Effects of an African Circle Dance Programme on Internally Displaced Persons with Depressive Symptoms: A Quasi-Experimental Study


Abstract
:1. Introduction
2. Methods
2.1. Ethical Considerations
2.2. Participants
2.3. Interventions
2.3.1. Development of Psychoeducation Talks
2.3.2. Development of the ACD Dance Protocol
2.3.3. Intervention Group
2.3.4. Control Group
2.3.5. Trial Process
2.4. Objective
2.5. Outcomes
2.6. Sample Size
2.7. Assignment Methods
2.8. Blinding
2.9. Unit of Analysis
2.10. Statistical Methods
- (1)
- Demographic variables that are known to be associated with dependent variables in the literature (i.e., age, gender, education, marital status, and employment) [74], and
- (2)
- Outcome variables (i.e., depression, anxiety, and stress) that were not balanced between groups at baseline because they are known to be associated [75].
3. Results
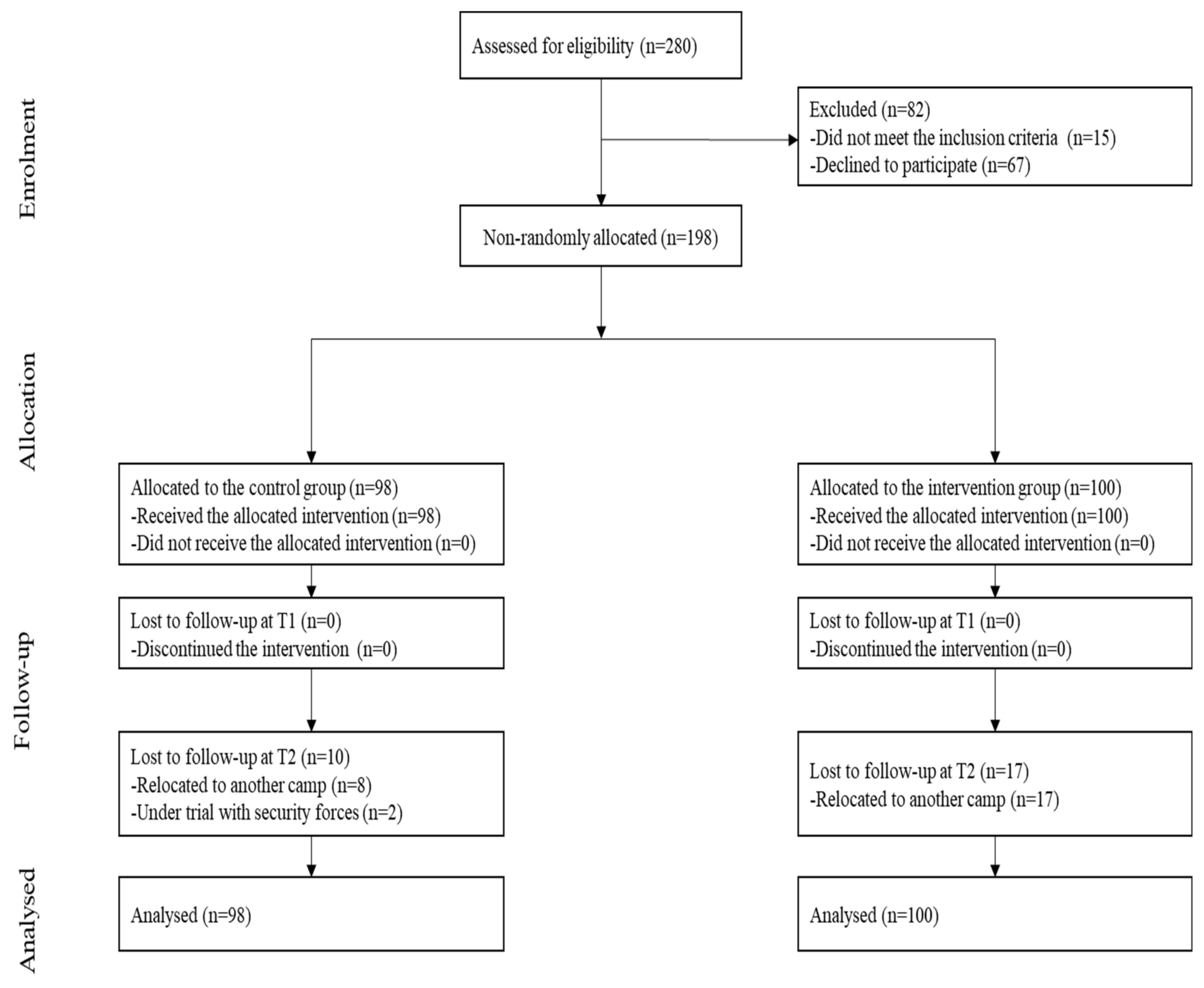
3.1. Participant Flow
3.2. Recruitment
3.3. Baseline Data
Demographic and Clinical Profiles at Baseline
3.4. Baseline Equivalence
3.5. Numbers Analysed
3.6. Outcomes and Estimation
Effects of the ACD Intervention
3.7. Adverse Events
4. Discussion
4.1. Interpretation
4.2. Generalizability
4.3. Overall Evidence
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mooney, E. The concept of internal displacement and the case for internally displaced persons as a category of concern. Refug. Surv. Q. 2005, 24, 9–26. [Google Scholar] [CrossRef]
- Internal Displacement Monitoring Centre Webpage. Global Report on Internal Displacement. Available online: https://www.internal-displacement.org/global-report/grid2020/ (accessed on 25 November 2020).
- Owoaje, E.; Uchendu, O.; Ajayi, T.; Cadmus, E. A review of the health problems of the internally displaced persons in Africa. Niger. Postgrad. Med J. 2016, 23, 161–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamid, A.A.; Musa, S.A. Mental health problems among internally displaced persons in Darfur. Int. J. Psychol. 2010, 45, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Martinec, R. Dance movement therapy in the wider concept of trauma rehabilitation. J. Trauma Rehabil. 2018, 1, 2. [Google Scholar]
