
Measuring Risk Perception in Pregnant Women in Heavily Polluted Areas: A New Methodological Approach from the NEHO Birth Cohort

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Risk Perception Questionnaire
2.2. Risk Perception Indices
- the hazard perception index (HPI);
- the exposure hazard perception index (EHPI);
- the health risk perception index (HRPI);
- the risk perception index (RPI).
2.3. Exploratory Factorial Analysis Indices
2.4. Latent Class Analysis
3. Results
3.1. Socio-Demographic Information
3.2. Risk Perception Indices
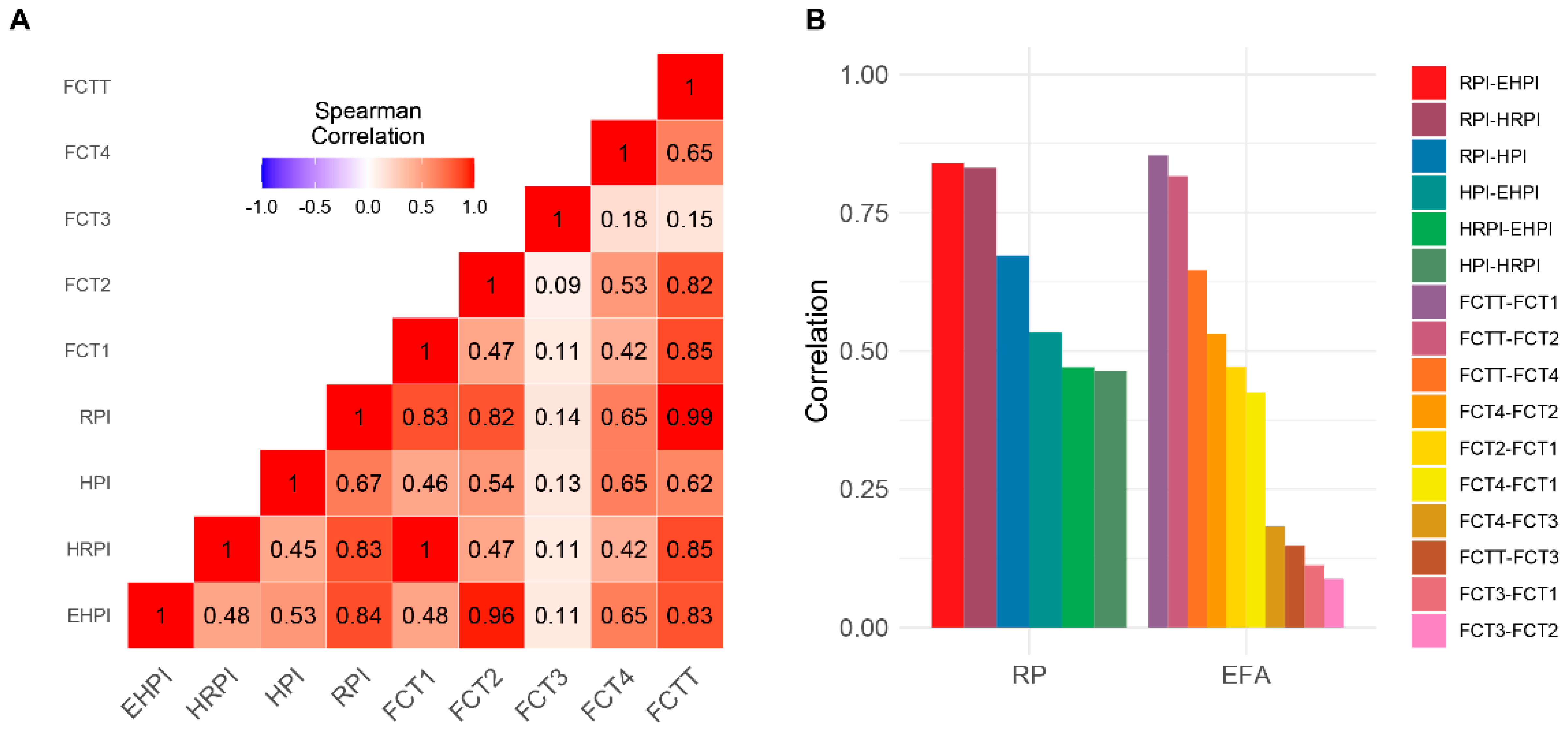
3.3. Exploratory Factorial Analysis Indices
- Factor 1 (FCT1) corresponds, in terms of building items, to the HRPI index, evaluating the health aspects of the perceived risk.
- Factor 2 (FCT2) includes the items measuring the degree of risk perception in relation to water, air, and food pollution, and thus is equivalent to EHPI.
- Factor 3 (FCT3) includes only one item that is a measure of road traffic level perception.
- Factor 4 (FCT4) is composed of items evaluating the perception of noise and olfactory pollution (see Table S1 in the Supplementary Material).
