
In-Hospital Mortality in Non-COVID-19-Related Diseases before and during the Pandemic: A Regional Retrospective Study


Abstract
:1. Introduction
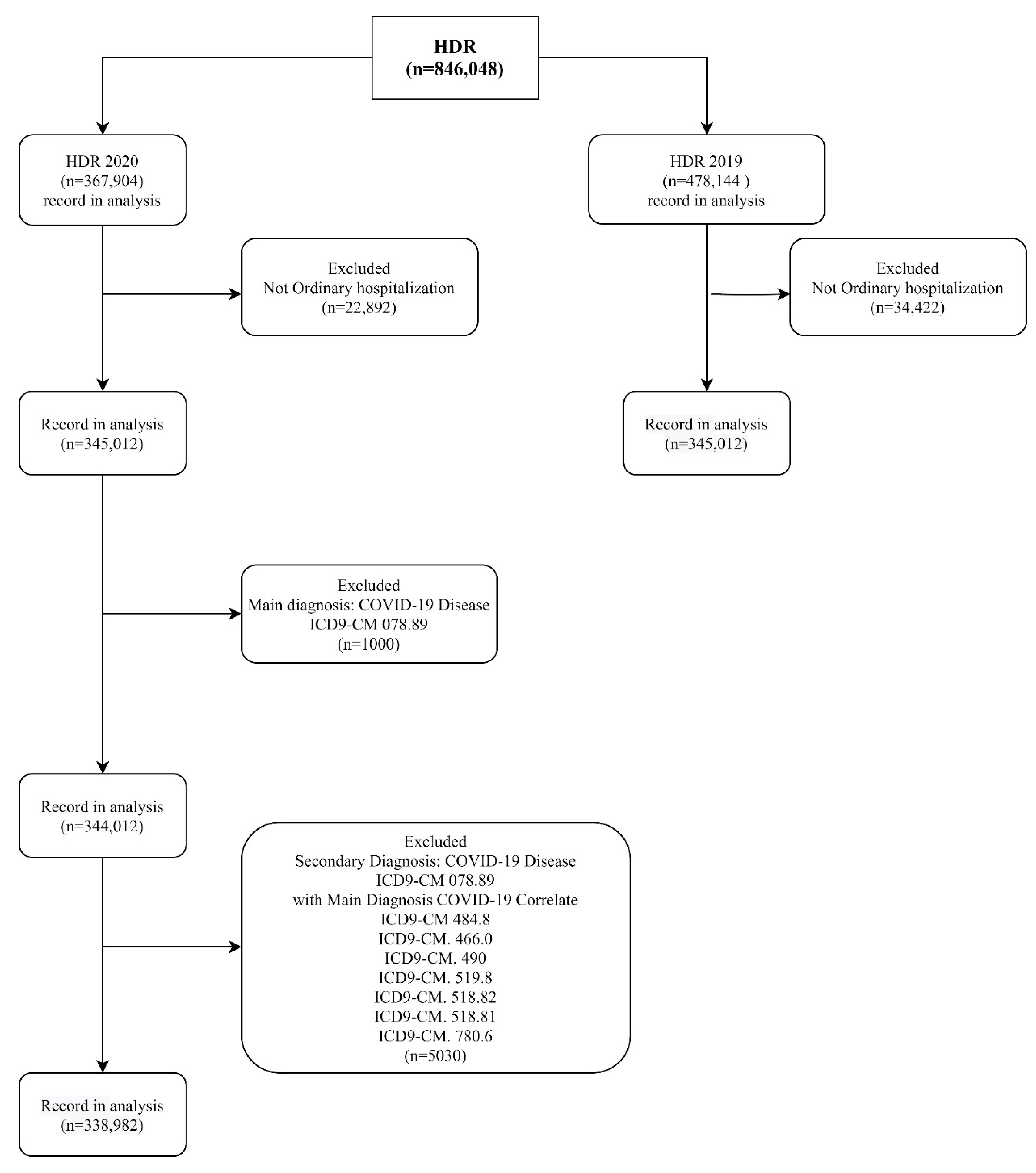
2. Materials and Methods
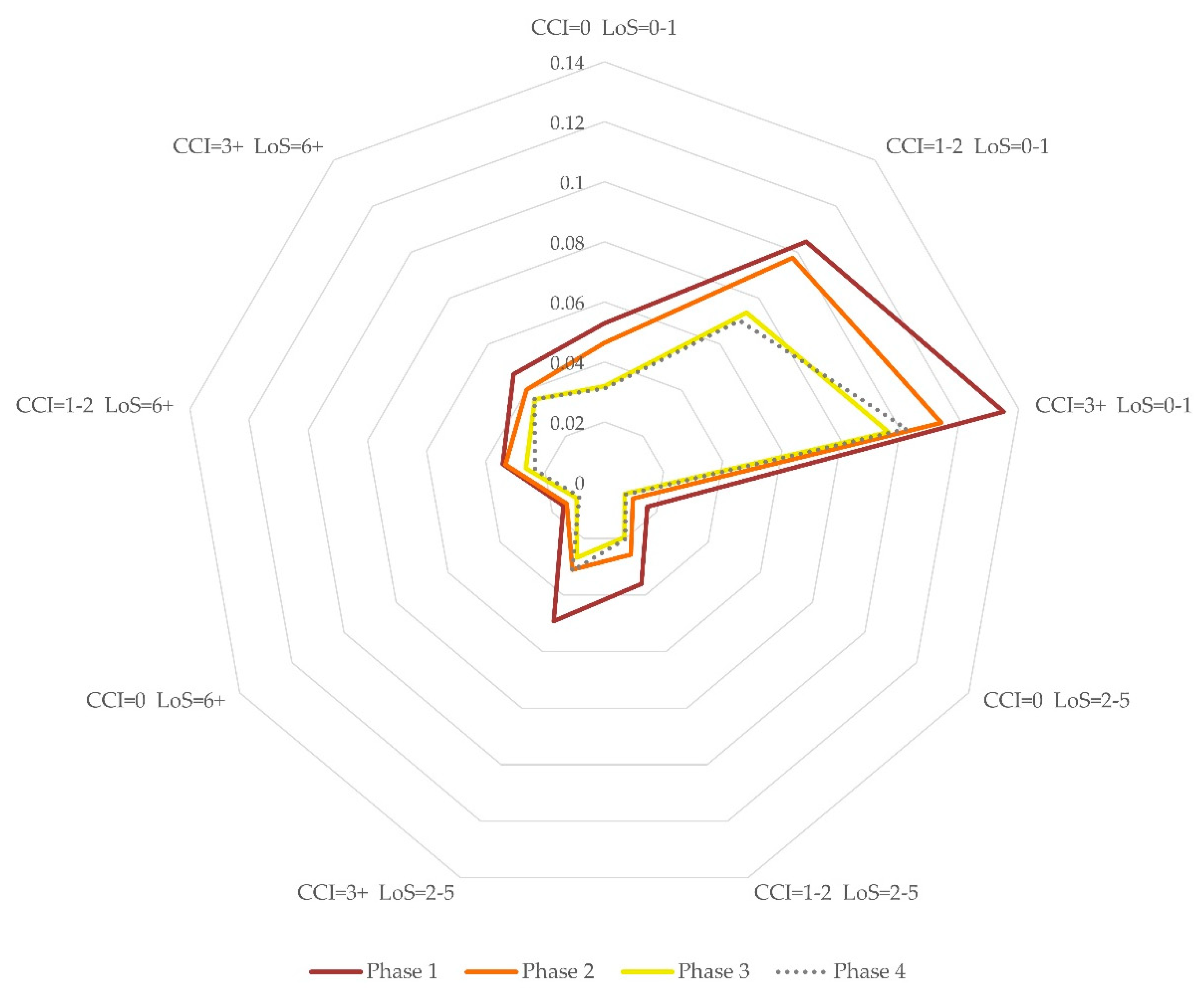
- Phase 1, from 1 March 2020 to 30 April 2020, “total lockdown”, with a high level of restrictions: ban on leaving the house except out of necessity, suspension of educational services, closure of all commercial activities and public offices [6];
- Phase 3, from 16 June 2020 to 30 September 2020, with a low level of restriction: suspension of educational indoor service, reduction of the number of people accessing commercial activities [23].
- Phase 4, from 1 January 2019 to 29 February 2020, with no restrictions except quarantine for COVID-19 patients.