- Makwana, N. Disaster and its impact on mental health: A narrative review. J. Fam. Med. Prim. Care 2019, 8, 3090–3095. [Google Scholar] [CrossRef]
- Bohnet, H.; Cottier, F.; Hug, S. Conflict-induced IDPs and the Spread of Conflict. J. Confl. Resolut 2018, 62, 691–716. [Google Scholar] [CrossRef] [Green Version]
- Kamara, J.K.; Cyril, S.; Renzaho, A.M.N. The social and political dimensions of internal displacement in Uganda: Challenges and opportunities-a systematic review. Afr. Stud. 2017, 76, 444–473. [Google Scholar] [CrossRef]
- Manea, L.M.S.; Gilbody, S.P.D.; McMillan, D.P.D. A diagnostic meta-analysis of the Patient Health Questionnaire-9 (PHQ-9) algorithm scoring method as a screen for depression. Gen. Hosp. Psychiat. 2015, 37, 67–75. [Google Scholar] [CrossRef]
- Tafet, G.E.; Nemeroff, C.B. The Links Between Stress and Depression: Psychoneuroendocrinological, Genetic, and Environmental Interactions. J. Neuropsychiatry Clin. N. 2016, 28, 77–88. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.; Khan, R.A. Chronic stress leads to anxiety and depression. Ann. Psychiatry Ment. Health 2017, 5, 1091. [Google Scholar]
- Morina, N.; Akhtar, A.; Barth, J.; Schnyder, U. Psychiatric disorders in refugees and internally displaced persons after forced displacement: A systematic review. Front. Psychiatry 2018, 9, 433. [Google Scholar] [CrossRef] [PubMed]
- Thapa, S.B.; Hauff, E. Psychological distress among displaced persons during an armed conflict in Nepal. Soc. Psychiatry Epidemiol. 2005, 40, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Henderson, J.; Henderson, G.; Lavikainen, J.; McDaid, D. Actions against Depression: Improving Mental Health and Well Being by Combating the Adverse Health, Social and Economic Consequences of Depression; Commission of the European Communities, Health and Consumer Protection Directorate: Luxembourgh, 2004; Available online: http://eprints.lse.ac.uk/id/eprint/13833 (accessed on 15 December 2020).
