder, R.K.; Evans, C.E.L.; Booth, D.; Yoong, S.L.; Reilly, K.; Finch, M.; Wolfenden, L. The effectiveness of lunchbox interventions on improving the foods and beverages packed and consumed by children at centre-based care or school: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 38. [Google Scholar] [CrossRef] [Green Version]
- Sisson, S.B.; Krampe, M.; Anundson, K.; Castle, S. Obesity prevention and obesogenic behavior interventions in child care: A systematic review. Prev. Med. 2016, 87, 57–69. [Google Scholar] [CrossRef]
- Wolfenden, L.; Barnes, C.; Lane, C.; McCrabb, S.; Brown, H.M.; Gerritsen, S.; Barquera, S.; Vejar, L.S.; Munguia, A.; Yoong, S.L. Consolidating evidence on the effectiveness of interventions promoting fruit and vegetable consumption: An umbrella review. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 11. [Google Scholar] [CrossRef]
- Ayers Looby, A.; Frost, N.; Gonzalez-Nahm, S.; Grossman, E.R.; Ralston, A.J.; Benjamin-Neelon, S.E. State Regulations to Support Children’s Cultural and Religious Food Preferences in Early Care and Education. Matern. Child Health J. 2020, 24, 121–126. [Google Scholar] [CrossRef] [Green Version]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- de Onis, M.; Blössner, M.; Borghi, E. Global prevalence and trends of overweight and obesity among preschool children. Am. J. Clin. Nutr. 2010, 92, 1257–1264. [Google Scholar] [CrossRef] [Green Version]
- Nanney, M.S.; LaRowe, T.L.; Davey, C.; Frost, N.; Arcan, C.; O.Meara, J. Obesity prevention in early child care settings: A bistate (Minnesota and Wisconsin) assessment of best practices, implementation difficulty, and barriers. Health Educ. Behav. 2017, 44, 23–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farewell, C.V.; Powers, J.N.; Maiurron, E.; Scarbro, S.; Quinlan, J.; Puma, J. Implementation of policy, system and environment changes in early childhood education settings. Int. J. Care Educ. Policy 2020, 14, 1–12. [Google Scholar] [CrossRef]
- Bergling, E.; Farewell, C.; Puma, J. Development of a Dissemination and Implementation Framework for an Early Childhood Obesity Prevention Program. J. Nutr. Educ. Behav. 2020, 52, 1160–1165. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Guideline | Jurisdiction Area | Publisher | Year Published | Target Group | Overall Quality Assessment | Risk Factors Targeted | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| DB | PA | SB | ST | SLP | ||||||
| Ten ways to empower children to live healthy lives: standards to empower childcare facilities in Arizona (3rd Ed) [48] | Arizona, USA | Arizona Nutrition Network | 2016 | Children 0–6 years | Recommended with modifications | ✓ | ✓ | ✓ | ✓ | |
| Action Plan for Preventing Child and Adolescent Obesity. Promoting Healthy Lifestyles and Preventing Obesity in the Child Care setting [49] | Iowa, USA | The Child and Adolescent Obesity Task Force | 1999 | Children in child care | Not recommended | ✓ | ✓ | ✓ | ✓ | |
| Active Early: a Winconsin guide for improving childhood physical activity (2nd Ed) [42] | Winconsin, USA | Winconsin Department of Health Services | 2018 | Children 0–6 years | Recommended with modifications | ✓ | ✓ | ✓ | ||
| Healthy Bites: a Winconsin guide for improving childhood nutrition (2nd Ed) [33] | Winconsin, USA | Winconsin Department of Health Services | 2019 | Children 0–6 years | Recommended with modification | ✓ | ||||
| Australian 24-h movement guidelines for the early years (birth to 5 years) [43] | Australia | Australian Government, Department of Health | 2019 | Children 0–5 years | Recommended with modifications | ✓ | ✓ | ✓ | ✓ | |
| Position of the Academy of Nutrition and Dietetics: Benchmarks for Nutrition in Childcare [50] | USA | Academy of Nutrition and Dietetics | 2018 | Children 2–5 years | Recommended with modifications | ✓ | ✓ | |||
