
The Efficacy of a Calamansi-Containing Energy Drink on Running Performance and Recovery in NCAA Division I Middle-Distance Runners: A Preliminary Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
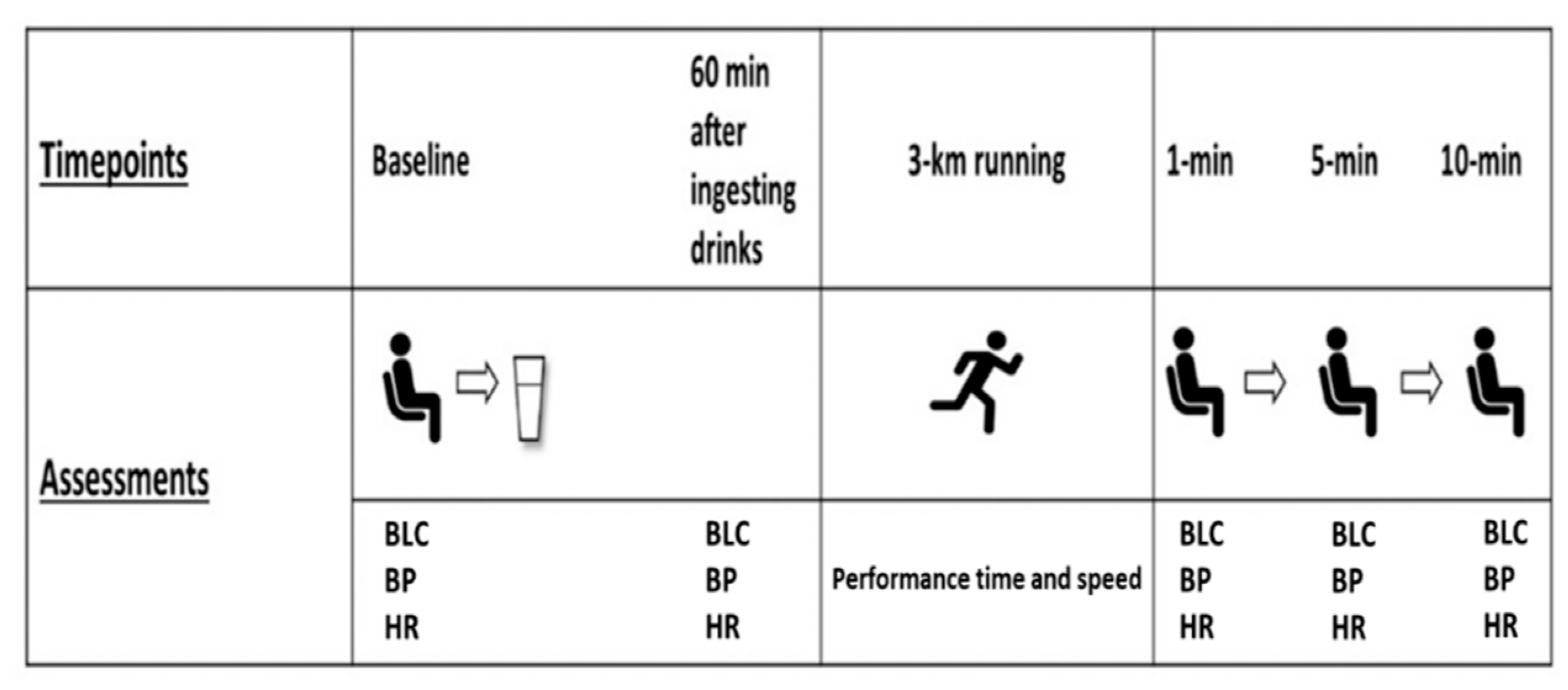
2.1. Study Design
2.2. Participants
2.3. Body Composition
2.4. Blood Lactate Concentration Measurement
2.5. Blood Pressure and Heart Rate Measurements
2.6. 3-Km Running Trials
2.7. ED and Placebo Drink
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Vento, K.A.; Wardenaar, F.C. Third-party testing nutritional supplement knowledge, attitudes, and use among an NCAA I collegiate student-athlete population. Front. Sports Act. Living 2020, 2, 115. [Google Scholar] [CrossRef]
- Reissig, C.J.; Strain, E.C.; Griffiths, R.R. Caffeinated energy drinks—A growing problem. Drug Alcohol Depend. 2009, 99, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Pickering, C.; Grgic, J. Caffeine and exercise: What next? Sports Med. 2019, 49, 1007–1030. [Google Scholar] [CrossRef] [Green Version]
- Wiklund, U.; Karlsson, M.; Öström, M.; Messner, T. Influence of energy drinks and alcohol on post-exercise heart rate recovery and heart rate variability. Clin. Physiol. Funct. Imaging 2009, 29, 74–80. [Google Scholar] [CrossRef]
- Bunsawat, K.; White, D.W.; Kappus, R.M.; Baynard, T. Caffeine delays autonomic recovery following acute exercise. Eur. J. Prev. Cardiol. 2015, 22, 1473–1479. [Google Scholar] [CrossRef]
- Wikoff, D.; Welsh, B.T.; Henderson, R.; Brorby, G.P.; Britt, J.; Myers, E.; Goldberger, J.; Lieberman, H.R.; O’Brien, C.; Peck, J. Systematic review of the potential adverse effects of caffeine consumption in healthy adults, pregnant women, adolescents, and children. Food Chem. Toxicol. 2017, 109, 585–648. [Google Scholar] [CrossRef] [PubMed]
- Muacevic, A.; Adler, J.; Hanif, M.; Saleem, S.; Naz, S.; Sundas, F. Energy Drinks and Atrial Fibrillation: An Unusual Case of Caution. Cureus 2020, 12, e10807. [Google Scholar]
- Brunton, V.; Kneale, D.; Sowden, A.; Sutcliffe, K.; Thomas, J. Caffeinated Energy Drinks and Effects in UK Young People; UCL Institute of Education: London, UK, 2019. [Google Scholar]
