
An Updated Meta-Analysis of Remote Blood Pressure Monitoring in Urban-Dwelling Patients with Hypertension




Abstract
:1. Introduction
2. Materials and Methods
2.1. Searching for Eligible Studies
2.2. Inclusion and Exclusion Criteria
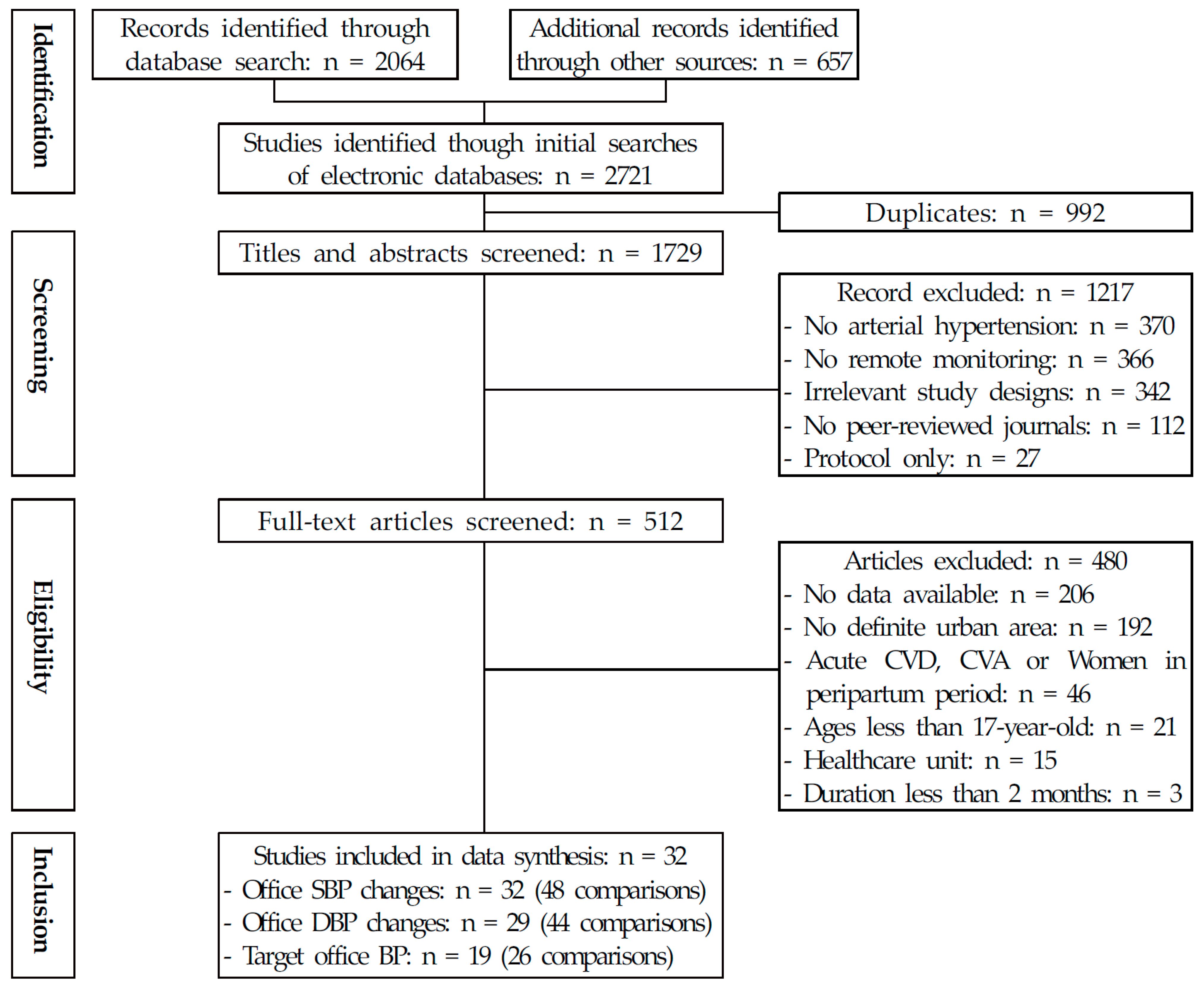
2.3. Study Selection
2.4. Data Extraction and Coding
2.5. Quality Assessment and Publication Bias
2.6. Statistical Analysis
3. Results
3.1. Study Characteristics
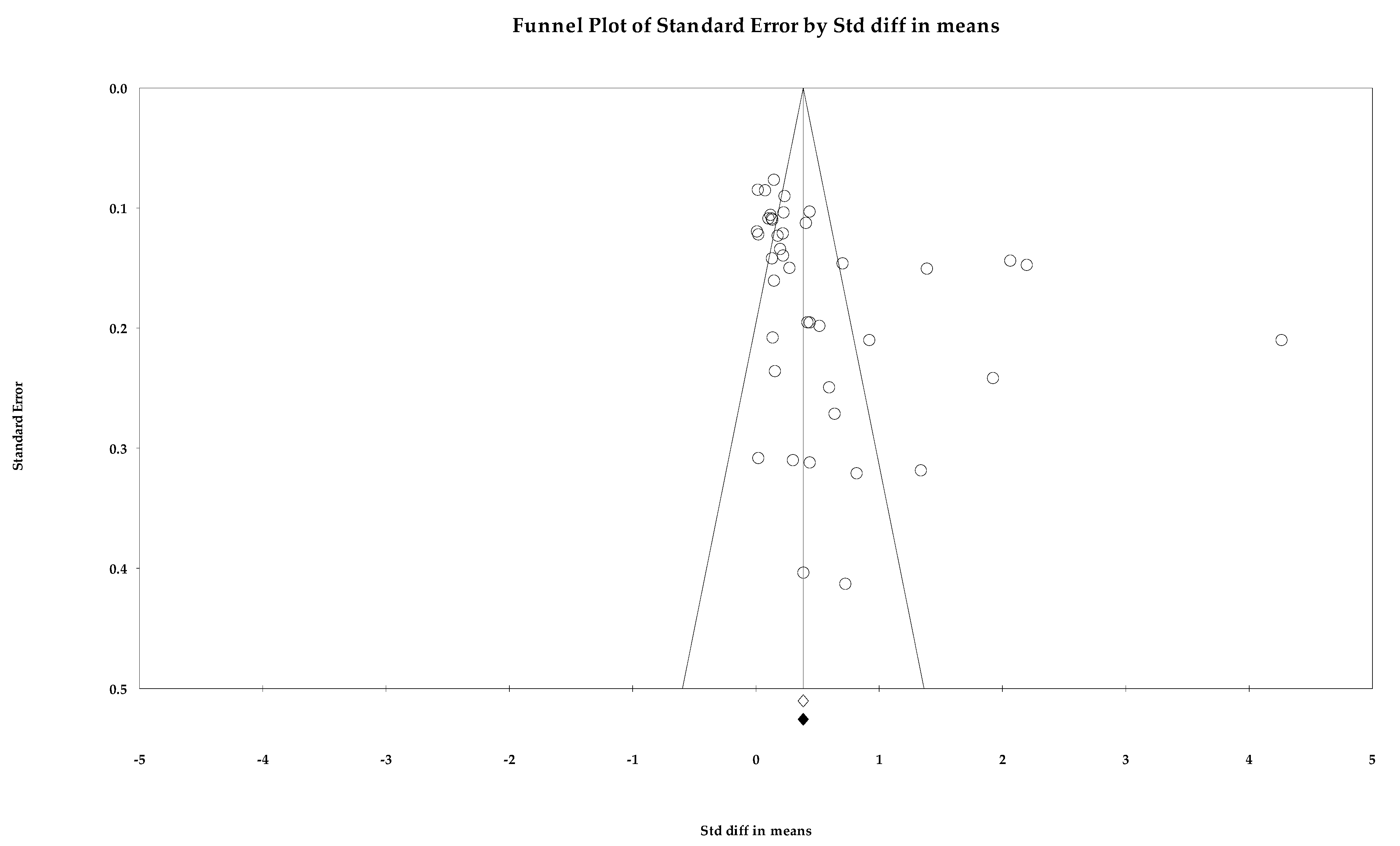
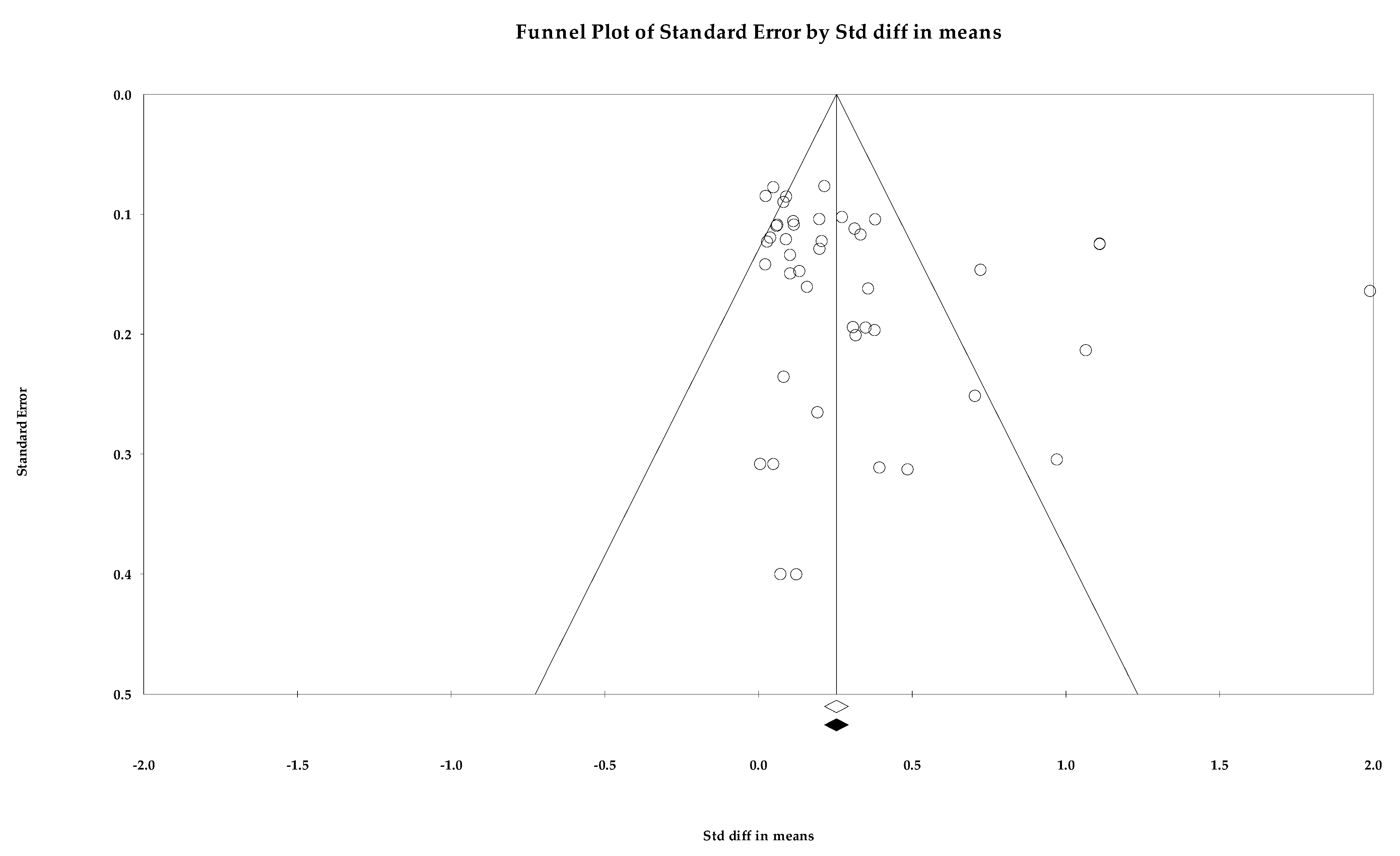
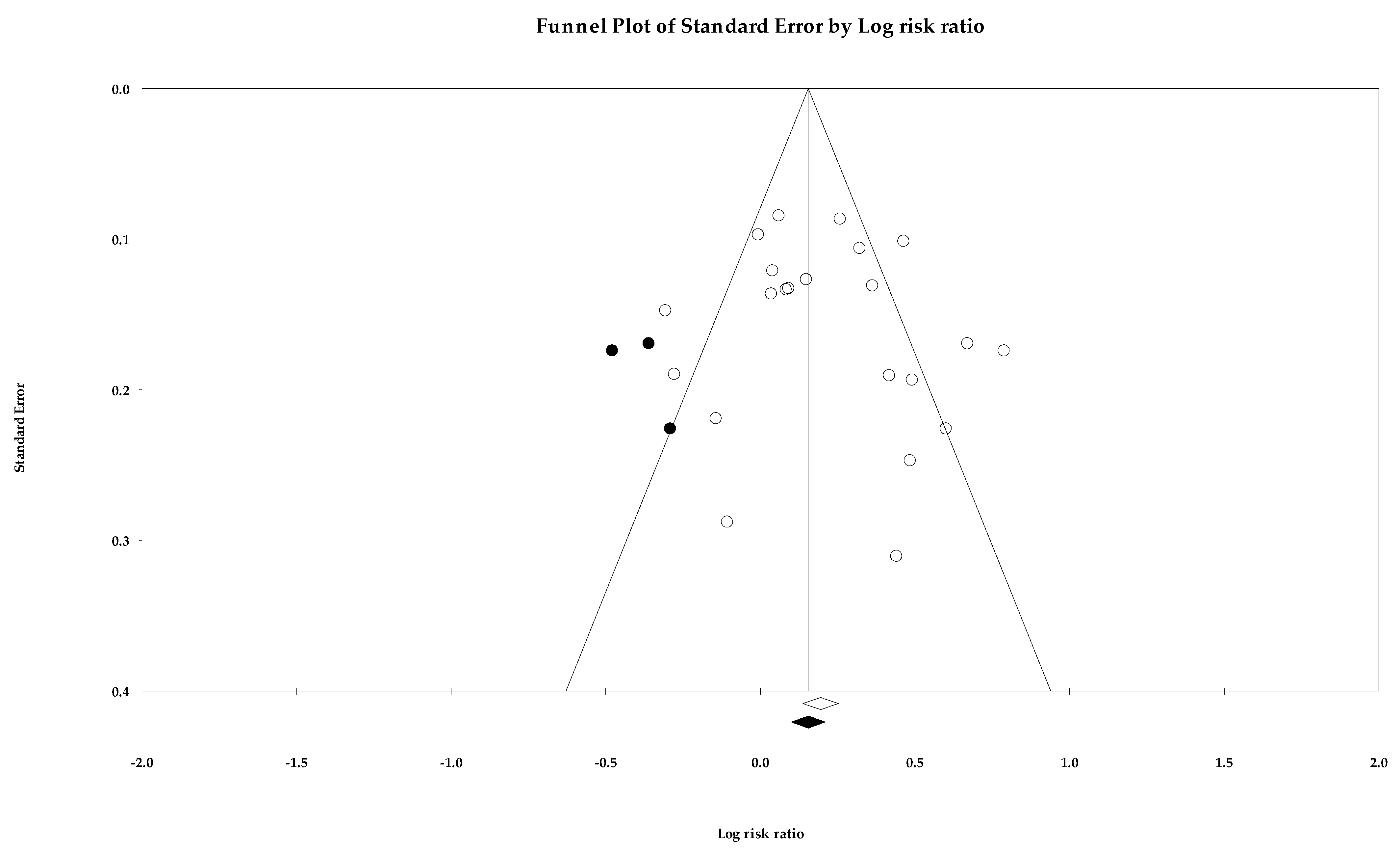
3.2. Risk Assessment
3.3. Primary Outcomes
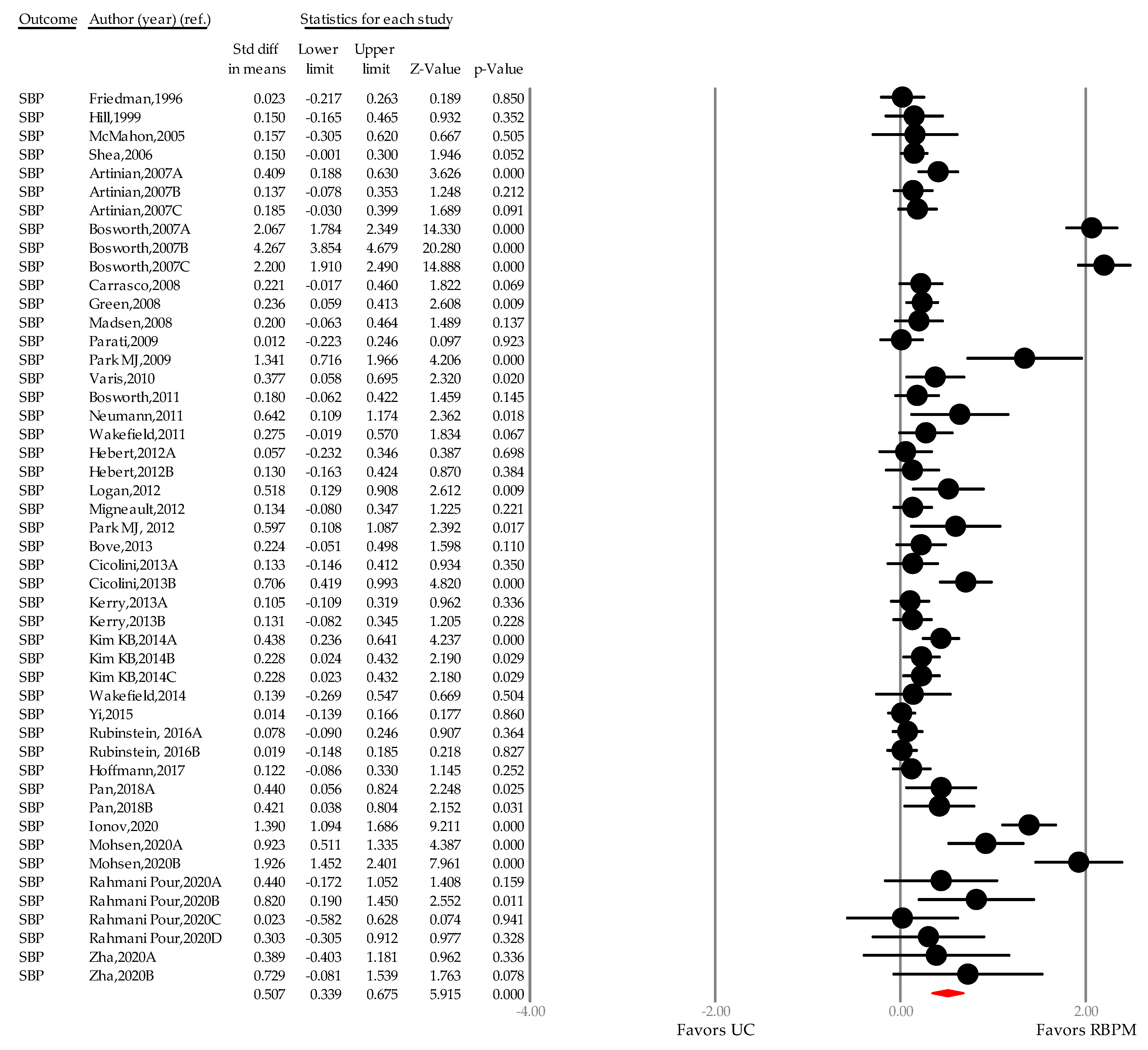
3.3.1. Systolic Blood Pressure
3.3.2. Diastolic Blood Pressure
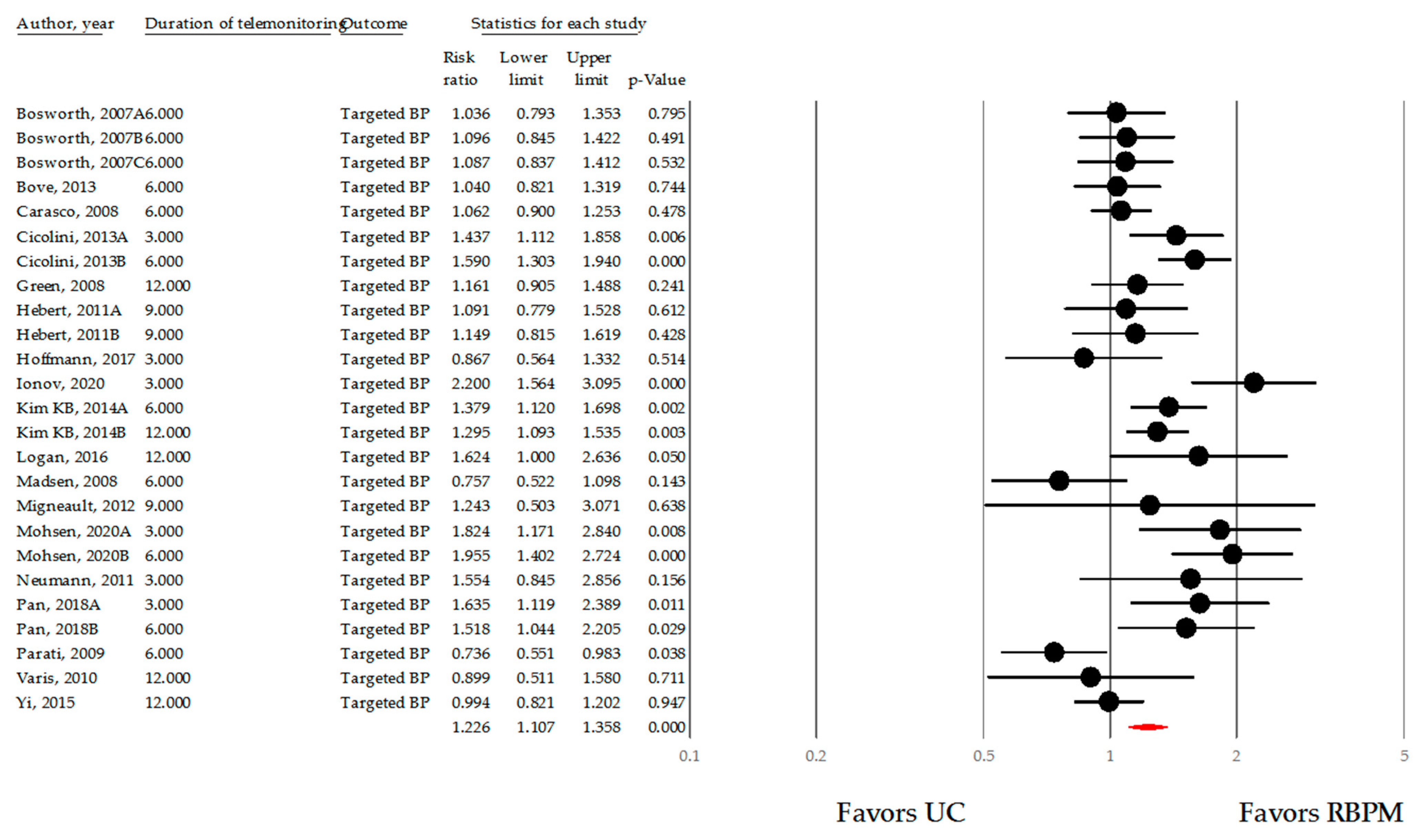
3.3.3. Target Blood Pressure Rate
3.4. Subgroup Analysis
3.4.1. City Size
3.4.2. Medically Underserved Areas
3.4.3. Duration of Intervention
3.4.4. Setting
3.4.5. Frequency of Remote Transmission of Blood Pressure Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Searching Strategy via Cochrane Library
- MeSH descriptor: [Hypertension] explode all trees
- hypertensi* OR high blood pressure
- OR/1,2
- MeSH descriptor: [Urban population] explode all trees
- MeSH descriptor: [Urban health] explode all trees urban health [Mesh]
- MeSH descriptor: [Urban health services] explode all trees
- MeSH descriptor: [Cities] explode all trees
- urban* OR city OR cities OR central cit*
- OR/4–8
- AND/3,10
- MeSH descriptor: [Telemedicine] explode all trees
- MeSH descriptor: [Telemetry] explode all trees
- MeSH descriptor: [Blood pressure monitoring, ambulatory] explode all trees
- telemedicine OR telemetry OR telenurs* OR telemonitor* OR eHealth OR telehealth OR remote monitor* OR technolog* OR telephone OR smartphone OR internet
- OR/12–15
- AND/11,16
- randomised controlled trial OR randomized controlled
- controlled clinical trial
- randomised [tiab] OR randomized [tiab]
- 2placebo [tiab]
- drug therapy [sh]
- groups [tiab]
- clinical trials as topic [tiab]
- randomly [tiab]
- trial [tiab]
- OR/18–26
- 27 NOT cluster randomized controlled trials
- 28 NOT cross over study
- AND/17,29
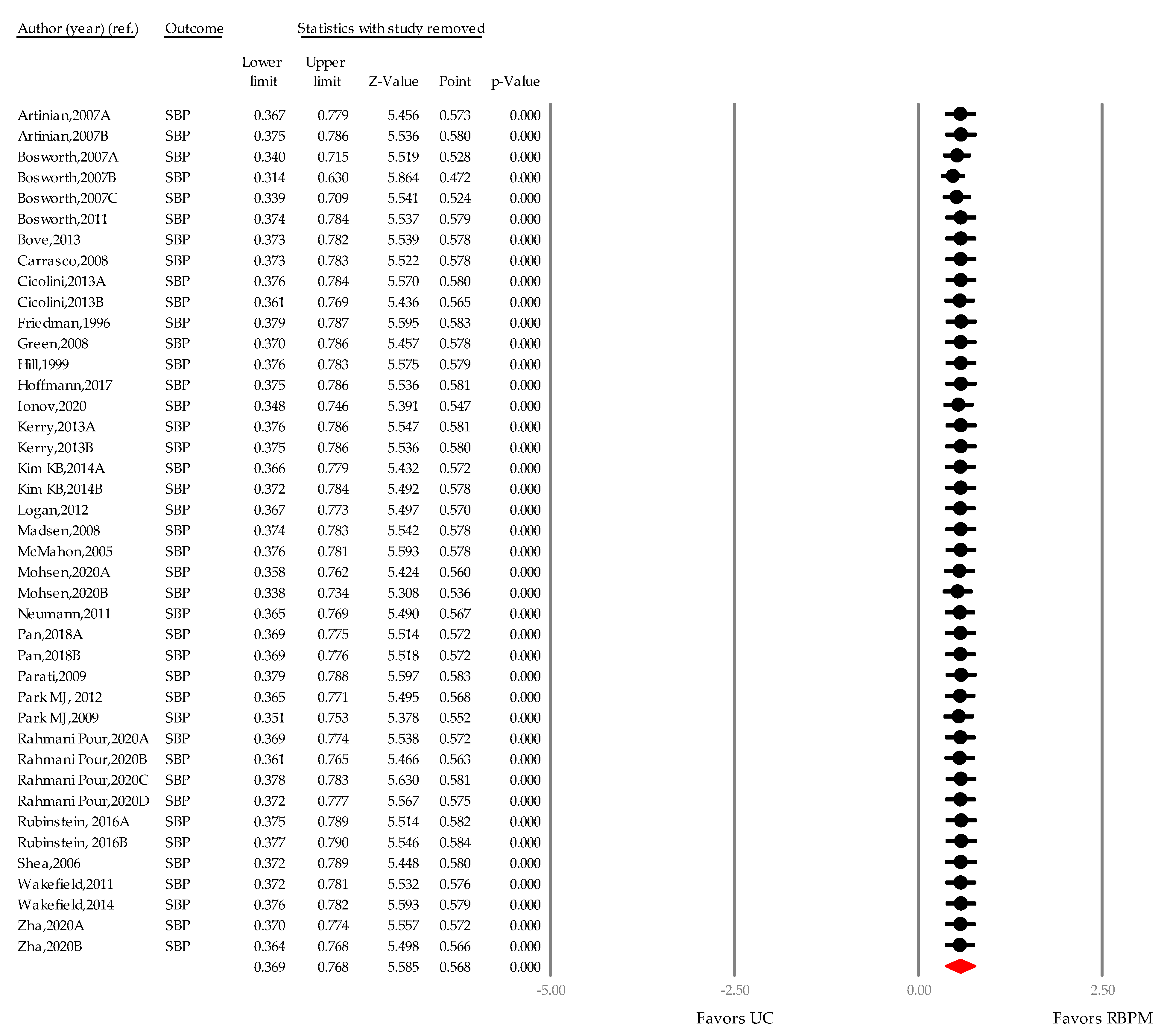
Appendix B. Sensitivity Test Based on a “One-Study Removed” Approach

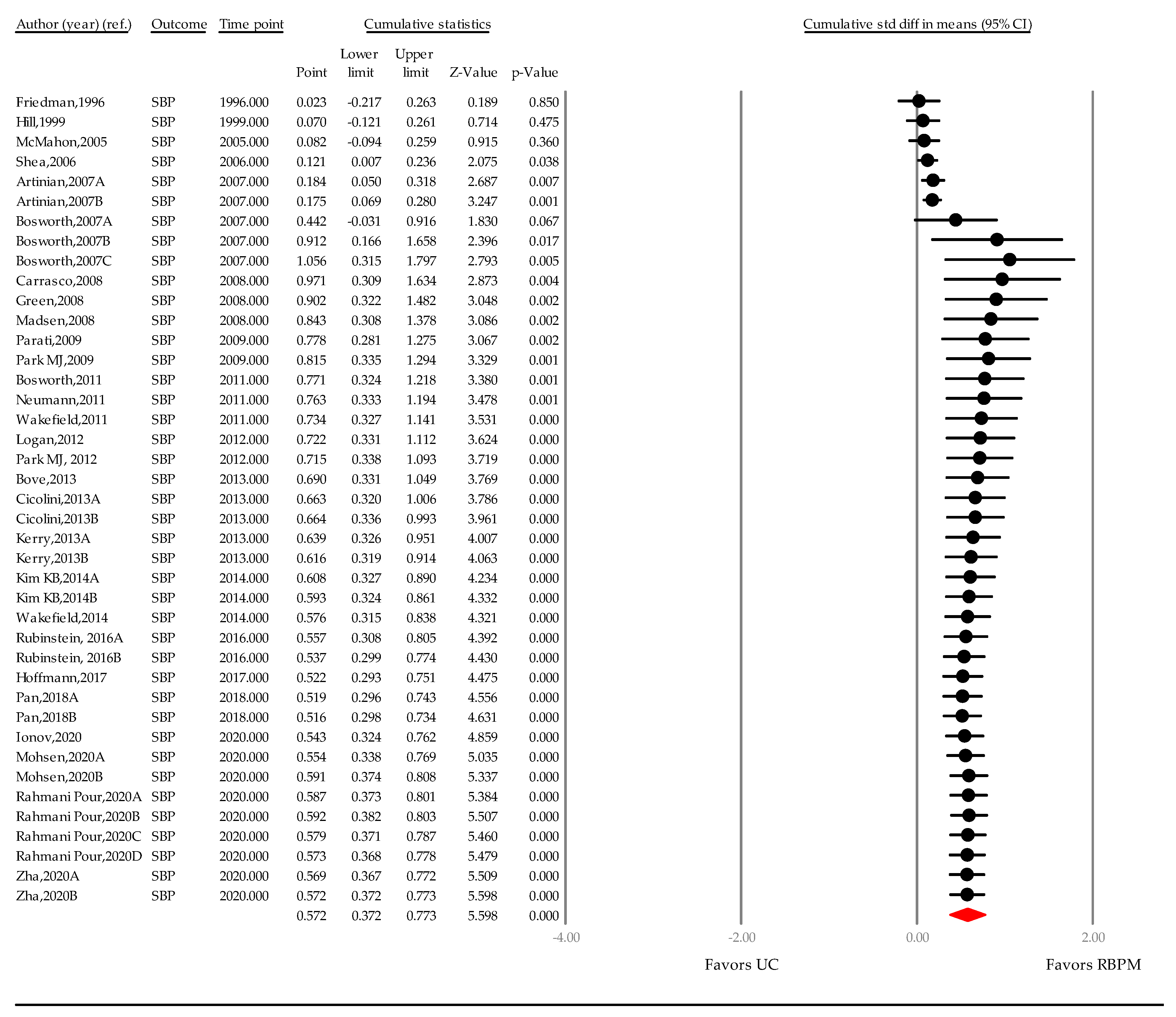
Appendix C. Cumulative Meta-Analysis of RBPM According to the SMD of SBP

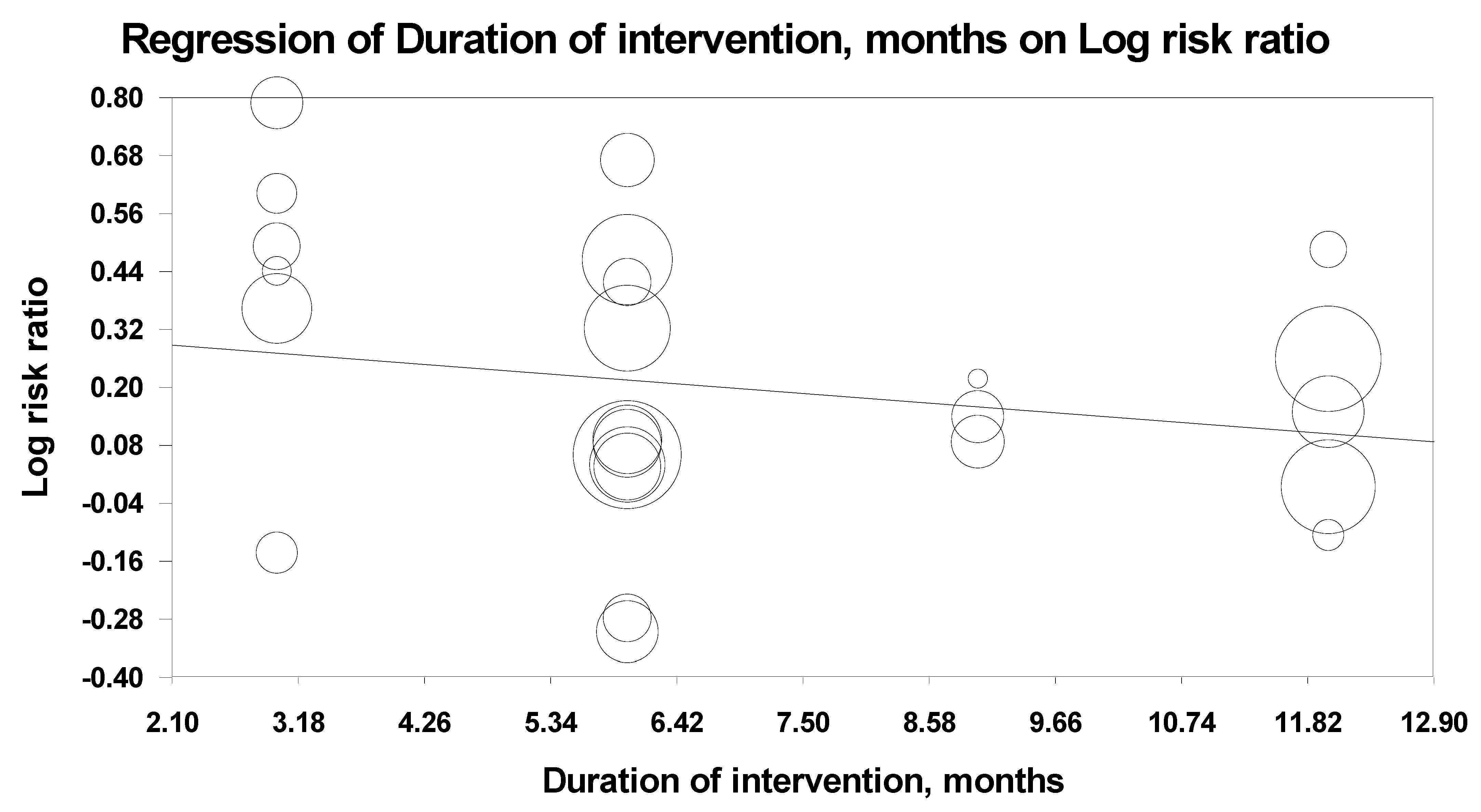
Appendix D. Meta-Regression of Risk Ratio According to RBPM Duration