| Best Practices for Healthy Eating: a guide to help children grow up healthy [34] | Delaware, USA | Nemours Health and Prevention Service | 2008 | Children 0–6 years | Recommended with modifications | ✓ | ||||
| Best Practices for Physical Activity: for organizations serving children and youth a guide to help children grow up healthy [44] | Delaware, USA | Nemours Health and Prevention Service | 2009 | Children 0–6 years | Recommended with modifications | ✓ | ✓ | ✓ | ||
| Canadian 24-h movement guidelines for the early years (0–4 years): an integration of physical activity, sedentary behaviour and sleep [45] | Canada | The Canadian Society for Exercise Physiology | 2017 | Children 0–4 years | Recommended without modifications | ✓ | ✓ | ✓ | ✓ | |
| Caring for Children [35] | NSW, Australia | NSW Ministry of Health | 2014 | Children 0–5 years | Recommended with modifications | ✓ | ||||
| Caring for our children, National Health and Safety Performance Standards: Guidelines for Early Care and Education Programs [51] | Washington, USA | American Academy of Paediatrics, American Public Health Association and National Resource Centre for Health and Safety in Child Care and Early Education | 2012 | Children 0–6 years | Recommended without modifications | ✓ | ✓ | ✓ | ||
| Early childcare obesity prevention recommendations [52] | USA | Harvard T.H. Chan School of Public Health | - | Children 0–6 years | Recommended with modifications | ✓ | ✓ | ✓ | ✓ | ✓ |
| Early childhood obesity prevention policies [53] | USA | Committee on Obesity Prevention Policies for Young Children, Institute of Medicine | 2011 | Children 0–5 years | Recommended without modifications | ✓ | ✓ | ✓ | ✓ | ✓ |
| Eat Better Start Better: Voluntary Food and Drink Guidelines for Early Years Setting in England—a Practical Guide [36] | United Kingdom | Action for Children | 2017 | Children 6 months–4 years | Recommended with modifications | ✓ | ||||
| Eating Well for Under-5s in Child Care: Practical and nutritional guidelines, 2nd edition [54] | United Kingdom | The Caroline Walker Trust | 2006 | Children 0–5 years | Recommended with modifications | ✓ | ✓ | |||
| Enacting eight policies to prevent childhood obesity: projected outcomes for Louisiana [46] | Louisiana, USA | Pennington Biomedical Research Center, Louisiana State University System | 2013 | Children 1–5 years | Recommended with modifications | ✓ | ✓ | ✓ | ✓ | |
| Food and Nutrition Guidelines for Pre-school services [55] | Ireland | Health promotion unit department of health and children | 2004 | Children 0–5 years | Recommended with modifications | ✓ | ✓ | |||
| Food & Nutrition for childcare settings: Best Practice guidance [56] | Wales | Llywodraeth Cymru Welsh Government | 2018 | Children 0–5 years | Recommended with modifications | ✓ | ✓ | ✓ | ✓ | |
| Get Up & Grow: Healthy Eating and Physical Activity for Early Childhood [57] | Australia | Australian Government Department of Health and Ageing | 2009 | Children 0–5 years | Recommended with modifications | ✓ | ✓ | |||
| Menu Planning in Childcare [37] | ACT, Australia | ACT Nutrition Support Service | 2016 | Children 0–5 years | Recommended with modifications | ✓ | ||||
| Long Day Care Menu Planner [38] | NT, Australia | Northern Territory Government | 2016 | Children 0–4 years | Recommended with modifications | ✓ | ||||
| Start Right, Eat Right [39] | VIC, Australia | State Government of Victoria, Department of Health | 2004 | Children 2–4 years | Recommended with modifications | ✓ | ||||
| Healthy Food and Drink Guidance- Early Learning Services [40] | New Zealand | Ministry of Health, Manatu Hauora, New Zealand Government | 2020 | Children 0–6 years | Recommended with modifications | ✓ | ||||
| Healthy Kids, Healthy Future [58] | USA | Nemours, Children’s Health System | - | Children 0–5 years | Recommended with modifications | ✓ | ✓ | ✓ | ||
| Improving healthy weight in children: The healthiest next generation initiative [59] | Washington State, USA | Washington State Department of Health | 2014 | Children 3–4 years | Recommended with modifications | ✓ | ✓ | |||