- Caine, J.J.; Geracioti, T.D. Taurine, energy drinks, and neuroendocrine effects. Clevel. Clin. J. Med. 2016, 83, 895–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yatabe, Y.; Miyakawa, S.; Ohmori, H.; Adachi, H.M.T. Effects of Taurine Administration on Exercise; Springer: Berlin/Heidelberg, Germany, 2009; pp. 245–252. [Google Scholar]
- Maleki, V.; Mahdavi, R.; Hajizadeh-Sharafabad, F.; Alizadeh, M. A comprehensive insight into potential roles of taurine on metabolic variables in type 2 diabetes: A systematic review. Pharm. Sci. 2020, 26, 225–238. [Google Scholar] [CrossRef]
- Balshaw, T.G.; Bampouras, T.M.; Barry, T.J.; Sparks, S.A. The effect of acute taurine ingestion on 3-km running performance in trained middle-distance runners. Amino Acids 2013, 44, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, T.; Matsuzaki, Y.; Ikegami, T.; Miyakawa, S.; Doy, M.; Tanaka, N.; Bouscarel, B. Optimal and effective oral dose of taurine to prolong exercise performance in rat. Amino Acids 2004, 27, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Koma, R.; Terasawa, N. Pre-Exercise Glucose Ingestion May Improve Endurance Capacity in East Asian Student Athletes with Lower Blood Glucose Response. J. Nutr. Sci. Vitaminol. 2020, 66, 150–157. [Google Scholar] [CrossRef]
- Pomportes, L.; Brisswalter, J. Carbohydrate mouth rinse effects on physical and cognitive performance: Benefits and limitations in sports. Sci. Sports 2020, 35, 200–206. [Google Scholar] [CrossRef]
- Powers, S.K.; Deminice, R.; Ozdemir, M.; Yoshihara, T.; Bomkamp, M.P.; Hyatt, H. Exercise-induced oxidative stress: Friend or foe? J. Sport Health Sci. 2020, 9, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Reid, H.; Foster, C. Infographic. Physical activity benefits for adults and older adults. Br. J. Sports Med. 2017, 51, 1441–1442. [Google Scholar] [CrossRef] [PubMed]
- Powers, S.K.; Ji, L.L.; Kavazis, A.N.; Jackson, M.J. Reactive oxygen species: Impact on skeletal muscle. Compr. Physiol. 2011, 1, 941. [Google Scholar] [PubMed] [Green Version]
- Savini, I.; Catani, M.V.; Duranti, G.; Ceci, R.; Sabatini, S.; Avigliano, L. Vitamin C homeostasis in skeletal muscle cells. Free Radic. Biol. Med. 2005, 38, 898–907. [Google Scholar] [CrossRef] [PubMed]