3. Results
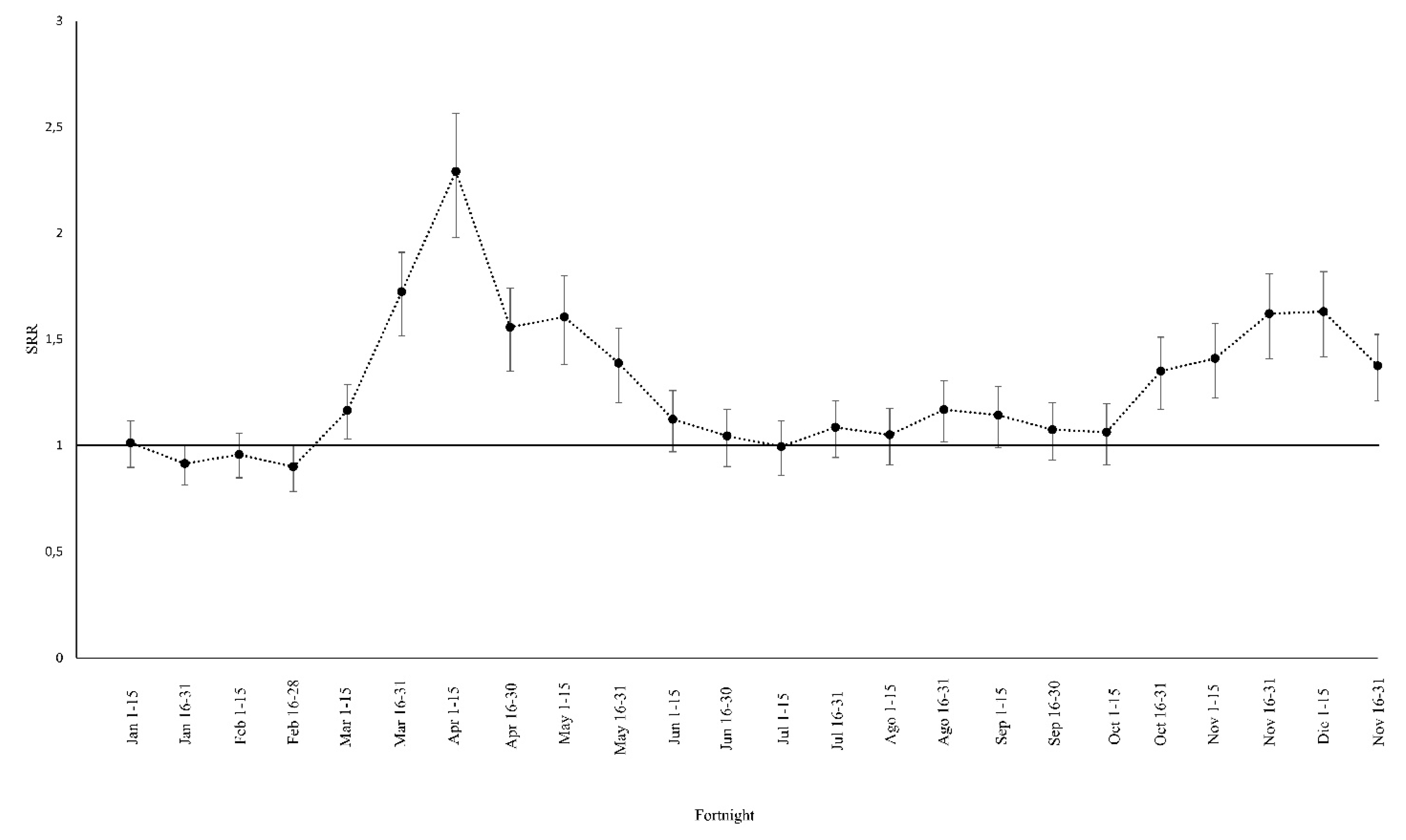
3.1. Standardized Mortality Rates. Comparison between 2019 and 2020
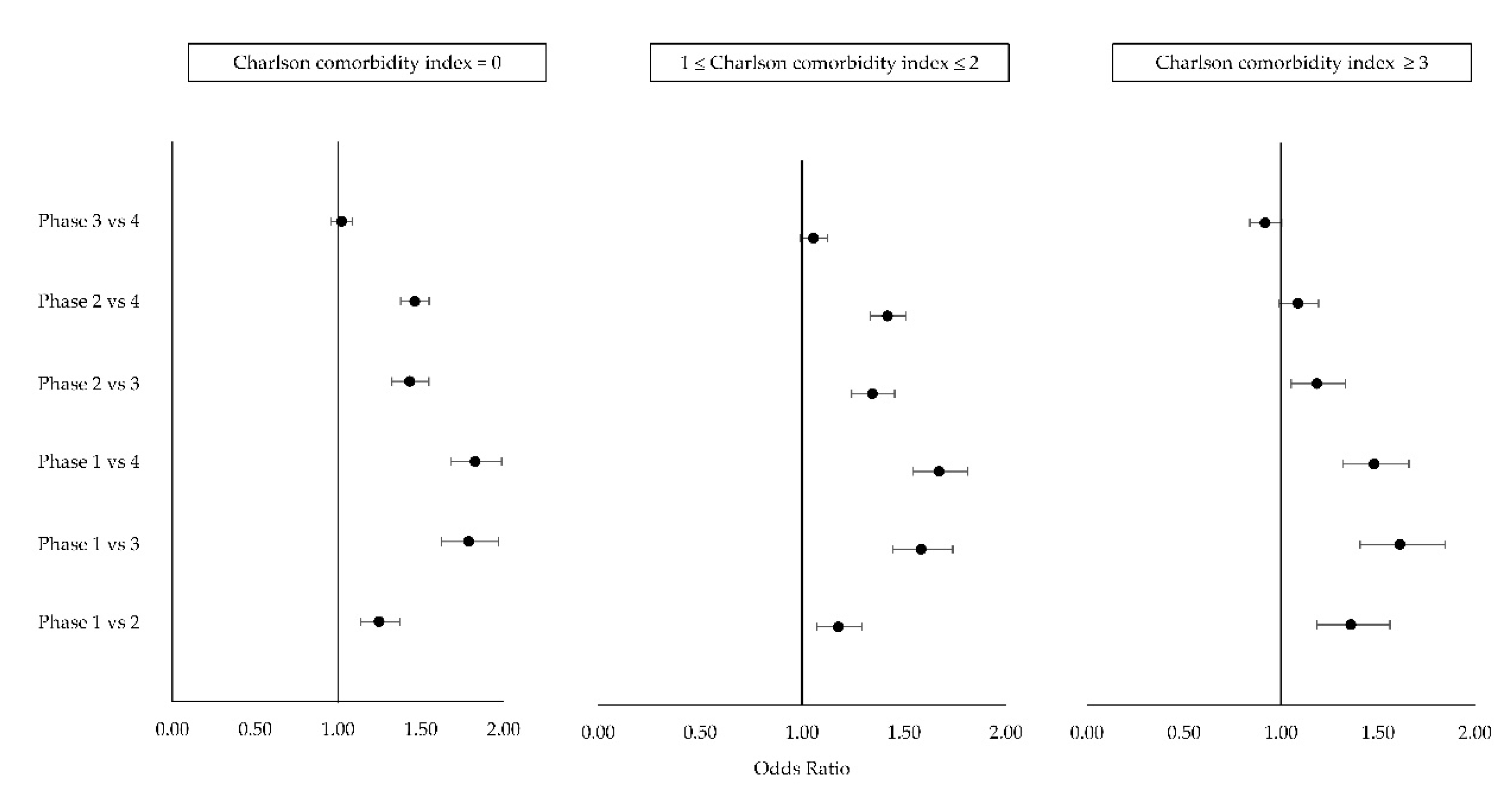
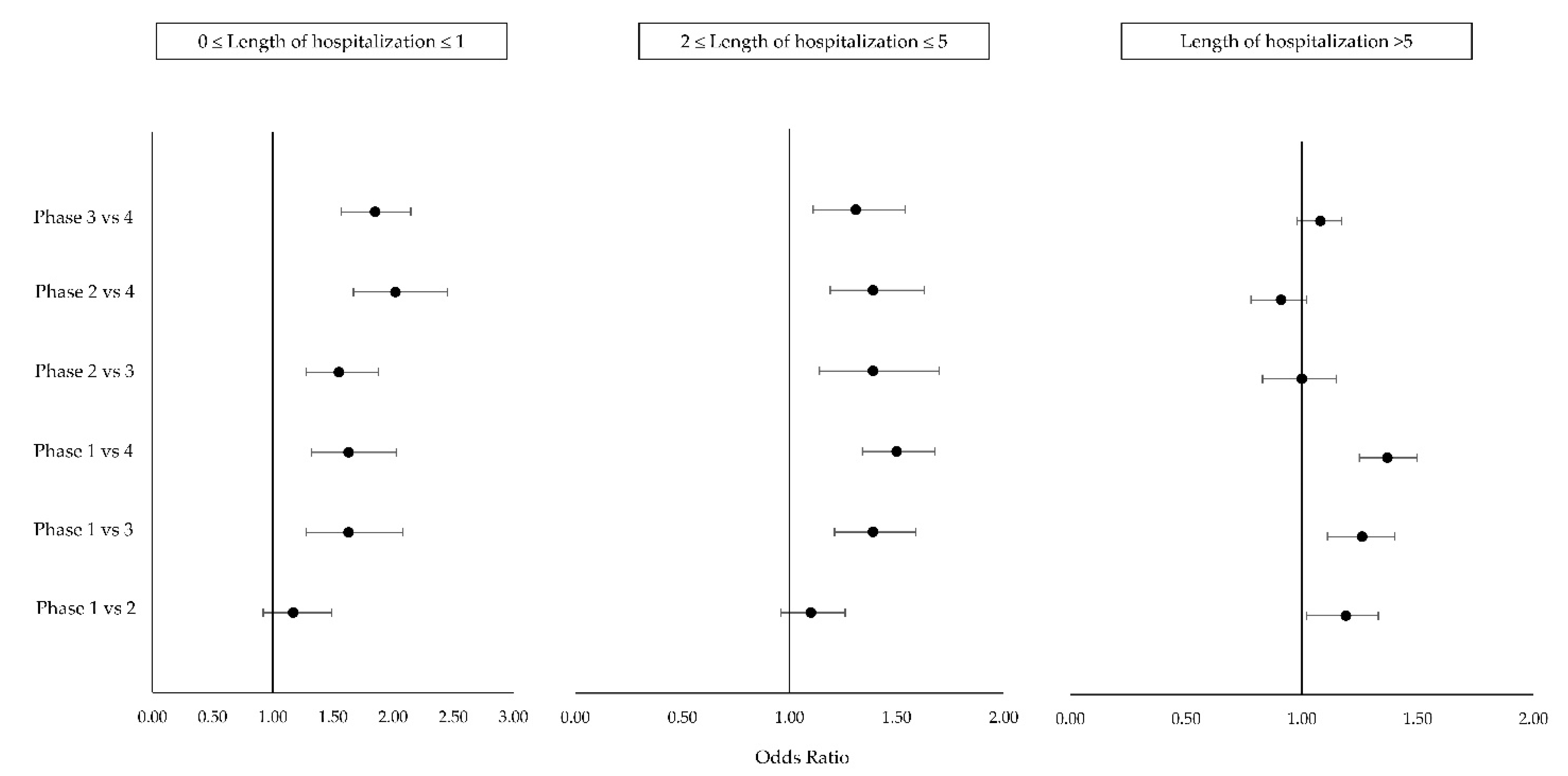
3.2. Effect of the Pandemic Phases on Mortality: Multivariable Model
4. Discussion
5. Study Limitation
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Annual Report on Hospital Activity, Data from Hospital Discharge Forms 2019, Ministry of Health. Available online: http://www.salute.gov.it/portale/temi/p2_4.jsp?lingua=italiano&tema=Assistenza,%20ospedale%20e%20territorio&area=ricoveriOspedalieri (accessed on 6 August 2021).
- Odone, A.; Delmonte, D.; Scognamiglio, T.; Signorelli, C. COVID-19 Deaths in Lombardy, Italy: Data in Context. Lancet Public Health 2020, 5, e310. [Google Scholar] [CrossRef]
