
Symptoms of Autism, Comorbid Mental Health Conditions and Challenging Behaviors among Toddlers with Down Syndrome at Low Risk for ASD—Characterization Using the BISCUIT—Parts 1–3


Abstract
:1. Introduction
Current Study
2. Materials and Methods
2.1. Design
2.2. Participants and Procedure
2.3. Instruments
2.4. Analyses
3. Results
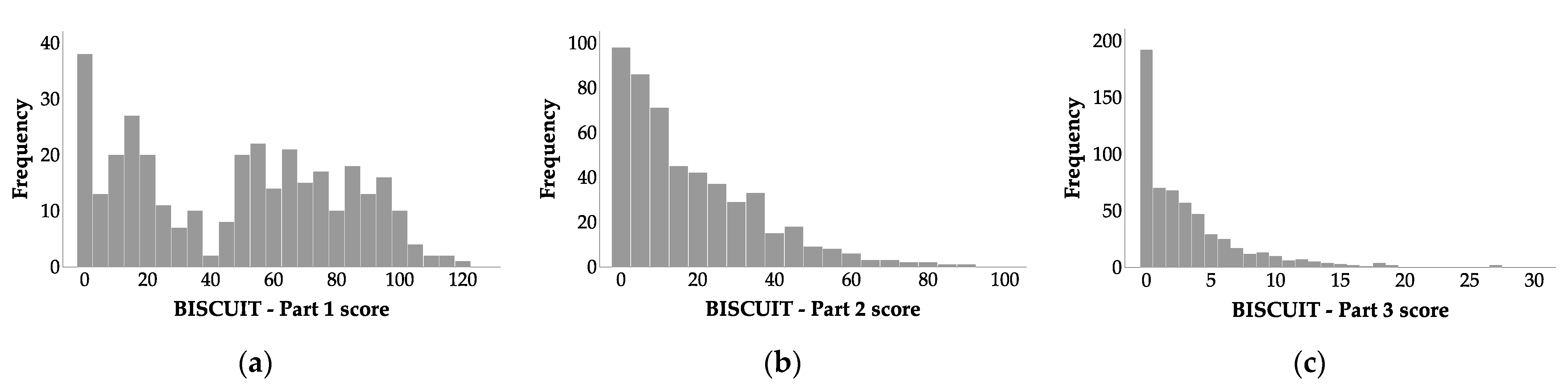
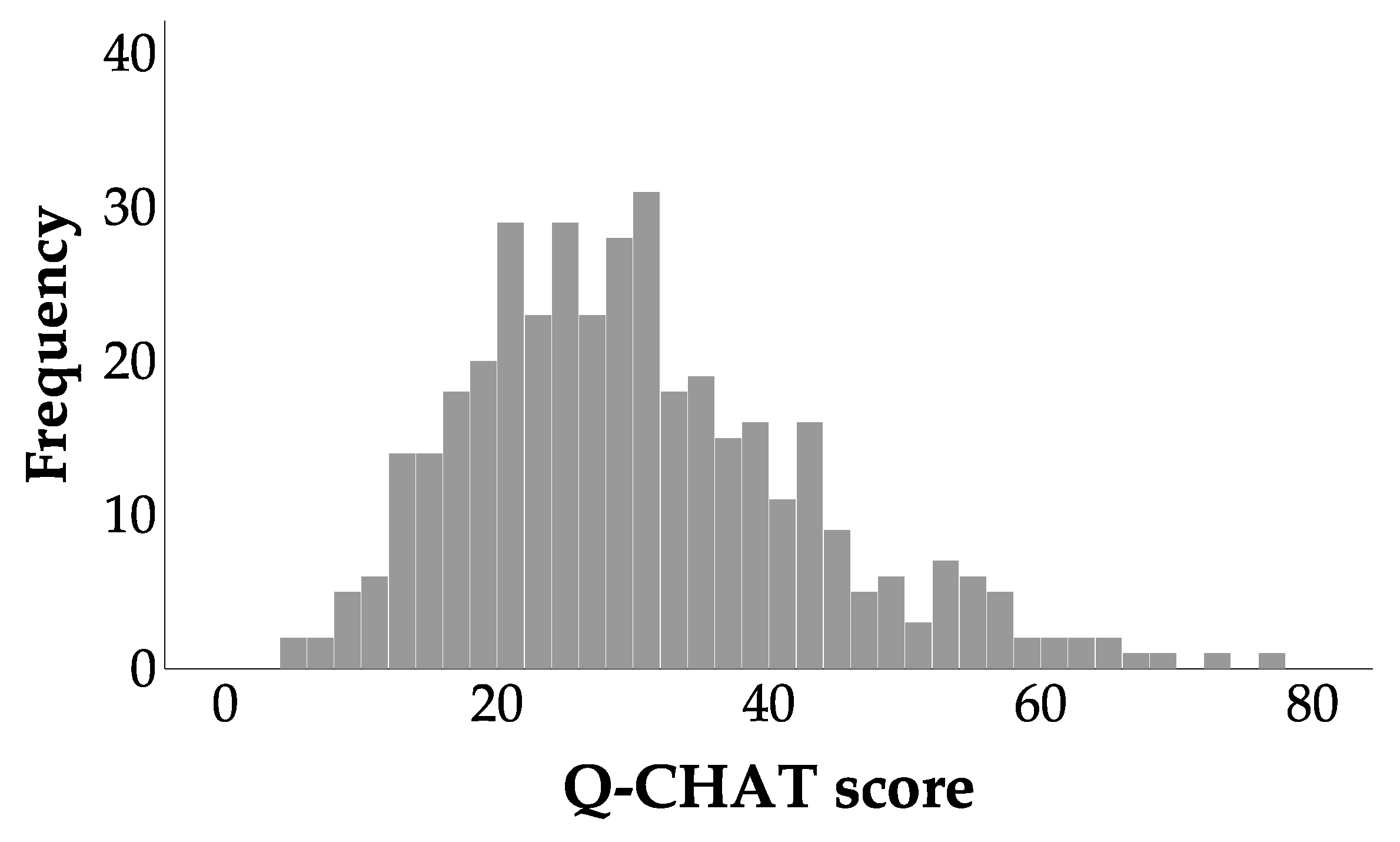
3.1. Distributions of BISCUIT and Q-CHAT Scores
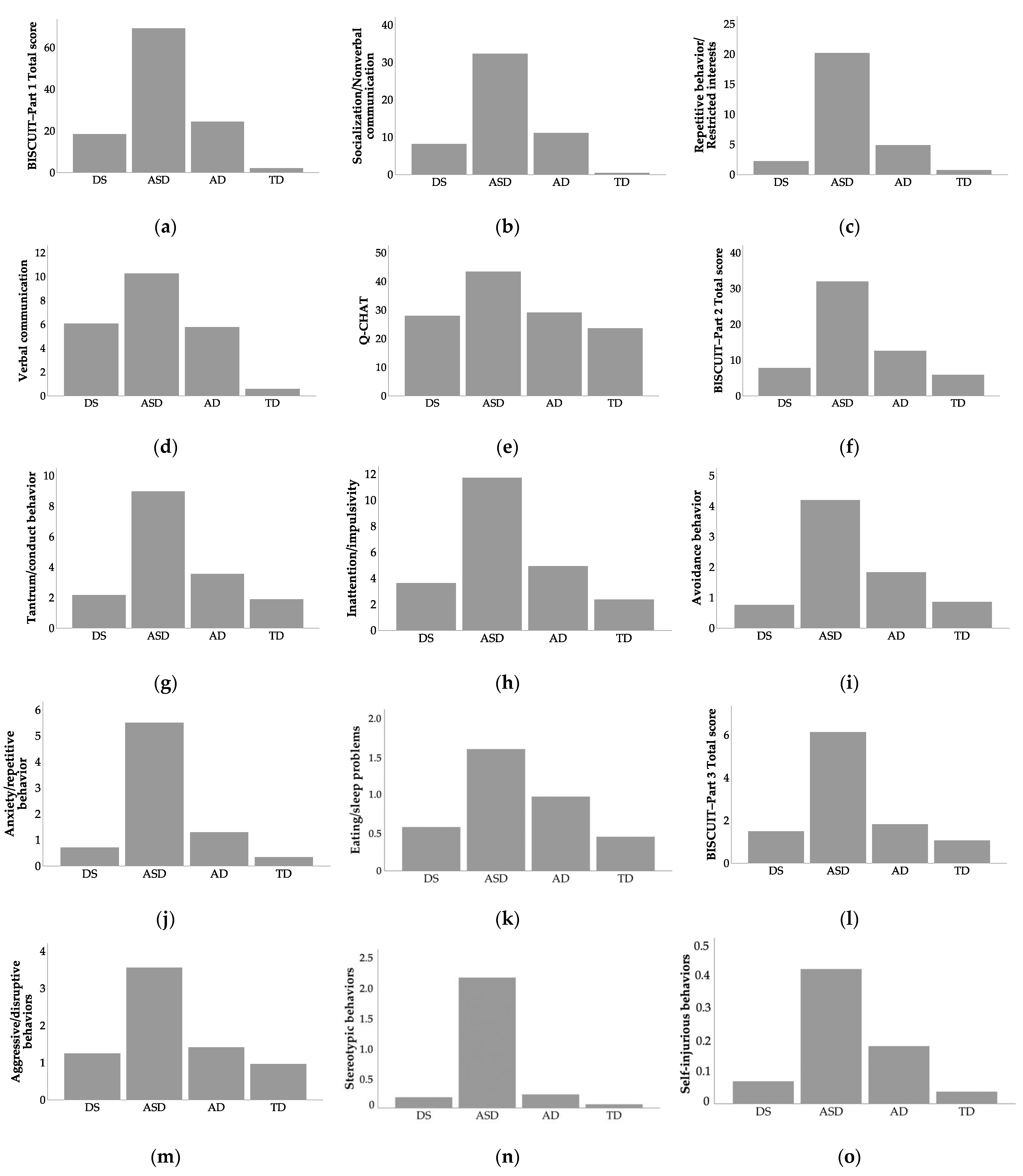
3.2. Group Comparisons
3.3. Symptoms of Autism Spectrum Disorders
3.3.1. BISCUIT–Part 1
3.3.2. Q-CHAT
3.4. Symptoms of Comorbid Mental Health Conditions
3.4.1. BISCUIT—Part 2 Total Score
3.4.2. Tantrum/Conduct Behavior
3.4.3. Inattention/Impulsivity
3.4.4. Avoidance Behavior
3.4.5. Anxiety/Repetitive Behavior
3.4.6. Eating/Sleep Problems
3.5. Symptoms of Challenging Behaviors
3.5.1. BISCUIT–Part 3 Total Score
3.5.2. Aggressive/Disruptive Behaviors
3.5.3. Stereotypic Behaviors
3.5.4. Self-Injurious Behaviors