Appendix E. Subgroup Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Number of Studies | Summary WMD of SBP, mmHg (95% CI) | Heterogeneity, I2 (%) Using an FEM (p-Value) | Heterogeneity, Tau-Squared (τ2) Using an FEM |
|---|---|---|---|---|
| Overall | 48 | 4.464 (3.371–5.556) | 70.908 (p < 0.001) | 9.200 |
| City size (population) | ||||
| <1 million | 22 | 3.860 (2.271–5.450) | 0.000 (p = 0.478) | 0.000 |
| >1 million | 26 | 5.056 (3.503–6.609) | 82.177 (p < 0.001) | 17.368 |
| Medically underserved areas | ||||
| Underserved | 17 | 3.213 (1.521–4.905) | 48.904 (p = 0.012) | 2.793 |
| Not underserved | 31 | 5.224 (3.878–6.569) | 73.152 (p < 0.001) | 12.943 |
| Duration (month) | ||||
| ≤3 | 15 | 6.198 (4.019–8.377) | 70.060 (p < 0.001) | 14.069 |
| 6 | 14 | 4.479 (2.524–6.433) | 84.562 (p < 0.001) | 17.240 |
| 9 | 4 | 2.116 (-1.816–6.048) | 0.000 (p = 0.752) | 0.000 |
| 12 | 12 | 3.436 (1.281–5.591) | 34.656 (p = 0.113) | 1.646 |
| Setting | ||||
| Primary care clinic | 14 | 2.981 (1.323–4.639) | 45.243 (p = 0.034) | 1.989 |
| Community health center | 12 | 3.512 (1.651–5.373) | 31.670 (p = 0.138) | 1.883 |
| Hospital | 22 | 6.333 (4.750–7.917) | 73.401 (p < 0.001) | 17.133 |
| Frequency of data transmission | ||||
| Daily | 13 | 5.881 (3.898–7.864) | 14.635 (p = 0.297) | 1.637 |
| Weekly | 15 | 4.024 (2.641–5.406) | 53.610 (p = 0.007) | 4.505 |
| Bi-weekly | 4 | 3.941 (1.428–6.454) | 0.000 (p = 0.622) | 0.000 |
| Monthly | 6 | 1.803 (-0.234–3.841) | 21.639 (p = 0.271) | 0.552 |
References
- Kishore, S.P.; Heller, D.J.; Vasan, A. Beyond hypertension: Integrated cardiovascular care as a path to comprehensive primary care. B. World Health Organ. 2018, 96, 219–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [PubMed]
- Chow, C.K.; Teo, K.K.; Rangarajan, S.; Islam, S.; Gupta, R.; Avezum, A.; Bahonar, A.; Chifamba, J.; Dagenais, G.; Diaz, R.; et al. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA 2013, 310, 959–968. [Google Scholar] [CrossRef] [Green Version]
- Egan, B.M.; Li, J.; Hutchison, F.N.; Ferdinand, K.C. Hypertension in the United States, 1999 to 2012: Progress toward Healthy People 2020 goals. Circulation 2014, 130, 1692–1699. [Google Scholar] [CrossRef] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2018, 138, e484–e594. [Google Scholar] [PubMed]
- Ward, A.M.; Takahashi, O.; Stevens, R.; Heneghan, C. Home measurement of blood pressure and cardiovascular disease: Systematic review and meta-analysis of prospective studies. J. Hypertens. 2012, 30, 449–456. [Google Scholar] [CrossRef]