- Livingston, E.; Bucher, K. Coronavirus Disease 2019 (COVID-19) in Italy. JAMA 2020, 323, 1335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibertoni, D.; Adja, K.Y.C.; Golinelli, D.; Reno, C.; Regazzi, L.; Lenzi, J.; Sanmarchi, F.; Fantini, M.P. Patterns of COVID-19 Related Excess Mortality in the Municipalities of Northern Italy during the First Wave of the Pandemic. Health Place 2021, 67, 102508. [Google Scholar] [CrossRef] [PubMed]
- Kinross, P.; Suetens, C.; Gomes Dias, J.; Alexakis, L.; Wijermans, A.; Colzani, E.; Monnet, D.L. ECDC Public Health Emergency Team Rapidly Increasing Cumulative Incidence of Coronavirus Disease (COVID-19) in the European Union/European Economic Area and the United Kingdom, 1 January to 15 March 2020. Euro Surveill 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- D.L. 23 February 2020, n.6 “Urgent Measures in Containement and Management of the Epidemiological Emergency from COVID-19” (G.U. no 45 of 23-2-2020). Available online: https://www.gazzettaufficiale.it/eli/id/2020/02/23/20G00020/sg (accessed on 5 August 2021).
- DPCM 11 March 2020, “Further Implementing Provisions of the D.L. 23 February, no 6, Containing Urgent Measures on Containment and Management of the Epidemiological Emergency from COVID-19, Applicable on the Entire National Territory” (G.U. no. 64 of 11/03/2020). Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/11/20A01605/sg (accessed on 5 August 2021).