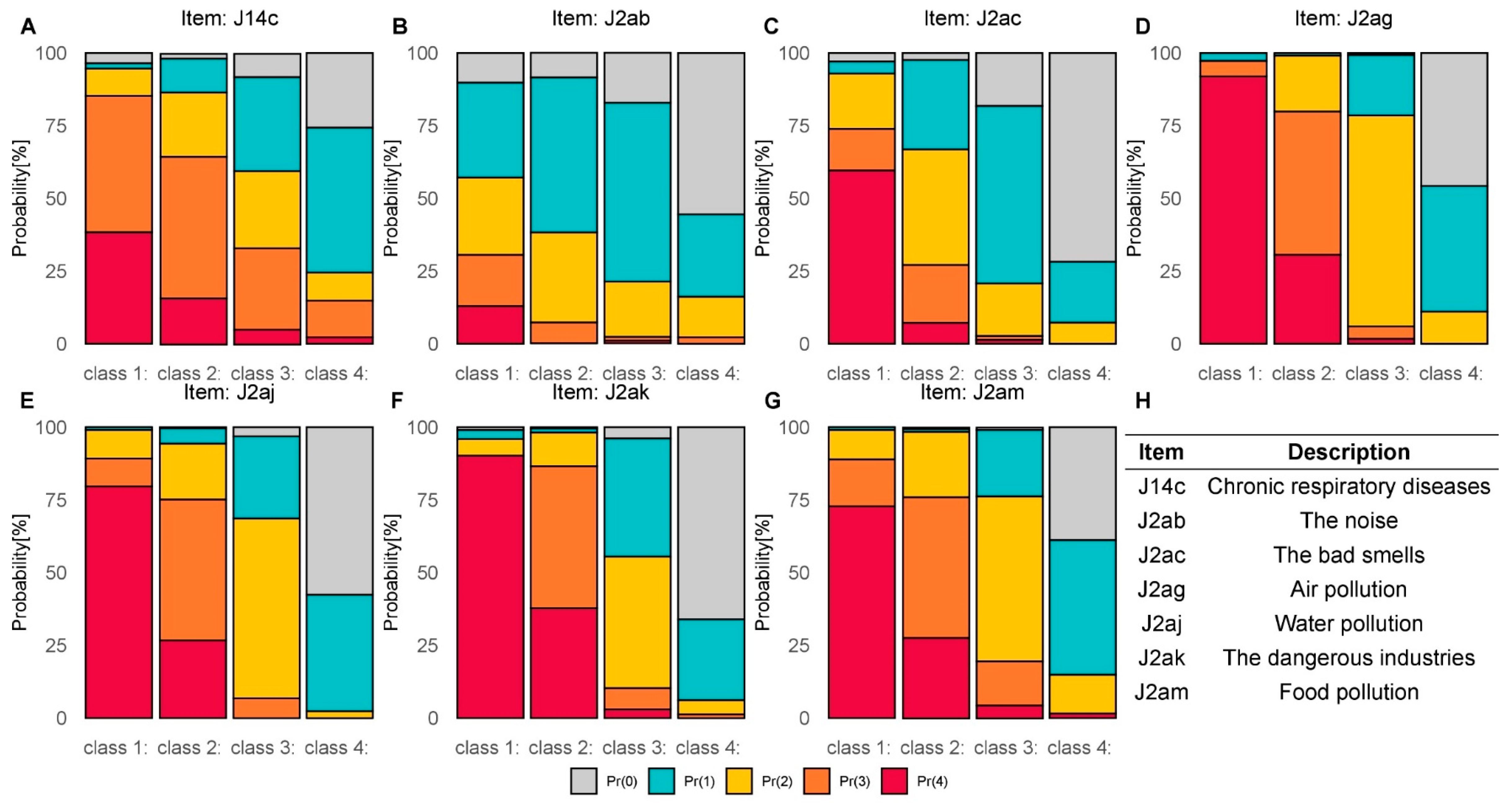
3.4. Latent Class Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barker, D.J.P. The origins of the developmental origins theory. J. Intern. Med. 2007, 261, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Prüss-Üstün, A.; Wolf, J.; Corvalán, C.; Bos, R.; Neira, M. Preventing Disease through Healthy Environments: A Global Assessment of the Burden of Disease from Environmental Risks, 2nd ed.; World Health Organization: Geneva, Switzerland, 2016; ISBN 978-92-4-156519-6. [Google Scholar]
- Fleming, T.P.; Watkins, A.J.; Velazquez, M.A.; Mathers, J.C.; Prentice, A.M.; Stephenson, J.; Barker, M.; Saffery, R.; Yajnik, C.S.; Eckert, J.J.; et al. Origins of lifetime health around the time of conception: Causes and consequences. Lancet 2018, 391, 1842–1852. [Google Scholar] [CrossRef]
- European Environment Agency, Human Activities. Available online: https://www.eea.europa.eu/publications/92-827-5122-8/page011.html (accessed on 20 September 2021).
- D’Alessandro, D.; Arletti, S.; Azara, A. Strategies for Disease Prevention and Health Promotion in Urban Areas: Erice 50 Charter. Ann. Ig. 2017, 6, 481–493. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. Healthy Environments for Healthier People. 2018. Available online: https://www.euro.who.int/__data/assets/pdf_file/0006/367188/eceh-eng.pdf (accessed on 20 September 2021).
