
Association between Relative Handgrip Strength and Chronic Lower Back Pain: A Nationwide Cross-Sectional Analysis of the Korea National Health and Nutrition Examination Survey




Abstract
:1. Introduction
2. Materials and Methods
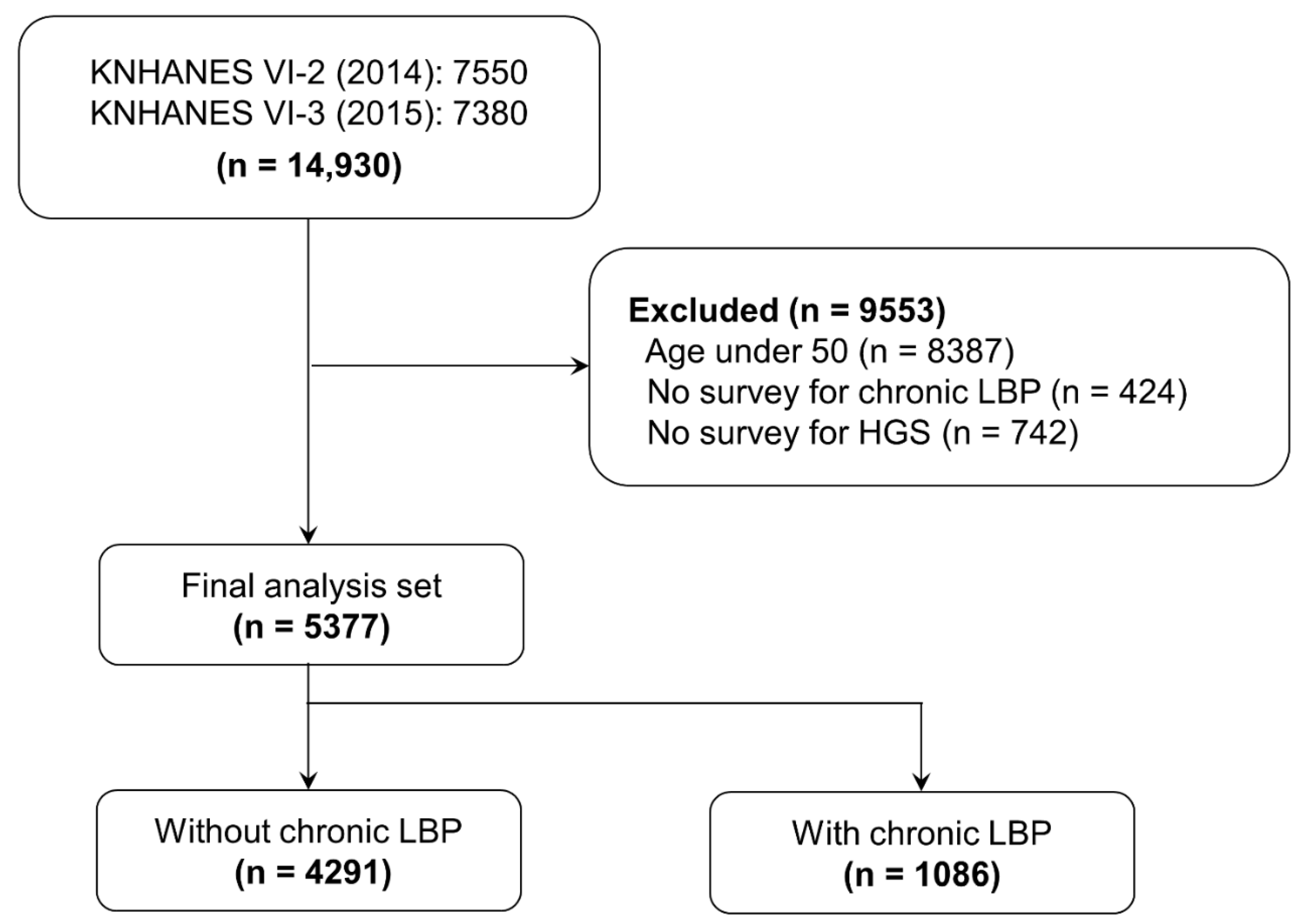
2.1. Study Design
2.2. Data Collection
2.3. Definition of Chronic Lower Back Pain
2.4. Measurement of Handgrip Strength
2.5. Demographic, Health-Related, and Social Variables
2.6. Statistical Analysis
3. Results
3.1. General Characteristics of Participants with Lower Back Pain
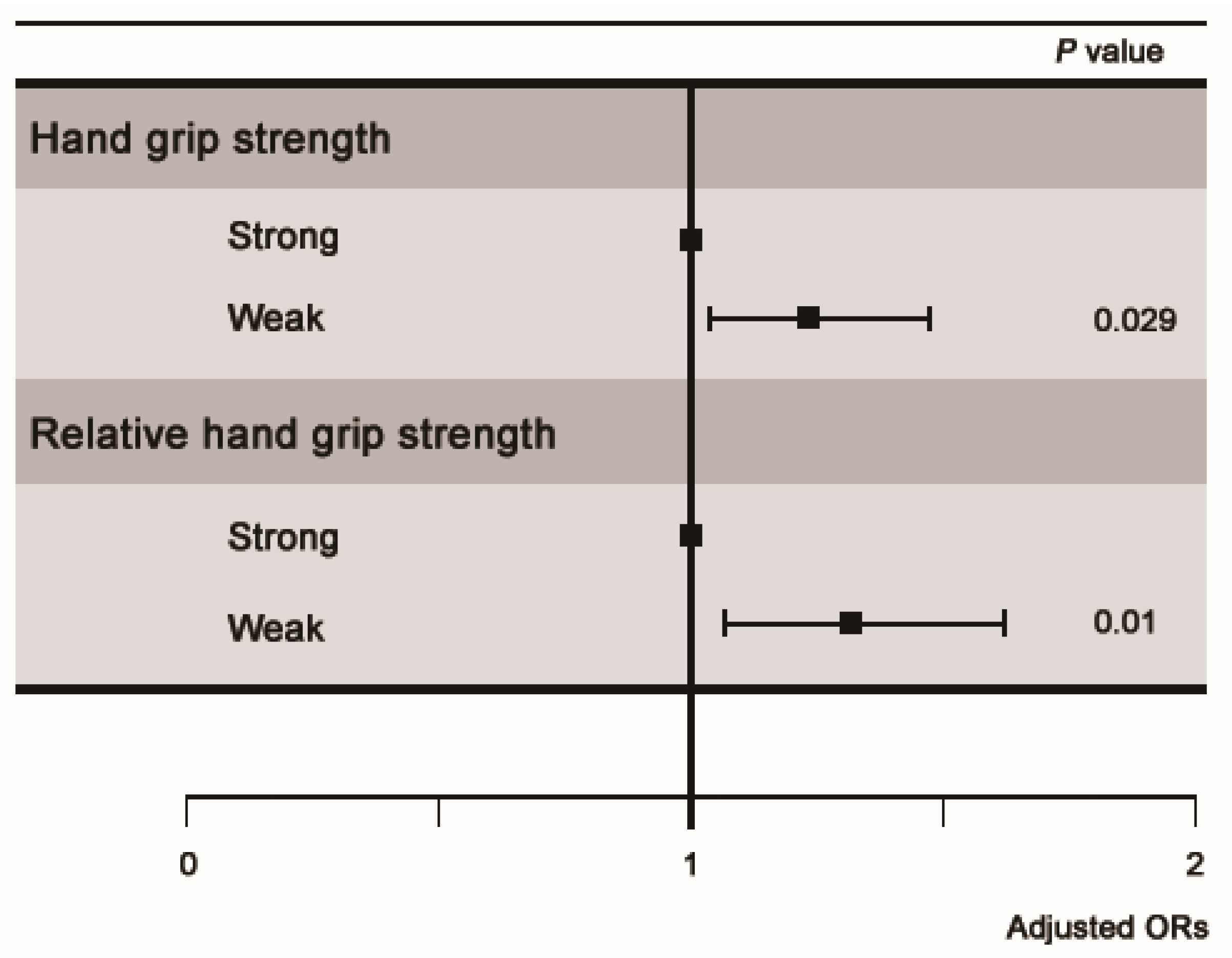
3.2. Association between Chronic Lower Back Pain and Handgrip Strength
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoy, D.; Brooks, P.; Blyth, F.; Buchbinder, R. The epidemiology of low back pain. Best Pract Res. Clin. Rheumatol. 2010, 24, 769–781. [Google Scholar] [CrossRef] [PubMed]
- Dreinhöfer, K.E.; Kirschner, P. Bone and Joint Decade 2000–2010. Dtsch Ärztebl Int. 2000, 97, A3478–A3481. [Google Scholar]
- Manchikanti, L.; Singh, V.; Falco, F.J.; Benyamin, R.M.; Hirsch, J.A. Epidemiology of low back pain in adults. Neuromodulation 2014, 17, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.H.; Beom, J.W.; Lee, T.S.; Lim, J.H.; Lee, T.H.; Yuk, J.H. Trunk muscles strength as a risk factor for nonspecific low back pain: A pilot study. Ann. Rehabil. Med. 2014, 38, 234. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Hoshino, Y.; Nakamura, K.; Kariya, Y.; Saita, K.; Ito, K. Trunk muscle weakness as a risk factor for low back pain: A 5-year prospective study. Spine 1999, 24, 54–57. [Google Scholar] [CrossRef]
- Tosato, M.; Marzetti, E.; Cesari, M.; Savera, G.; Miller, R.R.; Bernabei, R.; Landi, F.; Calvani, R. Measurement of muscle mass in sarcopenia: From imaging to biochemical markers. Aging Clin. Exp. Res. 2017, 29, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.R.; Jeon, Y.J.; Kim, M.C.; Jeong, T.; Koo, W.R. Reference values for hand grip strength in the South Korean population. PLoS ONE 2018, 13, e0195485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.; Rolland, Y.; Schneider, S.M. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W. Muscle strength: Clinical and prognostic value of hand-grip dynamometry. Curr. Opin. Nutr. Metab. Care 2015, 18, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Hand-grip dynamometry predicts future outcomes in aging adults. J. Geriatr. Phys. Ther. 2008, 31, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Moraes, G.M.; Marson, R.A.; de Sá Rego, F.M.; Borba, N.E.; Rodrigues, N.G.; da Silva, N.J. The relationship between handgrip strength and total muscle strength in the Brazilian army military personnel. Med. Sport 2018, 71, 461–473. [Google Scholar]
- Park, S.M.; Kim, G.U.; Kim, H.J.; Kim, H.; Chang, B.; Lee, C.; Yeom, J.S. Low handgrip strength is closely associated with chronic low back pain among women aged 50 years or older: A cross-sectional study using a national health survey. PLoS ONE 2018, 13, e0207759. [Google Scholar] [CrossRef]
- Zhang, S.; Chen, H.; Xu, H.; Yi, Y.; Wang, S.; Wu, D. Association between handgrip strength and subsequent vertebral-fracture risk following percutaneous vertebral augmentation. J. Bone Miner. Metab. 2021, 39, 186–192. [Google Scholar] [CrossRef]
- Kwon, O.; Kim, H.; Shen, F.; Park, S.; Chang, B.; Lee, C.; Yeom, J.S. Influence of Hand Grip Strength on Surgical Outcomes After Surgery for Adult Spinal Deformity. Spine 2020, 45, E1493–E1499. [Google Scholar] [CrossRef]
- Chen, L.; Lee, W.; Peng, L.; Liu, L.; Arai, H.; Akishita, M. Recent advances in sarcopenia research in Asia: 2016 update from the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2016, 17, 767.e1–767.e7. [Google Scholar] [CrossRef]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; Mclean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M. The FNIH sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol. Ser. A Biomed. Sci. Med Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef]
- Choquette, S.; Bouchard, D.R.; Doyon, C.Y.; Sénéchal, M.; Brochu, M.; Dionne, I.J. Relative strength as a determinant of mobility in elders 67-84 years of age. a nuage study: Nutrition as a determinant of successful aging. J. Nutr. Health Aging 2010, 14, 190–195. [Google Scholar] [CrossRef]
