
Racism and Cancer Screening among Low-Income, African American Women: A Multilevel, Longitudinal Analysis of 2-1-1 Texas Callers

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Conceptual Framework
2.3. Study Setting and Participants
2.4. Data Collection
2.4.1. Cancer Screening Outcome
2.4.2. Indicators of Racism
Perceived Racial Discrimination
Racial Residential Segregation
2.4.3. Covariates
2.5. Data Analysis
3. Results
3.1. Descriptive Statistics
3.2. Perceived Racial Discrimination and Cancer Screening
3.3. Racial Residential Segregation and Cancer Screening
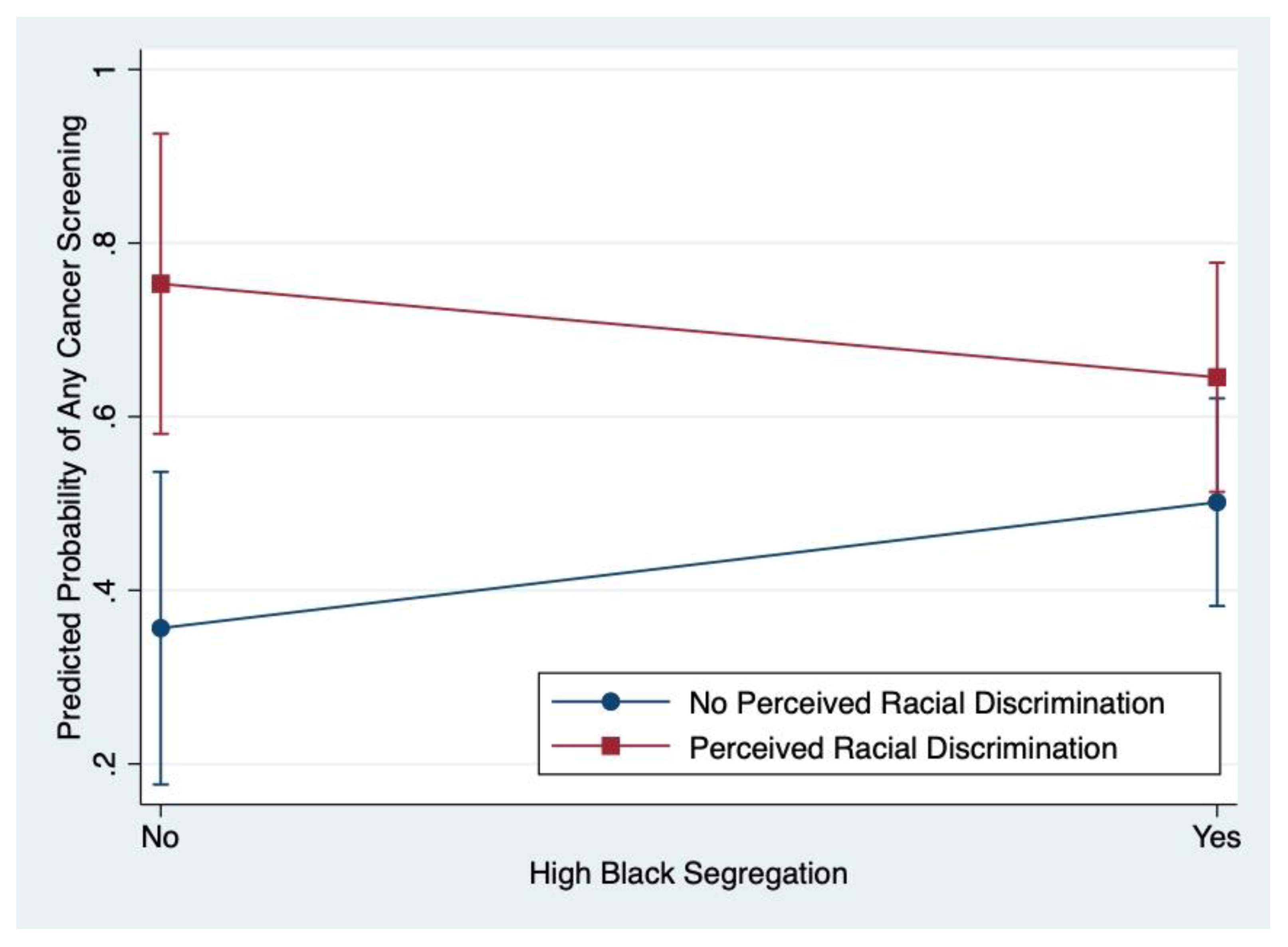
3.4. Modifying Effect of Perceived Racial Discrimination on Racial Residential Segregation and Cancer Screening
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Cancer Society. Cancer Prevention & Early Detection Facts & Figures 2019–2020; American Cancer Society: Atlanta, GA, USA, 2019. [Google Scholar]
- National Cancer Institute. Cancer Disparities. Available online: https://www.cancer.gov/about-cancer/understanding/disparities (accessed on 2 May 2020).