- McManus, R.J.; Mant, J.; Bray, E.P.; Holder, R.; Jones, M.I.; Greenfield, S.; Kaambwa, B.; Banting, M.; Bryan, S.; Little, P.; et al. Telemonitoring and self-management in the control of hypertension (TASMINH2): A randomised controlled trial. Lancet 2010, 376, 163–172. [Google Scholar] [CrossRef]
- McManus, R.; Mant, J.; Haque, M.; Bray, E.P.; Bryan, S.; Greenfield, S.; Jones, M.I.; Jowett, S.; Little, P.; Peñaloza, C.; et al. Effect of self-monitoring and medication self-titration on systolic blood pressure in hypertensive patients at high risk of cardiovascular disease: The TASMIN-SR randomized clinical trial. JAMA 2014, 312, 799–808. [Google Scholar] [CrossRef]
- Tucker, K.L.; Sheppard, J.P.; Stevens, R.; Bosworth, H.B.; Bove, A.; Bray, E.P.; Earle, K.; George, J.; Godwin, M.; Green, B.B.; et al. Self-monitoring of blood pressure in hypertension: A systematic review and individual patient data meta-analysis. PLoS Med. 2017, 14, e1002389. [Google Scholar] [CrossRef]
- Kim, Y.N.; Shin, D.G.; Park, S.; Lee, C.H. Randomized clinical trial to assess the effectiveness of remote patient monitoring and physician care in reducing office blood pressure. Hypertens. Res. 2015, 38, 491–497. [Google Scholar] [CrossRef]
- Green, B.B.; Anderson, M.L.; Cook, A.J.; Catz, S.; Fishman, P.A.; McClure, J.B.; Reid, R.J. e-Care for heart wellness: A feasibility trial to decrease blood pressure and cardiovascular risk. Am. J. Prev. Med. 2014, 46, 368–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parati., G.; Ochoa, J.E.; Postel-Vinay, N.; Pellegrini, D.; Torlasco, C.; Omboni, S.; McManus, R. Home Blood Pressure Telemonitoring: Conventional Approach and Perspectives from Mobile Health Technology. In Home Blood Pressure Monitoring; Springer: Cham, Switzerland, 2019; pp. 103–119. [Google Scholar] [CrossRef]
- Omboni, S.; McManus, R.J.; Bosworth, H.B.; Chappell, L.C.; Green, B.B.; Kario, K.; Logan, A.G.; Magid, D.J.; McKinstry, B.; Margolis, K.L.; et al. Evidence and Recommendations on the Use of Telemedicine for the Management of Arterial Hypertension: An International Expert Position Paper. Hypertension 2020, 76, 1368–1383. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Yang, H.; Xia, X.; Lu, X.; Lin, J.; Liu, F.; Gu, D. Interactive Mobile Health Intervention and Blood Pressure Management in Adults. Hypertension 2019, 74, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Duan, Y.; Xie, Z.; Dong, F.; Wu, Z.; Lin, Z.; Sun, N.; Xu, J. Effectiveness of home blood pressure telemonitoring: A systematic review and meta-analysis of randomised controlled studies. J. Hum. Hypertens. 2017, 31, 427–437. [Google Scholar] [CrossRef]
