
Development and Pilot Testing of a Smartphone-Based Self-Care Program for Patients with Chronic Hepatitis B


Abstract
:1. Introduction
2. Materials and Methods
2.1. Phase I: Development of a Self-Care Program
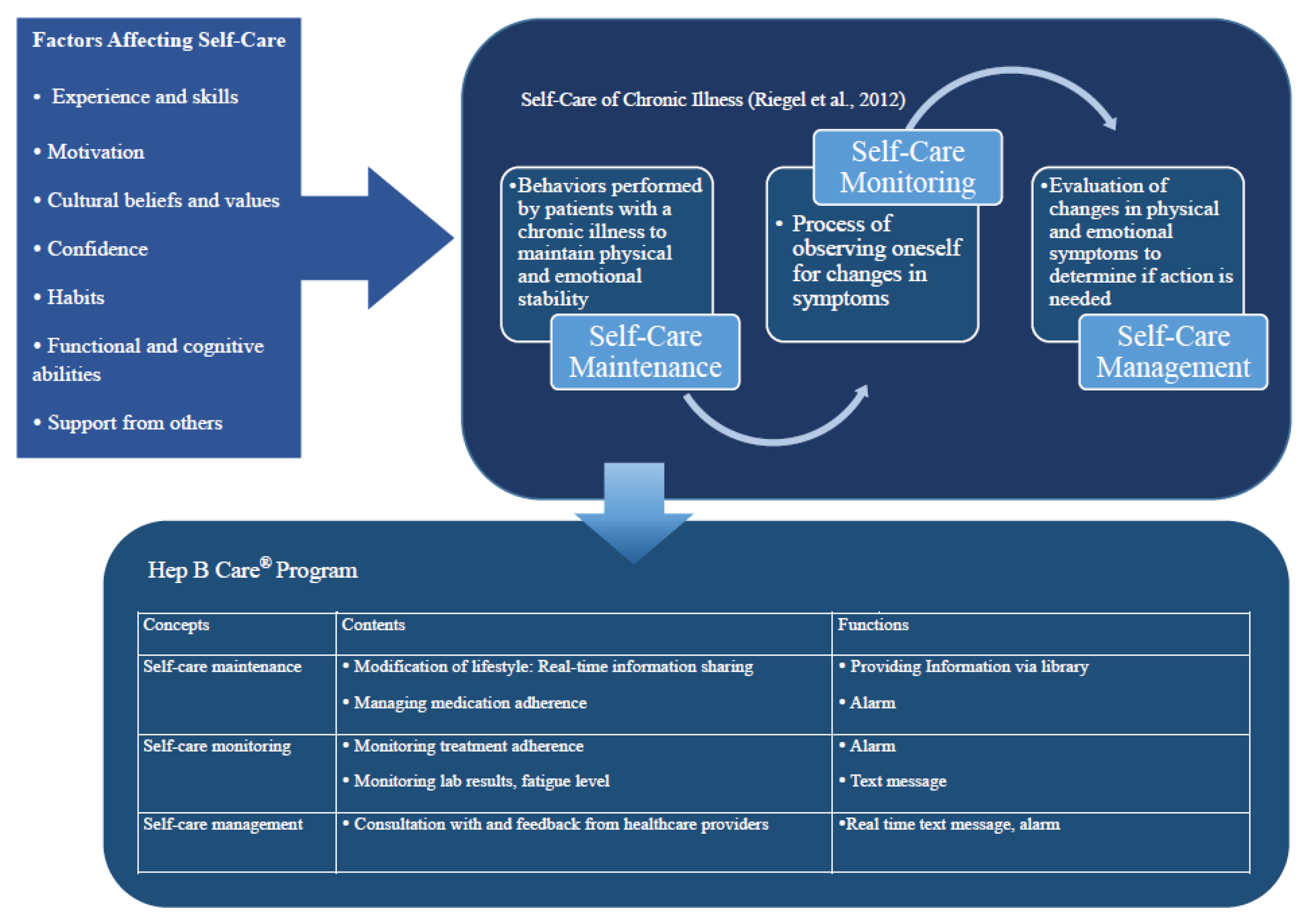
2.1.1. Theoretical Basis for Intervention
2.1.2. Literature Review for the Selection of Intervention Content
2.1.3. Expert Content Review
2.2. Phase II: Self-Care Program Pilot Test
2.2.1. Intervention Protocol: EG Versus CG
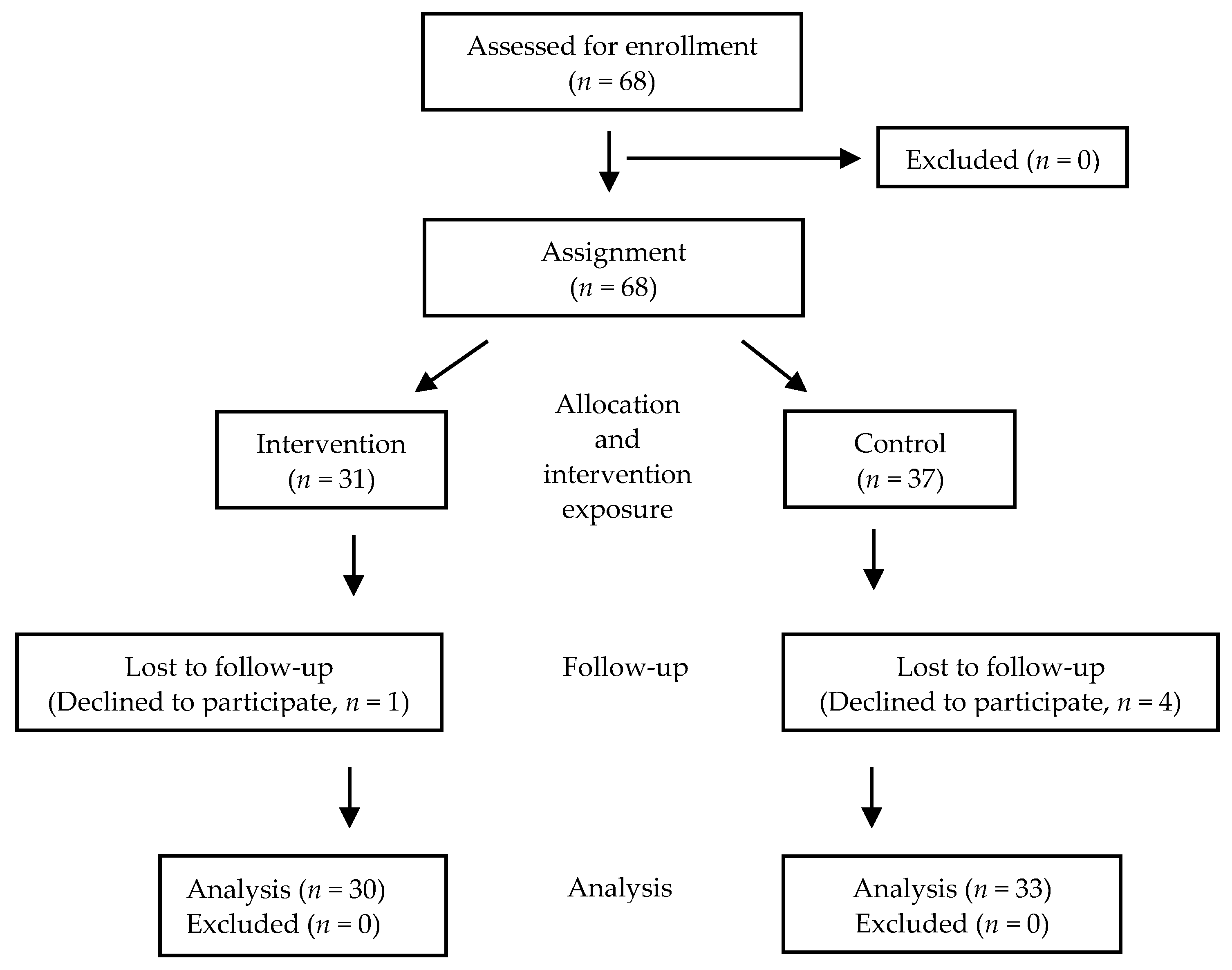
2.2.2. Setting and Sample
2.2.3. Outcome Measurements