- Lawman, H.G.; Troiano, R.P.; Perna, F.M.; Wang, C.; Fryar, C.D.; Ogden, C.L. Associations of relative handgrip strength and cardiovascular disease biomarkers in US adults, 2011–2012. Am. J. Prev. Med. 2016, 50, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.M.; Kim, S.; Bae, J.; Kim, S.H.; Won, Y.J. Association between relative hand-grip strength and chronic cardiometabolic and musculoskeletal diseases in Koreans: A cross-sectional study. Arch. Gerontol. Geriatr. 2021, 92, 104181. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y. The Korea National Health and nutrition examination survey (KNHANES): Current status and challenges. Epidemiol. Health 2014, 36, e2014002. [Google Scholar] [CrossRef] [Green Version]
- Noh, H.M.; Park, Y.S. Handgrip strength, dynapenia, and mental health in older Koreans. Sci. Rep. 2020, 10, 4004. [Google Scholar] [CrossRef] [Green Version]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing. 2011, 40, 423–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palacio-Agüero, A.; Díaz-Torrente, X.; Dourado, D.Q.S. Relative handgrip strength, nutritional status and abdominal obesity in Chilean adolescents. PLoS ONE 2020, 15, e0234316. [Google Scholar] [CrossRef] [PubMed]
- Punnett, L.; Pruss-Utun, A.; Nelson, D.I.; Fingerhut, M.A.; Leigh, J.; Tak, S.; Phillips, S. Estimating the global burden of low back pain attributable to combined occupational exposures. Am. J. Ind. Med. 2005, 48, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Park, S.M.; Kim, H.J.; Jang, S.; Kim, H.; Chang, B.; Lee, C.; Yeom, J.S. Depression is closely associated with chronic low back pain in patients over 50 years of age: A cross-sectional study using the sixth Korea National Health and Nutrition Examination Survey (KNHANES VI-2). Spine 2018, 43, 1281–1288. [Google Scholar] [CrossRef]
- Pozo-Cruz, B.D.; Gusi, N.; Adsuar, J.C.; Pozo-Cruz, J.D.; Parraca, J.A.; Hernandez-Moncholi, M. Musculoskeletal fitness and health-related quality of life characteristics among sedentary office workers affected by sub-acute, non-specific low back pain: A cross-sectional study. Physiotherapy 2013, 99, 194–200. [Google Scholar] [CrossRef]
- Hartvigsen, J.; Frederiksen, H.; Christensen, K. Physical and mental function and incident low back pain in seniors: A population-based two-year prospective study of 1387 Danish twins aged 70 to 100 years. Spine 2006, 31, 1628–1632. [Google Scholar] [CrossRef]