- United Nations Department of Economic and Social Affairs. World Urbanization Prospects: The 2018 Revision; online edition; United Nations Department of Economic and Social Affairs: New York, NY, USA, 2018. [Google Scholar]
- Omboni, S.; Gazzola, T.; Carabelli, G.; Parati, G. Clinical usefulness and cost effectiveness of home blood pressure telemonitoring: Meta-analysis of randomized controlled studies. J. Hypertens. 2013, 31, 455–467, discussion 67–68. [Google Scholar] [CrossRef]
- Choi, W.S.; Park, J.; Choi, J.Y.B.; Yang, J.S. Stakeholders’ resistance to telemedicine with focus on physicians: Utilizing the Delphi technique. J. Telemed. Telecare 2019, 25, 378–385. [Google Scholar] [CrossRef]
- Choi, W.S.; Choi, J.H.; Oh, J.; Shin, I.S.; Yang, J.S. Effects of Remote Monitoring of Blood Pressure in Management of Urban Hypertensive Patients: A Systematic Review and Meta-Analysis. Telemed. J. e-Health 2020, 26, 744–759. [Google Scholar] [CrossRef]
- Jovell, A.J.; Navarro-Rubio, M.D. [Evaluation of scientific evidence]. Med. Clin. 1995, 105, 740–743. [Google Scholar]
- Wosik, J.; Fudim, M.; Cameron, B.; Gellad, Z.F.; Cho, A.; Phinney, D.; Curtis, S.; Roman, M.; Poon, E.G.; Ferranti, J.; et al. Telehealth transformation: COVID-19 and the rise of virtual care. J. Am. Med. Inform. Assoc. 2020, 27, 957–962. [Google Scholar] [CrossRef]
- Cowie, M.R.; Lam, C.S.P. Remote monitoring and digital health tools in CVD management. Nat. Rev. Cardiol. 2021, 18, 457–458. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 502 [updated September 2009]; Wiley: New York, NY, USA, 2009. [Google Scholar]
- Bosworth, H.B.; Olsen, M.K.; McCant, F.; Harrelson, M.; Gentry, P.; Rose, C.; Goldstein, M.K.; Hoffman, B.B.; Powers, B.; Oddone, E.Z. Hypertension Intervention Nurse Telemedicine Study (HINTS): Testing a multifactorial tailored behavioral/educational and a medication management intervention for blood pressure control. J. Am. Heart Assoc. 2007, 153, 918–924. [Google Scholar] [CrossRef]
- Kerry, S.; Markus, H.; Khong, T.; Cloud, G.; Tulloch, J.; Coster, D.; Ibison, J.; Oakeshott, P. Home blood pressure monitoring with nurse-led telephone support among patients with hypertension and a history of stroke: A community-based randomized controlled trial. CMAJ 2012, 185, 23–31. [Google Scholar] [CrossRef] [Green Version]
- Pan, F.; Wu, H.; Liu, C.; Zhang, X.; Peng, W.; Wei, X.; Gao, W. Effects of home telemonitoring on the control of high blood pressure: A randomised control trial in the Fangzhuang Community Health Center, Beijing. Aust. J. Prim. Health 2018, 24, 398–403. [Google Scholar] [CrossRef]