- Aizer, A.A.; Wilhite, T.J.; Chen, M.-H.; Graham, P.L.; Choueiri, T.K.; Hoffman, K.E.; Martin, N.E.; Trinh, Q.-D.; Hu, J.C.; Nguyen, P.L. Lack of reduction in racial disparities in cancer-specific mortality over a 20-year period. Cancer 2014, 120, 1532–1539. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.; Wen, W.; Morgans, A.K.; Pao, W.; Shu, X.-O.; Zheng, W. Disparities by Race, Age, and Sex in the Improvement of Survival for Major Cancers: Results From the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) Program in the United States, 1990 to 2010. JAMA Oncol. 2015, 1, 88–96. [Google Scholar] [CrossRef]
- U.S. Cancer Statistics Working Group. U.S. Cancer Statistics Data Visualizations Tool, based on November 2018 submission data (1999–2016). Available online: www.cdc.gov/cancer/dataviz (accessed on 3 February 2020).
- American Cancer Society. Cancer Facts & Figures for African Americans 2019–2021; American Cancer Society: Atlanta, GA, USA, 2019. [Google Scholar]
- Debarros, M.; Steele, S.R. Colorectal cancer screening in an equal access healthcare system. J Cancer 2013, 4, 270–280. [Google Scholar] [CrossRef]
- Center for Health Statistics. Texas Behavioral Risk Factor Surveillance System. 2016. Available online: http://healthdata.dshs.texas.gov/CommunitySurveys/BRFSS (accessed on 3 February 2020).
- Bambhroliya, A.B.; Burau, K.D.; Sexton, K. Spatial Analysis of County-Level Breast Cancer Mortality in Texas. J. Environ. Public Health 2012, 2012, 959343. [Google Scholar] [CrossRef] [Green Version]
- Haddock, N. Clinic Capacity and Spatial Access to Preventive Breast Health Services for Underserved Survivors across Texas. Ph.D. Dissertation, The University of Texas School of Public Health, Houston, TX, USA, 2014. [Google Scholar]
- Highfield, L. Spatial Patterns of Breast Cancer Incidence and Uninsured Women of Mammography Screening Age. Breast J. 2013, 19, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Office of Disease Prevention & Health Promotion. Healthy People 2020: Cancer Objective C-15 Increase the Proportion of Women Who Receive a Cervical Cancer Screening Based on the Most Recent Guidelines. Available online: https://www.healthypeople.gov/2020/data-search/Search-the-Data#objid=4053; (accessed on 3 February 2020).
- U.S. Preventive Services Task Force. Screening for Breast Cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2016, 164, 279–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Office of Disease Prevention & Health Promotion. Healthy People 2020: Cancer Objective C-16 Increase the Proportion of Adults Who Receive a Colorectal Cancer Screening Based on the Most Recent Guidelines. Available online: https://www.healthypeople.gov/2020/data-search/Search-the-Data#objid=4054; (accessed on 3 February 2020).
- Healthy People 2020. Discrimination. Available online: https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-health/interventions-resources/discrimination#1 (accessed on 30 January 2019).