- Elias, A.K.; Georgia, L.; Malone, D.A., Jr. Side effects of antidepressants: An overview. Clevel Clin. J. Med. 2006, 73, 351–361. [Google Scholar] [CrossRef]
- Haviland, M.G.; MacMurray, J.P.; Cummings, M.A. The relationship between alexithymia and depressive symptoms in a sample of newly abstinent alcoholic inpatients. Psychother. Psychosom. 1988, 49, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Kandola, A.; Ashdown-Franks, G.; Hendrikse, J.; Sabiston, C.M.; Stubbs, B. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav. Rev. 2019, 107, 525–539. [Google Scholar] [CrossRef] [PubMed]
- Rebar, A.L.; Stanton, R.; Geard, D.; Short, C.; Duncan, M.J.; Vandelanotte, C. A meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health Psychol. Rev. 2015, 9, 366–378. [Google Scholar] [CrossRef] [PubMed]
- Bolton, P.; Bass, J.; Betancourt, T.; Speelman, L.; Onyango, G.; Clougherty, K.F.; Neugebauer, R.; Murray, L.; Verdeli, H. Interventions for Depression Symptoms Among Adolescent Survivors of War and Displacement in Northern Uganda: A Randomized Controlled Trial. JAMA-J. Am. Med. Assoc. 2007, 298, 519–527. [Google Scholar] [CrossRef] [Green Version]
- Sonderegger, R.; Rombouts, S.; Ocen, B.; McKeever, R.S. Trauma rehabilitation for war-affected persons in northern Uganda: A pilot evaluation of the EMPOWER programme. Br. J. Clin. Psychol. 2011, 50, 234–249. [Google Scholar] [CrossRef]
- Sit, H.F.; Ling, R.; Lam, A.I.F.; Chen, W.; Latkin, C.A.; Hall, B.J. The Cultural Adaptation of Step-by-Step: An intervention to address depression among Chinese young adults. Front. Psychiatry 2020, 11, 650. [Google Scholar] [CrossRef]
- Catalan-Matamoros, D.; Gomez-Conesa, A.; Stubbs, B.; Vancampfort, D. Exercise improves depressive symptoms in older adults: An umbrella review of systematic reviews and meta-analyses. Psychiatry Res. 2016, 244, 202–209. [Google Scholar] [CrossRef]
- Carter, T.; Morres, I.D.; Meade, O.; Callaghan, P. The effect of exercise on depressive symptoms in adolescents: A systematic review and meta-analysis. J. Am. Acad. Child. Adolesc. Psychiatry 2016, 55, 580–590. [Google Scholar] [CrossRef] [PubMed]
- Krogh, J.; Hjorthøj, C.; Speyer, H.; Gluud, C.; Nordentoft, M. Exercise for patients with major depression: A systematic review with meta-analysis and trial sequential analysis. BMJ Open 2017, 7, e014820. [Google Scholar] [CrossRef]
- Adamson, B.C.M.S.; Ensari, I.E.; Motl, R.W.P. Effect of Exercise on Depressive Symptoms in Adults With Neurologic Disorders: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehab. 2015, 96, 1329–1338. [Google Scholar] [CrossRef] [PubMed]
- Morres, I.D.; Hatzigeorgiadis, A.; Stathi, A.; Comoutos, N.; Arpin-Cribbie, C.; Krommidas, C.; Theodorakis, Y. Aerobic exercise for adult patients with major depressive disorder in mental health services: A systematic review and meta-analysis. Depress. Anxiety 2019, 36, 39–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glowacki, K.; Duncan, M.J.; Gainforth, H.; Faulkner, G. Barriers and facilitators to physical activity and exercise among adults with depression: A scoping review. Ment. Health Phys. Act. 2017, 13, 108–119. [Google Scholar] [CrossRef]
- Jancey, J.; Lee, A.; Howat, P.; Clarke, A.; Wang, K.; Shilton, T. Reducing Attrition in Physical Activity Programs for Older Adults. J. Aging Phys. Act. 2007, 15, 152–165. [Google Scholar] [CrossRef]
- Van Daele, T.; Hermans, D.; Van Audenhove, C.; Van den Bergh, O. Stress reduction through psychoeducation: A meta-analytic review. Health Educ. Behav. 2012, 39, 474–485. [Google Scholar] [CrossRef] [Green Version]