- Zha, P.; Qureshi, R.; Porter, S.; Chao, Y.Y.; Pacquiao, D.; Chase, S.; O’Brien-Richardson, P. Utilizing a Mobile Health Intervention to Manage Hypertension in an Underserved Community. West. J. Nurs. Res. 2020, 42, 201–209. [Google Scholar] [CrossRef]
- Artinian, N.T.; Flack, J.M.; Nordstrom, C.K.; Hockman, E.M.; Washington, O.G.; Jen, K.L.; Fathy, M. Effects of nurse-managed telemonitoring on blood pressure at 12-month follow-up among urban African Americans. Nurs. Res. 2007, 56, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Cicolini, G.; Simonetti, V.; Comparcini, D.; Celiberti, I.; Di Nicola, M.; Capasso, L.M.; Flacco, M.E.; Bucci, M.; Mezzetti, A.; Manzoli, L. Efficacy of a nurse-led email reminder program for cardiovascular prevention risk reduction in hypertensive patients: A randomized controlled trial. Int. J. Nurs. Stud. 2014, 51, 833–843. [Google Scholar] [CrossRef] [PubMed]
- Hebert, P.; Sisk, J.; Tuzzio, L.; Casabianca, J.; Pogue, V.; Wang, J.; Chen, Y.; Cowles, C.; McLaughlin, M.A. Nurse-led disease management for hypertension control in a diverse urban community: A randomized trial. J. Gen. Intern. Med. 2012, 27, 630–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.B.; Han, H.R.; Huh, B.; Nguyen, T.; Lee, H.; Kim, M.T. The effect of a community-based self-help multimodal behavioral intervention in Korean American seniors with high blood pressure. Am. J. Hypertens. 2014, 27, 1199–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magda, M.M.; Riad, N.A.; Badawy, A.E.; EI Gafar, S.E.A.; El-Hammed, B.M.A.; Eltomy, E.M. Tele-nursing versus Routine Outpatient Teaching for Improving Arterial Blood Pressure and Body Mass Index for Hypertensive Patients. Am. J. Nurs. Res. 2020, 8, 18–26. [Google Scholar]
- Pour, E.R.; Aliyari, S.; Farsi, Z.; Ghelich, Y. Comparing the effects of interactive and noninteractive education using short message service on treatment adherence and blood pressure among patients with hypertension. Nurs. Midwifery Stud. 2020, 9, 68–76. [Google Scholar]
- Rubinstein, A.; Miranda, J.J.; Beratarrechea, A.; Diez-Canseco, F.; Kanter, R.; Gutierrez, L.; Bernabé-Ortiz, A.; Irazola, V.; Fernandez, A.; Letona, P.; et al. Effectiveness of an mHealth intervention to improve the cardiometabolic profile of people with prehypertension in low-resource urban settings in Latin America: A randomised controlled trial. Lancet Diabetes Endocrinol. 2016, 2016 4, 52–63. [Google Scholar] [CrossRef]
- The Cochrane Collaboration. Review Manager (RevMan)[Computer Program], Version 5.4 for Windows; The Cochrane Collaboration: Oxford, UK, 2020.