- Lorch, S.A.; Enlow, E. The role of social determinants in explaining racial/ethnic disparities in perinatal outcomes. Pediatr. Res. 2015, 79, 141. [Google Scholar] [CrossRef]
- Paradies, Y.; Ben, J.; Denson, N.; Elias, A.; Priest, N.; Pieterse, A.; Gupta, A.; Kelaher, M.; Gee, G. Racism as a Determinant of Health: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0138511. [Google Scholar] [CrossRef] [Green Version]
- Pascoe, E.A.; Smart Richman, L. Perceived discrimination and health: A meta-analytic review. Psychol. Bull. 2009, 135, 531–554. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, M.T.; Branscombe, N.R.; Postmes, T.; Garcia, A. The consequences of perceived discrimination for psychological well-being: A meta-analytic review. Psychol. Bull. 2014, 140, 921. [Google Scholar] [CrossRef]
- Shavers, V.L.; Fagan, P.; Jones, D.; Klein, W.M.P.; Boyington, J.; Moten, C.; Rorie, E. The State of Research on Racial/Ethnic Discrimination in The Receipt of Health Care. Am. J. Public Health 2012, 102, 953–966. [Google Scholar] [CrossRef] [Green Version]
- Walker, R.J.; Strom Williams, J.; Egede, L.E. Influence of Race, Ethnicity and Social Determinants of Health on Diabetes Outcomes. Am. J. Med Sci. 2016, 351, 366–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, D.R.; Lawrence, J.A.; Davis, B.A. Racism and Health: Evidence and Needed Research. Annu. Rev. Public Health 2019, 40, 102–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, D.R.; Collins, C. Racial Residential Segregation: A Fundamental Cause of Racial Disparities in Health. Public Health Rep. 2001, 116, 404–416. [Google Scholar] [CrossRef]
- Williams, D.R.; Sternthal, M. Understanding Racial-ethnic Disparities in Health: Sociological Contributions. J. Health Soc. Behav. 2010, 51, S15–S27. [Google Scholar] [CrossRef] [PubMed]
- Gee, G.C.; Ford, C.L. Structural Racism and Health Inequities: Old Issues, New Directions. Du Bois Rev. Soc. Sci. Res. Race 2011, 8, 115–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawley, L.M.; Ahn, D.K.; Winkleby, M.A. Perceived Medical Discrimination and Cancer Screening Behaviors of Racial and Ethnic Minority Adults. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1937–1944. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, E.A.; Rathouz, P.J.; Karavolos, K.; Everson-Rose, S.A.; Janssen, I.; Kravitz, H.M.; Lewis, T.T.; Powell, L.H. Perceived Discrimination Is Associated with Reduced Breast and Cervical Cancer Screening: The Study of Women’s Health Across the Nation (SWAN). J. Womens Health 2014, 23, 138–145. [Google Scholar] [CrossRef]
- Facione, N.C.; Facione, P.A. Perceived Prejudice in Healthcare and Women’s Health Protective Behavior. Nurs. Res. 2007, 56, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Hoyo, C.; Yarnall, K.S.H.; Skinner, C.S.; Moorman, P.G.; Sellers, D.; Reid, L. Pain predicts non-adherence to pap smear screening among middle-aged African American women. Prev. Med. 2005, 41, 439–445. [Google Scholar] [CrossRef]
- Mouton, C.P.; Carter-Nolan, P.L.; Makambi, K.H.; Taylor, T.R.; Palmer, J.R.; Rosenberg, L.; Adams-Campbell, L.L. Impact of perceived racial discrimination on health screening in black women. J. Health Care Poor Underserved 2010, 21, 287–300. [Google Scholar] [CrossRef]
- Benjamins, M.R. Race/Ethnic Discrimination and Preventive Service Utilization in a Sample of Whites, Blacks, Mexicans, and Puerto Ricans. Med. Care 2012, 50, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Hausmann, L.R.M.; Jeong, K.; Bost, J.E.; Ibrahim, S.A. Perceived Discrimination in Health Care and Use of Preventive Health Services. J. Gen. Intern. Med. 2008, 23, 1679–1684. [Google Scholar] [CrossRef] [Green Version]
- Shariff-Marco, S.; Klassen, A.C.; Bowie, J.V. Racial/ethnic differences in self-reported racism and its association with cancer-related health behaviors. Am. J. Public Health 2010, 100, 364–374. [Google Scholar] [CrossRef] [PubMed]
- Fowler-Brown, A.; Ashkin, E.; Corbie-Smith, G.; Thaker, S.; Pathman, D.E. Perception of racial barriers to health care in the rural South. J. Health Care Poor Underserved 2006, 17, 86–100. [Google Scholar] [CrossRef]
- Dailey, A.B.; Kasl, S.V.; Holford, T.R.; Jones, B.A. Perceived Racial Discrimination and Nonadherence to Screening Mammography Guidelines: Results from the Race Differences in the Screening Mammography Process Study. Am. J. Epidemiol. 2007, 165, 1287–1295. [Google Scholar] [CrossRef] [PubMed]