- Dettori, M.; Pittaluga, P.; Busonera, G.; Gugliotta, C.; Azara, A.; Piana, A.; Arghittu, A.; Castiglia, P. Environmental Risks Perception Among Citizens Living Near Industrial Plants: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 4870. [Google Scholar] [CrossRef] [PubMed]
- Vrijheid, M.; Casas, M.; Gascon, M.; Valvi, D.; Nieuwenhuijsen, M. Environmental pollutants and child health—A review of recent concerns. Int. J. Hyg. Environ. Health 2016, 219, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Duan, X.; Feng, W.; He, J.; Cao, S.; Liu, S.; Shi, D.; Wang, H.; Wu, F. Health risks to metals in multimedia via ingestion pathway for children in a typical urban area of China. Chemosphere 2019, 226, 381–387. [Google Scholar] [CrossRef]
- Gluckman, P.D.; Hanson, M.A.; Cooper, C.; Thornburg, K.L. Effect of In Utero and Early-Life Conditions on Adult Health and Disease. N. Engl. J. Med. 2008, 359, 61–73. [Google Scholar] [CrossRef] [Green Version]
- Friedrich, M.J. Global Impact of Air Pollution on Children’s Health. JAMA 2018, 320, 2412. [Google Scholar] [CrossRef]
- Bustaffa, E.; Minichilli, F.; Andreassi, M.G.; Carone, S.; Coi, A.; Cori, L.; Faita, F.; Faita, F.; Grecchi, S.; Minoia, C.; et al. Epidemiological surveillance in areas with environmental pollution by natural or anthropogenic arsenic (SEpiAs CCM 2010). Epidemiol. Prev. 2014, 68, 27–94. [Google Scholar]
- De Felip, E.; Bianchi, F.; Bove, C.; Cori, L.; D’Argenzio, A.; D’Orsi, G.; Fusco, M.; Miniero, R.; Ortolani, R.; Palombino, R.; et al. Priority persistent contaminants in people dwelling in critical areas of Campania Region, Italy (SEBIOREC biomonitoring study). Sci. Total Environ. 2014, 487, 420–435. [Google Scholar] [CrossRef]
- Mudu, P.; Terracini, B.; Martuzzi, M. Human Health in Areas with Industrial Contamination; WHO Regional Office for Europe: Copenhagen, Denmark, 2014; ISBN 9789289050050. [Google Scholar]
- Colles, A.; Ardeleanu, E.R.; Cendeias, C.; Ranzi, A.; Demeter, Z.; Hofer, A.; Kowalska, M.; Makris, K.C.; Arrebola, J.P.; Schoeters, G.; et al. Human biomonitoring as a tool for exposure assessment in industrially contaminated sites (ICSs). Lessons learned within the ICS and Health European Network. Epidemiol. Prev. 2019, 43, 249–259. [Google Scholar] [CrossRef]
- Uhl, M.; Santos, R.R.; Costa, J.; Santos, O.; Virgolino, A.; Evans, D.S.; Murray, C.; Mulcahy, M.; Ubong, D.; Sepai, O.; et al. Chemical exposure: European citizens’ perspectives, trust, and concerns on human biomonitoring initiatives, information needs, and scientific results. Int. J. Environ. Res. Public Health 2021, 18, 1532. [Google Scholar] [CrossRef]
- Renn, O.; Kastenholz, H. Risk Communication Chemical Product Risks: An OECD Background Paper; Bundesinstitut für gesundheitlichen Verbraucherschutz und Veterinärmedizin: Berlin, Germany, 2000. [Google Scholar]
- Wise, T.; Zbozinek, T.D.; Michelini, G.; Hagan, C.C.; Mobbs, D. Changes in risk perception and self-reported protective behaviour during the first week of the COVID-19 pandemic in the United States. R. Soc. Open Sci. 2020, 7, 200742. [Google Scholar] [CrossRef] [PubMed]
- Bödeker, B.; Betsch, C.; Wichmann, O. Skewed risk perceptions in pregnant women: The case of influenza vaccination. BMC Public Health 2015, 15, 1308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, A.F.; Carter, C.S.; Davis, J.M.; Golding, J.; Adejumo, O.; Pyra, M.; Connelly, J.J.; Rubin, L.H. Childbirth and symptoms of postpartum depression and anxiety: A prospective birth cohort study. Arch. Womens Ment. Health 2016, 19, 219–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Junge, C.; von Soest, T.; Weidner, K.; Seidler, A.; Eberhard-Gran, M.; Garthus-Niegel, S. Labor pain in women with and without severe fear of childbirth: A population-based, longitudinal study. Birth 2018, 45, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Martínez, A.; Martínez-Vazquez, S.; Rodríguez-Almagro, J.; Delgado-Rodríguez, M.; Martínez-Galiano, J. Elaboration and Validation of Two Predictive Models of Postpartum Traumatic Stress Disorder Risk Formed by Variables Related to the Birth Process: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 18, 92. [Google Scholar] [CrossRef]
- Ruggieri, S.; Drago, G.; Colombo, P.; Alesci, A.; Augello, P.; Bisbano, A.; Bucolo, A.; Dattoli, P.; De Sole, R.; La Runa, V.; et al. Three contaminated sites in southern Italy. The Neonatal Environment and Health Outcomes cohort: Protocol for a longitudinal birth cohort study. BMJ Open 2019, 9, e029471. [Google Scholar] [CrossRef] [Green Version]
- Ruggieri, S.; Maltese, S.; Drago, G.; Cibella, F.; Panunzi, S. The Neonatal Environment and Health Outcomes (NEHO) Birth Cohort Study: Behavioral and Socioeconomic Characteristics and Drop-Out Rate from a Longitudinal Birth Cohort in Three Industrially Contaminated Sites in Southern Italy. Int. J. Environ. Res. Public Health 2021, 18, 1252. [Google Scholar] [CrossRef]
- Drago, G.; Ruggieri, S.; Bianchi, F.; Sampino, S.; Cibella, F. Birth cohorts in highly contaminated sites: A tool for monitoring the relationships between environmental pollutants and children’s health. Front. Public Health 2020, 8, 125. [Google Scholar] [CrossRef]
- Longo, V.; Longo, A.; Di Sano, C.; Cigna, D.; Cibella, F.; Di Felice, G.; Colombo, P. In vitro exposure to 2,2′,4,4′-tetrabromodiphenyl ether (PBDE-47) impairs innate inflammatory response. Chemosphere 2019, 219, 845–854. [Google Scholar] [CrossRef]
- Albano, G.D.; Moscato, M.; Montalbano, A.M.; Anzalone, G.; Gagliardo, R.; Bonanno, A.; Giacomazza, D.; Barone, R.; Drago, G.; Cibella, F.; et al. Can PBDEs affect the pathophysiologic complex of epithelium in lung diseases? Chemosphere 2020, 241, 125087. [Google Scholar] [CrossRef]