- Hoppel, C. The role of carnitine in normal and altered fatty acid metabolism. Am. J. Kidney Dis. 2003, 41, S4–S12. [Google Scholar] [CrossRef]
- Russell, K.; Wyatt, F.B.; Yoo, D.S. Effects of Energy Drink on Metabolic Response and Exercise Performance Post Basketball Game Simulation. Int. J. Exerc. Sci. 2017, 2, 85. [Google Scholar]
- Campbell, C.; Prince, D.; Braun, M.; Applegate, E.; Casazza, G.A. Carbohydrate-supplement form and exercise performance. Int. J. Sport Nutr. Exerc. Metab. 2008, 18, 179–190. [Google Scholar] [CrossRef]
- Siri, W.E. Body Composition from Fluid Spaces and Density: Analysis of Methods. 1956. Available online: https://escholarship.org/content/qt6mh9f4nf/qt6mh9f4nf.pdf (accessed on 17 October 2021).
- Jackson, A.S.; Pollock, M.L. Generalized equations for predicting body density of men. Br. J. Nutr. 1978, 40, 497–504. [Google Scholar] [CrossRef] [Green Version]
- Kulandaivelan, S.; Verma, S.; Mukhopadhyay, S.; Vignesh, N. Test retest reproducibility of a hand-held lactate analyzer in healthy men. J. Exerc. Sci. Physiother. 2009, 5, 30–33. [Google Scholar]
- Beck, T.W.; Housh, T.J.; Schmidt, R.J.; Johnson, G.O.; Housh, D.J.; Coburn, J.W.; Malek, M.H. The acute effects of a caffeine-containing supplement on strength, muscular endurance, and anaerobic capabilities. J. Strength Cond. Res. 2006, 20, 506–510. [Google Scholar]
- Prins, P.J.; Goss, F.L.; Nagle, E.F.; Beals, K.; Robertson, R.J.; Lovalekar, M.T.; Welton, G.L. Energy drinks improve five-kilometer running performance in recreational endurance runners. J. Strength Cond. Res. 2016, 30, 2979–2990. [Google Scholar] [CrossRef]
- Felippe, L.C.; Ferreira, G.A.; Learsi, S.K.; Boari, D.; Bertuzzi, R.; Lima-Silva, A.E. Caffeine increases both total work performed above critical power and peripheral fatigue during a 4-km cycling time trial. J. Appl. Physiol. 2018, 124, 1491–1501. [Google Scholar] [CrossRef] [Green Version]