2.2.4. Data Collection
2.2.5. Statistical Analyses
2.2.6. Ethical Considerations
3. Results
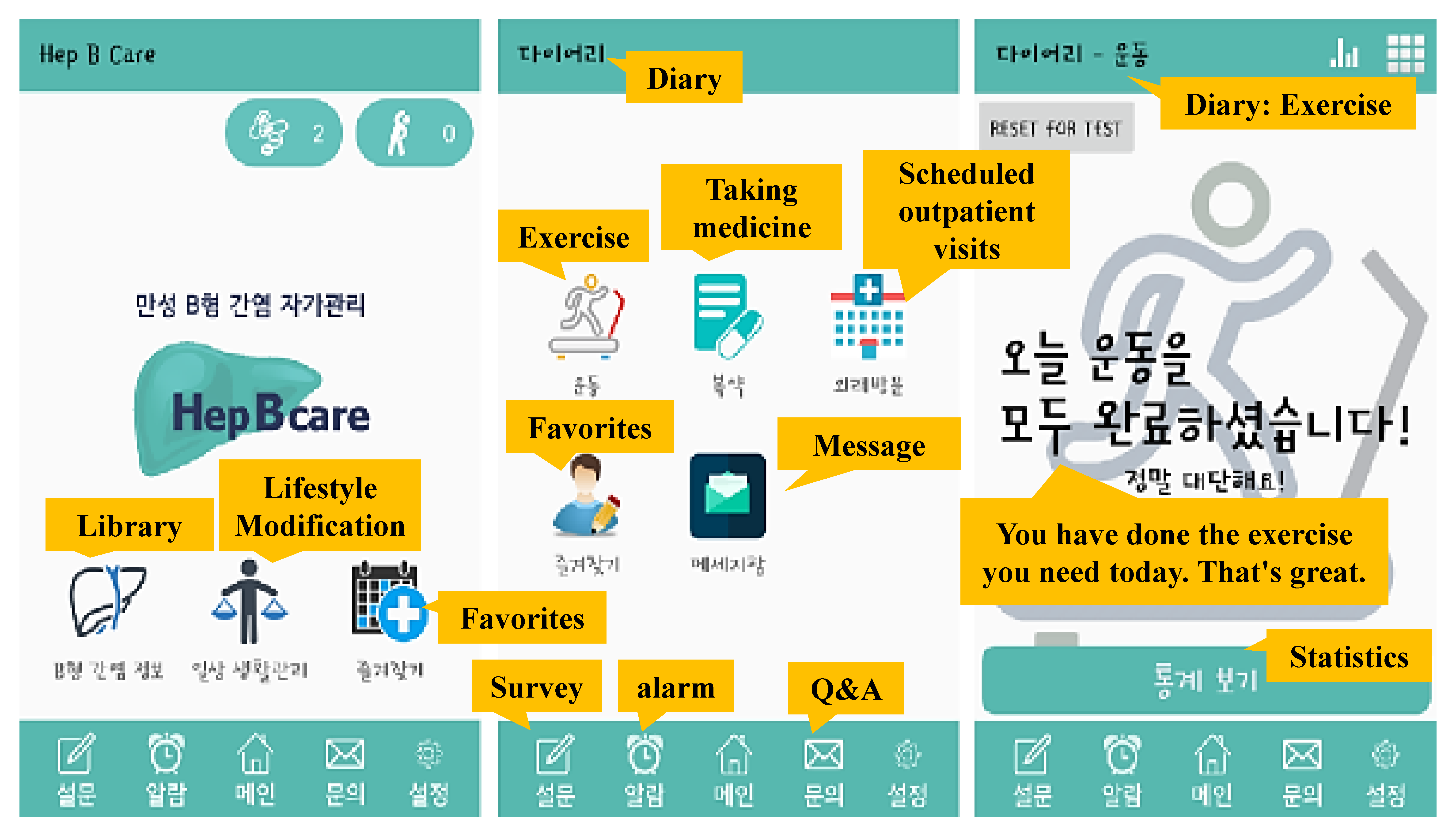
3.1. Part I: Development of Hep B Care®
Content and Functions
3.2. Part II: Pilot Study of Feasibility of the Hep B Care® Program
3.2.1. Results by Measured Outcomes
Cortisol
Knowledge
Fatigue
Depression
Anxiety
Quality of Life (QOL)
Medication Adherence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Hepatitis b. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 6 August 2021).
- Korean Association for the Study of the Liver. Kasl clinical practice guidelines for management of chronic hepatitis b. Clin. Mol. Hepatol. 2019, 25, 93–159. [Google Scholar] [CrossRef] [Green Version]
- Korean Society for The Study of Obesity. 2018 Clinical Practice Guidelines for Overweight and Obesity in Korea; Korea Society for The Study of Obesity: Seoul, Korea, 2018. [Google Scholar]
- Korea Statistical Information Service. Trend in Seroprevalence of Hepatitis b Surface Antigen(hbs ag) in Korea: Sex, 10 Years or Older. Available online: http://kosis.kr/statHtml/statHtml.do?orgId=117&tblId=DT_11702_N109 (accessed on 20 December 2018).