- DPCM 22 March 2020 “Further Implementing Provisions of the D.L. 23 February, no 6, Containing Urgent Measures on Containment and Management of the Epidemiological Emergency from COVID-19, Applicable on the Entire National Territory” (GU no 76 of 22-03-2020). Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/22/20A01807/sg (accessed on 5 August 2021).
- DPCM 26 April 2020, “Further Implementing Provisions of the D.L. 23 February, no 6, Containing Urgent Measures on Containment and Management of the Epidemiological Emergency from COVID-19, Applicable on the Entire National Territory” (GU no 108 of 27-04-2020). Available online: https://www.gazzettaufficiale.it/eli/id/2020/04/27/20A02352/sg (accessed on 5 August 2021).
- Ministry of Health, Italy, Rome, Circular 1 March 2020, Prot. no 2627–Increase in the Availability of Beds in the National Health Service and Further Indications Relating to the Management of the COVID-19 Emergency. Available online: https://www.sicp.it/wp-content/uploads/2020/03/Circolare-2627-_Min-Sal_1-mar-20.pdf (accessed on 5 August 2021).
- Ministry of Health, Italy, Rome, Circular 16 March 2020, Prot. no 7422-Guidelines for the Remodelling of Scheduled Activities Deferred in the Course of Emergency from COVID-19. Available online: http://www.prefettura.it/FILES/AllegatiPag/1221/Circolare_del_Ministero_della_Salute_n.7422_del_16_marzo_2020.pdf (accessed on 5 August 2021).
- Ministry of Health, Italy, Rome, Circular 25 March 2020, Prot. no 7865-Update of the Organizational Guidelines for Hospital and Territorial Service in COVID-19 Emergency. Available online: https://www.frareg.com/cms/wp-content/uploads/2020/03/circolare_7865_25032020.pdf (accessed on 5 August 2021).
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The Impact of the COVID-19 Pandemic on Cancer Deaths Due to Delays in Diagnosis in England, UK: A National, Population-Based, Modelling Study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]
- Adelhoefer, S.; Berning, P.; Solomon, S.B.; Maybody, M.; Whelton, S.P.; Blaha, M.J.; Dzaye, O. Decreased Public Pursuit of Cancer-Related Information during the COVID-19 Pandemic in the United States. Cancer Causes Control. 2021, 32, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Santi, L.; Golinelli, D.; Tampieri, A.; Farina, G.; Greco, M.; Rosa, S.; Beleffi, M.; Biavati, B.; Campinoti, F.; Guerrini, S.; et al. Non-COVID-19 Patients in Times of Pandemic: Emergency Department Visits, Hospitalizations and Cause-Specific Mortality in Northern Italy. PLoS ONE 2021, 16, e0248995. [Google Scholar] [CrossRef] [PubMed]
- İlhan, B.; Bozdereli Berikol, G.; Dogan, H. Impact of COVID-19 Outbreak on Emergency Visits and Emergency Consultations: A Cross-Sectional Study. Cureus 2021, 13, e14052. [Google Scholar] [CrossRef] [PubMed]
- Havenon, A.D.; Ney, J.P.; Callaghan, B.; Hohmann, S.; Shippey, E.; Yaghi, S.; Anadani, M.; Majersik, J.J. Characteristics and Outcomes among US Patients Hospitalized for Ischemic Stroke before vs. during the COVID-19 Pandemic. JAMA Netw. Open 2021, 4, e2110314. [Google Scholar] [CrossRef] [PubMed]
- Mafham, M.M.; Spata, E.; Goldacre, R.; Gair, D.; Curnow, P.; Bray, M.; Hollings, S.; Roebuck, C.; Gale, C.P.; Mamas, M.A.; et al. COVID-19 Pandemic and Admission Rates for and Management of Acute Coronary Syndromes in England. Lancet 2020, 396, 381–389. [Google Scholar] [CrossRef]
- Mesnier, J.; Cottin, Y.; Coste, P.; Ferrari, E.; Schiele, F.; Lemesle, G.; Thuaire, C.; Angoulvant, D.; Cayla, G.; Bouleti, C.; et al. Hospital Admissions for Acute Myocardial Infarction before and after Lockdown According to Regional Prevalence of COVID-19 and Patient Profile in France: A Registry Study. Lancet Public Health 2020, 5, e536–e542. [Google Scholar] [CrossRef]
- Hospital Mortality-A Neglected but Rich Source of Information Supporting the Transition to Higher Quality Health Systems in Low and Middle Income Countries|BMC Medicine|Full Text. Available online: https://0-bmcmedicine-biomedcentral-com.brum.beds.ac.uk/articles/10.1186/s12916-018-1024-8 (accessed on 5 August 2021).