- Grollman, E.A.; Hagiwara, N. Measuring Self-Reported Discrimination: Trends in Question Wording Used in Publicly Accessible Datasets. Soc. Curr. 2017, 4, 287–305. [Google Scholar] [CrossRef]
- Kressin, N.R.; Raymond, K.L.; Manze, M. Perceptions of race/ethnicity-based discrimination: A review of measures and evaluation of their usefulness for the health care setting. J. Health Care Poor Underserved 2008, 19, 697–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krieger, N.; Smith, K.; Naishadham, D.; Hartman, C.; Barbeau, E.M. Experiences of discrimination: Validity and reliability of a self-report measure for population health research on racism and health. Soc. Sci. Med. 2005, 61, 1576–1596. [Google Scholar] [CrossRef] [Green Version]
- Thoits, P.A. Stress and Health: Major Findings and Policy Implications. J. Health Soc. Behav. 2010, 51, S41–S53. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.R.; Mohammed, S.A. Discrimination and racial disparities in health: Evidence and needed research. J. Behav. Med. 2009, 32, 20–47. [Google Scholar] [CrossRef] [Green Version]
- Kramer, M.R.; Hogue, C.R. Is Segregation Bad for Your Health? Epidemiol. Rev. 2009, 31, 178–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, K.; Borrell, L.N. Racial/ethnic residential segregation: Framing the context of health risk and health disparities. Health Place 2011, 17, 438–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mobley, L.R.; Subramanian, S.; Tangka, F.K.; Hoover, S.; Wang, J.; Hall, I.J.; Singh, S.D. Breast Cancer Screening Among Women with Medicaid, 2006–2008: A Multilevel Analysis. J. Racial Ethn. Health Disparities 2017, 4, 446–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buehler, J.W.; Castro, J.C.; Cohen, S.; Zhao, Y.; Melly, S.; Moore, K. Personal and Neighborhood Attributes Associated with Cervical and Colorectal Cancer Screening in an Urban African American Population. Prev. Chronic Dis. 2019, 16, E118. [Google Scholar] [CrossRef] [Green Version]
- Mobley, L.R.; Kuo, T.-M.; Driscoll, D.; Clayton, L.; Anselin, L. Heterogeneity in mammography use across the nation: Separating evidence of disparities from the disproportionate effects of geography. Int. J. of Health Geogr. 2008, 7, 32. [Google Scholar] [CrossRef] [Green Version]
- Borrell, L.N.; Kiefe, C.I.; Diez-Roux, A.V.; Williams, D.R.; Gordon-Larsen, P. Racial discrimination, racial/ethnic segregation, and health behaviors in the CARDIA study. Ethn. Health 2013, 18, 227–243. [Google Scholar] [CrossRef] [Green Version]
- Hunt, M.O.; Wise, L.A.; Jipguep, M.-C.; Cozier, Y.C.; Rosenberg, L. Neighborhood Racial Composition and Perceptions of Racial Discrimination: Evidence From the Black Women’s Health Study. Soc. Psychol. Q. 2007, 70, 272–289. [Google Scholar] [CrossRef] [Green Version]
- Ford, C.L.; Airhihenbuwa, C.O. The public health critical race methodology: Praxis for antiracism research. Soc. Sci. Med. 2010, 71, 1390–1398. [Google Scholar] [CrossRef]
- Andersen, R.M. Revisiting the Behavioral Model and Access to Medical Care: Does it Matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef]
- Patrick, D.L.; Stein, J.; Porta, M.; Porter, C.Q.; Ricketts, T.C. Poverty, Health Services, and Health Status in Rural America. Milbank Q. 1988, 66, 105–136. [Google Scholar] [CrossRef] [Green Version]
- Phillips, K.A.; Morrison, K.R.; Andersen, R.; Aday, L.A. Understanding the context of healthcare utilization: Assessing environmental and provider-related variables in the behavioral model of utilization. Health Serv. Res. 1998, 33, 571–596. [Google Scholar]
- Thrasher, A.D.; Clay, O.J.; Ford, C.L.; Stewart, A.L. Theory-Guided Selection of Discrimination Measures for Racial/ Ethnic Health Disparities Research Among Older Adults. J. Aging Health 2012, 24, 1018–1043. [Google Scholar] [CrossRef] [PubMed]
- Ford, C.L.; Daniel, M.; Earp, J.A.L.; Kaufman, J.S.; Golin, C.E.; Miller, W.C. Perceived Everyday Racism, Residential Segregation, and HIV Testing Among Patients at a Sexually Transmitted Disease Clinic. Am. J. Public Health 2009, 99, S137–S143. [Google Scholar] [CrossRef]
- Fernandez, M.E.; Savas, L.S.; Atkinson, J.S.; Ricks, K.B.; Ibekwe, L.N.; Jackson, I.; Castle, P.E.; Jobe, D.; Vernon, S.W. Evaluation of a 2-1-1 Telephone Navigation Program to Increase Cancer Control Behaviors: Results from a Randomized Controlled Trial. Am. J. Health Promot. In press.