- Seo, I.S.; Song, M.J.; Yoo, Y.S.; Kim, H.S. Comparison for hepatitis b knowledge, self care practice and quality of life according to the disease activity among patients with the hepatitis b virus. J. Korean Public Health Nur. 2017, 31, 257–271. [Google Scholar]
- Cui, Y.; Moriyama, M.; Chayama, K.; Liu, Y.; Ya, C.; Muzembo, B.A.; Rahman, M.M. Efficacy of a self-management program in patients with chronic viral hepatitis in china. BMC Nurs. 2019, 18, 44. [Google Scholar] [CrossRef]
- Hyun, C.S.; Ventura, W.R.; Kim, S.S.; Yoon, S.; Lee, S. A community- based hepatitis b linkage-to-care program: A case study on asian americans chronically infected with hepatitis b virus. Hepatol. Med. Policy 2016, 1, 6. [Google Scholar] [CrossRef] [Green Version]
- Iribarren, S.J.; Cato, K.; Falzon, L.; Stone, P.W. What is the economic evidence for mhealth? A systematic review of economic evaluations of mhealth solutions. PLoS ONE 2017, 12, e0170581. [Google Scholar] [CrossRef] [PubMed]
- McPherson, S.; Wicks, C.; Tercelli, I. Patient experiences of psychological therapy for depression: A qualitative metasynthesis. BMC Psychiatry 2020, 20, 313. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Ming, W.K.; You, J.H. The cost-effectiveness of digital health interventions on the management of cardiovascular diseases: Systematic review. J. Med. Internet Res. 2019, 21, e13166. [Google Scholar] [CrossRef] [PubMed]
- Guerriero, C.; Cairns, J.; Roberts, I.; Rodgers, A.; Whittaker, R.; Free, C. The cost-effectiveness of smoking cessation support delivered by mobile phone text messaging: Txt2stop. Eur. J. Health Econ. 2013, 14, 789–797. [Google Scholar] [CrossRef] [Green Version]
- Dennison, L.; Morrison, L.; Conway, G.; Yardley, L. Opportunities and challenges for smartphone applications in supporting health behavior change: Qualitative study. J. Med. Internet Res. 2013, 15, e86. [Google Scholar] [CrossRef] [PubMed]
- Turner-McGrievy, G.M.; Beets, M.W.; Moore, J.B.; Kaczynski, A.T.; Barr-Anderson, D.J.; Tate, D.F. Comparison of traditional versus mobile app self-monitoring of physical activity and dietary intake among overweight adults participating in an mhealth weight loss program. J. Am. Med. Inform. Assoc. 2013, 20, 513–518. [Google Scholar] [CrossRef]
- Heath, G.; Cooke, R.; Cameron, E. A theory-based approach for developing interventions to change patient behaviours: A medication adherence example from paediatric secondary care. Healthcare 2015, 3, 1228–1242. [Google Scholar] [CrossRef] [Green Version]
- Riegel, B.; Jaarsma, T.; Stromberg, A. A middle-range theory of self-care of chronic illness. ANS Adv. Nurs. Sci. 2012, 35, 194–204. [Google Scholar] [CrossRef] [Green Version]
- Jang, Y.; Kim, J.H.; Lee, H.; Lee, K.; Ahn, S.H. A quantile regression approach to explain the relationship of fatigue and cortisol, cytokine among koreans with hepatitis b. Sci. Rep. 2018, 8, 16434. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Wang, G.; Hsu, F.C.; Xu, J.; Pei, X.; Zhao, B.; Shetty, A. Effects of depression, anxiety, stigma, and disclosure on health-related quality of life among chronic hepatitis b patients in dalian, China. Am. J. Trop. Med. Hyg. 2020, 102, 988–994. [Google Scholar] [CrossRef] [PubMed]
- Orem, D.E. A concept of self-care for the rehabilitation client. Rehabil. Nurs. 1985, 10, 33–36. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. Easl 2017 clinical practice guidelines on the management of hepatitis b virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.H. Development and evaluation of a program to promote self management in patients with chronic hepatitis b. J. Korean Acad. Nurs. 2012, 42, 258–268. [Google Scholar] [CrossRef] [Green Version]