- Souza, D.B.; Del Coso, J.; Casonatto, J.; Polito, M.D. Acute effects of caffeine-containing energy drinks on physical performance: A systematic review and meta-analysis. Eur. J. Nutr. 2017, 56, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Niles, E.S.; Lachowetz, T.; Garfi, J.; Sullivan, W.; Smith, J.C.; Leyh, B.P.; Headley, S.A. Carbohydrate-protein drink improves time to exhaustion after recovery from endurance exercise. J. Exerc. Physiol. Online 2001, 4, 45–52. [Google Scholar]
- Khanna, G.; Manna, I. Supplementary effect of carbohydrate-electrolyte drink on sports performance, lactate removal & cardiovascular response of athletes. Indian J. Med. Res. 2005, 121, 665. [Google Scholar] [PubMed]
- Neufer, P.D.; Costill, D.L.; Flynn, M.G.; Kirwan, J.P.; Mitchell, J.B.; Houmard, J. Improvements in exercise performance: Effects of carbohydrate feedings and diet. J. Appl. Physiol. 1987, 62, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Chambers, E.; Bridge, M.; Jones, D. Carbohydrate sensing in the human mouth: Effects on exercise performance and brain activity. J. Physiol. 2009, 587, 1779–1794. [Google Scholar] [CrossRef] [PubMed]
- Hargreaves, M.; Hawley, J.A.; Jeukendrup, A. Pre-exercise carbohydrate and fat ingestion: Effects on metabolism and performance. J. Sports Sci. 2004, 22, 31–38. [Google Scholar] [CrossRef]
- Marmy-Conus, N.; Fabris, S.; Proietto, J.; Hargreaves, M. Preexercise glucose ingestion and glucose kinetics during exercise. J. Appl. Physiol. 1996, 81, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Candow, D.G.; Kleisinger, A.K.; Grenier, S.; Dorsch, K.D. Effect of sugar-free Red Bull energy drink on high-intensity run time-to-exhaustion in young adults. J. Strength Cond. Res. 2009, 23, 1271–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahnama, N.; Gaeini, A.A.; Kazemi, F. The effectiveness of two energy drinks on selected indices of maximal cardiorespiratory fitness and blood lactate levels in male athletes. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2010, 15, 127. [Google Scholar]
- Halliwill, J.R.; Buck, T.M.; Lacewell, A.N.; Romero, S.A. Postexercise hypotension and sustained postexercise vasodilatation: What happens after we exercise? Exp. Physiol. 2013, 98, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Kenney, M.J.; Seals, D.R. Postexercise hypotension. Key features, mechanisms, and clinical significance. Hypertension 1993, 22, 653–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braakhuis, A.J. Effect of vitamin C supplements on physical performance. Curr. Sports Med. Rep. 2012, 11, 180–184. [Google Scholar] [CrossRef]