- Meekums, B.; Karkou, V.; Nelson, E.A. Dance movement therapy for depression. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [Green Version]
- Duberg, A.; Möller, M.; Sunvisson, H. “I feel free”: Experiences of a dance intervention for adolescent girls with internalizing problems. Int. J. Qual. Stud. Heal. 2016, 11, 31946. [Google Scholar] [CrossRef]
- Karampoula, E.; Panhofer, H. The circle in dance movement therapy: A literature review. Arts Psychother. 2018, 58, 27–32. [Google Scholar] [CrossRef]
- Phibion, O.S.; Aedige, T.N. The Basarwa melon throwing circle dance (Siqciru/Sigcuru): The case of Kaudwane village in Kweneng West District of Botswana. J. Music Danc. 2019, 9, 1–5. [Google Scholar]
- Abiola, O. A Historical, Theoretical, and Cultural Analysis of Africana Dance and Theatre. Evoke 2019, 1, 1. [Google Scholar]
- Schwender, T.M.; Spengler, S.; Oedl, C.; Mess, F. Effects of dance interventions on aspects of the participants’ self: A systematic review. Front. Psychol. 2018, 9, 1130. [Google Scholar] [CrossRef] [PubMed]
- Murrock, C.J.; Graor, C.H. Depression, Social Isolation, and the Lived Experience of Dancing in Disadvantaged Adults. Arch. Psychiatr. Nurs. 2016, 30, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, N.M.; Wall, D.J. African Dance as Healing Modality Throughout the Diaspora: The Use of Ritual and Movement to Work Through Trauma. J. Pan Afr. Stud. 2011, 4, 234–252. [Google Scholar]
- Folkman, S.; Lazarus, R.S. Stress, Appraisal, and Coping; Springer Publishing Company: New York, NY, USA, 1984. [Google Scholar]
- Martin, L.; Oepen, R.; Bauer, K.; Nottensteiner, A.; Mergheim, K.; Gruber, H.; Koch, S.C. Creative arts interventions for stress management and prevention-a systematic review. Behav. Sci. 2018, 8, 28. [Google Scholar] [CrossRef] [Green Version]
- Bendel-Rozow, T. Recovery-Oriented Dance Movement Therapy: A Controlled Trial in Mental Health Rehabilitation. Ph.D. Thesis, Lesley University, Cambridge, MA, USA, 2020. [Google Scholar]
- Daviu, N.; Bruchas, M.R.; Moghaddam, B.; Sandi, C.; Beyeler, A. Neurobiological links between stress and anxiety. Neurobiol. Stress. 2019, 11, 100191. [Google Scholar] [CrossRef]
- Hatfield, A.B.; Lefley, H.P. Families of the Mentally Ill: Coping and Adaptation; Guilford Press: New York, NY, USA, 1987. [Google Scholar]
- Goodman, R. Contemporary Trauma Theory and Trauma-Informed Care in Substance Use Disorders: A Conceptual Model for Integrating Coping and Resilience. Adv. Soc. Work. 2017, 18, 186–201. [Google Scholar] [CrossRef]
- Al-Sulaiman, R.J.; Bener, A.; Doodson, L.; Al Bader, S.B.; Ghuloum, S.; Lemaux, A.; Bugrein, H.; Alassam, R.; Karim, A. Exploring the effectiveness of crisis counseling and psychoeducation in relation to improving mental well-being, quality of life and treatment compliance of breast cancer patients in Qatar. Int. J. Womens Health 2018, 10, 285–298. [Google Scholar] [CrossRef] [Green Version]
- Hindi, F.S. How attention to interoception can inform dance/movement therapy. Am. J. Dance Ther. 2012, 34, 129–140. [Google Scholar] [CrossRef]
- Dieterich-Hartwell, R. Dance/movement therapy in the treatment of post traumatic stress: A reference model. Arts Psychother. 2017, 54, 38–46. [Google Scholar] [CrossRef]