- Jang, Y.; Kim, J.H.; Lee, K. Validation of the revised piper fatigue scale in koreans with chronic hepatitis b. PLoS ONE 2017, 12, e0177690. [Google Scholar] [CrossRef] [Green Version]
- Piper, B.F.; Dibble, S.L.; Dodd, M.J.; Weiss, M.C.; Slaughter, R.E.; Paul, S.M. The revised piper fatigue scale: Psychometric evaluation in women with breast cancer. Oncol. Nurs. Forum 1998, 25, 677–684. [Google Scholar]
- Lee, M.K.; Lee, Y.H.; Park, S.H.; Sohn, C.H.; Jung, Y.J.; Hong, S.K.; Lee, B.G.; Jang, P.; Yun, A. A standardization study of beck depression inventory (i): Korean version (k-bdi): Reliability land factor analysis. J. Psychopathol. 1995, 4, 77–95. [Google Scholar]
- Kwon, S.-M. Differential Roles of Dysfunctional Attitudes and Automatic Thoughts in Depression: An Integrated Cognitive Model of Depression; University of Queensland: St. Lucia, Australia, 1992. [Google Scholar]
- Kwon, S.M.; Oei, T.P. Differential causal roles of dysfunctional attitudes and automatic thoughts in depression. Cognit. Ther. Res. 1992, 16, 309–328. [Google Scholar] [CrossRef]
- Jang, Y.; Ahn, S.H.; Lee, K.; Lee, J.; Kim, J.H. Psychometric evaluation of the korean version of the hepatitis b quality of life questionnaire. PLoS ONE 2019, 14, e0213001. [Google Scholar] [CrossRef] [PubMed]
- Morisky, D.E.; Green, L.W.; Levine, D.M. Concurrent and predictive validity of a self-reported measure of medication adherence. Med. Care 1986, 24, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Robotin, M.; Patton, Y.; George, J. Getting it right: The impact of a continuing medical education program on hepatitis b knowledge of australian primary care providers. Int. J. Gen. Med. 2013, 6, 115–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koman, D. Increasing hepatitis c virus knowledge through an evidence-based educational intervention. Gastroenterol. Nurs. 2018, 41, 95–102. [Google Scholar] [CrossRef]
- Wojcikowski, K.; Kirk, L. Immediate detailed feedback to test-enhanced learning: An effective online educational tool. Med. Teach. 2013, 35, 915–919. [Google Scholar] [CrossRef]
- Schwartz, L.A.; Daniel, L.C.; Henry-Moss, D.; Bonafide, C.P.; Li, Y.; Psihogios, A.M.; Butler, E.S.; Szalda, D.; Ver Hoeve, E.S.; Hobbie, W.L.; et al. Feasibility and acceptability of a pilot tailored text messaging intervention for adolescents and young adults completing cancer treatment. Psychooncology 2020, 29, 164–172. [Google Scholar] [CrossRef]
- Wu, X.; Guo, X.; Zhang, Z. The efficacy of mobile phone apps for lifestyle modification in diabetes: Systematic review and meta-analysis. JMIR Mhealth Uhealth 2019, 7, e12297. [Google Scholar] [CrossRef]
- Gong, E.; Baptista, S.; Russell, A.; Scuffham, P.; Riddell, M.; Speight, J.; Bird, D.; Williams, E.; Lotfaliany, M.; Oldenburg, B. My diabetes coach, a mobile app-based interactive conversational agent to support type 2 diabetes self-management: Randomized effectiveness-implementation trial. J. Med. Internet Res. 2020, 22, e20322. [Google Scholar] [CrossRef]
- World Health Organization. Patient Engagement. Available online: https://apps.who.int/iris/bitstream/handle/10665/252269/9789241511629-eng.pdf;jsessionid=F52633A53EF3C99D0FF6107A9641B70C?sequence=1 (accessed on 20 December 2018).