3.6. Correlations between Participants’ Age, BISCUIT–Parts 1–3 and Q-CHAT Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| DS | ASD | AD | TD | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | Min–Max | M | SD | Min–Max | M | SD | Min–Max | M | SD | Min–Max | |
| BISCUIT–Part 1 Total score | 18.556 | 11.126 | 5–67 | 69.330 | 21.782 | 10–118 | 24.568 | 20.568 | 1–81 | 2.149 | 3.695 | 0–15 |
| Socialization/Nonverbal communication | 8.222 | 6.324 | 2–36 | 32.361 | 10.371 | 1–48 | 11.184 | 11.862 | 0–42 | 0.5 | 1.353 | 0–6 |
| Repetitive behavior/Restricted interests | 2.259 | 2.586 | 0–13 | 20.221 | 8.229 | 4–46 | 4.895 | 5.913 | 0–23 | 0.792 | 1.54 | 0–6 |
| Verbal communication | 6.074 | 2.386 | 1–13 | 10.274 | 3.299 | 0–14 | 5.79 | 3.772 | 0–12 | 0.6 | 1.364 | 0–6 |
| Q-CHAT | 28.024 | 7.413 | 13–42 | 43.500 | 12.685 | 17–80 | 29.262 | 11.032 | 5–62 | 23.641 | 8.940 | 5–60 |
| BISCUIT–Part 2 Total score | 8.556 | 7.350 | 0–37 | 32.748 | 17.294 | 3–104 | 13.434 | 13.686 | 0–70 | 6.444 | 8.019 | 0–43 |
| Tantrum/conduct behavior | 2.315 | 2.394 | 0–9 | 9.287 | 5.739 | 0–34 | 4.434 | 5.300 | 0–30 | 2.640 | 3.563 | 0–19 |
| Inattention/impulsivity | 3.574 | 3.178 | 0–12 | 11.762 | 6.412 | 0–30 | 4.816 | 5.447 | 0–27 | 2.028 | 3.287 | 0–19 |