- Salem, V.; Izzi-Engbeaya, C.; Coello, C.; Thomas, D.; Chambers, E.; Comninos, A.; Buckley, A.; Win, Z.; Al-Nahhas, A.; Rabiner, E. Glucagon increases energy expenditure independently of brown adipose tissue activation in humans. Diabetes Obes. Metab. 2016, 18, 72–81. [Google Scholar] [CrossRef] [Green Version]
- Galley, H.F.; Thornton, J.; Howdle, P.D.; Walker, B.E.; Webster, N.R. Combination oral antioxidant supplementation reduces blood pressure. Clin. Sci. 1997, 92, 361–365. [Google Scholar] [CrossRef] [Green Version]
- Duffy, S.; Gokce, N.; Holbrook, M.; Huang, A.; Frei, B.; Keaney Jr, J.F.; Vita, J.A. Treatment of hypertension with ascorbic acid. Lancet 1999, 354, 2048–2049. [Google Scholar] [CrossRef]
- Sun, Q.; Wang, B.; Li, Y.; Sun, F.; Li, P.; Xia, W.; Zhou, X.; Li, Q.; Wang, X.; Chen, J. Taurine supplementation lowers blood pressure and improves vascular function in prehypertension: Randomized, double-blind, placebo-controlled study. Hypertension 2016, 67, 541–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullan, B.A.; Young, I.S.; Fee, H.; McCance, D.R. Ascorbic acid reduces blood pressure and arterial stiffness in type 2 diabetes. Hypertension 2002, 40, 804–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abebe, W.; Mozaffari, M.S. Role of taurine in the vasculature: An overview of experimental and human studies. Am. J. Cardiovasc. Dis. 2011, 1, 293. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Mean ± SD |
|---|---|
| Age (years) | 20.8 ± 1.5 |
| Height (cm) | 173.8 ± 9.9 |
| Weight (kg) | 60.5 ± 10.7 |
| Body mass index (kg/m2) | 20.0 ± 2.5 |
| Sum of skinfold thickness (mm) | 34.6 ± 16.9 |
| Body fat percentage (%) | 9.3 ± 5.1 |
| Systolic BP (mmHg) | 116.7 ± 8.2 |
| Diastolic BP (mmHg) | 70.9 ± 12.2 |
| Resting heart rate (beats/min) | 58.7 ± 9.5 |
| Resting lactate concentration (mmol/L) | 1.67 ± 0.7 |
| Trial | Baseline | Before Running | R 1 min | R 5 min | R 10 min | F-value | |||