- Jin, J.; Sklar, G.E.; Oh, V.M.S.; Li, S.C. Factors affecting therapeutic compliance: A review from the patient’s perspective. Ther. Clin. Risk Manag. 2008, 4, 269–286. [Google Scholar]
- Lin, W.S.; Lee, T.T.; Yang, Y.H.; Mills, M.E. Environmental factors affecting self-management of chronic hepatitis b from the patients’ perspective. J. Clin. Nurs. 2019, 28, 4128–4138. [Google Scholar] [CrossRef]
- Thakkar, J.; Kurup, R.; Laba, T.L.; Santo, K.; Thiagalingam, A.; Rodgers, A.; Woodward, M.; Redfern, J.; Chow, C.K. Mobile telephone text messaging for medication adherence in chronic disease: A meta-analysis. JAMA Intern. Med. 2016, 176, 340–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayer, J.E.; Fontelo, P. Meta-analysis on the effect of text message reminders for hiv-related compliance. AIDS Care 2017, 29, 409–417. [Google Scholar] [CrossRef]
- De Bellis, A.; Bellastella, G.; Pernice, V.; Cirillo, P.; Longo, M.; Maio, A.; Scappaticcio, L.; Maiorino, M.I.; Bellastella, A.; Esposito, K.; et al. Hypothalamic-pituitary autoimmunity and related impairment of hormone secretions in chronic fatigue syndrome. J. Clin. Endocrinol. Metab. 2021. [Google Scholar] [CrossRef]
- Fotos, N.V.; Elefsiniotis, I.; Patelarou, A.; Giakoumidakis, K.; Patelarou, E.; Kouros, A.; Brokalaki, H. Psychological disorders and quality of life among patients with chronic viral hepatitis: A single-center cross-sectional study with pair-matched healthy controls. Gastroenterol. Nurs. 2018, 41, 206–218. [Google Scholar] [CrossRef]
- Keskin, G.; Gumus, A.B.; Orgun, F. Quality of life, depression, and anxiety among hepatitis b patients. Gastroenterol. Nurs. 2013, 36, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Lemos, M.F.; Lemos-Neto, S.V.; Barrucand, L.; Verçosa, N.; Tibirica, E. Preoperative education reduces preoperative anxiety in cancer patients undergoing surgery: Usefulness of the self-reported beck anxiety inventory. Braz. J. Anesthesiol. 2019, 69, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Petricone-Westwood, D.; Jones, G.; Mutsaers, B.; Leclair, C.S.; Tomei, C.; Trudel, G.; Dinkel, A.; Lebel, S. A systematic review of interventions for health anxiety presentations across diverse chronic illnesses. Int. J. Behav. Med. 2019, 26, 3–16. [Google Scholar] [CrossRef]
- Abbasi, A.; Ghezeljeh, T.N.; Farahani, M.A. Effect of the self-management education program on the quality of life in people with chronic heart failure: A randomized controlled trial. Electron. Physician 2018, 10, 7028–7037. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Han, J.; Li, Y.; Sun, X.; Lin, P.; Chen, Y.; Gao, F.; Li, Z.; Zhang, S.; Sun, W. Effects of orem’s self-care model on the life quality of elderly patients with hip fractures. Pain Res. Manag. 2020, 2020, 5602683. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.; Song, R.; Choi, S.W. Effects of self-care health behaviors on quality of life mediated by cardiovascular risk factors among individuals with coronary artery disease: A structural equation modeling approach. Asian Nurs. Res. 2016, 10, 158–163. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Experimental (n = 30) | Control (n = 33) | |||||
