
Barriers and Motivators to Physical Activity Prior to Starting a Community-Based Walking Program


Abstract
:1. Introduction
Study Background
2. Materials and Methods
2.1. Study Design
2.2. Participants and Recruitment
2.3. Measures
2.4. Analysis
3. Results
3.1. Participants
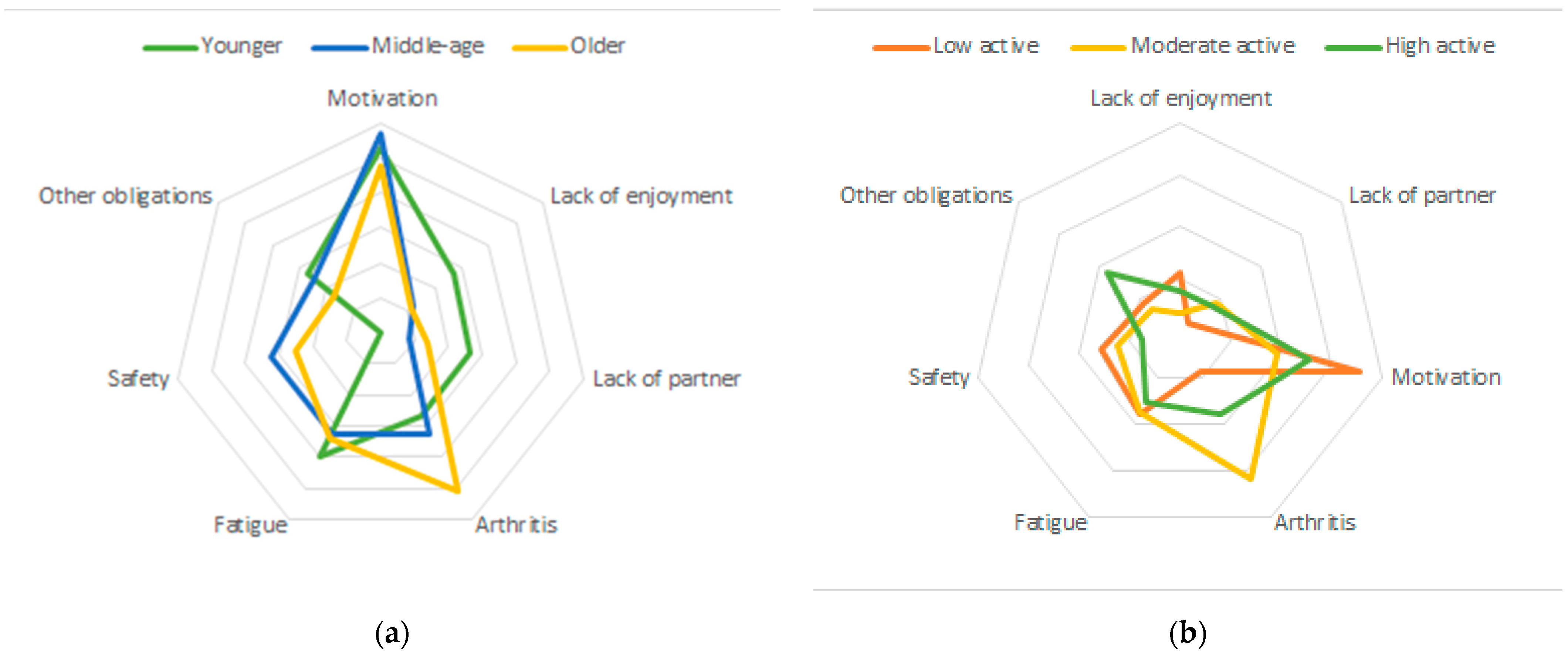
3.2. Barriers to Walking
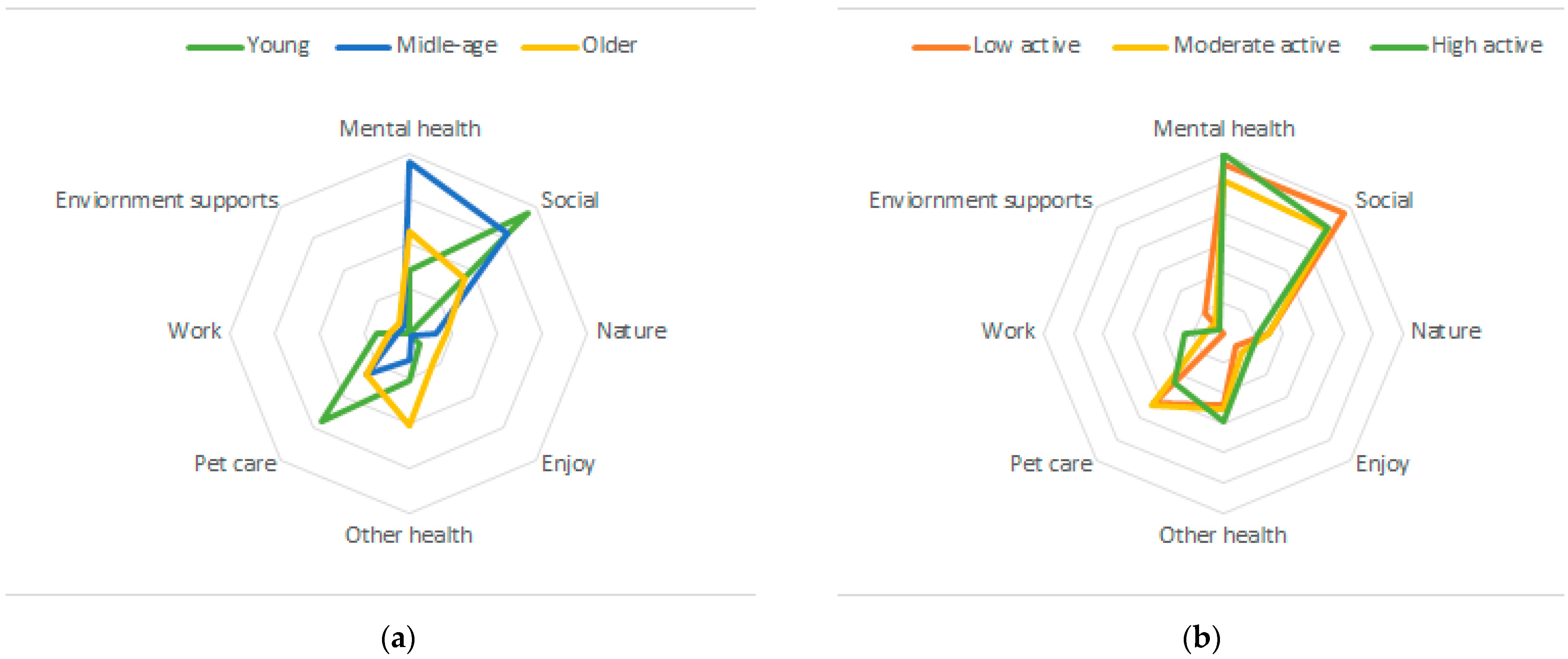
3.3. Motivators to Walking
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Centers for Disease Control and Prevention. Lack of Physical Activity. 2019. Available online: https://www.cdc.gov/chronicdisease/resources/publications/factsheets/physical-activity.htm (accessed on 27 July 2021).
- U.S. Department of Health and Human Services. Step it Up! The Surgeon General’s Call to Action to Promote Walking and Walkable Communities; U.S. Department of Health and Human Services, Office of the Surgeon General: Washington, DC, USA, 2015.
- Perry, C.; Rosenfeld, A.; Kendall, J. Rural women walking for health. West. J. Nurs. Res. 2008, 30, 295–316. [Google Scholar] [CrossRef]
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report. Washington D.C. 2018. Available online: https://health.gov/our-work/physical-activity/current-guidelines/scientific-report (accessed on 27 July 2021).
- Foster, C.; Kelly, P.; Reid, H.A.B.; Roberts, N.; Murtagh, E.M.; Humphreys, D.K.; Panter, J.; Milton, K. What works to promote walking at the population level? A systematic review. Br. J. Sports Med. 2018, 52, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Ory, M.G.; Yoon, J.; Forjuoh, S.N. Neighborhood walking among overweight and obese adults: Age variations in barriers and motivators. J. Community Health 2013, 38, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Capalb, D.J.; O’Halloran, P.; Liamputtong, P. Why older people engage in physical activity: An exploratory study of participants in a community-based walking program. Aust. J. Prim. Health 2014, 20, 74–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Normansell, R.; Smith, J.; Victor, C.; Cook, D.G.; Kerry, S.; Iliffe, S.; Ussher, M.; Fox-Rushby, J.; Whincup, P.; Harris, T. Numbers are not the whole story: A qualitative exploration of barriers and facilitators to increased physical activity in a primary care based walking intervention. BMC Public Health 2014, 14, 1272. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef]
- White, S.M.; Wójcicki, T.R.; McAuley, E. Social cognitive influences on physical activity behavior in middle-aged and older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2012, 67, 18–26. [Google Scholar] [CrossRef]
- Alharbi, M.; Gallagher, R.; Neubeck, L.; Bauman, A.; Prebill, G.; Kirkness, A.; Randall, S. Exercise barriers and the relationship to self-efficacy for exercise over 12 months of a lifestyle-change program for people with heart disease and/or diabetes. Eur. J. Cardiovasc. Nurs. 2017, 16, 309–317. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Self Control; W.H. Freeman and Company: New York, NY, USA, 1997. [Google Scholar]
- Richards, E.A.; Woodcox, S. County extension-delivered, e-mail mediated walking intervention: A program evaluation. Health Educ. J. 2018, 7, 615–624. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Barriers to Being Physically Active Quiz. Available online: https://www.cdc.gov/diabetes/ndep/pdfs/8-road-to-health-barriers-quiz-508.pdf (accessed on 20 August 2021).