- Di Bella, C.; Traina, A.; Giosuè, C.; Carpintieri, D.; Lo Dico, G.M.; Bellante, A.; Del Core, M.; Falco, F.; Gherardi, S.; Uccello, M.M.; et al. Heavy metals and PAHS in meat, milk, and seafood from Augusta area (southern Italy): Contamination levels, dietary intake, and human exposure assessment. Front. Public Health 2020, 8, 273. [Google Scholar] [CrossRef] [PubMed]
- Gorini, F.; Bustaffa, E.; Bolignano, D.; Cori, L.; Faita, F.; Gastaldelli, A.; Interdonato, M.; Minichilli, F.; Quattrone, G.; Squadrito, F.; et al. Biomarkers of exposure and early effect in three contaminated sites of southern Italy: Protocols for etiological epidemiological studies. BMJ Open 2020, 10, e036160. [Google Scholar] [CrossRef] [PubMed]
- Montalbano, A.M.; Albano, G.D.; Anzalone, G.; Moscato, M.; Gagliardo, R.; Di Sano, C.; Bonanno, A.; Ruggieri, S.; Cibella, F.; Profita, M. Cytotoxic and genotoxic effects of the flame retardants (PBDE-47, PBDE-99 and PBDE-209) in human bronchial epithelial cells. Chemosphere 2020, 245, 125600. [Google Scholar] [CrossRef] [PubMed]
- Pagliaro, M.; Meneguzzo, F. Oil refining in Sicily: A critical perspective looking to the future. Energy Sci. Eng. 2020, 8, 566–573. [Google Scholar] [CrossRef]
- Marchiol, L.; Fellet, G.; Boscutti, F.; Montella, C.; Mozzi, R.; Guarino, C. Gentle remediation at the former “Pertusola Sud” zinc smelter: Evaluation of native species for phytoremediation purposes. Ecol. Eng. 2013, 53, 343–353. [Google Scholar] [CrossRef]
- Lima, M.L.; Barnett, J.; Vala, J. Risk perception and technological development at a societal level. Risk Anal. 2005, 25, 1229–1239. [Google Scholar] [CrossRef]
- Gerber, B.J.; Neeley, G.W. Perceived Risk and Citizen Preferences for Governmental Management of Routine Hazards. Policy Stud. J. 2005, 33, 395–418. [Google Scholar] [CrossRef]
- Signorino, G.; Beck, E. Addressing Risk Perception and Local Attitudes. Risk Perception Survey in Two High-Risk Areas. Human Health in Areas with Industrial Contamination 15; WHO Regional Office for Europe: Copenhagen, Denmark, 2014; p. 232. [Google Scholar]
- Bianchi, F.; Bustaffa, E.; Coi, A.; Cori, L.; Curzio, O.; Gorini, F.; Minichilli, F.; Santoro, M. Percezione del Rischio Legato alle Emissioni degli Impianti Geotermici nella Popolazione dei Territori dell’Amiata. 2019. Available online: https://publications.cnr.it/doc/437136 (accessed on 20 September 2021).
- Coi, A.; Minichilli, F.; Bustaffa, E.; Carone, S.; Santoro, M.; Bianchi, F.; Cori, L. Risk perception and access to environmental information in four areas in Italy affected by natural or anthropogenic pollution. Environ. Int. 2016, 95, 8–15. [Google Scholar] [CrossRef]
- Bena, A.; Gandini, M.; Cadum, E.; Procopio, E.; Salamina, G.; Orengia, M.; Farina, E. Risk perception in the population living near the Turin municipal solid waste incineration plant: Survey results before start-up and communication strategies. BMC Public Health 2019, 19, 483. [Google Scholar] [CrossRef]
- Minichilli, F.; Gorini, F.; Ascari, E.; Bianchi, F.; Coi, A.; Fredianelli, L.; Licitra, G.; Manzoli, F.; Mezzasalma, L.; Cori, L. Annoyance Judgment and Measurements of Environmental Noise: A Focus on Italian Secondary Schools. Int. J. Environ. Res. Public Health 2018, 15, 208. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, S.; Cribari-Neto, F. Beta Regression for Modelling Rates and Proportions. J. Appl. Stat. 2004, 31, 799–815. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: http://www.R-project.org (accessed on 20 September 2021).
- Lennon, S.L. Risk perception in pregnancy: A concept analysis. J. Adv. Nurs. 2016, 72, 2016–2029. [Google Scholar] [CrossRef]
- Robinson, M.; Pennell, C.E.; McLean, N.J.; Tearne, J.E.; Oddy, W.H.; Newnham, J.P. Risk perception in pregnancy: Context, consequences, and clinical implications. Eur. Psychol. 2015, 20, 120–127. [Google Scholar] [CrossRef]
- Landrigan, P.J.; Fuller, R.; Fisher, S.; Suk, W.A.; Sly, P.; Chiles, T.C.; Bose-O’Reilly, S. Pollution and children’s health. Sci. Total Environ. 2019, 650, 2389–2394. [Google Scholar] [CrossRef]
- Manisalidis, I.; Stavropoulou, E.; Stavropoulos, A.; Bezirtzoglou, E. Environmental and health impacts of air pollution: A Review. Front. Public Health 2020, 8, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durmuş-Özdemir, E.; Şener, S. The Impact of Higher Education on Environmental Risk Perceptions. CUBR 2016, 15, 459–471. [Google Scholar] [CrossRef] [Green Version]
- Carducci, A.; Fiore, M.; Azara, A.; Bonaccorsi, G.; Bortoletto, M.; Caggiano, G.; Calamusa, A.; De Donno, A.; De Giglio, O.; Dettori, M.; et al. Environment and health: Risk perception and its determinants among Italian university students. Sci. Total Environ. 2019, 691, 1162–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khammaneechan, P.; Okanurak, K.; Sithisarankul, P.; Tantrakarnapa, K.; Norramit, P. Community concerns about a healthcare-waste incinerator. J. Risk Res. 2011, 14, 847–858. [Google Scholar] [CrossRef]
- Cavazza, N.; Rubichi, S. Ways of thinking about the incinerator: A typology of citizens’ mindsets. Soc. Sci. J. 2014, 51, 422–430. [Google Scholar] [CrossRef]
- Cori, L.; Donzelli, G.; Gorini, F.; Bianchi, F.; Curzio, O. Risk Perception of Air Pollution: A Systematic Review Focused on Particulate Matter Exposure. Int. J. Environ. Res. Public Health 2020, 17, 6424. [Google Scholar] [CrossRef] [PubMed]
- ARPA Sicily, NOSE (Network for Odour SEnsitivity). Available online: https://www.arpa.sicilia.it/temi-ambientali/aria/nose-network-for-odour-sensitivity/ (accessed on 20 September 2021).