- SDO Coding Guidelines for SARS Cov-2 Disease. Available online: https://www.soresa.it/pa/Contenuti/Flussi%20Sanitari/SDO/Linee%20Guida%20Ministero%20COVID-19/Linee%20Guida%20codifica%20SDO%20COVID19.pdf (accessed on 5 August 2021).
- D.L. 7 October 2020, no 125, “Urgent Measures Connected with the Extension of the Declaration of the State of Epidemiological Emergency from COVID-19, for the Deferral of Electoral Consultations for the Year 2020 and for the Continuity of Operation of the COVID Alert System, as Well as for the Implementation of the Directive EU 2020/739 of 3 June 2020, and Urgent Provions on Tax Collection" (GU no. 248 of 7-10-2020). Available online: https://www.gazzettaufficiale.it/eli/id/2020/10/07/20G00144/sg (accessed on 5 August 2021).
- DPCM 11 June 2020, “Further Implementing Provisions of the D.L. no 19 of 25 March 2020, Containing Urgent Measures to Cope with the Epidemiological Emergency from COVID-19, and D.L. no 33 of 16 May 2020, Containing Additional Urgent Measures to Cope with the Epidemiological Emergency form COVID-19”. Available online: https://www.gazzettaufficiale.it/eli/id/2020/06/11/20A03194/sg (accessed on 5 August 2021).
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Butt, J.H.; Fosbøl, E.L.; Gerds, T.A.; Andersson, C.; Kragholm, K.; Biering-Sørensen, T.; Andersen, J.; Phelps, M.; Andersen, M.P.; Gislason, G.; et al. All-Cause Mortality and Location of Death in Patients with Established Cardiovascular Disease before, during, and after the COVID-19 Lockdown: A Danish Nationwide Cohort Study. Eur. Heart J. 2021, 42, 1516–1523. [Google Scholar] [CrossRef] [PubMed]
- EpiCentro FluNews: Archive. Available online: https://www.epicentro.iss.it/influenza/FluNewsArchivio (accessed on 5 August 2021).
- Influenza Vaccination-Comparisons of Cover in the General Population in 2020–2021. Available online: https://www.salute.gov.it/imgs/C_17_tavole_19_3_0_file.pdf (accessed on 5 August 2021).
- Jeffery, M.M.; D’Onofrio, G.; Paek, H.; Platts-Mills, T.F.; Soares, W.E.; Hoppe, J.A.; Genes, N.; Nath, B.; Melnick, E.R. Trends in Emergency Department Visits and Hospital Admissions in Health Care Systems in 5 States in the First Months of the COVID-19 Pandemic in the US. JAMA Intern. Med. 2020, 180, 1328–1333. [Google Scholar] [CrossRef] [PubMed]
- Stirparo, G.; Oradini-Alacreu, A.; Migliori, M.; Villa, G.F.; Botteri, M.; Fagoni, N.; Signorelli, C.; Sechi, G.M.; Zoli, A. Public Health Impact of the COVID-19 Pandemic on the Emergency Healthcare System. J. Public Health 2021, fdab212. [Google Scholar] [CrossRef] [PubMed]
- Covid19-Italy Situation. Available online: https://opendatadpc.maps.arcgis.com/apps/dashboards/b0c68bce2cce478eaac82fe38d4138b1 (accessed on 5 August 2021).