- Vrinceanu, T.; Esmail, A.; Berryman, N.; Predovan, D.; Vu, T.T.M.; Villalpando, J.M.; Pruessner, J.C.; Bherer, L.J.S. Dance your stress away: Comparing the effect of dance/movement training to aerobic exercise training on the cortisol awakening response in healthy older adults. Stress 2019, 22, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Duberg, A.; Jutengren, G.; Hagberg, L.; Möller, M. The effects of a dance intervention on somatic symptoms and emotional distress in adolescent girls: A randomized controlled trial. J. Int. Med. Res. 2020, 48, 300060520902610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuller, T.; Pearson, M.; Peters, J.L.; Anderson, R. Evaluating the impact and use of Transparent Reporting of Evaluations with Non-randomised Designs (TREND) reporting guidelines. BMJ Open 2012, 2, e002073. [Google Scholar] [CrossRef] [Green Version]
- Parkitny, L.; McAuley, J. The Depression Anxiety Stress Scale (DASS). J. Physiother. 2010, 56, 204. [Google Scholar] [CrossRef] [Green Version]
- Rosanna Chau, M.W.; Chan, S.P.; Wong, Y.W.; Lau, M.Y.P. Reliability and validity of the Modified Functional Ambulation Classification in patients with hip fracture. Hong Kong Physiother. J. 2013, 31, 41–44. [Google Scholar] [CrossRef] [Green Version]
- Turner, S. What Is a Refugee Camp? Explorations of the Limits and Effects of the Camp. J. Refug. Stud. 2016, 29, 139–148. [Google Scholar] [CrossRef]
- Displacement Tracking Matrix, International Organization for Migration Webpage. Nigeria—Teachers’ Village and Stadium Camp Biometric Registration Update. Available online: https://dtm.iom.int/reports/nigeria-%E2%80%94-teachers-village-and-stadium-camp-biometric-registration-update-april-2019 (accessed on 20 November 2019).
- Aluh, D.O.; Okoro, R.N.; Zimboh, A. The prevalence of depression and post-traumatic stress disorder among internally displaced persons in Maiduguri, Nigeria. JPMH 2019, 19, 19–168. [Google Scholar] [CrossRef]
- United Nations Office for the Coordination of Humanitarian Affairs Webpage. North-East Nigeria: Flash Update Fire at Muna Garageel-Badawe IDP Camp, Jere LGA, Borno State. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/OCHA_NGA_FlashUpdate_MunaGarageFireOutbreak_26052020.pdf (accessed on 15 November 2020).
- Donker, T.; Griffiths, K.M.; Cuijpers, P.; Christensen, H. Psychoeducation for depression, anxiety and psychological distress: A meta-analysis. BMC Med. 2009, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- National Health System Webpage. 10 Stress Busters. Available online: https://www.nhs.uk/conditions/stress-anxiety-depression/reduce-stress/ (accessed on 15 October 2019).
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Strassel, J.K.; Cherkin, D.C.; Steuten, L.; Sherman, K.J.; Vrijhoef, H.J. A systematic review of the evidence for the effectiveness of dance therapy. Altern. Health Med. 2011, 17, 50–59. [Google Scholar]
- Dauda, S.K.; Cho, R.Y.; Wong, E. The Effect of Dance Intervention on Stress in Adults Living with Depression: A Systematic Review. In Proceedings of the 23rd East. Asian Forum of Nursing Scholars: Advancing Nursing Scholars in the Era of Global Transformation and Disruptive Innovation, Chiang Mai, Thailand, 10–11 January 2020. [Google Scholar]
- Hsu, C.-C.; Sandford, B.A. The Delphi technique: Making sense of consensus. Pr. Assess. Res. Eval. 2007, 12, 10. [Google Scholar]
- Academic Invest Webpage. What is a dance specialist? Available online: https://www.academicinvest.com/arts-careers/dance-careers/what-is-a-dance-specialist (accessed on 20 November 2020).
- Salihu, D.; Wong, E.M.L.; Leung, D.Y.P. Depression Anxiety Stress Scale Hausa version (DASS-21 H). In Psychology Foundation of Australia; University of New South Wales: New South Wales, Australia; Available online: http://www2.psy.unsw.edu.au/Groups/Dass/Hausa/Hausa.htm (accessed on 17 October 2020).