| Avoidance behavior | 0.778 | 1.327 | 0–6 | 4.178 | 4.139 | 0–18 | 1.724 | 2.580 | 0–12 | 0.893 | 1.662 | 0–9 |
| Anxiety/repetitive behavior | 0.648 | 1.231 | 0–7 | 5.342 | 3.950 | 0–21 | 1.263 | 2.435 | 0–16 | 0.315 | 0.657 | 0–4 |
| Eating/sleep problems | 0.593 | 1.281 | 0–6 | 1.574 | 1.939 | 0–8 | 0.842 | 1.600 | 0–7 | 0.433 | 0.938 | 0–5 |
| BISCUIT–Part 3 Total score | 1.500 | 1.537 | 0–7 | 6.137 | 4.688 | 0–27 | 1.828 | 2.657 | 0–12 | 1.072 | 1.847 | 0–10 |
| Aggressive/disruptive behaviors | 1.250 | 1.225 | 0–5 | 3.562 | 3.452 | 0–19 | 1.419 | 2.108 | 0–11 | 0.971 | 1.725 | 0–9 |
| Stereotypic behaviors | 0.179 | 0.431 | 0–2 | 2.151 | 1.600 | 0–6 | 0.226 | .662 | 0–4 | 0.063 | 0.280 | 0–2 |
| Self-injurious behaviors | 0.071 | 0.260 | 0–1 | 0.425 | 0.722 | 0–3 | 0.183 | 0.625 | 0–4 | 0.039 | 0.193 | 0–1 |
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- World Health Organization. International Classification of Diseases, 11th ed.; World Health Organization: Geneva, Switzerland, 2018. Available online: https://icd.who.int (accessed on 1 August 2021).