- Egger, M.; Davey-Smith, G.; Altman, D. (Eds.) Systematic Reviews in Healthcare: Meta-Analysis in Context; John Wiley & Sons: New York, NY, USA, 2008. [Google Scholar]
- Takeshima, N.; Sozu, T.; Tajika, A.; Ogawa, Y.; Hayasaka, Y.; Furukawa, T.A. Which is more generalizable, powerful and interpretable in meta-analyses, mean difference or standardized mean difference? BMC Med. Res. Methodol. 2014, 14, 30. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Hill, M.; Bone, L.; Hilton, S.; Roary, M.; Kelen, G.; Levine, D. A clinical trial to improve high blood pressure care in young urban black men: Recruitment, follow-up, and outcomes. Am. J. Hypertens. 1999, 12, 548–554. [Google Scholar] [CrossRef] [Green Version]
- Friedman, R.H.; Kazis, L.E.; Jette, A.; Smith, M.B.; Stollerman, J.; Torgerson, J.; Carey, K. A telecommunications system for monitoring and counseling patients with hypertension: Impact on medication adherence and blood pressure control. Am. J. Hypertens. 1996, 9, 285–292. [Google Scholar] [CrossRef] [Green Version]
- McMahon, G.; Gomes, H.; Hickson, H.S.; Hu, T.; Levine, B.; Conlin, P. Web-based care management in patients with poorly controlled diabetes. Diabetes Care 2005, 28, 1624–1629. [Google Scholar] [CrossRef] [Green Version]
- Shea, S.; Weinstock, R.; Starren, J.; Teresi, J.; Palmas, W.; Field, L.; Morin, P.; Goland, R.; Izquierdo, R.E.; Wolff, L.T.; et al. A randomized trial comparing telemedicine case management with usual care in older, ethnically diverse, medically underserved patients with diabetes mellitus. J. Am. Med. Inform. Assoc. 2006, 13, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Carrasco, M.P.; Salvador, C.H.; Sagredo, P.G.; Marquez-Montes, J.; de Mingo, M.A.G.; Fragua, J.A.; Rodríguez, M.C.; García-Olmos, L.M.; García-López, F.; Muñoz Carrero, A.; et al. Impact of patient-general practitioner short-messages-based interaction on the control of hypertension in a follow-up service for low-to-medium risk hypertensive patients: A randomized controlled trial. IEEE Trans. Inf. Technol. Biomed. 2008, 12, 780–791. [Google Scholar] [CrossRef]
- Green, B.B.; Cook, A.J.; Ralston, J.D.; Fishman, P.A.; Catz, S.L.; Carlson, J. Effectiveness of home blood pressure monitoring, Web communication, and pharmacist care on hypertension control: A randomized controlled trial. JAMA 2008, 299, 2857–2867. [Google Scholar] [CrossRef] [Green Version]
- Madsen, L.B.; Kirkegaard, P.; Pedersen, E.B. Blood pressure control during telemonitoring of home blood pressure. A randomized controlled trial during 6 months. Blood Press. 2008, 17, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Parati, G.; Omboni, S.; Albini, F.; Piantoni, L.; Giuliano, A.; Revera, M.; Illyes, M.; Mancia, G.; Tele, B.S.G. Home blood pressure telemonitoring improves hypertension control in general practice. The TeleBPCare study. J. Hypertens. 2009, 27, 198–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, M.; Kim, H.; Kim, K. Cellular phone and Internet-based individual intervention on blood pressure and obesity in obese patients with hypertension. Int. J. Med. Inform. 2009, 78, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Varis, J.; Kantola, I. The choice of home blood pressure result reporting method is essential: Results mailed to physicians did not improve hypertension control compared with ordinary office-based blood pressure treatment. Blood Press. 2010, 19, 319–324. [Google Scholar] [CrossRef]
- Hoffmann-Petersen, N.; Lauritzen, T.; Bech, J.N.; Pedersen, E.B. Short-term telemedical home blood pressure monitoring does not improve blood pressure in uncomplicated hypertensive patients. J. Hum. Hypertens. 2017, 31, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Ionov, M.V.; Zhukova, O.V.; Yudina, Y.S.; Avdonina, N.G.; Emelyanov, I.V.; Kurapeev, D.I.; Zvartau, N.E.; Konradi, A.O. Value-based approach to blood pressure telemonitoring and remote counseling in hypertensive patients. Blood Press. 2020, 30, 1–11. [Google Scholar] [CrossRef]
- Logan, A.G.; Irvine, M.J.; McIsaac, W.J.; Tisler, A.; Rossos, P.G.; Easty, A.; Feig, D.S.; Cafazzo, J.A. Effect of Home Blood Pressure Telemonitoring With Self-Care Support on Uncontrolled Systolic Hypertension in Diabetics. Hypertension 2012, 60, 51–57. [Google Scholar] [CrossRef] [Green Version]
- Neumann, C.L.; Menne, J.; Rieken, E.M.; Fischer, N.; Weber, M.H.; Haller, H.; Schulz, E.G. Blood pressure telemonitoring is useful to achieve blood pressure control in inadequately treated patients with arterial hypertension. J. Hum. Hypertens. 2011, 25, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Wakefield, B.J.; Holman, J.E.; Ray, A.; Scherubel, M.; Adams, M.R.; Hillis, S.L.; Rosenthal, G.E. Effectiveness of home telehealth in comorbid diabetes and hypertension: A randomized, controlled trial. Telemed. J. e-Health 2011, 17, 254–261. [Google Scholar] [CrossRef]
- Bosworth, H.B.; Powersm, B.J.; Olsen, M.K.; McCant, F.; Grubber, J.; Smith, V.; Gentry, P.W.; Rose, C.; Van Houtven, C.; Wang, V.; et al. Home blood pressure management and improved blood pressure control: Results from a randomized controlled trial. Arch. Intern. Med. 2011, 171, 1173–1180. [Google Scholar] [CrossRef] [Green Version]
- Migneault, J.; Dedier, J.; Wright, J.; Heeren, T.; Campbell, M.; Morisky, D.; Rudd, P.; Friedman, R.H. A culturally adapted telecommunication system to improve physical activity, diet quality, and medication adherence among hypertensive African-Americans: A randomized controlled trial. Ann. Behav. Med. 2012, 43, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Kim, H. Evaluation of mobile phone and Internet intervention on waist circumference and blood pressure in post-menopausal women with abdominal obesity. Int. J. Med. Eng. Inform. 2012, 81, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Bove, A.; Homko, C.; Santamore, W.; Kashem, M.; Kerper, M.; Elliott, D. Managing hypertension in urban underserved subjects using telemedicine--a clinical trial. Am. Heart J. 2013, 165, 615–621. [Google Scholar] [CrossRef]
- Wakefield, B.J.; Koopman, R.J.; Keplinger, L.E.; Bomar, M.; Bernt, B.; Johanning, J.L.; Kruse, R.L.; Davis, J.W.; Wakefield, D.S.; Mehr, D.R. Effect of home telemonitoring on glycemic and blood pressure control in primary care clinic patients with diabetes. Telemed. J. e-Health 2014, 20, 199–205. [Google Scholar] [CrossRef]
- Yi, S.; Tabaei, B.; Angell, S.; Rapin, A.; Buck, M.; Pagano, W.; Maselli, F.J.; Simmons, A. Self-blood pressure monitoring in an urban, ethnically diverse population: A randomized clinical trial utilizing the electronic health record. Circ. Cardiovasc. Qual. Outcomes 2015, 8, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A.C. Chapter 8: Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J., Thomas, J., Eds.; Cochrane: London, UK, 2021; Available online: wwwtrainingcochraneorg/handbook (accessed on 5 August 2021).
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56(2), 455–463. [Google Scholar] [CrossRef]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- OECD Indicators. Health at a Glance 2019: OECD Indicators; OECD Publishing: Paris, French, 2019. [Google Scholar]
- Hwang, J.Y.; Kim, K.Y.; Lee, K.H. Factors that influence the acceptance of telemetry by emergency medical technicians in ambulances: An application of the extended technology acceptance model. Telemed. J. e-Health 2014, 20, 1127–1134. [Google Scholar] [CrossRef] [Green Version]
- National Center for Health Statistics (US). Health, United States, 2013: With Special Feature on Prescription Drugs. National Center for Health Statistics (US): Hyattsville, MD, USA, 2014. [Google Scholar]
- Neal, B.; MacMahon, S.; Chapman, N. Effects of ACE inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: Results of prospectively designed overviews of randomised trials. Blood Pressure Lowering Treatment Trialists’ Collaboration. Lancet 2000, 356, 1955–1964. [Google Scholar] [PubMed]
- Cook, N.R.; Cohen, J.; Hebert, P.R.; Taylor, J.O. Hennekens, C.H. Implications of small reductions in diastolic blood pressure for primary prevention. Arch Intern. Med. 1995, 155, 701–709. [Google Scholar] [CrossRef]
- Law, M.R.; Morris, J.K.; Wald, N.J. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: Meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ 2009, 338, b1665. [Google Scholar] [CrossRef] [Green Version]
- Hammersley, V.; Parker, R.; Paterson, M.; Hanley, J.; Pinnock, H.; Padfield, P.; Stoddart, A.; Park, H.G.; Sheikh, A.; McKinstry, B. Telemonitoring at scale for hypertension in primary care: An implementation study. PLoS Med. 2020, 17, e1003124. [Google Scholar] [CrossRef]
- Omboni, S. Telemedicine During the COVID-19 in Italy: A Missed Opportunity? Telemed. J. e-Health 2020, 26, 973–975. [Google Scholar] [CrossRef] [Green Version]
- Margolis, K.L.; Asche, S.E.; Dehmer, S.P.; Bergdall, A.R.; Green., B.B.; Sperl-Hillen, J.M.; Nyboer, R.A.; Pawloski, P.A.; Maciosek, M.V.; Trower, N.K.; et al. Long-term Outcomes of the Effects of Home Blood Pressure Telemonitoring and Pharmacist Management on Blood Pressure Among Adults With Uncontrolled Hypertension: Follow-up of a Cluster Randomized Clinical Trial. JAMA Netw. Open 2018, 1, e181617. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 Practice Guidelines for the management of arterial hypertension of the European Society of Hypertension and the European Society of Cardiology: ESH/ESC Task Force for the Management of Arterial Hypertension. J. Hypertens. 2018, 36, 2284–2309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hjelm, N.M. Benefits and drawbacks of telemedicine. J. Telemed. Telecare 2005, 11, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Filchev, R.; Pavlova, D.; Dimova, R.; Dovramadjiev, T. Healthcare System Sustainability by Application of Advanced Technologies in Telemedicine and eHealth. In International Conference on Human Interaction and Emerging Technologies; Springer: Cham, Switzerland, 2021; pp. 1011–1017. [Google Scholar]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]