|---|---|---|---|---|---|---|---|---|---|
| G (η2p) | T (η2p) | G × T (η2p) | |||||||
| BLC (mmol/L) | E | 1.6 (0.63) | 2 (0.63) | 13.2 (2.41) | 11.8 (2.72) | 10.2 (2.84) | 0.12 (0.014) | 136.18 * (0.945) | 0.55 (0.064) |
| P | 1.9 (0.77) | 2.2 (1.21) | 13 (2.18) | 11.2 (1.91) | 9.6 (2.12) | ||||
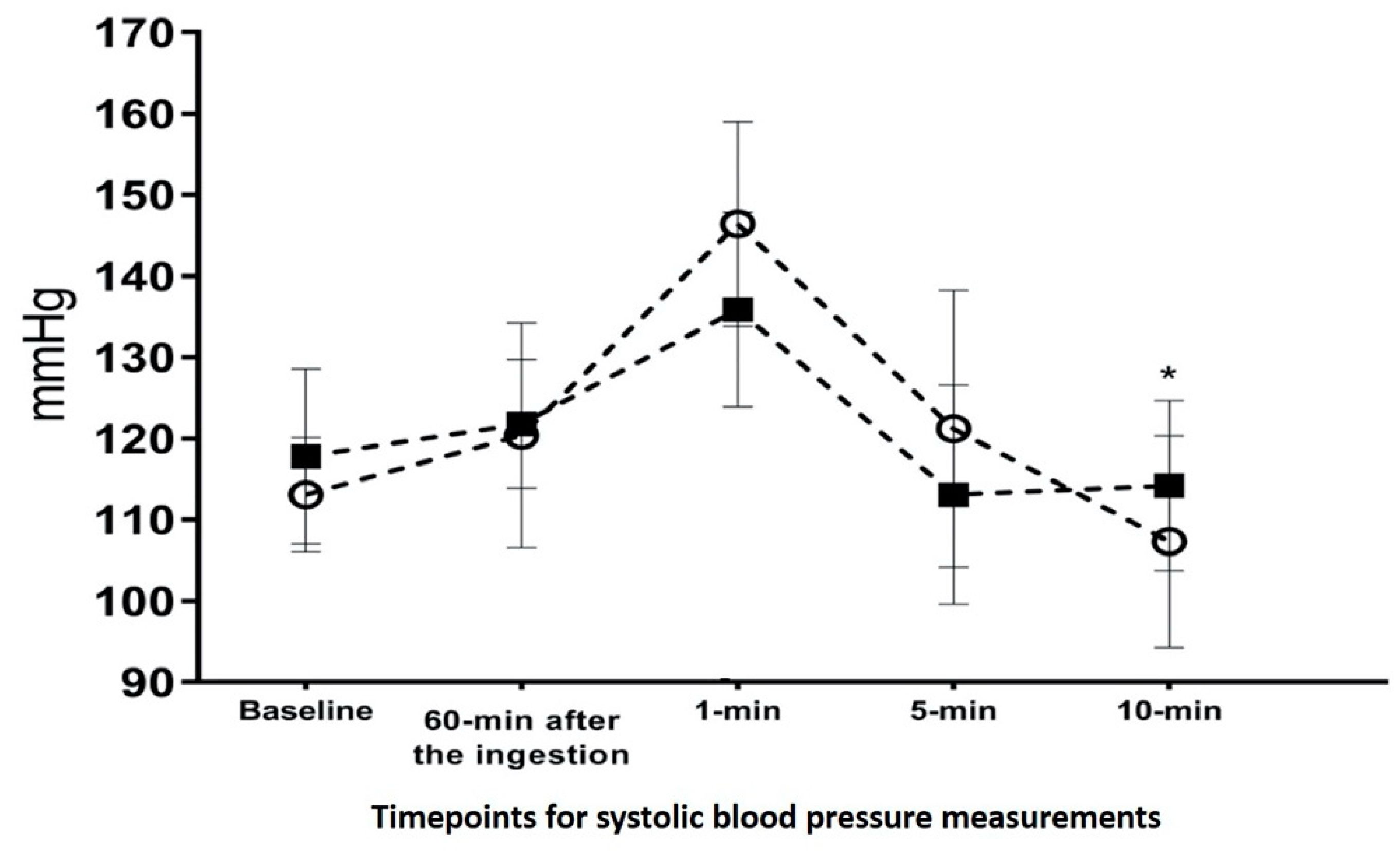
| Systolic (mmHg) | E | 113.1 (7.10) | 120.4 (13.85) | 146.4 (12.61) | 121.2 (17.07) | 107.3 (13.06) | 0.11 (0.039) | 19.97 * (0.796) | 5.04 + (0.326) |
| P | 117.8 (10.77) | 121.8 (13.85) | 135.9 (12.61) | 113.1 (17.07) | 114.2 (13.06) | ||||
| Diastolic (mmHg) | E | 69.2 (8.14) | 72.2 (7.28) | 73.4 (13.22) | 67 (7.45) | 71.6 (11.81) | 0.57 (0.060) | 3.65 * (0.289) | 1.54 (0.146) |
| P | 70.8 (7.54) | 74.9 (5.03) | 71.3 (9.18) | 65.3 (8.43) | 62.6 (9.90) | ||||
| Heart rate (beats/min) | E | 64.3 (15.68) | 86.1 (13.90) | 129.2 (20.74) | 119.2 (14.37) | 112.4 (17.84) | 0.88 (0.089) | 95.38 * (0.914) | 0.72 (0.074) |
| P | 60.4 (11.87) | 88.2 (16.67) | 124.3 (19.27) | 112.7 (15.56) | 108.7 (13.66) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alansare, A.B.; Hayman, J.; Lee, J.-M.; Seo, M.-W.; Yoo, D.; Jung, H.C. The Efficacy of a Calamansi-Containing Energy Drink on Running Performance and Recovery in NCAA Division I Middle-Distance Runners: A Preliminary Study. Int. J. Environ. Res. Public Health 2021, 18, 11023. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111023
Alansare AB, Hayman J, Lee J-M, Seo M-W, Yoo D, Jung HC. The Efficacy of a Calamansi-Containing Energy Drink on Running Performance and Recovery in NCAA Division I Middle-Distance Runners: A Preliminary Study. International Journal of Environmental Research and Public Health. 2021; 18(21):11023. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111023
Chicago/Turabian StyleAlansare, Abdullah B., Josh Hayman, Jung-Min Lee, Myong-Won Seo, Deoksu Yoo, and Hyun Chul Jung. 2021. "The Efficacy of a Calamansi-Containing Energy Drink on Running Performance and Recovery in NCAA Division I Middle-Distance Runners: A Preliminary Study" International Journal of Environmental Research and Public Health 18, no. 21: 11023. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111023