- Zalewski, K.; Alt, C.; Arvinen-Barrow, M. Identifying barriers to remaining physically active after rehabilitation: Differences in perception between physical therapists and older adult patients. J. Orthop. Sports Phys. Ther. 2014, 44, 415–424. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Dzewaltowski, D.A. Physical activity determinants: A social cognitive approach. Med. Sci. Sports Exerc. 1994, 26, 1395–1399. [Google Scholar] [CrossRef] [PubMed]
- Mailey, E.L.; Phillips, S.M.; Dlugonski, D.; Conroy, D.E. Overcoming barriers to exercise among parents: A social cognitive theory perspective. J. Behav. Med. 2016, 39, 599–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaughan, C.A.; Ghosh-Dastidar, M.; Dubowitz, T. Attitudes and Barriers to Healthy Diet and Physical Activity: A Latent Profile Analysis. Health Educ. Behav. 2018, 45, 381–393. [Google Scholar] [CrossRef] [PubMed]
- Conn, V.S.; Hafdahl, A.R.; Minor, M.A.; Nielsen, P.J. Physical activity interventions among adults with arthritis: Meta-analysis of outcomes. Semin. Arthritis Rheum. 2008, 37, 307–316. [Google Scholar] [CrossRef] [PubMed]
- de Vries, J.D.; van Hooff, M.L.M.; Geurts, S.A.E.; Kompier, M.A.J. Exercise to reduce work-related fatigue among employees: A randomized controlled trial. Scand. J. Work Environ. Health 2017, 43, 337–349. [Google Scholar] [CrossRef] [PubMed]
- Puetz, T.W.; Flowers, S.S.; O’Connor, P.J. A randomized controlled trial of the effect of aerobic exercise training on feelings of energy and fatigue in sedentary young adults with persistent fatigue. Psychother. Psychosom. 2008, 77, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Chou, C.P.; Huh, J.; Leventhal, A.; Dunton, G. Associations of Affective Responses During Free-Living Physical Activity and Future Physical Activity Levels: An Ecological Momentary Assessment Study. Int. J. Behav. Med. 2017, 24, 513–519. [Google Scholar] [CrossRef]
- Pretty, J.; Hine, P.; Sellens, M.; South, N.; Griffin, M. Green exercise in the UK countryside: Effects on health and psychological well-being, and implications for policy and planning. J. Environ. Plan. Manag. 2007, 50, 211–231. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Mean | Standard Deviation | |
|---|---|---|
| Age | 52.1 | 13.4 |
| N | % | |
| Gender | ||
| Male | 122 | 8.2 |
| Female | 1356 | 90.9 |
| Race | ||
| White | 1416 | 95.0 |
| Non-White | 58 | 3.9 |
| Education | ||
| High school | 214 | 14.4 |
| Some college | 282 | 18.9 |
| 2–4 year college | 608 | 40.8 |
| Master’s or higher | 369 | 24.8 |
| Household income | ||
| <$40,000 | 248 | 16.6 |
| $40,000–$69,999 | 372 | 25.0 |
| $70,000–$89,999 | 243 | 16.3 |
| ≥$90,000 | 396 | 26.6 |
| Physical activity level | ||
| Low active | 440 | 29.5 |
| Moderately active | 520 | 34.9 |
| High active | 531 | 35.6 |
| Total (n = 1491) | Low Active (n = 459) | Moderate Active (n = 509) | High Active (n = 522) | Young (n = 158) | Middle Aged (n = 602) | Older Aged (n = 577) | |
|---|---|---|---|---|---|---|---|
| Barriers (reported yes) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) |
| Poor weather **+ | 986 (66.1) | 336 (73.2) | 338 (66.3) | 312 (59.8) | 116 (73.4) | 405 (67.2) | 418 (63.1) |
| Time *++ | 746 (50.3) | 252 (55.0) | 260 (51.0) | 234 (45.4) | 102 (64.6) | 363 (60.6) | 243 (36.8) |
| Difficulty walking **++ | 123 (8.3) | 64 (14.0) | 38 (7.5) | 21 (4.1) | 13 (8.2) | 32 (5.3) | 74 (11.2) |
| Health ** | 97 (6.5) | 48 (10.5) | 26 (5.1) | 23 (4.5) | 11 (7.0) | 37 (6.2) | 46 (7.0) |