| Study | Included Participants | Participants Number | Participants’ Age Interval (Years) | Duration (Months) | City Name (Country) | Population of City | Setting | Description of Intervention | Intervention Frequency | Outcomes | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| UC | RBPM | Age Interval | UC | RBPM | |||||||||
| Bosworth (2007) [25] | Treated hypertensive patients | 150 | 150 | Child, Adult, Older Adult | Not reported | Not reported | 18 | Durham (USA) | 232,299 in 2005 | Durham VA general internal medicine clinics (Not underserved) | Nurse-administered tailored behavioral intervention with telemedicine device connected to telephone | Once a day | 1. Primary: BP control. 2. Secondary: knowledge and perceived risks related with hypertension |
| Bosworth (2007) [25] | Treated hypertensive patients | 150 | 150 | Child, Adult, Older Adult | Not reported | Not reported | 18 | Durham (USA) | 232,299 in 2005 | Durham VA general internal medicine clinics (Not underserved) | Nurse-administered medication management | Once a day | 1. Primary: BP control 2. Secondary: knowledge and perceived risks related with hypertension |
| Bosworth (2007) [25] | Treated hypertensive patients | 150 | 150 | Child, Adult, Older Adult | Not reported | Not reported | 18 | Durham (USA) | 232,299 in 2005 | Durham VA general internal medicine clinics (Not underserved) | Nurse-administered tailored behavioral intervention and medication management | Once a day | 1. Primary: BP control 2. Secondary: knowledge and perceived risks related with hypertension |
| Kerry (2013) [26] | Hypertensive patients with history of stroke or transient ischemic attack | 169 | 168 | 16 or older (Child, Adult, Older Adult) Average: 71.9 | 72.6 ± 11.4 | 71.1 ± 12.6 | 6 | London (UK) | 6,984,772 in 2007 | Community healthcare center (Not underserved) | Home BP monitoring with nurse-led support through telephone | Twice a week | Reduction of SBP |
| Kerry (2013) [26] | Hypertensive patients with history of stroke or transient ischemic attack | 169 | 168 | 16 or older (Child, Adult, Older Adult) Average: 71.9 | 72.6 ± 11.4 | 71.1 ± 12.6 | 12 | London (UK) | 6,984,772 in 2007 | Community healthcare center (Not underserved) | Home BP monitoring with nurse-led support through telephone | Twice a week | Reduction of SBP |
| Pan (2018) [27] | Patients diagnosed hypertension | 55 | 52 | Between 35 and 75. Average: 57.2 | 56.55 ± 9.80 | 57.8 ± 10.87 | 3 | Beijing (China) | 11,895,973 in 2016 | Fangzhuang Community Health Center (Not underserved) | Mobile phone-linked computer system | Once a day | BP control |
| Pan (2018) [27] | Patients diagnosed hypertension | 55 | 52 | Between 35 and 75. Average: 57.2 | 56.55 ± 9.80 | 57.8 ± 10.87 | 6 | Beijing (China) | 11,895,973 in 2016 | Fangzhuang Community Health Center (Not underserved) | Mobile phone-linked computer system | Once a day | BP control |
| Zha (2020) [28] | Uncontrolled hypertensive patients | 13 | 12 | Between 18 and 64. Average: 52.3 | 55.5 ± 5.2 | 48.9 ± 8.0 | 3 | Newark (USA) | 278,366 in 2016 | Jordan and Harris Community Health Center (Local community health center) (Underserved) | Smartphone-linked system by nurse | Visit office once a week. Instant feedback after all measurements. | BP control (Changes in SBP and DBP), perceived self-efficacy, HRQOL |
| Zha (2020) [28] | Uncontrolled hypertensive patients | 13 | 12 | Between 18 and 64. Average: 52.3 | 55.5 ± 5.2 | 48.9 ± 8.0 | 6 | Newark (USA) | 278,366 in 2016 | Jordan and Harris Community Health Center (Local community health center) (Underserved) | Smartphone-linked system by nurse | Visit office once a week. Instant feedback after all measurements. | BP control (Changes in SBP and DBP), perceived self-efficacy, HRQOL |
| Artinian (2007) [29] | African American hypertensive patients | 157 | 164 | 18 or more | 60.2 ± 12.3 | 59.1 ± 13.0 | 3 | Detroit (USA) | 594,562 in 2002 | Family community center (Underserved) | Telephonic transmission with BP monitoring device linked to telephone | Once a week | Office BP changes (SBP, DBP) |
| Artinian (2007) [29] | African American hypertensive patients | 163 | 168 | 18 or more | 60.2 ± 12.3 | 59.1 ± 13.0 | 6 | Detroit (USA) | 594,562 in 2002 | Family community center (Undeserved) | Telephonic transmission with BP monitoring device linked to telephone | Once a month | Office BP changes (SBP, DBP) |
| Artinian (2007) [29] | African American hypertensive patients | 169 | 167 | 18 or more | 60.2 ± 12.3 | 59.1 ± 13.0 | 12 | Detroit (USA) | 594,562 in 2002 | Family community center (Undeserved) | Telephonic transmission with BP monitoring device linked to telephone | Once a month | Office BP changes (SBP, DBP) |
| Cicolini (2013) [30] | Treated or untreated hypertensive patients | 98 | 100 | Between 18 and 80. (Adult, Older Adult) Average: 59.1 | 58.3 ± 13.9 | 59.8 ± 15.0 | 3 | Chieti (Italy) | 43,824 in 2011 | Italian Hypertension Primary Care Center (Not underserved) | Nurse-led reminder through e-mail | Once a week | 1. BP changes 2. BMI, alcohol consumption, cigarette smoking, adherence to therapy |
| Cicolini (2013) [30] | Treated or untreated hypertensive patients | 98 | 100 | Between 18 and 80. (Adult, Older Adult) Average: 59.1 | 58.3 ± 13.9 | 59.8 ± 15.0 | 6 | Chieti (Italy) | 43,824 in 2011 | Italian Hypertension Primary Care Center (Not underserved) | Nurse-led reminder through e-mail | Once a week | 1. BP changes 2. BMI, alcohol consumption, cigarette smoking, adherence to therapy |
| Hebert (2012) [31] | Uncontrolled hypertensive patients | 83 | 85 | 18 or more. Average: 60.8 | (61.3 ± 11.7) | 61.3 ± 11.7 | 9 | New York (USA) | 8,174,959 in 2010 | One academic medical center, two medium-sized hospitals, one community hospital (Underserved) | Telephone | Once a week (Meetings: once in two weeks) | Blood pressure reduction |
| Hebert (2012) [31] | Uncontrolled hypertensive patients | 78 | 79 | 18 or more. Average: 60.8 Average: 60.8 | (61.3 ± 11.7) | 61.3 ± 11.7 | 18 | New York (USA) | 7,721,457 in 2010 | One academic medical center, two medium-sized hospitals, one community hospital (Underserved) | Telephone | Once a week (Meetings: once in two weeks) | Blood pressure reduction |
| Kim (2014) [32] | Uncontrolled Korean–American hypertensive seniors | 192 | 191 | 60 or older adult. Average: 70.9 | 71.2 ± 5.6 | 70.6 ± 5.0 | 6 | Ellicott City (USA) | 60,489 in 2007 | Korean Resource Center (Hospital) (Not Undeserved) | Telephone-monitoring system and telephone counseling | At least once a week (Measurement: at least twice a day, Monthly telephone counseling) | Changes in SBP and DBP |
| Kim (2014) [32] | Uncontrolled Korean–American hypertensive seniors | 185 | 187 | 60 or older adult. Average: 70.9 | 71.2 ± 5.6 | 70.6 ± 5.0 | 12 | Ellicott City (USA) | 60,489 in 2007 | Korean Resource Center (Hospital) (Not Undeserved) | Telephone-monitoring system and telephone counseling | At least once a week (Measurement: at least twice a day, Monthly telephone counseling, | Changes in SBP and DBP |
| Kim (2014) [32] | Uncontrolled Korean–American hypertensive seniors | 185 | 184 | 60 or older adult. Average: 70.9 | 71.2 ± 5.6 | 70.6 ± 5.0 | 18 | Ellicott City (USA) | 60,489 in 2007 | Korean Resource Center (Hospital) (Not Undeserved) | Telephone-monitoring system and telephone counseling | At least once a week (Measurement: at least twice a day, Monthly telephone counseling, | Changes in SBP and DBP |
| Mohsen (2020) [33] | Treated hypertensive patients with antihypertensive medication | 50 | 50 | Between 35 and 65. Average: 56.41 | 55.01 ± 7.50 | 57.81 ± 9.52 | 3 | Shibin El Kom (Egypt) | 190.064 in 2019 | Medical outpatient clinic of Menoufia University Hospital (Not Undeserved) | Tele-nursing intervention with telephone support | Twice a week (Measurement: every day) | 1. Reduction of SBP and DBP 2. BMI difference |
| Mohsen (2020) [33] | Treated hypertensive patients with medication | 50 | 50 | Between 35 and 65. Average: 56.41 | 55.01 ± 7.50 | 57.81 ± 9.52 | 6 | Shibin El Kom (Egypt) | 190.064 in 2019 | Medical outpatient clinic of Menoufia University Hospital (Not Undeserved) | Tele-nursing intervention with telephone support | Twice a week. (Measurement: every day) | 1. Reduction of SBP and DBP 2. BMI difference |
| Pour (2020) [34] | Treated hypertensive patients with medication | 21 | 21 | Between 35 and 64. Average: 55.7 | 56.71 ± 5.73 | 54.71 ± 6.11 | 3 | Tehran (Iran) | 7,250,693 in 2019 | Military hospital (Not underserved) | Interactive SMS | Once a week | BP control (Changes in SBP and DBP), |
| Pour (2020) [34] | Treated hypertensive patients with medication | 21 | 21 | Between 35 and 64. Average: 55.7 | 56.71 ± 5.73 | 54.71 ± 6.11 | 4 | Tehran (Iran) | 7,250,693 in 2019 | Military hospital (Not underserved) | Interactive SMS | Once a week | BP control (Changes in SBP and DBP), |
| Pour (2020) [34] | Treated hypertensive patients with medication | 21 | 21 | Between 35 and 64. Average: 55.7 | 56.71 ± 5.73 | 54.71 ± 6.11 | 3 | Tehran (Iran) | 7,250,693 in 2019 | Military hospital (Not underserved) | Non-Interactive SMS | Once a week | BP control (Changes in SBP and DBP), |
| Pour (2020) [34] | Treated hypertensive patients with medication | 21 | 21 | Between 35 and 64. Average: 55.7 | 56.71 ± 5.73 | 54.71 ± 6.11 | 4 | Tehran (Iran) | 7,250,693 in 2019 | Military hospital (Not underserved) | Non-Interactive SMS | Once a week | BP control (Changes in SBP and DBP), |