- Beaufort, I.N.; De Weert-Van Oene, G.H.; Buwalda, V.A.; de Leeuw, J.R.J.; Goudriaan, A.E. The depression, anxiety and stress scale (DASS-21) as a screener for depression in substance use disorder inpatients: A pilot study. Eur. Addict. Res. 2017, 23, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Gomez, F.J.C. A guide to the depression, anxiety and stress scale (DASS 21). Cesphn 2016. [Google Scholar]
- Da Silva, H.A.; dos Passos, M.H.P.; de Oliveira, V.M.A.; Palmeira, A.C.; Pitangui, A.C.R.; Araújo, R.C. Short version of the Depression Anxiety Stress Scale-21: Is it valid for Brazilian adolescents? Einstein (São Paulo) 2016, 14, 486–493. [Google Scholar] [CrossRef] [Green Version]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Norton, P.J. Depression Anxiety and Stress Scales (DASS-21): Psychometric analysis across four racial groups. Anxiety Stress Coping 2007, 20, 253–265. [Google Scholar] [CrossRef]
- Gloster, A.T.; Rhoades, H.M.; Novy, D.; Klotsche, J.; Senior, A.; Kunik, M.; Wilson, N.; Stanley, M.A. Psychometric properties of the Depression Anxiety and Stress Scale-21 in older primary care patients. J. Affect. Disord. 2008, 110, 248–259. [Google Scholar] [CrossRef] [Green Version]
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychol. Assess 1998, 10, 176. [Google Scholar] [CrossRef]
- Kreidler, S.M.; Muller, K.E.; Grunwald, G.K.; Ringham, B.M.; Coker-Dukowitz, Z.T.; Sakhadeo, U.R.; Barón, A.E.; Glueck, D.H. Glimmpse: Online power computation for linear models with and without a baseline covariate. J. Stat. Softw. 2013, 54, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Pinniger, R.; Brown, R.F.; Thorsteinsson, E.B.; McKinley, P. Argentine tango dance compared to mindfulness meditation and a waiting-list control: A randomised trial for treating depression. Complement. Med. 2012, 20, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Suresh, K. An overview of randomization techniques: An unbiased assessment of outcome in clinical research. J. Hum. Reprod. Sci. 2011, 4, 8. [Google Scholar] [CrossRef] [PubMed]
- Akhtar-Danesh, N.; Landeen, J. Relation between depression and sociodemographic factors. Int. J. Ment. Health Syst. 2007, 1, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammen, C. Stress and depression. Annu. Rev. Clin. 2005, 1, 293–319. [Google Scholar] [CrossRef] [Green Version]
- Ialongo, C. Understanding the effect size and its measures. Biochem. Med. 2016, 26, 150–163. [Google Scholar] [CrossRef] [Green Version]
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Wang, C.; Paik, M.C. A weighting approach for GEE analysis with missing data. Commun. Stat. Theory Methods 2011, 40, 2397–2411. [Google Scholar] [CrossRef]
- West, J.; Otte, C.; Geher, K.; Johnson, J.; Mohr, D.C. Effects of hatha yoga and african dance on perceived stress, affect, and salivary cortisol. Ann. Behav. Med. 2004, 28, 114–118. [Google Scholar] [CrossRef]
- Everly, G.S.; Lating, J.M. The Anatomy and Physiology of the Human Stress Response; Springer: New York, NY, USA, 2019; pp. 19–56. [Google Scholar]
- Koch, S.C. Arts and health: Active factors and a theory framework of embodied aesthetics. ArtS Psychother. 2017, 54, 85–91. [Google Scholar] [CrossRef]