- Enders, C.K. Applied Missing Data Analysis; Guilford Press: New York, NY, USA, 2020. [Google Scholar]
- American Cancer Society. History of ACS Recommendations for the Early Detection of Cancer in People Without Symptoms. Available online: https://www.cancer.org/health-care-professionals/american-cancer-society-prevention-early-detection-guidelines/overview/chronological-history-of-acs-recommendations.html (accessed on 3 June 2021).
- U.S. Census Bureau. 2015 American Community Survey 5-Year (2011–2015) Estimates Data Profiles: Table DP05: Non-Hispanic Black or African American Alone/Total Population. Available online: https://data.census.gov/cedsci/table?q=race%20and%20ethnicity&tid=ACSDP5Y2015.DP05&hidePreview=true (accessed on 20 July 2021).
- U.S. Census Bureau. 2015 American Community Survey 5-Year (2011–2015) Estimates Subject Tables, Table S1701: Population for Whom Poverty Status Is Determined. Available online: https://data.census.gov/cedsci/table?q=poverty&tid=ACSST5Y2015.S1701&hidePreview=true (accessed on 20 July 2021).
- U.S. Census Bureau. 2015 American Community Survey 5-Year (2011–2015) Estimates Subject Tables, Table S1501: Population 25 Years and Over with High School Graduate/Bachelor’s Degree. Available online: https://data.census.gov/cedsci/table?q=education&tid=ACSST5Y2015.S1501&hidePreview=true (accessed on 20 July 2021).
- Boustan, L.P. Racial Residential Segregation in American Cities; National Bureau of Economic Research: Cambridge, MA, USA, 2013. [Google Scholar]
- Ihlanfeldt, K.R.; Scafidi, B. Black Self-Segregation as a Cause of Housing Segregation: Evidence from the Multi-City Study of Urban Inequality. J. Urban Econ. 2002, 51, 366–390. [Google Scholar] [CrossRef]
- Krysan, M.; Farley, R. The Residential Preferences of Blacks: Do They Explain Persistent Segregation? Soc. Forces 2002, 80, 937–980. [Google Scholar] [CrossRef]
- Sudano, J.J.; Perzynski, A.; Wong, D.W.; Colabianchi, N.; Litaker, D. Neighborhood racial residential segregation and changes in health or death among older adults. Health Place 2013, 19, 80–88. [Google Scholar] [CrossRef] [Green Version]
- Pruitt, S.L.; Lee, S.J.C.; Tiro, J.A.; Xuan, L.; Ruiz, J.M.; Inrig, S. Residential racial segregation and mortality among black, white, and Hispanic urban breast cancer patients in Texas, 1995 to 2009. Cancer 2015, 121, 1845–1855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutler, D.M.; Glaeser, E.L.; Vigdor, J.L. The Rise and Decline of the American Ghetto. J. Political Econ. 1999, 107, 455–506. [Google Scholar] [CrossRef]
- Brown, L.A.; Chung, S.-Y. Spatial segregation, segregation indices and the geographical perspective. Popul. Space Place 2006, 12, 125–143. [Google Scholar] [CrossRef]
- Schafer, J.L. Multiple imputation: A primer. Stat. Methods Med Res. 1999, 8, 3–15. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis: A Global Perspective, 7th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2009; p. 816. [Google Scholar]
- Liang, K.Y.; Zeger, S.L. Regression Analysis for Correlated Data. Annu. Rev. Public Health 1993, 14, 43–68. [Google Scholar] [CrossRef]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- StataCorp. Stata Statistical Software; Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- Selvin, S. Statistical Analysis of Epidemiologic Data; Oxford University Press: Oxford, UK, 2004. [Google Scholar]