- Cori, L.; Bianchi, F.; Sprovieri, M.; Cuttitta, A.; Ruggieri, S.; Alessi, A.L.; Biondo, G.; Gorini, F. Communication and Community Involvement to Support Risk Governance. Int. J. Environ. Res. Public Health 2019, 16, 4356. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| AUGUSTA PRIOLO | CROTONE | MILAZZO | COHORT | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Quantitative Variables | TOTAL | NCPS | LRA | TOTAL | NCPS | LRA | TOTAL | NCPS | LRA | TOTAL | NCPS | LRA |
| * p value = 0.99 | * p value = 0.035 | * p value = 0.14 | & p value = 0.049 | % p value = 0.19 | ||||||||
| Age (years) | 31.3 (±4.9) | 31.3 (±4.97) | 31.3 (±4.9) | 31.2 (±5) | 31.8 (±5.3) | 29.9 (±4.2) | 32.7 (±4.3) | 33.3 (±4) | 31.8 (±4.6) | 31.5 (±4.9) | 31.6 (±5) | 31.1 (±4.8) |
| * p value = 0.14 | * p value = 0.53 | * p value = 0.33 | & p value = 0.29 | %p value = 0.07 | ||||||||
| BMI (kg/m2) | 23.5 (±4.6) | 23.8 (±4.79) | 23.1 (±4.3) | 23.2 (±3.8) | 23.3 (±4.05) | 22.9 (±3.1) | 22.7 (±3.8) | 23 (±4) | 22.2 (±3.6) | 23.3 (±4.3) | 23.6 (±4.5) | 22.9 (±4) |
| * p value = 0.38 | * p value = 0.15 | * p value = 0.61 | & p value = 0.015 | % p value = 0.09 | ||||||||
| Weight (kg) | 12.1 (±4.1) | 11.9 (±3.93) | 12.3 (±4.3) | 11.4 (±4.4) | 10.9 (±3.75) | 12.3 (±5.2) | 13.1 (±4.1) | 12.9 (±4.1) | 13.4 (±4.2) | 12.1 (±4.1) | 11.9 (±3.9) | 12.5 (±4.5) |
| * p value = 0.016 | * p value = 0.23 | * p value = 0.05 | & p value = 0.37 | % p value < 0.01 | ||||||||
| Crowding Index | 1.16 (±0.56) | 1.21 (±0.61) | 1.07 (±0.46) | 1.13 (±0.54) | 1.17 (±0.55) | 1.05 (±0.49) | 1.06 (±0.45) | 1.14 (±0.47) | 0.95 (±0.4) | 1.14 (±0.54) | 1.19 (±0.58) | 1.05 (±0.45) |
| AUGUSTA PRIOLO | CROTONE | MILAZZO | COHORT | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TOTAL | NPCS | LRA | TOTAL | NPCS | LRA | TOTAL | NPCS | LRA | TOTAL | NPCS | LRA | |
| 406 (66.5%) | 253 (62.3%) | 153 (37.7%) | 121 (19.8%) | 82 (67.8%) | 39 (32.2%) | 84 (13.7%) | 50 (59.5%) | 34 (40.5%) | 611 | 385 (63.0%) | 226 (37.0%) | |
| Marital status | * p value = 0.26 | * p value = 0.097 | * p value = 0.65 | & p value = 0.44 | % p value = 0.04 | |||||||
| Married | 256 (63.4%) | 154 (61.3%) | 102 (66.7%) | 84 (69.4%) | 52 (63.5%) | 32 (82.1%) | 59 (70.2%) | 34 (68%) | 25 (73.5%) | 399 (65.5%) | 240 (62.7%) | 159 (70.4%) |
| Maiden | 145 (35.9%) | 94 (37.5%) | 51 (33.3%) | 35 (28.9%) | 28 (34.1%) | 7 (17.9%) | 24 (28.6%) | 15 (30%) | 9 (26.5%) | 204 (33.5%) | 137 (35.8%) | 67 (29.6%) |
| Divorced/Separated | 3 (0.7%) | 3 (1.2%) | 0 (0%) | 2 (1.7%) | 2 (2.4%) | 0 (0%) | 1 (1.2%) | 1 (2%) | 0 (0%) | 6 (1%) | 6 (1.5%) | 0 (0%) |
| Total | 404 (100%) | 251 (100%) | 153 (100%) | 121 (100%) | 82 (100%) | 39 (100%) | 84 (100%) | 50 (100%) | 34 (100%) | 609 (100%) | 383 (100%) | 226 (100%) |
| Educational level | * p value = 0.43 | * p value = 0.67 | * p value < 0.01 | & p value = 0.02 | % p value = 0.13 | |||||||
| Second. school or lower qualific. | 74 (18.3%) | 50 (19.8%) | 24 (15.8%) | 17 (14.3%) | 10 (12.3%) | 7 (18.4%) | 5 (6%) | 3 (6%) | 2 (5.9%) | 96 (15.8%) | 63 (16.4%) | 33 (14.7%) |
| High school | 220 (54.5%) | 138 (54.8%) | 82 (53.9%) | 63 (52.9%) | 44 (54.4%) | 19 (50%) | 44 (52.4%) | 33 (66%) | 11 (32.4%) | 327 (53.9%) | 215 (56.2%) | 112 (50%) |
| Degree or higher qualific. | 110 (27.2%) | 64 (25.4%) | 46 (30.3%) | 39 (32.8%) | 27 (33.3%) | 12 (31.6%) | 35 (41.6%) | 14 (28%) | 21 (61.7%) | 184 (30.3%) | 105 (27.4%) | 79 (35.3%) |
| Total | 404 (100%) | 252 (100%) | 152 (100%) | 119 (100%) | 81 (100%) | 38 (100%) | 84 (100%) | 50 (100%) | 34 (100%) | 607 (100%) | 383 (100%) | 224 (100%) |