- Kattenstroth, J.-C.; Kolankowska, I.; Kalisch, T.; Dinse, H.R. Superior sensory, motor, and cognitive performance in elderly individuals with multi-year dancing activities. Front. Aging Neurosci. 2010, 2. [Google Scholar] [CrossRef] [Green Version]
- Wiedenhofer, S.; Hofinger, S.; Wagner, K.; Koch, S.C. Active Factors in Dance/Movement Therapy: Health Effects of Non-Goal-Orientation in Movement. Am. J. Danc. Ther. 2017, 39, 113–125. [Google Scholar] [CrossRef]
- Schmalzl, L.; Crane-Godreau, M.A.; Payne, P. Movement-based embodied contemplative practices: Definitions and paradigms. Front. Hum. Neurosci. 2014, 8, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sphere, P. Humanitarian Charter and Minimum Standards in Humanitarian Response, 3rd ed.; Sphere Project: Geneva, Switzerland, 2011. [Google Scholar]
- Shin, L.M.; Liberzon, I. The Neurocircuitry of Fear, Stress, and Anxiety Disorders. Neuropsychopharmacology 2010, 35, 169–191. [Google Scholar] [CrossRef] [PubMed]
- Vehovar, V.; Toepoel, V.; Steinmetz, S. Non-probability sampling. In The Sage Handbook Survey Methods; SAGE: New York, NY, USA, 2016; pp. 329–345. [Google Scholar]
- Vickers, A.J.; Altman, D.G. Analysing controlled trials with baseline and follow up measurements. BMJ 2001, 323, 1123. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Time | Session Name | Contents |
|---|---|---|
| Psychoeducation (60-min) | ||
| 5 min | Check-in session | Self-introduction, activity introduction |
| 40 min | Education session | Lecture on facts relating to the psychological effect of stress, how to cope in an IDP camp, resources available in the IDP camp, and coping skills depicted on the “10 stress Busters” [57]. |
| 5 min | Clarification session | Answer questions raised by the participants |
| 10 min | Oral quiz session | Evaluate the participants’ knowledge |
| Dance intervention (75-min) | ||
| 5 min | Check-in session | Self-introduction, activity introduction |
| 10 min | Warm-up session | Preparation for the dance |
| 50 min | ACD session | Dance exercise under the teaching and supervision of a dance specialist |
| 10 min | Cool-down session | Preparation to end the dance |
| Tasks | Baseline | Treatment Phase | Follow-Up | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Week | ||||||||||
| −2 to 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 to 12 | |
| Informed consent | X | |||||||||
| Obtain participant’s Assent | X | |||||||||
| Intervention | ||||||||||
| ACD Dance | X | X | X | X | X | X | X | X | ||
| Psychoeducation | X | X | ||||||||
| Control | ||||||||||
| Psychoeducation | X | X | ||||||||
| Outcomes | ||||||||||
| #Depression | X | X | X | |||||||
| #Anxiety | X | X | X | |||||||
| #Stress | X | X | X | |||||||
| Process monitoring | ||||||||||
| Compliance | X | X | X | X | X | X | X | X | ||
| Reasons for withdrawal | X | X | X | X | X | X | X | X | ||
| Adverse events/safety | X | X | X | X | X | X | X | X | ||
| Participants’ Characteristics | All (n = 198) | Control (n = 98) | Intervention (n = 100) | p-Value |
|---|---|---|---|---|
| Age, n (%) | ||||
| 18–29 years | 102 (51.5) | 60 (61.2) | 42 (42.0) | 0.195 |
| 30–49 years | 80 (40.4) | 32 (32.7) | 48 (48.0) | |
| 50 years above | 16 (8.1) | 6 (6.1) | 10 (10.0) | |
| Gender, n (%) | 0.582 | |||
| Male | 71 (35.9) | 37 (37.8) | 34 (34.0) | |
| Female | 127 (64.1) | 61 (62.2) | 66 (66.0) | |
| Education, n (%) | ||||