- Arnett, M.J.; Thorpe, R.J., Jr.; Gaskin, D.J.; Bowie, J.V.; LaVeist, T.A. Race, Medical Mistrust, and Segregation in Primary Care as Usual Source of Care: Findings from the Exploring Health Disparities in Integrated Communities Study. J. Urban Health 2016, 93, 456–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, K.; Haas, J.S.; Williams, D.R. Elucidating the Role of Place in Health Care Disparities: The Example of Racial/Ethnic Residential Segregation. Health Serv. Res. 2012, 47, 1278–1299. [Google Scholar] [CrossRef] [PubMed]
- Bediako, S.M.; Kwate, N.O.A.; Rucker, R. Dietary behavior among African Americans: Assessing cultural identity and health consciousness. Ethn. Dis. 2004, 14, 527–532. [Google Scholar] [PubMed]
- Nevarez, L.; Hovick, S.R.; Enard, K.R.; Lloyd, S.M.; Kahlor, L.A. Race/Ethnic Variations in Predictors of Health Consciousness Within the Cancer Prevention Context. Am. J. Health Promot. 2020, 34, 740–746. [Google Scholar] [CrossRef]
- Ford, C.L.; Airhihenbuwa, C.O. Critical Race Theory, Race Equity, and Public Health: Toward Antiracism Praxis. Am. J. Public Health 2010, 100, S30–S35. [Google Scholar] [CrossRef]
- Wong, D.W.S. Modeling Local Segregation: A Spatial Interaction Approach. Geogr. Environ. Model. 2002, 6, 81–97. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| INDIVIDUAL-LEVEL CHARACTERISTICS | |||||
|---|---|---|---|---|---|
| Total Sample | Perceived Racial Discrimination 1 | Racial Residential Segregation 1 | |||
| No (n = 82) | Yes (n = 67) | No (n = 48) | Yes (n = 101) | ||
| Age (years), mean (SD) | 48.1 (11.4) | 49 (10.1) | 47.0 (12.8) | 49.1 (9.1) | 47.7 (12.3) |
| p = 0.2978 | p = 0.4779 | ||||
| Marital Status, n (%) | |||||
| Not Married | 132 (89.2) | 73 (89.0) | 59 (89.4) | 43 (89.6) | 89 (89.0) |
| Married or Living with a Someone | 16 (10.8) | 9 (11.0) | 7 (10.6) | 5 (10.4) | 11 (11.0) |
| p = 0.943 | p = 0.915 | ||||
| Education, n (%) | |||||
| Less than High School | 21 (14.1) | 12 (14.6) | 9 (13.4) | 8 (16.7) | 13 (12.9) |
| High School or GED | 56 (37.6) | 32 (39.0) | 24 (35.8) | 17 (35.4) | 39 (38.6) |
| Post High School 2 | 72 (48.3) | 38 (46.3) | 34 (50.8) | 23 (47.9) | 49 (48.5) |
| p = 0.867 | p = 0.809 | ||||
| Annual Household Income, n (%) | |||||
| None–USD 9999 | 61 (40.9) | 37 (45.1) | 24 (35.8) | 23 (47.9) | 38 (37.6) |
| USD 10,000–USD 19,999 | 53 (35.6) | 25 (30.5) | 28 (41.8) | 16 (33.3) | 37 (36.6) |
| USD 20,000 or more | 35 (23.5) | 20 (24.4) | 15 (22.4) | 9 (18.8) | 26 (25.7) |
| p = 0.338 | p = 0.445 | ||||
| Health Insurance Status, n (%) | |||||
| No Insurance (or CHIP only) | 64 (43.0) | 35 (42.7) | 29 (43.3) | 20 (41.7) | 44 (43.6) |
| Public and/or Private Insurance | 85 (57.1) | 47 (57.3) | 38 (56.7) | 28 (58.3) | 57 (56.4) |
| p = 0.941 | p = 0.827 | ||||
| Number of Cancer Screenings Needed, mean (SD) | 1.6 (0.7) | 1.7 (0.73) | 1.6 (0.72) | 1.9 (0.8) | 1.5 (0.7) |
| p = 0.3368 | p = 0.0045 ** | ||||
| Social Support | |||||