| Let’s Go! Health Care Toolkit [60] | Portland, Maine, USA | Maine Health | 2015 | - | Recommended with modifications | ✓ | ✓ | ✓ | ✓ | |
| Menu planning guidelines for long day care [41] | VIC, Australia | Healthy Eating Advisory Service | 2020 | Children 1–5 years | Recommended with modifications | ✓ | ||||
| Missouri Move Smart Child Care [47] | Missouri, USA | Missouri Department of Health and Senior Services | 2018 | Children 0–5 years | Recommended with modifications | ✓ | ✓ | ✓ | ||
| Model Child care health policies (5th Edition) [61] | Pennsylvania, USA | Early childhood education Linkage system: Healthy child care Pennsylvania | 2014 | Young children in childcare | Recommended with modifications | ✓ | ✓ | ✓ | ✓ | |
| Much & Move [62] | NSW, Australia | NSW Ministry of Health | 2017 | Children 0–5 years | Recommended with modifications | ✓ | ✓ | ✓ | ✓ | ✓ |
| Nutrition and Physical Activity Best Practices for Child Care Centers [63] | New York City, USA | NYC Health | 2015 | Children 0–5 years | Recommended with modifications | ✓ | ✓ | ✓ | ✓ | ✓ |
| Nutritional Guidance for early years food choices for children aged 1–5 years in early education and childcare settings [64] | Edinburgh, Scotland | Scottish Executive | 2006 | Children 1–5 years | Recommended with modifications | ✓ | ✓ | |||
| Nutrition and Wellness Tips for Young Children: provider handbook for the child and adult care food program [65] | Virginia, USA | USDA Food and Nutrition Service | 2013 | Children 2–5 years | Recommended with modifications | ✓ | ✓ | ✓ | ||
| Right Bite, Easy Guide to Healthy Food and Drink Supply for South Australian Schools and Preschools [66] | SA, Australia | SA Department of Education and Children’s Services and SA Health | 2008 | Children in pre-school | Recommended with modifications | ✓ | ||||
| Setting the Table- Nutritional Guidance and Food Standards for Early Years Childcare Providers in Scotland [67] | Scotland, UK | NHS: Health Scotland | 2018 | Children 1–5 years | Recommended with modifications | ✓ | ✓ | ✓ | ||
| Sit less, move more, sleep well: Active play guidelines for under-fives (NZ) [17] | New Zealand | Ministry of Health. Manatu Hauora. | 2017 | Children 0–5 years | Recommended with modifications | ✓ | ✓ | ✓ | ||
| The preschool initiative: building a healthy foundation for life [68] | Philadelphia, USA | The Food Trust | 2011 | Children 3–5 years | Recommended with modifications | ✓ | ✓ | |||
| Wellness Guidelines for Alaska’s Young Children: A toolkit for child care providers and families [69] | Alaska, USA | State of Alaska, Department of Health and Social Services. | 2017 | Children 0–5 years | Recommended with modifications | ✓ | ✓ | ✓ | ✓ | |
| ANGELO * Modifiable Environment | Recommended Dietary Behavior Policy and Practice Themes | Frequency of Recommendation |
|---|---|---|
| Physical | 1. Set Nutrition Standards For The Food And Beverages Available In Early Childhood Education And Care (ECEC) Setting | 30 [33,34,35,36,38,39,40,41,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69] |
| 1.1. Nutrition standards, recommended serving sizes for foods, snacks, meals and beverages provided are aligned with national nutrition guidelines | 28 [33,34,35,36,38,39,40,41,49,50,51,52,53,54,55,56,57,58,59,60,62,63,64,65,66,67,68,69] | |
| 1.2. Provide a variety of healthy foods from the main food groups in age appropriate portion sizes | 28 [33,34,35,36,38,39,40,41,49,50,51,52,53,54,55,56,57,58,59,60,62,63,64,65,66,67,68,69] | |
| 1.3. Specific standards for ECEC food service menus | 18 [33,34,35,36,38,39,41,49,51,52,54,56,59,63,65,66,67,69] | |
| 1.4. Water should be widely available to children at all times | 23 [33,34,35,36,38,40,41,49,51,54,55,56,57,58,59,61,62,63,64,65,67,68,69] | |
| 1.5. Limit serves and types of sugar sweetened beverages (including fruit juice) | 25 [33,34,35,36,38,40,41,48,49,50,51,52,54,55,56,58,59,60,61,63,64,65,67,68,69] | |