- Lai, M.-C.; Lombardo, M.V.; Baron-Cohen, S. Autism. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef]
- Hazen, E.P.; Stornelli, J.L.; O’Rourke, J.A.; Koesterer, K.; McDougle, C.J. Sensory Symptoms in Autism Spectrum Disorders. Harv. Rev. Psychiatry 2014, 22, 112–124. [Google Scholar] [CrossRef] [Green Version]
- Catalá-López, F.; Ridao, M.; Hurtado, I.; Núñez-Beltrán, A.; Gènova-Maleras, R.; Alonso-Arroyo, A.; Tobías, A.; Aleixandre-Benavent, R.; Catalá, M.A.; Tabarés-Seisdedos, R. Prevalence and comorbidity of autism spectrum disorder in Spain: Study protocol for a systematic review and meta-analysis of observational studies. Syst. Rev. 2019, 8, 141. [Google Scholar] [CrossRef] [Green Version]
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G.; et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR. Surveill. Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef]
- Tordjman, S.; Cohen, D.; Coulon, N.; Anderson, G.M.; Botbol, M.; Canitano, R.; Roubertoux, P.L. Reframing autism as a behavioral syndrome and not a specific mental disorder: Implications of genetic and phenotypic heterogeneity. Neurosci. Biobehav. Rev. 2017, 80, 210. [Google Scholar] [CrossRef]
- Richards, C.; Jones, C.; Groves, L.; Moss, J.; Oliver, C. Prevalence of autism spectrum disorder phenomenology in genetic disorders: A systematic review and meta-analysis. Lancet Psychiatry 2015, 2, 909–916. [Google Scholar] [CrossRef] [Green Version]
- Mégarbané, A.; Ravel, A.; Mircher, C.; Sturtz, F.; Grattau, Y.; Rethoré, M.-O.; Delabar, J.-M.; Mobley, W.C. The 50th anniversary of the discovery of trisomy 21: The past, present, and future of research and treatment of Down syndrome. Genet. Med. 2009, 11, 611–616. [Google Scholar] [CrossRef] [Green Version]
- Bull, M.J. Down Syndrome. N. Engl. J. Med. 2020, 382, 2344–2352. [Google Scholar] [CrossRef]
- Chapman, R.S.; Hesketh, L.J. Behavioral phenotype of individuals with Down syndrome. Ment. Retard. Dev. Disabil. Res. Rev. 2000, 6, 84–95. [Google Scholar] [CrossRef]
- Silverman, W. Down syndrome: Cognitive phenotype. Ment. Retard. Dev. Disabil. Res. Rev. 2007, 13, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Karmiloff-Smith, A.; al-Janabi, T.; D’Souza, H.; Groet, J.; Massand, E.; Mok, K.; Startin, C.; Fisher, E.; Hardy, J.; Nizetic, D.; et al. The importance of understanding individual differences in Down syndrome. F1000Research 2016, 5, 389. [Google Scholar] [CrossRef] [PubMed]
- DiGuiseppi, C.; Hepburn, S.; Davis, J.M.; Fidler, D.J.; Hartway, S.; Lee, N.; Miller, L.; Ruttenber, M.; Robinson, C. Screening for Autism Spectrum Disorders in Children with Down Syndrome. J. Dev. Behav. Pediatr. 2010, 31, 181–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kent, L.; Evans, J.; Paul, M.; Sharp, M. Comorbidity of autistic spectrum disorders in children with Down syndrome. Dev. Med. Child Neurol. 2007, 41, 153–158. [Google Scholar] [CrossRef]
- Oxelgren, U.W.; Myrelid, Å.; Annerén, G.; Ekstam, B.; Göransson, C.; Holmbom, A.; Isaksson, A.; Åberg, M.; Gustafsson, J.; Fernell, E. Prevalence of autism and attention-deficit-hyperactivity disorder in Down syndrome: A population-based study. Dev. Med. Child Neurol. 2016, 59, 276–283. [Google Scholar] [CrossRef]
- Warner, G.; Moss, J.; Smith, P.; Howlin, P. Autism Characteristics and Behavioural Disturbances in ∼ 500 Children with Down’s Syndrome in England and Wales. Autism Res. 2014, 7, 433–441. [Google Scholar] [CrossRef]