- McLean, R.R.; Shardell, M.D.; Alley, D.E.; Cawthon, P.M.; Fragala, M.S.; Harris, T.B.; Kenny, A.M.; Peters, K.W.; Ferrucci, L.; Guralnik, J.M. Criteria for clinically relevant weakness and low lean mass and their longitudinal association with incident mobility impairment and mortality: The foundation for the National Institutes of Health (FNIH) sarcopenia project. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2014, 69, 576–583. [Google Scholar] [CrossRef]
- Tanishima, S.; Hagino, H.; Matsumoto, H.; Tanimura, C.; Nagashima, H.J. Association between sarcopenia and low back pain in local residents prospective cohort study from the GAINA study. BMC Musculoskelet. Disord. 2017, 18, 452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakai, Y.; Matsui, H.; Ito, S.; Hida, T.; Ito, K.; Koshimizu, H.; Harada, A. Sarcopenia in elderly patients with chronic low back pain. Osteoporos. Sarcopenia 2017, 3, 195–200. [Google Scholar] [CrossRef]
- Rosenberg, I.H. Epidemiologic and methodologic problems in determining nutritional status of older people.(Summary comments). Am. J. Clin. Nutr. 1989, 50, 1231–1233. [Google Scholar] [CrossRef]
- Frontera, W.R.; Hughes, V.A.; Lutz, K.J.; Evans, W.J. A cross-sectional study of muscle strength and mass in 45- to 78-yr-old men and women. J. Appl. Physiol. 1991, 71, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Cheon, Y.H.; Kim, H.O.; Suh, Y.S.; Kim, M.G.; Yoo, W.; Kim, R.B.; Yang, H.; Lee, S.; Park, K. Relationship between decreased lower extremity muscle mass and knee pain severity in both the general population and patients with knee osteoarthritis: Findings from the KNHANES V 1–2. PLoS ONE 2017, 12, e0173036. [Google Scholar] [CrossRef] [PubMed]
- Einterz, S.F.; Gilliam, R.; Lin, F.C.; McBride, J.M.; Hanson, L.C. Development and testing of a decision aid on goals of care for advanced dementia. J. Am. Med. Dir. Assoc. 2014, 15, 251–255. [Google Scholar] [CrossRef] [Green Version]