|---|---|---|---|---|---|---|---|
| Mean ± SD or n (%) | χ2 or t | p | |||||
| Age, years | 55.0 ± 7.35 | 52.3 ± 7.35 | 1.446 | 0.153 | |||
| Sex | Male | 21 | (70.0) | 21 | (63.6) | 0.286 | 0.789 |
| Female | 9 | (30.0) | 12 | (36.4) | |||
| Marital status | Married | 27 | (90.0) | 32 | (97.0) | 1.284 | 0.340 |
| Single or widowed | 3 | (10.0) | 1 | (3.0) | |||
| Occupation | Employed | 15 | (50.0) | 22 | (66.7) | 1.801 | 0.208 |
| Unemployed | 15 | (50.0) | 11 | (33.3) | |||
| Education | ≤High school | 11 | (36.7) | 17 | (51.5) | 1.403 | 0.312 |
| >High school | 19 | (63.3) | 16 | (48.5) | |||
| Household income (Month, KRW) | <2 million | 4 | (13.4) | 3 | (9.1) | 3.507 | 0.676 |
| 2–3 million | 3 | (10.0) | 6 | (18.2) | |||
| 3–4 million | 5 | (16.7) | 3 | (9.1) | |||
| 4–5 million | 7 | (23.2) | 8 | (24.2) | |||
| 5–6 million | 11 | (36.7) | 13 | (39.4) | |||
| Length of diagnosis (months) | 90.8 ± 55.06 | 97.1 ± 84.69 | −0.242 | 0.811 | |||
| Hospitalization | Yes | 6 | (20.0) | 7 | (21.2) | 0.014 | 1.000 |
| No | 24 | (80.0) | 26 | (78.8) | |||
| Family history of HBV | Yes | 23 | (76.7) | 25 | (75.8) | 0.007 | 1.00 |
| No | 7 | (23.3) | 8 | (24.2) | |||
| Comorbidity | Yes | 7 | (23.3) | 10 | (30.3) | 0.387 | 0.581 |
| No | 23 | (76.7) | 23 | (69.7) | |||
| Taking antivirals | Yes | 30 | (100.0) | 33 | (100.0) | ||
| Duration of taking antivirals (months) | 88.6 ± 60.47 | 87.6 ± 48.90 | 0.069 | 0.945 | |||
| HBV DNA | Target not detected | 11 | (36.7) | 9 | (27.3) | 2.350 | 0.329 |
| <20 | 14 | (46.7) | 13 | (39.4) | |||
| ≥20 | 5 | (16.6) | 11 | (33.3) | |||
| AST | 27.3 ± 15.98 | 24.4 ± 9.07 | 0.908 | 0.367 | |||
| ALT | 24.2 ± 13.42 | 26.6 ± 21.9 | −0.526 | 0.601 | |||
| Variables | Experimental Group (n = 30) | Control Group (n = 33) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | ||||||||||
| Mean ± SD | t | (p) | Mean ± SD | t | (p) | ||||||||
| Cortisol | 1.90 | ±0.44 | 2.02 | ±0.44 | −2.19 | (0.037 *) | 1.47 | ±0.62 | 1.35 | ±0.48 | 1.03 | (0.313) | |
| Knowledge | Total | 78.98 | ±11.39 | 83.65 | ±1.49 | −2.81 | (0.009 *) | 74.92 | ±13.66 | 77.39 | ±16.11 | −1.47 | (0.152) |
| GE | 89.29 | ±24.09 | 94.05 | ±13.00 | −1.00 | (0.326) | 87.69 | ±18.19 | 90.91 | ±20.87 | −1.21 | (0.235) | |
| TM | 77.23 | ±18.34 | 85.71 | ±13.91 | −2.75 | (0.011 *) | 74.62 | ±19.13 | 77.27 | ±21.30 | −0.96 | (0.344) | |
| IP | 72.62 | ±19.88 | 75.00 | ±15.38 | −0.61 | (0.547) | 62.12 | ±20.53 | 65.15 | ±23.33 | −0.97 | (0.338) | |
| TR | 89.29 | ±12.74 | 89.29 | ±13.86 | 0 | (1.000) | 85.45 | ±13.48 | 86.06 | ±15.40 | −0.20 | (0.845) | |
| DA | 71.43 | ±16.27 | 77.68 | ±20.79 | −1.57 | (0.129) | 71.97 | ±19.52 | 75.00 | ±22.53 | −0.75 | (0.458) | |
| Fatigue | 4.07 | ±2.50 | 4.09 | ±2.70 | −0.11 | (0.914) | 3.83 | ±2.21 | 3.68 | ±2.00 | 0.78 | (0.442) | |
| Depression | 10.23 | ±10.75 | 9.73 | ±10.66 | 0.44 | (0.663) | 8.36 | ±8.82 | 7.18 | ±6.78 | 1.08 | (0.286) | |
| Anxiety | 30.27 | ±10.04 | 27.90 | ±9.01 | 2.17 | (0.038 *) | 29.24 | ±8.70 | 27.15 | ±4.96 | 1.67 | (0.101) | |
| HBQOL | Total | 63.31 | ±22.60 | 65.43 | ±22.05 | −1.02 | (0.317) | 67.28 | ±21.41 | 66.79 | ±20.23 | 0.25 | (0.807) |