- Howlin, P.; Wing, L.; Gould, J. The recognition of autism in children with down syndrome-implications for intervention and some speculations about pathology. Dev. Med. Child Neurol. 2008, 37, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Mammad, K.; Chkirat, M.; Kriouile, Y.; Alaoui, A.M. Children with Down Syndrome (DS), and Autism Spectrum Disorder (ASD): Difficulties of Screening and Management of This Dual Diagnosis about 3 Cases. Psychology 2019, 10, 931–939. [Google Scholar] [CrossRef] [Green Version]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule, 2nd ed.; Western Psychological Corporation: Los Angeles, CA, USA, 2012. [Google Scholar]
- Oxelgren, U.W.; Åberg, M.; Myrelid, Å.; Annerén, G.; Westerlund, J.; Gustafsson, J.; Fernell, E. Autism needs to be considered in children with Down Syndrome. Acta Paediatr. 2019, 108, 2019–2026. [Google Scholar] [CrossRef]
- Godfrey, M.; Hepburn, S.; Fidler, D.J.; Tapera, T.; Zhang, F.; Rosenberg, C.R.; Lee, N.R. Autism spectrum disorder (ASD) symptom profiles of children with comorbid Down syndrome (DS) and ASD: A comparison with children with DS-only and ASD-only. Res. Dev. Disabil. 2019, 89, 83–93. [Google Scholar] [CrossRef]
- Hamner, T.; Hepburn, S.; Zhang, F.; Fidler, D.; Rosenberg, R.; Robins, D.L.; Lee, N.R. Cognitive Profiles and Autism Symptoms in Comorbid Down Syndrome and Autism Spectrum Disorder. J. Dev. Behav. Pediatr. 2020, 41, 172–179. [Google Scholar] [CrossRef]
- Magyar, C.I.; Pandolfi, V.; Dill, C.A. An Initial Evaluation of the Social Communication Questionnaire for the Assessment of Autism Spectrum Disorders in Children with Down Syndrome. J. Dev. Behav. Pediatr. 2012, 33, 134–145. [Google Scholar] [CrossRef]
- Molloy, C.A.; Murray, D.S.; Kinsman, A.; Castillo, H.; Mitchell, T.; Hickey, F.J.; Patterson, B. Differences in the clinical presentation of Trisomy 21 with and without autism. J. Intellect. Disabil. Res. 2009, 53, 143–151. [Google Scholar] [CrossRef]
- Warner, G.; Howlin, P.; Salomone, E.; Moss, J.; Charman, T. Profiles of children with Down syndrome who meet screening criteria for autism spectrum disorder (ASD): A comparison with children diagnosed with ASD attending specialist schools. J. Intellect. Disabil. Res. 2016, 61, 75–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Channell, M.M.; Phillips, B.A.; Loveall, S.J.; Conners, F.A.; Bussanich, P.M.; Klinger, L.G. Patterns of autism spectrum symptomatology in individuals with Down syndrome without comorbid autism spectrum disorder. J. Neurodev. Disord. 2015, 7, 5. [Google Scholar] [CrossRef] [Green Version]
- Constantino, J.; Gruber, C. Social Responsiveness Scale; Western Psychological Services: Los Angeles, CA, USA, 2005. [Google Scholar]
- Channell, M.M. The Social Responsiveness Scale (SRS-2) in school-age children with Down syndrome at low risk for autism spectrum disorder. Autism Dev. Lang. Impair. 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Constantino, J.N.; Gruber, C.P. Social Responsiveness Scale, 2nd ed.; Western Psychological Services: Los Angeles, CA, USA, 2012. [Google Scholar]
- Hepburn, S.; Philofsky, A.; Fidler, D.J.; Rogers, S. Autism symptoms in toddlers with Down syndrome: A descriptive study. J. Appl. Res. Intellect. Disabil. 2007, 21, 48–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H., Jr.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The Autism Diagnostic Observation Schedule—Generic: A Standard Measure of Social and Communication Deficits Associated with the Spectrum of Autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef]
- Matson, J.L.; Wilkins, J.; Sevin, J.A.; Knight, C.; Boisjoli, J.A.; Sharp, B. Reliability and item content of the Baby and Infant Screen for Children with aUtIsm Traits (BISCUIT): Parts 1–3. Res. Autism Spectr. Disord. 2009, 3, 336–344. [Google Scholar] [CrossRef]