- Schaible, H.G.; Ebersberger, A.; Von Banchet, G.S. Mechanisms of pain in arthritis. Ann. N. Y. Acad. Sci. 2002, 966, 343–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Indahl, A.; Velund, L.; Reikeraas, O. Good prognosis for low back pain when left untampered: A randomized clinical trial. Spine 1995, 20, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Kuh, D.; Cooper, C.; Sayer, A.A. Global variation in grip strength: A systematic review and meta-analysis of normative data. Age Ageing 2016, 45, 209–216. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Without Chronic LBP (n = 4291) | With Chronic LBP (n = 1086) | p-Value |
|---|---|---|---|
| Age, years | 63.48 ± 8.84 | 67.13 ± 9.14 | <0.001 |
| Sex, n (%) | <0.001 | ||
| Male | 2115 (49.29) | 300 (27.62) | |
| MFemale | 2176 (50.71) | 786 (72.38) | |
| Obesity (BMI, kg/m2), n (%) | 0.042 | ||
| Underweight (<18.5) | 102 (2.38) | 24 (2.21) | |
| Normal (18.5–24.9) | 2651 (61.78) | 628 (57.83) | |
| Obese (≥25) | 1538 (35.84) | 434 (39.96) | |
| Duration of sleep, h | 6.67 ± 1.43 | 6.38 ± 1.65 | <0.001 |
| Smoking, n (%) | 0.003 | ||
| Non-/Ex -smoker | 3653 (85.13) | 964 (88.77) | |
| Current smoker | 638 (14.87) | 122 (11.23) | |
| Alcohol consumption, n (%) | <0.001 | ||
| None | 1654 (38.55) | 531 (48.9) | |
| ≤1 drink/month | 1027 (23.93) | 279 (25.69) | |
| 2 drinks/month to 3 drinks/week | 1229 (28.64) | 203 (18.69) | |
| ≥4 drinks/week | 381 (8.88) | 73 (6.72) | |
| Education level, n (%) | <0.001 | ||
| ≤6 years | 1478 (34.44) | 641 (59.02) | |
| 7–9 years | 820 (19.1) | 161 (14.82) | |
| 10–12 years | 1181 (27.55) | 186 (17.13) | |
| ≥13 years | 812 (18.92) | 98 (9.02) | |
| Occupation, n (%) | <0.001 | ||
| Unemployed (student, housewife, etc.) | 1869 (43.56) | 642 (59.12) | |
| Office work | 555 (12.93) | 65 (5.98) | |
| Sales and services | 543 (12.65) | 101 (9.3) | |
| Agriculture, forestry, and fishery | 849 (19.79) | 156 (14.36) | |
| Machine fitting and simple labor | 475 (11.07) | 122 (11.23) | |
| Household income, n (%) | <0.001 | ||
| Low | 1068 (24.89) | 478 (44.01) | |
| Low-moderate | 1181 (27.53) | 267 (24.59) | |
| Moderate-high | 981 (22.86) | 173 (15.93) | |
| High | 1061 (24.73) | 168 (15.47) | |
| Aerobic physical activity, n (%) | 1046 (26.86) | 175 (16.36) | <0.001 |