| Working condition | * p value = 0.44 | * p value = 0.014 | * p value = 0.09 | & p value < 0.01 | % p value = 0.85 | |||||||
| NO | 267 (66.6%) | 170 (68%) | 97 (64.2%) | 62 (52.1%) | 36 (44.4%) | 26 (68.4%) | 26 (31%) | 19 (38%) | 7 (20.6%) | 355 (58.8%) | 225 (59.1%) | 130 (58.3%) |
| YES | 134 (33.4%) | 80 (32%) | 54 (35.8%) | 57 (47.9%) | 45 (55.6%) | 12 (31.6%) | 58 (69%) | 31 (62%) | 27 (79.4%) | 249 (41.2%) | 156 (40.9%) | 93 (41.7%) |
| Total | 401 (100%) | 250 (100%) | 151 (100%) | 119 (100%) | 81 (100%) | 38 (100%) | 84 (100%) | 50 (100%) | 34 (100%) | 604 (100%) | 381 (100%) | 223 (100%) |
| Active smoke | * p value = 0.57 | * p value = 0.96 | * p value = 0.34 | & p value = 0.53 | % p value = 0.84 | |||||||
| NO | 366 (90.6%) | 229 (91.2%) | 137 (89.5%) | 111 (92.5%) | 75 (92.6%) | 36 (92.3%) | 79 (94%) | 46 (92%) | 33 (97.1%) | 556 (91.4%) | 350 (91.6%) | 206 (91.2%) |
| YES | 38 (9.4%) | 22 (8.8%) | 16 (10.5%) | 9 (7.5%) | 6 (7.4%) | 3 (7.7%) | 5 (6%) | 4 (8%) | 1 (2.9%) | 52 (8.6%) | 32 (8.4%) | 20 (8.8%) |
| Total | 404 (100%) | 251 (100%) | 153 (100%) | 120 (100%) | 81 (100%) | 39 (100%) | 84 (100%) | 50 (100%) | 34 (100%) | 608 (100%) | 382 (100%) | 226 (100%) |
| Passive smoke | * p value = 0.10 | * p value = 0.93 | * p value = 0.87 | & p value < 0.01 | % p value = 0.24 | |||||||
| NO | 377 (92.9%) | 239 (94.5%) | 138 (90.2%) | 105 (86.8%) | 71 (86.6%) | 34 (87.2%) | 65 (77.4%) | 39 (78%) | 26 (76.5%) | 547 (89.5%) | 349 (90.6%) | 198 (87.6%) |
| YES | 29 (7.1%) | 14 (5.5%) | 15 (9.8%) | 16 (13.2%) | 11 (13.4%) | 5 (12.8%) | 19 (22.6%) | 11 (22%) | 8 (23.5%) | 64 (10.5%) | 36 (9.4%) | 28 (12.4%) |
| Total | 406 (100%) | 253 (100%) | 153 (100%) | 121 (100%) | 82 (100%) | 39 (100%) | 84 (100%) | 50 (100%) | 34 (100%) | 611 (100%) | 385 (100%) | 226 (100%) |
| Consumption of alcohol | * p value = 0.41 | * p value = 0.10 | * p value = 0.24 | & p value < 0.01 | % p value = 0.04 | |||||||
| NO | 400 (98.8%) | 248 (98.4%) | 152 (99.3%) | 107 (91.5%) | 69 (88.5%) | 38 (97.4%) | 72 (85.7%) | 41 (82%) | 31 (91.2%) | 579 (95.5%) | 358 (94.2%) | 221 (97.8%) |
| YES | 5 (1.2%) | 4 (1.6%) | 1 (0.7%) | 10 (8.5%) | 9 (11.5%) | 1 (2.6%) | 12 (14.3%) | 9 (18%) | 3 (8.8%) | 27 (4.5%) | 22 (5.8%) | 5 (2.2%) |
| Total | 405 (100%) | 252 (100%) | 153 (100%) | 117 (100%) | 78 (100%) | 39 (100%) | 84 (100%) | 50 (100%) | 34 (100%) | 606 (100%) | 380 (100%) | 226 (100%) |
| Sport | * p value = 0.18 | * p value = 0.21 | * p value = 0.09 | & p value < 0.01 | % p value = 0.34 | |||||||
| NO | 385 (94.8%) | 237 (93.7%) | 148 (96.7%) | 105 (86.8%) | 69 (84.1%) | 36 (92.3%) | 75 (89.3%) | 47 (94%) | 28 (82.4%) | 565 (92.5%) | 353 (91.7%) | 212 (93.8%) |
| YES | 21 (5.2%) | 16 (6.3%) | 5 (3.3%) | 16 (13.2%) | 13 (15.9%) | 3 (7.7%) | 9 (10.7%) | 3 (6%) | 6 (17.6%) | 46 (7.5%) | 32 (8.3%) | 14 (6.2%) |
| Total | 406 (100%) | 253 (100%) | 153 (100%) | 121 (100%) | 82 (100%) | 39 (100%) | 84 (100%) | 50 (100%) | 34 (100%) | 611 (100%) | 385 (100%) | 226 (100%) |
| Pressure | * p value = 0.51 | * p value = 0.06 | * p value = 0.35 | & p value = 0.55 | % p value = 0.34 | |||||||
| NO | 366 (90.1%) | 230 (90.9%) | 136 (88.9%) | 113 (93.4%) | 79 (96.3%) | 34 (87.2%) | 76 (90.5%) | 44 (88%) | 32 (94.1%) | 555 (90.8%) | 353 (91.7%) | 202 (89.4%) |
| YES | 40 (9.9%) | 23 (9.1%) | 17 (11.1%) | 8 (6.6%) | 3 (3.7%) | 5 (12.8%) | 8 (9.5%) | 6 (12%) | 2 (5.9%) | 56 (9.2%) | 32 (8.3%) | 24 (10.6%) |
| Total | 406 (100%) | 253 (100%) | 153 (100%) | 121 (100%) | 82 (100%) | 39 (100%) | 84 (100%) | 50 (100%) | 34 (100%) | 611 (100%) | 385 (100%) | 226 (100%) |