- Rosenbaum, L. The Untold Toll-The Pandemic’s Effects on Patients without Covid-19. N. Engl. J. Med. 2020, 382, 2368–2371. [Google Scholar] [CrossRef] [PubMed]
- Hubert, H.; Baert, V.; Beuscart, J.-B.; Chazard, E. Use of Out-of-Hospital Cardiac Arrest Registries to Assess COVID-19 Home Mortality. BMC Med. Res. Methodol. 2020, 20, 305. [Google Scholar] [CrossRef] [PubMed]
- Rossen, L.M. Excess Deaths Associated with COVID-19, by Age and Race and Ethnicity—United States, January 26–October 3, 2020. MMWR Morb Mortal Wkly. Rep. 2020, 69, 1522. [Google Scholar] [CrossRef] [PubMed]
- Bilinski, A.; Emanuel, E.J. COVID-19 and Excess All-Cause Mortality in the US and 18 Comparison Countries. JAMA 2020, 324, 2100–2102. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | 2019 | 2020 | Total | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Sex | ||||||
| Male | 214.274 | 48.3 | 162.698 | 48.0 | 376.972 | 48.2 |
| Female | 229.448 | 51.7 | 176.284 | 52.0 | 405.732 | 51.8 |
| Age (years) | ||||||
| 0–4 | 46.034 | 10.4 | 36.346 | 10.7 | 82.380 | 10.5 |
| 5–14 | 14.680 | 3.3 | 8.353 | 2.5 | 23.033 | 2.9 |
| 15–24 | 18.218 | 4.1 | 12.756 | 3.8 | 30.974 | 4.0 |
| 25–44 | 70.994 | 16.0 | 56.757 | 16.7 | 127.751 | 16.3 |
| 45–64 | 98.052 | 22.1 | 75.082 | 22.2 | 173.134 | 22.1 |
| 65–74 | 76.613 | 17.3 | 60.572 | 17.9 | 137.185 | 17.5 |
| >75 | 119.131 | 26.9 | 89.116 | 26.3 | 208.247 | 26.6 |
| Hospital discharge | ||||||
| Death | 13.267 | 3.0 | 12.125 | 3.6 | 25.392 | 3.2 |
| Alive | 430.455 | 97.0 | 326.857 | 96.4 | 757.312 | 96.8 |
| Charlson Index (score) | ||||||
| 0 | 316.421 | 71.3 | 242.920 | 71.7 | 559.341 | 71.5 |
| 1–2 | 95.568 | 21.5 | 72.402 | 21.4 | 167.970 | 21.5 |
| ≥3 | 31.733 | 7.2 | 23.660 | 7.0 | 55.393 | 7.1 |
| Length of Stay (days) | ||||||
| 0–1 | 44.884 | 10.1 | 32.069 | 9.5 | 76.953 | 9.8 |
| 2–5 | 215.779 | 48.6 | 169.568 | 50.0 | 385.347 | 49.2 |
| 5+ | 183.059 | 41.3 | 137.345 | 40.5 | 320.404 | 40.9 |
| Parameter | Type 3 Effects | OR [CI 95%] 1 | ||
|---|---|---|---|---|
| Chi-Square | p-Value | |||
| Sex | Male | 7.8 | 0.0052 | 1.04 [1.01–1.07] |
| Female | Ref. | |||
| Age (years) | 0–4 | 10,199.1 | <0.0001 | 0.04 [0.03–0.05] |
| 5–14 | 0.01 [0–0.02] | |||
| 15–24 | 0.03 [0.02–0.05] | |||
| 25–44 | 0.06 [0.05–0.07] | |||
| 45–64 | 0.23 [0.22–0.24] | |||
| 65–74 | 0.4 [0.38–0.42] | |||
| >75 | Ref. | |||
| Phase | 1 | 397.4 | <0.0001 | 1.65 [1.53–1.79] |
| 2 | 1.31 [1.24–1.39] | |||
| 3 | 1.00 [0.94–1.06] | |||
| 4 | Ref. | |||
| Charlson Index (score) | 0 | 2973.6 | <0.0001 | 0.29 [0.27–0.31] |
| 1–2 | 0.71 [0.67–0.75] | |||
| 3+ | Ref. | |||
| Length of Stay (days) | 0–1 | 3196.5 | <0.0001 | 3.47 [3.27–3.68] |
| 2–5 | 0.84 [0.8–0.88] | |||
| 5+ | Ref. | |||
| Phase ∗ Ich class | 40.3 | <0.0001 | see Figure 3 | |
| Phase ∗ LoS class | 40.6 | <0.0001 | see Figure 4 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartolomeo, N.; Giotta, M.; Trerotoli, P. In-Hospital Mortality in Non-COVID-19-Related Diseases before and during the Pandemic: A Regional Retrospective Study. Int. J. Environ. Res. Public Health 2021, 18, 10886. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010886
Bartolomeo N, Giotta M, Trerotoli P. In-Hospital Mortality in Non-COVID-19-Related Diseases before and during the Pandemic: A Regional Retrospective Study. International Journal of Environmental Research and Public Health. 2021; 18(20):10886. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010886
Chicago/Turabian StyleBartolomeo, Nicola, Massimo Giotta, and Paolo Trerotoli. 2021. "In-Hospital Mortality in Non-COVID-19-Related Diseases before and during the Pandemic: A Regional Retrospective Study" International Journal of Environmental Research and Public Health 18, no. 20: 10886. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010886