- Dykens, E.M. Psychiatric and behavioral disorders in persons with Down syndrome. Ment. Retard. Dev. Disabil. Res. Rev. 2007, 13, 272–278. [Google Scholar] [CrossRef]
- Bhatia, M.S.; Kabra, M.; Sapra, S. Behavioral problems in children with Down syndrome. Indian Pediatr. 2005, 42, 675–680. [Google Scholar] [PubMed]
- Startin, C.M.; D’Souza, H.; Ball, G.; Hamburg, S.; Hithersay, R.; Hughes, K.M.O.; Massand, E.; Karmiloff-Smith, A.; Thomas, M.S.C.; Consortium, L.; et al. Health comorbidities and cognitive abilities across the lifespan in Down syndrome. J. Neurodev. Disord. 2020, 12, 4. [Google Scholar] [CrossRef]
- Achenbach, T.M. Manual for the Child Behavior Checklist/4-18 and 1991 Profile; Department of Psychiatry, University of Vermont: Burlington, VT, USA, 1991. [Google Scholar]
- Dieleman, L.M.; De Pauw, S.S.; Soenens, B.; Van Hove, G.; Prinzie, P. Behavioral Problems and Psychosocial Strengths: Unique Factors Contributing to the Behavioral Profile of Youth with Down Syndrome. Am. J. Intellect. Dev. Disabil. 2018, 123, 212–227. [Google Scholar] [CrossRef] [PubMed]
- Chebli, S.S.; Martin, V.; Lanovaz, M.J. Prevalence of Stereotypy in Individuals with Developmental Disabilities: A Systematic Review. Rev. J. Autism Dev. Disord. 2016, 3, 107–118. [Google Scholar] [CrossRef]
- Capone, G.T.; Grados, M.A.; Kaufmann, W.E.; Bernad-Ripoll, S.; Jewell, A. Down syndrome and comorbid autism-spectrum disorder: Characterization using the aberrant behavior checklist. Am. J. Med Genet. Part A 2005, 134A, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.C.; Capone, G.T.; Gray, R.M.; Cox, C.S.; Kaufmann, W.E. Autistic-spectrum disorders in down syndrome: Further delineation and distinction from other behavioral abnormalities. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2007, 144B, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Allison, C.; Baron-Cohen, S.; Wheelwright, S.; Charman, T.; Richler, J.; Pasco, G.; Brayne, C. The Q-CHAT (Quantitative CHecklist for Autism in Toddlers): A Normally Distributed Quantitative Measure of Autistic Traits at 18–24 Months of Age: Preliminary Report. J. Autism Dev. Disord. 2008, 38, 1414–1425. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Diseases: Diagnostic Criteria for Research, 10th ed.; World Health Organization: Geneva, Switzerland, 1992.
- Matson, J.L.; Wilkins, J.; Sharp, B.; Knight, C.; Sevin, J.A.; Boisjoli, J.A. Sensitivity and specificity of the Baby and Infant Screen for Children with aUtIsm Traits (BISCUIT): Validity and cutoff scores for autism and PDD-NOS in toddlers. Res. Autism Spectr. Disord. 2009, 3, 924–930. [Google Scholar] [CrossRef]
- Matson, J.L.; Wilkins, J.; Fodstad, J.C. The Validity of the Baby and Infant Screen for Children with aUtIsm Traits: Part 1 (BISCUIT: Part 1). J. Autism Dev. Disord. 2011, 41, 1139–1146. [Google Scholar] [CrossRef]
- Matson, J.L.; Boisjoli, J.A.; Hess, J.A.; Wilkins, J. Factor structure and diagnostic fidelity of the Baby and Infant Screen for Children with aUtIsm Traits–Part 1 (BISCUIT–part 1). Dev. Neurorehabilit. 2010, 13, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Matson, J.L.; Fodstad, J.C.; Mahan, S. Cutoffs, norms, and patterns of comorbid difficulties in children with developmental disabilities on the Baby and Infant Screen for Children with aUtIsm Traits (BISCUIT-Part 2). Res. Dev. Disabil. 2009, 30, 1221–1228. [Google Scholar] [CrossRef]
- Rojahn, J.; Matson, J.L.; Mahan, S.; Fodstad, J.C.; Knight, C.; Sevin, J.A.; Sharp, B. Cutoffs, norms, and patterns of problem behaviors in children with an ASD on the Baby and Infant Screen for Children with aUtIsm Traits (BISCUIT-Part 3). Res. Autism Spectr. Disord. 2009, 3, 989–998. [Google Scholar] [CrossRef]