| Functional Social Support Scale Score, mean (SD) | 22.8 (5.8) | 23.1 (5.9) | 22.5 (5.7) | 23.3 (5.4) | 22.6 (6.0) |
| p = 0.5221 | p = 0.5003 | ||||
| Levels of Perceived Functional Social Support, n (%) | |||||
| Low | 30 (28.3) | 22 (26.8) | 18 (26.9) | 10 (28.6) | 20 (28.2) |
| Moderate/High | 76 (71.7) | 60 (73.2) | 49 (73.1) | 25 (71.4) | 51 (71.8) |
| p = 0.996 | p = 0.965 | ||||
| Perceived Racial Discrimination | |||||
| Reported Experiences of Racial Discrimination, n (%) | |||||
| No | 82 (55.0) | - | - | 21 (43.8) | 61 (60.4) |
| Yes | 67 (45.0) | - | - | 27 (56.3) | 40 (39.6) |
| - | p = 0.056 † | ||||
| Number of Situations Reported in the Last 5 Years, mean (SD) | 1.6 (2.2) | - | - | 2.0 (2.3) | 1.5 (2.1) |
| - | p = 0.1875 † | ||||
| NEIGHBORHOOD-LEVEL CHARACTERISTICS | |||||
| Educational Attainment | |||||
| Percent Neighborhood with High School/GED 3, mean (SD) | 29.0 (8.7) | 28.4 (8.7) | 29.8 (8.7) | 25.8 (8.9) | 30.6 (8.2) |
| p = 0.3310 | p = 0.0016 ** | ||||
| Percent Neighborhood with Bachelor’s Degree 4, mean (SD) | 12.1 (9.2) | 11.7 (8.1) | 12.6 (10.3) | 13.3 (12.4) | 11.5 (7.1) |
| p = 0.5255 | p = 0.2522 | ||||
| Percent Neighborhood Below Federal Poverty Line, mean (SD) | 25.2 (11.9) | 25.4 (11.6) | 24.8 (12.3) | 25.0 (14.2) | 25.2 (10.7) |
| p = 0.7457 | p = 0.9229 | ||||
| Racial Residential Segregation | |||||
| Location Quotient (unitless), mean (SD) | 2.3 (1.5) | 2.6 (1.6) | 2.0 (1.4) | - | - |
| p = 0.0195 * | - | ||||
| Participants Living in High Black Segregated Neighborhood, n (%) | |||||
| No | 48 (32.2) | 21 (25.6) | 27 (40.3) | - | - |
| Yes | 101 (67.8) | 61 (74.4) | 40 (59.7) | - | - |
| p = 0.056 † | - | ||||
| Situtation Types | Total Sample n (%) |
|---|---|
| When gettting service in a store or restaurant | 48 (71.6) |
| While at work | 38 (56.7) |
| When getting hired or getting a job | 31 (46.3) |
| While on the street or in a public setting | 30 (44.8) |
| From the police or in the courts | 27 (40.3) |
| When getting credit, bank loans, or a mortgage (n = 48) | 17 (35.4) |
| In accessing or while getting medical care | 23 (34.3) |
| When getting housing | 19 (29.2) |
| While at school | 10 (14.9) |
| Total Sample | |
|---|---|
| Did Not Complete Any Needed Screening, n (%) | 65 (43.6) |
| Completed at Least One Needed Screening, n (%) | 84 (56.4) |
| Number of Cancer Screenings Completed, mean (SD) | 0.80 (0.87) |
| Unadjusted Bivariate Models | Adjusted Multivariable Models 1 | ||
|---|---|---|---|
| Discrimination Model | Segregation Model | ||
| INDICATORS OF RACISM | OR (95% CI) | aOR (95% CI) | aOR (95% CI) |
| Perceived Racial Discrimination | |||
| No | Reference | Reference | Not Included |
| Yes | 2.56 (1.31–4.97) ** | 2.79 (1.37–5.67) ** | Not Included |
| Racial Residential Segregation (High Black Segregation) | |||
| No | Reference | Not Included | Reference |
| Yes | 0.88 (0.44–1.76) | Not Included | 0.89 (0.44–1.79) |
| COVARIATES | |||
| Age (years) | 1.02 (0.99–1.05) † | 1.00 (0.96–1.04) | 1.00 (0.96–1.04) |
| Marital Status | |||
| Not Married | Reference | Not Included | Not Included |
| Married or Living with a Someone | 0.57 (0.20–1.63) | Not Included | Not Included |
| Education | |||