| Motivators (reported yes) | |||||||
| Health *++ | 1260 (84.6) | 383 (83.4) | 418(82.1) | 459 (87.9) | 121 (76.6) | 501 (83.2) | 577 (87.0) |
| Good weather **++ | 1061 (71.2) | 315 (68.6) | 389 (76.4) | 357 (68.4) | 130 (82.3) | 428 (71.1) | 457 (68.9) |
| Weight loss **++ | 1102 (74.0) | 361 (78.7) | 382 (75.1) | 359 (68.8) | 113 (71.5) | 475 (78.9) | 462 (69.7) |
| Weight maintenance ** | 489 (32.8) | 98 (21.4) | 171 (33.6) | 220 (42.2) | 47 (29.8) | 198 (32.9) | 225 (33.9) |
| N | % | Example Quotes | |
|---|---|---|---|
| Barriers (n = 141) | |||
| Lack of motivation | 37 | 26.2 | “I have no ambition to walk” “I’m just plain lazy” “I am really not motivated to walk” |
| Arthritis | 29 | 20.6 | “My knees hurt me” “I have hip pain” “I have arthritis in my ankle” |
| Fatigue | 27 | 17.0 | “I am too tired after work” “I don’t have enough energy, I need to rest” “At the end of the day I am exhausted” |
| Safety | 17 | 12.1 | “I am scared of being alone” “I don’t live in a safe area” “I don’t like to walk by myself when it is dark” “There are no sidewalks or paths easily available” |
| Family or work obligations | 15 | 10.6 | “I have too many family commitments” “I am always being a caretaker” “I need to be on my computer for work” |
| Lack of enjoyment | 10 | 7.1 | “I would rather do other things” “I don’t like to walk” “I have other interests” |
| Lack of a partner | 9 | 6.4 | “I don’t have a walking buddy” “My husband doesn’t want to walk with me” |
| Motivators (n = 282) | |||
| Stress relief and mental health | 82 | 29.1 | “I walk because it helps with my stress” “To de-stress and get out of the office” “Walking helps me gather my thoughts” “…to lighten my mood” |
| Socialization | 70 | 24.8 | “Walking gives me time with my spouse” “I like to walk with my family” “It gives me quality time with my son” “I get to talk with my friends” |
| Dog walks | 41 | 14.5 | “I have a new puppy” “My dogs need to walk” “I like to spend time with my dog” |
| Other health benefits | 38 | 13.5 | “Walking helps improve my sleep” “It helps my joints feel better” “I want to get off blood pressure medicines” |
| Connect with nature | 19 | 6.7 | “I enjoying being in nature and seeing wildlife” “I get relaxation from looking at the trees and the sky” “I feel connected to being outside” |
| Enjoyment | 14 | 5.0 | “I enjoy seeing my neighborhood” “I enjoy walking, it makes me happy” |
| House work or occupation | 11 | 3.9 | “Parking farther at work” “When I have heavy house chores” “Gardening and yard work” |
| Environmental or community supports | 7 | 2.5 | “Good sidewalks” “Access to places to walk to” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Richards, E.A.; Woodcox, S. Barriers and Motivators to Physical Activity Prior to Starting a Community-Based Walking Program. Int. J. Environ. Res. Public Health 2021, 18, 10659. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010659
Richards EA, Woodcox S. Barriers and Motivators to Physical Activity Prior to Starting a Community-Based Walking Program. International Journal of Environmental Research and Public Health. 2021; 18(20):10659. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010659
Chicago/Turabian StyleRichards, Elizabeth A., and Stephanie Woodcox. 2021. "Barriers and Motivators to Physical Activity Prior to Starting a Community-Based Walking Program" International Journal of Environmental Research and Public Health 18, no. 20: 10659. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010659