| 1.6. Offer age appropriate milk and beverages (i.e., no tea, coffee or energy drinks) | 22 [33,34,35,36,38,40,41,52,54,55,56,58,59,60,61,62,63,64,65,67,68,69] | |
| 1.7. Keep high energy, low nutrient foods (e.g., sweets, confectionary, high fat/salty snacks) out of the childcare | 10 [33,38,40,52,54,57,61,63,66,67] | |
| Policy | 2. Develop And Adopt A Healthy Eating Policy | 3 [39,55,59] |
| 2.1. Nutrition policy is reviewed (annually and/or by an expert i.e., dietitian) | 2 [55,59] | |
| 2.2. Parents are involved in the development of the policy | 2 [39,55] | |
| 2.3. Ensure staff are willing to working within the policy | 1 [39] | |
| 2.4. Provide a copy of the policy to parents and staff | 1 [55] | |
| Sociocultural | 3. Provide Opportunities For Nutrition Education | 11 [33,35,39,49,50,55,57,64,65,68,69] |
| 3.1. Offer a variety of food awareness/education activities (i.e., allow children to experiment with different foods (shapes, colors, textures), and discuss food preferences and family food traditions) | 11 [33,35,39,49,50,55,57,64,65,68,69] | |
| Sociocultural | 4. Staff Training In Nutrition Curriculum And Practices | 4 [39,49,50,53] |
| 4.1. Educators are trained in nutrition curriculum/education | 1 [39] | |
| 4.2. Educators are trained to understand children can be healthy at a variety of weights and avoid referring to child’s body size | 1 [49] | |
| 4.3. Educators are trained in implementing health eating practices | 2 [39,50] | |
| 4.4. Food Service Staff are trained food hygiene and safety | 1 [39] | |
| Sociocultural | 5. Educator Feeding Practices To Encourage Healthy Eating | 16 [33,38,39,48,49,50,53,54,55,56,58,59,61,62,63,69] |
| 5.1. Food is not to be used as reward or punishment | 9 [38,48,49,55,56,59,61,63,69] | |
| 5.2. Avoid celebrating special occasions with food or using as a reward | 2 [38,63] | |
| 5.3. Don’t force or bribe children to eat | 3 [55,63,69] | |
| 5.4. Encourage children to taste different fruit and vegetables each day (praise children for eating healthy foods) | 7 [33,54,55,56,61,62,63] | |
| 5.5. Educators should involve children in preparing food and laying and clearing the table | 3 [54,61,63] | |
| 5.6. Staff sit with children during meals, and role model healthy behaviors (i.e., eat and drink healthy food and beverages in front of children) | 5 [33,49,50,53,69] | |
| 5.7. Educators discuss the food served with children | 3 [39,49,58] | |
| Physical | 6. Create An Environment That Encourages And Promotes Healthy Eating | 25 [33,35,38,39,40,49,50,51,52,53,54,55,56,57,58,59,61,62,63,64,66,67,69] |
| 6.1. Allow children adequate time to eat | 9 [35,39,49,53,54,55,56,61,64] | |
| 6.2. Provide healthy options in appropriate serves, and allow children to self-serve (allow children to choose which foods they eat and how much) | 14 [33,35,39,49,53,54,55,57,58,61,62,64,69] | |
| 6.3. Continue to offer children healthy options (repeat exposure and offer equal options) | 5 [49,53,55,61,69] | |
| 6.4. Create a relaxed, enjoyable and social meal time environment (i.e., family style mealtimes to encourage child-child and child-educator interactions) | 12 [33,39,50,55,56,57,58,59,61,62,64,69] | |
| 6.5. Ensure regular and consistent meal and snack patterns (should be consistent and predictable schedule) | 10 [33,35,39,51,53,54,55,57,62,64] | |
| 6.6. Make fruit and vegetables snacks widely available and easily accessible | 1 [63] | |
| 6.7. Display healthy eating materials on the walls of the eating room | 1 [55] | |
| Sociocultural | 7. Parent Engagement | 9 [33,39,50,52,53,55,56,57,58,59,69] |
| 7.1. Encourage parents to pack healthy food from home and ensure foods bought from home meet nutrition written standards | 6 [50,52,53,55,57,69] | |
| 7.2. Encourage family involvement in healthy eating at the ECEC e.g., take menu suggestions from parents that are consistent with healthy eating guidelines | 6 [33,39,52,53,55,56] | |