| Rubinstein (2016) [35] | Untreated prehypertensive patients | 276 | 270 | Between 30 and 60. Average: 43.4 | 43.2 ± 8.4 | 43.6 ± 8.4 | 6 | Buenos Aires (Argentina) and Guatemala City (Guatemala) and Lima (Peru) | 12,271,254 (Buenos Aires) and 880,893 (Guatemala City) and 7,136,586 (Lima) in 2012 | Institute for Clinical Effectiveness and Health Policy (Buenos Aires, Argentina), Institute of Nutrition of Central America and Panama (Guatemala City, Guatemala), Universidad Peruana Cayetano Heredia (Lima, Peru) (Underserved) | Mobile phone transmission | Once a month | Mean changes in SBP and DBP |
| Rubinstein (2016) [35] | Untreated prehypertensive patients | 287 | 266 | Between 30 and 60. Average: 43.4 | 43.2 ± 8.4 | 43.6 ± 8.4 | 12 | Buenos Aires (Argentina) and Guatemala City (Guatemala) and Lima (Peru) | 12,271,254 (Buenos Aires) and 880,893 (Guatemala city) and 7,136,586 (Lima) in 2012 | Institute for Clinical Effectiveness and Health Policy (Buenos Aires, Argentina), Insitute of Nutrition of Central America and Panama (Guatemala City, Guatemala), Universidad Peruana Cayetano Heredia (Lima, Peru) (Underserved) | Mobile phone transmission | Once a month | Mean changes in SBP and DBP |
| Hill (1999) [41] | Black or African American hypertensive young male residents within hospital catchment area | 77 | 78 | Between 22 and 49 Average: 39.0 | 12 | Baltimore (USA) | 503,998 in 1995 | Johns Hopkins Hospital Outpatient General Clinical Research Center (Underserved) | Telephone | Once a month | Office BP changes | ||
| Friedman (1996) [42] | Treated hypertensive patients | 134 | 133 | Over 60 Average: 76.5 | 77 | 76 | 6 | Boston (USA) | 534,743 in 1994 | Senior centers in 29 different communities(Not underserved) | Telephone-linked computer system | Once a week | Office BP changes |
| McMahon (2005) [43] | Poorly controlled diabetics and hypertensive patients | 35 | 37 | Older than 18. Average: 63.5 | 63 ± 7 | 64 ± 7 | 12 | Boston (USA) | 580,352 in 2001 | Hospital (Not underserved) | Web-base | At least three times a week | Changes in A1c, BP, lipid profiles |
| Shea (2006) [44] | Diabetic hypertensive patients | 347 | 333 | 55 or older (Adult, Older Adult) Average: 70.8 ± 6.7 | 70.9 ± 6.8 | 70.8 ± 6.5 | 12 | Syracuse (USA) | 129,966 in 2005 | SUNY Upstate Medical University hospital, (Underserved) | Telephone-linked web system | Regularly | Changes in hemoglobin A1c, BP, cholesterol level |
| Carrasco (2008) [45] | Treated or untreated hypertensive patients | 142 | 131 | Average age: 62.5 | 62.8 ± 12.5 | 62.1 ± 11.9 | 3 | Madrid (Spain) | 3,116,909 in 2006 | 21 regional public health centers (the corporative network of the “Servicio Madrileno de Salud”) (Not underserved) | Mobile phone transmission | During the six-month follow-up, four times a week (Monday and Thursday, morning and night) | 1. BP control 2. the impact on patient QoL and anxiety, and economic aspects concerning the viability of the telemedicine system |
| Green (2008) [46] | Treated hypertensive patients | 247 | 246 | Between 25 and 75. (Adult, Older Adult) Average: 59.1 | 58.6 ± 8.5 | 59.5 ± 8.3 | 12 | Seattle, USA | 622,927 in 2006 | 10 medical centers within Group Health Research Institute (Not underserved) | Home BP monitors, instruction on their use, and proficiency training on web-based communication | Report once every two weeks (measurement at least twice a week) | Office SBP and DBP changes and control of BP |
| Madsen (2008) [47] | Treated or untreated hypertensive patients | 123 | 113 | Between 20 and 80. Average Age: 55.9 | 56.7 ± 11.6 | 55.0 ± 11.7 | 6 | Holstebro (Denmark) | 29,888 in 2004 | Holstebro Hospital (Not underserved) | PDA-embedded mobile-web phone (mobile) | Three times a week during the first 3 months and once a week during the last 3 months | Difference in systolic daytime ABPM change |
| Parati (2009) [48] | Uncontrolled hypertensive patients | 111 | 187 | Between 17 and 75. Average age: 57.5 | 58.1 ± 10.8 | 57.2 ± 10.7 | 6 | Milan (Italy) | 1,198,182 in 2006 | Primary care units in Milan (Not underserved) | Telephone-linked computer system | Regularly | Percentage of patients who reached normalization of BP |
| Park (2009) [49] | Obese hypertensive patients | 21 | 28 | Average age: 53.8 | 54.6 ± 11.0 | 53.2 ± 6.9 | 2 | Seoul (S. Korea) | 9,828,102 in 2007 | University-affiliated tertiary care hospital (Not underserved) | Telephone and internet transmission | Once a week | Change in blood pressure, body weight, waist circumference, and serum lipid profile |
| Varis (2010) [50] | Untreated hypertensive patients | 68 | 89 | Between 40 and 80 | Not reported | Not reported | 13 | Helsinki and Tampere and Turku (Finland) | 536,160 and 194,594 and 168,920 In 2007 | Not underserved | Letter to physician | Every five weeks (measurement every day) | Changes in BP and target BP |
| Hoffmann-Petersen (2017) [51] | Treated uncomplicated hypertensive patients | 181 | 175 | Between 55 and 64 Average: 60.4 | 60.4 ± 2.9 | 60.5 ± 2.6 | 3 | Holstebro (Denmark) | 30,885 in 2011 | Holstebro Regional Hospital (Not underserved) | Telephone and e-mail communication (Telephone-linked computer system) | Once every two weeks | Daytime ABPM reduction and percentage of target BP |
| Ionov (2020) [52] | Uncontrolled hypertension patients | 80 | 160 | Between 18 and 78 | 49 (20 to 77) | 47 (18 to 78) | 3 | Saint-Petersburg, (Russia) | 5,076,520 in 2019 | Federal Medical Research Center Hospital (Not underserved) | Mobile phone communication | Once a week (Measurement: twice a day) | Change of SBP and rate of BP control. |
| Logan (2012) [53] | Uncontrolled hypertensive and diabetic patients | 51 | 54 | 30 or more Average: 62.9 | 62.7 ± 7.8 | 63.1 ± 9.0 | 12 | Toronto (Canada) | 2,423,221 in 2011 | Mount Sinai Hospital (Not underserved) | Bluetooth-enabled BP device paired with smartphone (mobile-web) | Twice a day | Changes in ambulatory BP |
| Neumann (2011) [54] | Inadequately treated hypertensive patients | 29 | 28 | Between 18 and 80. Average age: 55.5 | 56.2 ± 17.4 | 54.7 ± 17.9 | 3 | Göttingen (Germany) | 119,161 in 2009 | Not underserved | Mobile phone-linked computer system | Once a Day | BP Control |
| Wakefield (2011) [55] | Type 2 diabetics and hypertensive patients | 97 | 83 | Between 40 and 89. Average: 48.1 | 67.9 ± 9.9 | 68.4 ± 9.5 | 6 | Iowa City (USA) | 67,548 in 2006 | Iowa City VA Health Care System (Not underserved) | Telephonic transmission | Every day | Changes in hemoglobin A1c and SBP |
| Bosworth (2011) [56] | Treated hypertensive patients | 137 | 127 | Child, Adult, Older Adult Average Age: 63.5 | 64 ± 10 | 63 ± 11 | 12 | Durham (USA) | 234,477 in 2006 | Durham VA Medical Center (Not underserved) | Telephonic transmission | Once a day | 1. BP control 2. SBP and DBP change |
| Migneault (2012) [57] | African American hypertensive patients | 140 | 125 | 35 or more. Average age: 56.5 | 56.8 ± 11.4 | 56.3 ± 10.6 | 8 | Boston (USA) | 590,971, in 2003 | Boston Medical Center primary care practices of a large, safety-net hospital and four affiliated community health centers. (Underserved) | Automated, computer-based, interactive telephone counseling system | Once a week | Change in diet quality, leisure time physical activity of moderate-or-greater intensity, and adherence to the antihypertensive medication regimen and change in BP. |
| Park (2012) [58] | Post-menopausal obese hypertensive patients | 33 | 34 | Average age: 56.7 | 57.6 ± 5.5 | 55.8 ± 5.7 | 3 | Seoul (S. Korea) | 9,828,102 in 2007 | University medical center (Not underserved) | Reporting on website. Mobile and internet transmission | Once a week. | Change in waist circumference, body weight, and blood pressure, fasting plasma glucose, and serum lipid levels |
| Bove (2013) [59] | Systolic hypertensive patients | 107 | 99 | Between 18 and 85 (Adult, Older Adult) Average: 59.6 | 58.2 ± 13.5 | 61.0 ± 13.6 | 6 | Philadelphia/Wilmington, USA | 1,480,457/109,499 in 2010 | University hospital (Underserved) | Telephone and internet-based System | Once a day | BP control at 6 months |
| Wakefield (2014) [60] | Type 2 diabetics and uncontrolled hypertensive patients | 43 | 40 | 18 or more. Average: 60.0 | 62.5 ± 10.9 | 57.7 ± 10.8 | 3 | Columbia (USA) | 112,498 in 2010 | University hospital (Not underserved) | Web System through mobile phone or personal computer | Twice a week (Measurement: every day) | Changes in hemoglobin A1c and SBP |
| Yi (2015) [61] | Uncontrolled hypertensive patients | 332 | 329 | 18 or more. Average: 61.3 | 61.3 ± 12.2 | 61.3 ± 11.9 | 9 | Bronx and Brooklyn and New York (USA) | 1,308,242 and 2,172,989 and 7,721,458 in 2010 | Riverdale Family Practice (Bronx), Lutheran Family Health Centers (Brooklyn), New York City Department of Health and Mental Hygiene (New York City), Heritage Health Care (New York City) (Underserved) | Telephone-linked computer system | Once a month (Measurement: every day) | Change in SBP and DBP and achievement of BP control |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.-H.; Shin, J.-H.; Park, J.; Choi, W.-S. An Updated Meta-Analysis of Remote Blood Pressure Monitoring in Urban-Dwelling Patients with Hypertension. Int. J. Environ. Res. Public Health 2021, 18, 10583. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010583
Park S-H, Shin J-H, Park J, Choi W-S. An Updated Meta-Analysis of Remote Blood Pressure Monitoring in Urban-Dwelling Patients with Hypertension. International Journal of Environmental Research and Public Health. 2021; 18(20):10583. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010583
Chicago/Turabian StylePark, Sang-Hyun, Jong-Ho Shin, Joowoong Park, and Woo-Seok Choi. 2021. "An Updated Meta-Analysis of Remote Blood Pressure Monitoring in Urban-Dwelling Patients with Hypertension" International Journal of Environmental Research and Public Health 18, no. 20: 10583. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010583