| Cardiovascular | * p value = 0.81 | - | * p value = 0.42 | & p value = 0.41 | % p value = 0.64 | |||||||
| NO | 390 (98.5%) | 241 (98.4%) | 149 (98.7%) | 118 (100%) | 80 (100%) | 38 (100%) | 81 (98.8%) | 49 (98%) | 32 (100%) | 589 (98.8%) | 370 (98.7%) | 219 (99.1%) |
| YES | 6 (1.5%) | 4 (1.6%) | 2 (1.3%) | 1 (1.2%) | 1 (2%) | 0 (0%) | 7 (1.2%) | 5 (1.3%) | 2 (0.9%) | |||
| Total | 396 (100%) | 245 (100%) | 151 (100%) | 118 (100%) | 80 (100%) | 38 (100%) | 82 (100%) | 50 (100%) | 32 (100%) | 596 (100%) | 375 (100%) | 221 (100%) |
| Cholesterol | * p value = 0.11 | *p value = 0.40 | * p value = 0.54 | & p value = 0.96 | % p value = 0.45 | |||||||
| NO | 374 (94.4%) | 233 (95.9%) | 141 (92.2%) | 112 (94.9%) | 75 (93.8%) | 37 (97.4%) | 77 (95.1%) | 46 (93.9%) | 31 (96.9%) | 563 (94.6%) | 354 (95.2%) | 209 (93.7%) |
| YES | 22 (5.6%) | 10 (4.1%) | 12 (7.8%) | 6 (5.1%) | 5 (6.3%) | 1 (2.6%) | 4 (4.9%) | 3 (6.1%) | 1 (3.1%) | 32 (5.4%) | 18 (4.8%) | 14 (6.3%) |
| Total | 396 (100%) | 243 (100%) | 153 (100%) | 118 (100%) | 80 (100%) | 38 (100%) | 81 (100%) | 49 (100%) | 32 (100%) | 595 (100%) | 372 (100%) | 223 (100%) |
| Psychic disorders | * p value = 0.72 | * p value = 0.38 | * p value = 0.64 | & p value = 0.54 | % p value = 0.81 | |||||||
| NO | 285 (70.2%) | 176 (69.6%) | 109 (71.2%) | 87 (71.9%) | 61 (74.4%) | 26 (66.7%) | 64 (76.2%) | 39 (78%) | 25 (73.5%) | 436 (71.4%) | 276 (71.7%) | 160 (70.8%) |
| YES | 121 (29.8%) | 77 (30.4%) | 44 (28.8%) | 34 (28.1%) | 21 (25.6%) | 13 (33.3%) | 20 (23.8%) | 11 (22%) | 9 (26.5%) | 175 (28.6%) | 109 (28.3%) | 66 (29.2%) |
| Total | 406 (100%) | 253 (100%) | 153 (100%) | 121 (100%) | 82 (100%) | 39 (100%) | 84 (100%) | 50 (100%) | 34 (100%) | 611 (100%) | 385 (100%) | 226 (100%) |
| AUGUSTA PRIOLO | CROTONE | MILAZZO | COHORT | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Indexes | TOTAL | NPCS | LRA | TOTAL | NPCS | LRA | TOTAL | NPCS | LRA | TOTAL | NPCS | LRA |
| * p value < 0.001 | * p value = 0.16 | * p value = 0.03 | & p value < 0.001 | % p value < 0.001 | ||||||||
| EHPI | 0.53 (±0.23) | 0.59 (±0.22) | 0.44 (±0.21) | 0.47 (±0.24) | 0.49 (±0.23) | 0.43 (±0.26) | 0.61 (±0.2) | 0.65 (±0.18) | 0.56 (±0.21) | 0.53 (±0.23) | 0.58 (±0.22) | 0.45 (±0.22) |
| * p value < 0.001 | * p value = 0.82 | * p value = 0.01 | & p value < 0.01 | % p value < 0.001 | ||||||||
| HRPI | 0.58 (±0.27) | 0.63 (±0.27) | 0.51 (±0.26) | 0.58 (±0.24) | 0.58 (±0.24) | 0.59 (±0.24) | 0.68 (±0.2) | 0.73 (±0.15) | 0.59 (±0.23) | 0.59 (±0.26) | 0.63 (±0.25) | 0.53 (±0.26) |
| * p value < 0.001 | * p value < 0.01 | * p value = 0.04 | & p value < 0.001 | % p value < 0.001 | ||||||||
| HPI | 0.45 (±0.26) | 0.51 (±0.26) | 0.33 (±0.23) | 0.34 (±0.23) | 0.38 (±0.23) | 0.25 (±0.18) | 0.57 (±0.24) | 0.61 (±0.22) | 0.5 (±0.24) | 0.44 (±0.26) | 0.5 (±0.26) | 0.35 (±0.23) |
| * p value < 0.001 | * p value = 0.45 | * p value < 0.01 | & p value < 0.001 | % p value < 0.001 | ||||||||
| RPI | 0.54 (±0.22) | 0.6 (±0.21) | 0.45 (±0.19) | 0.5 (±0.18) | 0.51 (±0.18) | 0.48 (±0.19) | 0.64 (±0.16) | 0.69 (±0.13) | 0.57 (±0.18) | 0.55 (±0.21) | 0.59 (±0.2) | 0.47 (±0.19) |
| AUGUSTA PRIOLO | CROTONE | MILAZZO | COHORT | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Indexes | TOTAL | NPCS | LRA | TOTAL | NPCS | LRA | TOTAL | NPCS | LRA | TOTAL | NPCS | LRA |
| * p value < 0.001 | * p value = 0.83 | * p value < 0.01 | & p value < 0.01 | % p value < 0.01 | ||||||||
| FACTOR 1 | 0.58 (±0.27) | 0.63 (±0.27) | 0.5 (±0.26) | 0.57 (±0.24) | 0.57 (±0.24) | 0.58 (±0.24) | 0.68 (±0.2) | 0.73 (±0.15) | 0.59 (±0.23) | 0.59 (±0.26) | 0.63 (±0.25) | 0.53 (±0.26) |