| HGS, kg | 29.68 ± 9.54 | 24.96 ± 8.4 | <0.001 |
| Strong | 2253 (52.51) | 427 (39.32) | <0.001 |
| Weak ** | 2038 (47.49) | 659 (60.68) | <0.001 |
| RHGS, kg * | 1.25 ± 0.41 | 1.04 ± 0.37 | <0.001 |
| Strong | 2269 (52.88) | 417 (38.4) | <0.001 |
| Weak ** | 2022 (47.12) | 669 (61.6) | <0.001 |
| Comorbidities, n (%) | |||
| Hypertension | 1509 (35.17) | 505 (46.5) | <0.001 |
| Diabetes | 541 (12.61) | 192 (17.68) | <0.001 |
| Dyslipidemia | 873 (20.34) | 320 (29.47) | <0.001 |
| Stroke | 136 (3.17) | 72 (6.63) | <0.001 |
| Angina | 109 (2.54) | 59 (5.43) | <0.001 |
| Myocardial infarction | 59 (1.37) | 26 (2.39) | 0.023 |
| Arthritis | 654 (16.69) | 423 (38.95) | <0.001 |
| Malignancy | 123 (2.87) | 34 (3.13) | 0.718 |
| Group | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| HGS | |||||||||
| Strong | 1 | 1 | 1 | ||||||
| Weak | 1.75 | 1.49–2.04 | <0.001 | 1.27 | 1.07–1.50 | 0.005 | 1.22 | 1.02–1.46 | 0.029 |
| RHGS | |||||||||
| Strong | 1 | 1 | 1 | ||||||
| Weak | 1.90 | 1.62–2.24 | <0.001 | 1.45 | 1.20–1.74 | <0.001 | 1.31 | 1.07–1.61 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.; Nah, S.; Jang, H.; Moon, J.; Han, S. Association between Relative Handgrip Strength and Chronic Lower Back Pain: A Nationwide Cross-Sectional Analysis of the Korea National Health and Nutrition Examination Survey. Int. J. Environ. Res. Public Health 2021, 18, 10770. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010770
Choi S, Nah S, Jang H, Moon J, Han S. Association between Relative Handgrip Strength and Chronic Lower Back Pain: A Nationwide Cross-Sectional Analysis of the Korea National Health and Nutrition Examination Survey. International Journal of Environmental Research and Public Health. 2021; 18(20):10770. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010770
Chicago/Turabian StyleChoi, Sungwoo, Sangun Nah, Haedong Jang, Jieun Moon, and Sangsoo Han. 2021. "Association between Relative Handgrip Strength and Chronic Lower Back Pain: A Nationwide Cross-Sectional Analysis of the Korea National Health and Nutrition Examination Survey" International Journal of Environmental Research and Public Health 18, no. 20: 10770. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010770