| 7.3. Provide a copy of written nutrition guidelines to parents | 3 [52,55,69] | |
| 7.4. Provide parents a copy of ECEC menu | 4 [52,55,56] | |
| 7.5. Offer parent nutrition education as part of the ECEC program | 1 [39] | |
| 7.6. Make parents aware of nutrition learning activities provided to children | 1 [39,69] |
| ANGELO * Modifiable Environment | Recommended Physical Activity Policy and Practice Themes | Frequency of Recommendation |
| Physical; Sociocultural | 1. Provide Opportunities For Children To Be Physically Active (More Is Better) | 28 [17,35,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,59,60,61,62,63,65,67,68,69] |
| 1.1. Ensure physical activity is incorporated into daily routines and formal childcare curriculum | 5 [42,52,53,54,63] | |
| 1.2. Include at least 180 min of physical activity of any intensity, spread throughout the day | 16 [42,43,45,48,50,52,53,55,57,59,60,62,65,67,68,69] | |
| 1.3. For children 3–4 years, include at least 60 min of moderate-to-vigorous physical activity during the day | 12 [43,45,48,51,52,54,59,61,62,65,68,69] | |
| 1.4. Include opportunities for adult-led, structured physical activity | 10 [42,44,47,48,51,53,59,63,65,69] | |
| 1.5. Include opportunities for unstructured physical activity, free play (play-time) | 9 [42,44,46,47,48,49,63,65,69] | |
| 1.6. Provide daily opportunities for activity through outdoor playtime (should be supervised) | 11 [17,42,44,49,51,53,55,56,61,65,69] | |
| 1.7. Provide opportunities for children to develop and practice gross motor and movement skills | 4 [49,51,62,63] | |
| 1.8. Include culturally appropriate physical activities | 1 [63] | |
| Policy; Sociocultural | 2. Develop And Adopt Policies For Physical Activity And Physical Activity Education Programs | 3 [33,53,69] |
| 2.1. Engage staff and parent support for physical activity standards | 1 [53] | |
| 2.2. Seek consultation from experts annually on the physical activity programs delivered in the childcare | 1 [53] | |
| 2.3. Provide parent education at least 2 times a year (to reduce screen time) | 1 [33] | |
| 2.4. Develop a written policy promoting physical activity and the removal of barriers to physical activity participation (including limiting screen time) | 1 [69] | |
| Sociocultural | 3. Offer Educator Training To Provide Safe And Developmentally Appropriate Physical Activity | 2 [53,69] |
| 3.1. Staff should be trained to provide guidance to parents to encourage physical activity | 1 [53] | |
| 3.2. Staff should be trained to provide guidance to parents in appropriate sleep duration | 1 [53] | |
| 3.3. Staff should be trained in encouraging child physical activity and decreasing sedentary behavior | 1 [53] | |
| 3.4. Offer staff annual training opportunities in physical activity programs and practices | 1 [69] | |
| Sociocultural | 4. Educators To Promote The Benefits Of Physical Activity With Children | 8 [44,49,53,59,63,65,68,69] |
| 4.1. Educators should model physical activity by participating in activities | 5 [17,49,53,63,69] | |
| 4.2. Engage children in physical activity they enjoy, including games and sport (age appropriate, fun and offer variety) | 5 [17,44,49,63,68] | |
| 4.3. Expressive play is encouraged e.g., music, dancing and make believe | 3 [17,49,63] | |
| 4.4. Educators embed physical activity into educational activities | 2 [49,53] | |
| 4.5. Avoid punishing children for being physical active | 1 [53] | |
| 4.6. Avoid withholding physical activity as a punishment | 4 [53,59,63,69] | |
| 4.7. Elimination games should be avoided as well as competitive activates and games | 3 [43,63,65] | |
| 4.8. Engage equal participation from boys and girls in physical activity | 1 [63] | |
| 4.9. Celebrate special occasions with physical activity (games, dancing and extra playground time). | 1 [63] | |