| PW | 76.94 | ±25.38 | 77.69 | ±25.05 | −0.25 | (0.806) | 78.79 | ±24.29 | 79.71 | ±23.69 | −0.45 | (0.658) | |
| AA | 43.06 | ±24.01 | 48.06 | ±28.34 | −1.85 | (0.075) | 48.23 | ±25.79 | 44.57 | ±26.32 | 0.98 | (0.333) | |
| ST | 65.00 | ±28.42 | 65.42 | ±26.74 | −0.16 | (0.874) | 69.82 | ±22.54 | 70.58 | ±23.01 | −0.29 | (0.771) | |
| WN | 78.89 | ±25.31 | 78.89 | ±24.64 | 0 | (1.000) | 80.30 | ±25.41 | 84.60 | ±20.21 | −1.18 | (0.248) | |
| VI | 64.58 | ±26.48 | 70.00 | ±29.43 | −1.58 | (0.125) | 68.18 | ±24.67 | 66.86 | ±22.34 | 0.46 | (0.652) | |
| VU | 42.22 | ±24.07 | 43.89 | ±26.98 | −0.46 | (0.651) | 51.52 | ±29.86 | 46.97 | ±27.31 | 0.92 | (0.363) | |
| Medication adherence | 1.20 | ± 1.10 | 1.17 | ±1.05 | 0.25 | (0.801) | 1.52 | ±1.12 | 1.24 | ±1.03 | 1.39 | (0.174) | |
| Variables | Range | Experimental (n = 30) | Control (n = 33) | F (p) | ||
|---|---|---|---|---|---|---|
| Pre-Post | Pre-Post | |||||
| LS Mean ± SE | ||||||
| Cortisol | 1.85 ± 0.08 | 1.39 ± 0.07 | 1.68 | (0.200) | ||
| Knowledge | Total | 0–100 | 82.68 ± 1.61 | 79.15 ± 1.47 | 9.15 | (0.004 *) |
| GE | 0–100 | 93.96 ± 2.68 | 91.50 ± 2.47 | 16.09 | (<0.001 *) | |
| TM | 0–100 | 85.16 ± 2.67 | 78.20 ± 2.46 | 5.51 | (0.022 *) | |
| IP | 0–100 | 73.52 ± 3.21 | 68.84 ± 2.92 | 6.59 | (0.013 *) | |
| TR | 0–100 | 87.97 ± 2.60 | 86.58 ± 2.38 | 1.39 | (0.243) | |
| DA | 0–100 | 77.82 ± 3.86 | 74.89 ± 3.55 | 0.008 | (0.931) | |
| Fatigue | 0–10 | 3.98 ± 0.22 | 3.77 ± 0.21 | 0.43 | (0.514) | |
| Depression | 0–63 | 8.93 ± 0.99 | 7.67 ± 0.95 | 0.49 | (0.487) | |
| Anxiety | 0–63 | 27.51 ± 0.87 | 27.31 ± 0.83 | 8.18 | (0.006 *) | |
| HBQOL | Total | 0–100 | 67.20 ± 2.00 | 65.27 ± 1.91 | 0.01 | (0.919) |
| PW | 0–100 | 78.44 ± 2.50 | 78.96 ± 2.38 | 0.22 | (0.640) | |
| AA | 0–100 | 50.78 ± 3.28 | 42.90 ± 3.12 | 0.57 | (0.452) | |
| ST | 0–100 | 67.48 ± 2.56 | 68.73 ± 2.45 | 0.43 | (0.836) | |
| WN | 0–100 | 79.42 ± 3.06 | 84.28 ± 2.92 | 2.80 | (0.100) | |
| VI | 0–100 | 71.63 ± 3.09 | 65.69 ± 2.95 | 0.29 | (0.594) | |
| VU | 0–100 | 47.70 ± 4.09 | 44.89 ± 3.86 | 1.13 | (0.292) | |
| Medication adherence | 1–4 | 1.29 ± 0.15 | 1.18 ± 0.14 | 1.04 | (0.312) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, Y.; Ahn, S.H.; Lee, K.; Kwon, O.Y.; Kim, J.H. Development and Pilot Testing of a Smartphone-Based Self-Care Program for Patients with Chronic Hepatitis B. Int. J. Environ. Res. Public Health 2021, 18, 11139. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111139
Jang Y, Ahn SH, Lee K, Kwon OY, Kim JH. Development and Pilot Testing of a Smartphone-Based Self-Care Program for Patients with Chronic Hepatitis B. International Journal of Environmental Research and Public Health. 2021; 18(21):11139. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111139
Chicago/Turabian StyleJang, Yeonsoo, Sang Hoon Ahn, Kyunghwa Lee, Oh Young Kwon, and Jeong Hyun Kim. 2021. "Development and Pilot Testing of a Smartphone-Based Self-Care Program for Patients with Chronic Hepatitis B" International Journal of Environmental Research and Public Health 18, no. 21: 11139. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111139