| No formal education | 147 (74.2) | 65 (66.3) | 82 (82.0) | 0.038 * |
| Primary education | 19.0 (9.6) | 13 (13.3) | 6 (6.0) | |
| High school or above | 32.0 (16.2) | 20 (20.4) | 12 (12.0) | |
| Marital status, n (%) | <0.001 ** | |||
| Married | 114 (57.6) | 49 (50.0) | 65 (65.0) | |
| Widowed | 25 (12.6) | 9 (9.2) | 16 (16.0) | |
| Divorced | 22 (11.1) | 10 (10.2) | 12 (12) | |
| Never married | 37 (18.7) | 30 (30.6) | 7 (7.0) | |
| Employment, n (%) | 0.174 | |||
| Employed | 8 (4.0) | 5 (5.1) | 3 (3.0) | |
| Unemployed | 184 (93.0) | 88 (89.8) | 96 (96.0) | |
| Retired | 6 (3.0) | 5 (5.1) | 1 (1.0) | |
| Anti-depressant, n (%) | 0.774 | |||
| Yes | 19 (9.6) | 10 (10.2) | 9 (9.0) | |
| No | 179 (90.4) | 88 (89.8) | 91 (91.0) | |
| Retired | 6 (3.0) | 5 (5.1) | 1 (1.0) | |
| DASS-21, mean (SD) | ||||
| Depression | 26.5 (4.1) | 25.2 (3.6) | 27.7 (4.2) | <0.001 ** |
| Anxiety | 23.4 (6.9) | 23.2 (8.1) | 23.6 (5.6) | 0.645 |
| Stress | 21.5 (6.5) | 21.8 (6.8) | 21.2 (6.1) | 0.532 |
| Variables | Time | Control (n = 98) Mean (SE) | Intervention (n = 100) Mean (SE) | GxT Interaction Effects β (95% CI) | p-Value |
|---|---|---|---|---|---|
| Depressive symptoms—Unadjusted | |||||
| T0 | 25.2 (0.4) | 27.7 (0.4) | |||
| T1 | 13.8 (0.7) * | 9.7 (0.7) * | −6.6 (−8.73, −4.41) | <0.001 | |
| T2 | 12.7 (0.8) * | 11.6 (0.4) * | −3.5 (−5.51, −1.47) | 0.001 | |
| Depressive symptoms—Adjusted | |||||
| T0 | 24.8 (2.7) | 26.1 (2.6) | |||
| T1 | 13.4 (2.7) * | 8.1 (2.7) * | −6.6 (−8.73, −4.41) | <0.001 | |
| T2 | 12.3 (2.7) * | 10.2 (2.8) * | −3.4 (−5.46, −1.39) | 0.001 | |
| Anxiety—Unadjusted | |||||
| T0 | 23.2 (0.8) | 23.6 (0.6) | |||
| T1 | 13.9 (0.8) * | 15.8 (0.7) * | 1.4 (−1.53, 4.26) | 0.355 | |
| T2 | 12.4 (0.8) * | 14.9 (0.6) * | 2.0 (−0.74, 4.71) | 0.153 | |
| Anxiety—Adjusted | |||||
| T0 | 21.3 (4.4) | 21.5 (4.3) | |||
| T1 | 12.1 (4.5) * | 13.6 (4.3) * | 1.4 (−1.53, 4.26) | 0.355 | |
| T2 | 10.5 (4.5) * | 12.7 (4.4) * | 2.0 (−0.69, 4.75) | 0.143 | |
| Stress—Unadjusted | |||||
| T0 | 21.8 (0.7) | 21.2 (0.6) | |||
| T1 | 5.5 (0.3) * | 3.0 (0.3) * | −1.9 (−3.94, 0.11) | 0.064 | |
| T2 | 9.6 (0.5) * | 5.7 (0.4) * | −3.3 (−5.46, −1.15) | 0.003 | |
| Stress—Adjusted | |||||
| T0 | 21.4 (3.6) | 20.5 (3.7) | |||
| T1 | 5.2 (3.6) * | 2.6 (3.5) * | −1.9 (−3.94, 0.11) | 0.064 | |
| T2 | 9.3 (3.6) * | 5.3 (3.6) * | −3.3 (−5.45, −1.14) | 0.003 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salihu, D.; Wong, E.M.L.; Kwan, R.Y.C. Effects of an African Circle Dance Programme on Internally Displaced Persons with Depressive Symptoms: A Quasi-Experimental Study. Int. J. Environ. Res. Public Health 2021, 18, 843. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020843
Salihu D, Wong EML, Kwan RYC. Effects of an African Circle Dance Programme on Internally Displaced Persons with Depressive Symptoms: A Quasi-Experimental Study. International Journal of Environmental Research and Public Health. 2021; 18(2):843. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020843
Chicago/Turabian StyleSalihu, Dauda, Eliza M. L. Wong, and Rick Y. C. Kwan. 2021. "Effects of an African Circle Dance Programme on Internally Displaced Persons with Depressive Symptoms: A Quasi-Experimental Study" International Journal of Environmental Research and Public Health 18, no. 2: 843. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020843