| * p value < 0.001 | * p value = 0.11 | * p value = 0.09 | & p value < 0.001 | % p value < 0.01 | ||||||||
| FACTOR 2 | 0.59 (±0.25) | 0.64 (±0.25) | 0.49 (±0.24) | 0.54 (±0.27) | 0.57 (±0.25) | 0.47 (±0.31) | 0.68 (±0.22) | 0.71 (±0.21) | 0.63 (±0.22) | 0.59 (±0.26) | 0.64 (±0.25) | 0.51 (±0.25) |
| * p value = 0.68 | * p value = 0.09 | * p value = 0.01 | &p = 0.33 | % p value = 0.03 | ||||||||
| FACTOR 3 | 0.47 (±0.26) | 0.48 (±0.26) | 0.46 (±0.27) | 0.46 (±0.34) | 0.49 (±0.32) | 0.37 (±0.37) | 0.51 (±0.3) | 0.58 (±0.28) | 0.41 (±0.3) | 0.47 (±0.28) | 0.49 (±0.28) | 0.44 (±0.29) |
| * p value < 0.001 | * p value = 0.48 | * p value < 0.001 | & p value < 0.001 | % p value < 0.01 | ||||||||
| FACTOR 4 | 0.44 (±0.21) | 0.5 (±0.21) | 0.34 (±0.17) | 0.32 (±0.19) | 0.33 (±0.2) | 0.31 (±0.18) | 0.49 (±0.22) | 0.56 (±0.18) | 0.39 (±0.23) | 0.42 (±0.22) | 0.47 (±0.22) | 0.34 (±0.18) |
| * p value < 0.001 | * p value = 0.62 | * p value < 0.001 | & p value < 0.001 | % p value < 0.01 | ||||||||
| TOTAL EFA | 0.56 (±0.22) | 0.62 (±0.21) | 0.47 (±0.19) | 0.52 (±0.19) | 0.53 (±0.19) | 0.51 (±0.19) | 0.65 (±0.16) | 0.71 (±0.13) | 0.58 (±0.18) | 0.57 (±0.21) | 0.61 (±0.21) | 0.49 (±0.19) |
| CLASS 1 High Risk | CLASS 2 Medium/High | CLASS 3 Low/Medium | CLASS 4 Low Risk | TOTAL | ||
|---|---|---|---|---|---|---|
| COHORT | 105 (17.2%) | 209 (34.2%) | 224 (36.7%) | 73 (11.9%) | p value | 611 |
| NPCS | ||||||
| AUGUSTA-PRIOLO | 68 (16.7%) | 141 (34.7%) | 148 (36.5%) | 49 (12.1%) | ** p value < 0.001 | 406 (66.4%) |
| CROTONE | 14 (11.6%) | 35 (28.9%) | 49 (40.5%) | 23 (19%) | 121 (19.8%) | |
| MILAZZO-VALLE del MELA | 23 (27.4%) | 33 (39.3%) | 27 (32.1%) | 1 (1.2%) | 84 (13.7%) | |
| AREA | ||||||
| AT RISK AREA | 91 (23.6%) | 143 (37.1%) | 120 (31.2%) | 31 (8.1%) | ** p value < 0.001 | 385 (63%) |
| LOCAL REFERENCE AREA | 14 (6.2%) | 66 (29.2%) | 104 (46%) | 42 (18.6%) | 226 (37%) | |
| Educational level | ||||||
| secondary school or lower qualification | 20 (20.8%) | 27 (28.1%) | 30 (31.3%) | 19 (19.8%) | ** p value = 0.016 | 96 (15.8%) |
| high school | 54 (16.5%) | 122 (37.4%) | 111 (33.9%) | 40 (12.2%) | 327 (53.9%) | |
| Degree or higher qualification | 30 (16.3%) | 58 (31.5%) | 82 (44.6%) | 14 (7.6%) | 184 (30.3%) | |
| Total | 104 (17.1%) | 207 (34.1%) | 223 (36.8%) | 73 (12%) | 607 (100%) | |
| AGE | 31.8 ±(4.99) | 32 ±(4.71) | 31.3 ±(4.79) | 30.1 ±(5.33) | * p value = 0.03 | 31.5 ±(4.89) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruggieri, S.; Maltese, S.; Drago, G.; Panunzi, S.; Cibella, F.; Bianchi, F.; Minichilli, F.; Cori, L. Measuring Risk Perception in Pregnant Women in Heavily Polluted Areas: A New Methodological Approach from the NEHO Birth Cohort. Int. J. Environ. Res. Public Health 2021, 18, 10616. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010616
Ruggieri S, Maltese S, Drago G, Panunzi S, Cibella F, Bianchi F, Minichilli F, Cori L. Measuring Risk Perception in Pregnant Women in Heavily Polluted Areas: A New Methodological Approach from the NEHO Birth Cohort. International Journal of Environmental Research and Public Health. 2021; 18(20):10616. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010616
Chicago/Turabian StyleRuggieri, Silvia, Sabina Maltese, Gaspare Drago, Simona Panunzi, Fabio Cibella, Fabrizio Bianchi, Fabrizio Minichilli, and Liliana Cori. 2021. "Measuring Risk Perception in Pregnant Women in Heavily Polluted Areas: A New Methodological Approach from the NEHO Birth Cohort" International Journal of Environmental Research and Public Health 18, no. 20: 10616. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010616