| Physical; Sociocultural | 5. Limit The Time Children Spend Sitting (Less Is Best) | 14 [17,42,43,44,45,47,48,49,52,53,57,62,63,67] |
| 5.1. Children should not be sitting for extended periods (or be restrained) for more than 30–60 min at a time | 12 [42,43,44,45,47,48,49,52,53,57,62,63] | |
| 5.2. When sedentary, children should be engaged in educational and creative pursuits, and be engaged socially. | 3 [43,45,62] | |
| 5.3. Engage children that tend to be sedentary in active play | 2 [45,49] | |
| Physical; Sociocultural | 6. Limit The Use Of Screen Time (Less Is Best) | 23 [17,33,42,43,44,45,46,47,48,49,51,52,53,56,57,59,60,61,62,63,65,67,69] |
| 6.1. No screen time is recommended for children <2 years | 16 [17,43,45,46,47,48,51,53,56,57,59,60,61,62,65,69] | |
| 6.2. No more than 1 h of screen time/week is recommended for children aged 2 or above | 18 [17,43,44,45,46,47,49,51,52,53,56,57,59,60,61,62,63,65] | |
| 6.3. Screens should not be used/available during mealtimes or nap times | 5 [48,51,61,65,69] | |
| 6.4. Limit the use of screen time for educational activities or active movement programs | 5 [42,47,61,65,69] | |
| 6.5. Parent permission should be requested for children to participate in any screen based activity | 1 [44] | |
| 6.6. Screen time should be supervised by an adult (to help children apply what they are learning) | 2 [44,51] | |
| 6.7. When offered, screen/digital media should be free from advertising, violence or should that tempt children to overuse | 4 [51,61,63,65] | |
| 6.8. Work with parents to limit overall screen time | 1 [33] | |
| Physical | 7. Support Healthy Sleeping Habits | 9 [17,43,45,52,53,56,60,61,62] |
| 7.1. Include a nap within the daily routine, with regular sleep and wake-up times | 6 [17,43,45,52,61,62] | |
| 7.2. Provide an environment that provides restful sleep: remove screen media from sleeping/napping areas and low noise | 4 [52,53,56,61] | |
| 7.3. Maintain a calm nap-time routine | 2 [52,53] | |
| Physical | 8. Create A Physical Environment That Promotes Physical Activity | 6 [44,49,53,54,63,69] |
| 8.1. Provide play equipment that encourages physical activity | 4 [44,49,53,54] | |
| 8.2. Provide simple play equipment to encourage creative play and exploration (e.g., cardboard boxes) and portable play equipment that encourages indoor and outdoor play | 4 [49,53,54,63] | |
| 8.3. Provide adequate space for children to be physically active | 4 [44,53,54,69] | |
| 8.4. Ensure the outdoor area offers variety in terms of secure equipment in shade, open grass and varying surfaces | 2 [53,54] | |
| 8.5. Ensure that the educator to child ratio is fairly low (i.e., less than 10 children to one educator) | 1 [63] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jackson, J.K.; Jones, J.; Nguyen, H.; Davies, I.; Lum, M.; Grady, A.; Yoong, S.L. Obesity Prevention within the Early Childhood Education and Care Setting: A Systematic Review of Dietary Behavior and Physical Activity Policies and Guidelines in High Income Countries. Int. J. Environ. Res. Public Health 2021, 18, 838. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020838
Jackson JK, Jones J, Nguyen H, Davies I, Lum M, Grady A, Yoong SL. Obesity Prevention within the Early Childhood Education and Care Setting: A Systematic Review of Dietary Behavior and Physical Activity Policies and Guidelines in High Income Countries. International Journal of Environmental Research and Public Health. 2021; 18(2):838. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020838
Chicago/Turabian StyleJackson, Jacklyn Kay, Jannah Jones, Hanh Nguyen, Isabella Davies, Melanie Lum, Alice Grady, and Sze Lin Yoong. 2021. "Obesity Prevention within the Early Childhood Education and Care Setting: A Systematic Review of Dietary Behavior and Physical Activity Policies and Guidelines in High Income Countries" International Journal of Environmental Research and Public Health 18, no. 2: 838. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020838