- Brislin, R.W. Back-Translation for Cross-Cultural Research. J. Cross-Cult. Psychol. 1970, 1, 185–216. [Google Scholar] [CrossRef]
- Matson, J.L.; Boisjoli, J.; Wilkins, J. The Baby and Infant Screen for Children with aUtIsm Traits (BISCUIT); Disability Consultants LLC: Baton Rouge, LA, USA, 2007. [Google Scholar]
- Glenn, J. Repetitive Behaviours and Restricted Interests in Individuals with Down Syndrome—One Way of Managing Their World? Brain Sci. 2017, 7, 66. [Google Scholar] [CrossRef] [Green Version]
- Evans, D.W.; Gray, F.L. Compulsive-like behavior in individuals with Down syndrome: Its relation to mental age level, adaptive and maladaptive behavior. Child Dev. 2000, 71, 288–300. [Google Scholar] [CrossRef]
- Fidler, D.J.; Hepburn, S.; Rogers, S. Early learning and adaptive behaviour in toddlers with Down syndrome: Evidence for an emerging behavioural phenotype? Down Syndr. Res. Pract. 2006, 9, 37–44. [Google Scholar] [CrossRef] [Green Version]
- Robins, D.L.; Fein, D.; Barton, M.L.; Green, J.A. The Modified Checklist for Autism in Toddlers: An Initial Study Investigating the Early Detection of Autism and Pervasive Developmental Disorders. J. Autism Dev. Disord. 2001, 31, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Davis, T.E., III; Fodstad, J.C.; Jenkins, W.S.; Hess, J.A.; Moree, B.N.; Dempsey, T.; Matson, J.L. Anxiety and avoidance in infants and toddlers with autism spectrum disorders: Evidence for differing symptom severity and presentation. Res. Autism Spectr. Disord. 2010, 4, 305–313. [Google Scholar] [CrossRef]
- Belardinelli, C.; Raza, M.; Taneli, T. Comorbid Behavioral Problems and Psychiatric Disorders in Autism Spectrum Disorders. J. Child. Dev. Disord. 2016, 2. [Google Scholar] [CrossRef]
- Casanova, M.F.; Frye, R.E.; Gillberg, C.; Casanova, E.L. Editorial: Comorbidity and Autism Spectrum Disorder. Front. Psychiatry 2020, 11, 617395. [Google Scholar] [CrossRef] [PubMed]
- Esbensen, A.J.; Hoffman, E.K.; Shaffer, R.; Chen, E.; Patel, L.; Jacola, L. Reliability of parent report measures of behaviour in children with Down syndrome. J. Intellect. Disabil. Res. 2018, 62, 785–797. [Google Scholar] [CrossRef]
- Matson, J.L.; Boisjoli, J.; Rojahn, J.; Hess, J. A factor analysis of challenging behaviors assessed with the Baby and Infant Screen for Children with aUtism Traits (BISCUIT-Part 3). Res. Autism Spectr. Disord. 2009, 3, 714–722. [Google Scholar] [CrossRef]
- Matson, J.L.; Matheis, M.; Burns, C.O.; Esposito, G.; Venuti, P.; Pisula, E.; Misiak, A.; Kalyva, E.; Tsakiris, V.; Kamio, Y.; et al. Examining cross-cultural differences in autism spectrum disorder: A multinational comparison from Greece, Italy, Japan, Poland, and the United States. Eur. Psychiatry 2017, 42, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.W.; Canavera, K.; Kleinpeter, F.L.; Maccubbin, E.; Taga, K. The Fears, Phobias and Anxieties of Children with Autism Spectrum Disorders and Down Syndrome: Comparisons with Developmentally and Chronologically Age Matched Children. Child Psychiatry Hum. Dev. 2005, 36, 3–26. [Google Scholar] [CrossRef]
- Fodstad, J.C.; Rojahn, J.; Matson, J.L. Emergent Comorbidity in At Risk Children with and without Autism Spectrum Disorder—A Cross-Sectional Study. J. Dev. Phys. Disabil. 2010, 22, 381–400. [Google Scholar] [CrossRef]
- Matson, J.L.; Hess, J.A.; Boisjoli, J.A. Comorbid psychopathology in infants and toddlers with autism and pervasive developmental disorders-not otherwise specified (PDD-NOS). Res. Autism Spectr. Disord. 2010, 4, 300–304. [Google Scholar] [CrossRef]
- Chandler, S.; Howlin, P.; Simonoff, E.; O’Sullivan, T.; Tseng, E.; Kennedy, J.; Charman, T.; Baird, G. Emotional and behavioural problems in young children with autism spectrum disorder. Dev. Med. Child Neurol. 2015, 58, 202–208. [Google Scholar] [CrossRef] [Green Version]