| Less than High School | Reference | Reference | Reference |
| High School or GED | 2.02 (0.72–5.62) † | 1.84 (0.58–5.83) | 1.84 (0.62–5.44) |
| Post High School 2 | 2.71 (0.99–7.37) † | 2.43 (0.74–7.95) | 2.49 (0.82–7.57) |
| Annual Household Income | |||
| None–USD 9999 | Reference | Reference | Reference |
| USD 10,000–USD 19,999 | 1.46 (0.69–3.06) | 1.50 (0.70–3.24) | 1.74 (0.84–3.61) |
| USD 20,000 or more | 1.98 (0.84–4.68) † | 2.07 (0.83–5.16) | 2.14 (0.85–5.36) |
| Health Insurance Status | |||
| No Insurance (or CHIP only) | Reference | Reference | Reference |
| Public and/or Private Insurance | 1.58 (0.82–3.04) † | 1.88 (0.84–4.19) | 1.88 (0.85–4.15) |
| Number of Cancer Screenings Needed | 1.53 (0.96–2.43) † | 1.60 (0.92–2.79) | 1.49 (0.87–2.56) |
| Neighborhood Educational Attainment | |||
| Percent with High School/GED 3 | 1.00 (0.96–1.03) | Not Included | Not Included |
| Percent with Bachelor’s Degree 4 | 0.99 (0.95–1.02) | Not Included | Not Included |
| Percent Neighborhood Below Federal Poverty Line | 0.99 (0.97–1.02) | Not Included | Not Included |
| Perceived Racial Discrimination Strata 1 | ||
|---|---|---|
| No (n = 82) | Yes (n = 67) | |
| EXPOSURES OF INTEREST | aOR (95% CI) | aOR (95% CI) |
| Racial Residential Segregation (High Black Segregation) | ||
| No | Reference | Reference |
| Yes | 1.90 (0.66–5.45) | 0.47 (0.13–1.72) |
| Age (years), mean (SD) | 0.97 (0.91–1.03) | 1.02 (0.96–1.08) |
| Education | ||
| Less than High School | Reference | Reference |
| High School or GED | 0.56 (0.12–2.54) | 7.30 (1.33–40.00) * |
| Post High School 2 | 1.13 (0.26–4.95) | 5.87 (0.91–37.72) †† |
| Annual Household Income | ||
| None–USD 9999 | Reference | Reference |
| USD 10,000–USD 19,999 | 0.89 (0.29–2.74) | 1.72 (0.42–7.03) |
| USD 20,000 or more | 2.49 (0.75–8.27) †† | 2.15 (0.43–10.75) |
| Health Insurance Status | ||
| No Insurance (or CHIP only) | Reference | Reference |
| Public and/or Private Insurance | 3.51 (1.12–10.96) * | 0.92 (0.29–2.98) |
| Number of Cancer Screenings Needed | 2.02 (0.88–4.64) †† | 2.00 (0.70–5.71) †† |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibekwe, L.N.; Fernández-Esquer, M.E.; Pruitt, S.L.; Ranjit, N.; Fernández, M.E. Racism and Cancer Screening among Low-Income, African American Women: A Multilevel, Longitudinal Analysis of 2-1-1 Texas Callers. Int. J. Environ. Res. Public Health 2021, 18, 11267. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111267
Ibekwe LN, Fernández-Esquer ME, Pruitt SL, Ranjit N, Fernández ME. Racism and Cancer Screening among Low-Income, African American Women: A Multilevel, Longitudinal Analysis of 2-1-1 Texas Callers. International Journal of Environmental Research and Public Health. 2021; 18(21):11267. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111267
Chicago/Turabian StyleIbekwe, Lynn N., Maria Eugenia Fernández-Esquer, Sandi L. Pruitt, Nalini Ranjit, and Maria E. Fernández. 2021. "Racism and Cancer Screening among Low-Income, African American Women: A Multilevel, Longitudinal Analysis of 2-1-1 Texas Callers" International Journal of Environmental Research and Public Health 18, no. 21: 11267. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111267