- Hartley, S.L.; Sikora, D.M.; McCoy, R. Prevalence and risk factors of maladaptive behaviour in young children with Autistic Disorder. J. Intellect. Disabil. Res. 2008, 52, 819–829. [Google Scholar] [CrossRef] [Green Version]
- Hill, A.P.; Zuckerman, K.E.; Hagen, A.D.; Kriz, D.J.; Duvall, S.W.; van Santen, J.; Nigg, J.; Fair, D.; Fombonne, E. Aggressive behavior problems in children with autism spectrum disorders: Prevalence and correlates in a large clinical sample. Res. Autism Spectr. Disord. 2014, 8, 1121–1133. [Google Scholar] [CrossRef] [Green Version]
- Feeley, K.; Jones, E. Strategies to address challenging behaviour in young children with Down syndrome. Down Syndr. Res. Pract. 2008, 12, 153–163. [Google Scholar] [CrossRef] [Green Version]
- Montagna, A.; Nosarti, C. Socio-Emotional Development Following Very Preterm Birth: Pathways to Psychopathology. Front. Psychol. 2016, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodas, N.V.; Eisenhower, A.; Blacher, J. Structural and Pragmatic Language in Children with ASD: Longitudinal Impact on Anxiety and Externalizing Behaviors. J. Autism Dev. Disord. 2017, 47, 3479–3488. [Google Scholar] [CrossRef] [PubMed]



| DS | ASD | AD | TD | |
|---|---|---|---|---|
| N (males) | 56 (33) | 220 (168) | 93 (57) | 209 (108) |
| M age in months (SD), range | 27.11 (5.792), 17–37 | 27.45 (5.690), 17–37 | 25.88 (4.982), 17–37 | 25.474 (5.713), 17–36 |
| M birthweight [g] (SD), range | 2946 (523) 1350–4230 | 3244 (637), 999–4600 | 2961 (867), 700–4450 | 3449 (511), 2090–4820 |
| N preterm | 0 | 25 | 9 | 0 |
| N ASD familial risk | 2 | 61 | 9 | 15 |
| M mother’s age [years] (SD) | 35 (0.5) | 31 (0.5) | Data missing | Data missing |
| M father’s age [years] (SD) | 36 (0.5) | 32 (0.6) | Data missing | Data missing |
| Only child | 29% | 45% | 39% | 45% |
| Additional information | - | Hearing problems n = 5; vision problems: n = 2 | Cerebral palsy n = 1; seizure disorder n = 1, vision problems n = 1 | - |
| Age | BISCUIT—Part 1 | BISCUIT—Part 2 | BISCUIT—Part 3 | ||
|---|---|---|---|---|---|
| BISCUIT–Part 1 | r | 0.012 | |||
| p | 0.831 | ||||
| n | 341 | ||||
| BISCUIT–Part 2 | r | 0.147 ** | 0.800 ** | ||
| p | 0.001 | <0.001 | |||
| n | 578 | 341 | |||
| BISCUIT–Part 3 | r | 0.156 ** | 0.614 ** | 0.801 ** | |
| p | <0.001 | <0.001 | <0.001 | ||
| n | 576 | 340 | 576 | ||
| Q-CHAT | r | −0.123 * | 0.788 ** | 0.687 * | 0.577 * |
| p | 0.015 | <0.001 | <0.001 | <0.001 | |
| n | 393 | 160 | 336 | 392 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pisula, E.; Niedźwiecka, A. Symptoms of Autism, Comorbid Mental Health Conditions and Challenging Behaviors among Toddlers with Down Syndrome at Low Risk for ASD—Characterization Using the BISCUIT—Parts 1–3. Int. J. Environ. Res. Public Health 2021, 18, 10684. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010684
Pisula E, Niedźwiecka A. Symptoms of Autism, Comorbid Mental Health Conditions and Challenging Behaviors among Toddlers with Down Syndrome at Low Risk for ASD—Characterization Using the BISCUIT—Parts 1–3. International Journal of Environmental Research and Public Health. 2021; 18(20):10684. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010684
Chicago/Turabian StylePisula, Ewa, and Alicja Niedźwiecka. 2021. "Symptoms of Autism, Comorbid Mental Health Conditions and Challenging Behaviors among Toddlers with Down Syndrome at Low Risk for ASD—Characterization Using the BISCUIT—Parts 1–3" International Journal of Environmental Research and Public Health 18, no. 20: 10684. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010684