
Development and Pilot Use of a Questionnaire to Assess the Knowledge of Midwives and Pediatric Nurses on Maternal Use of Analgesics during Lactation




Abstract
:1. Introduction
2. Materials and Methods
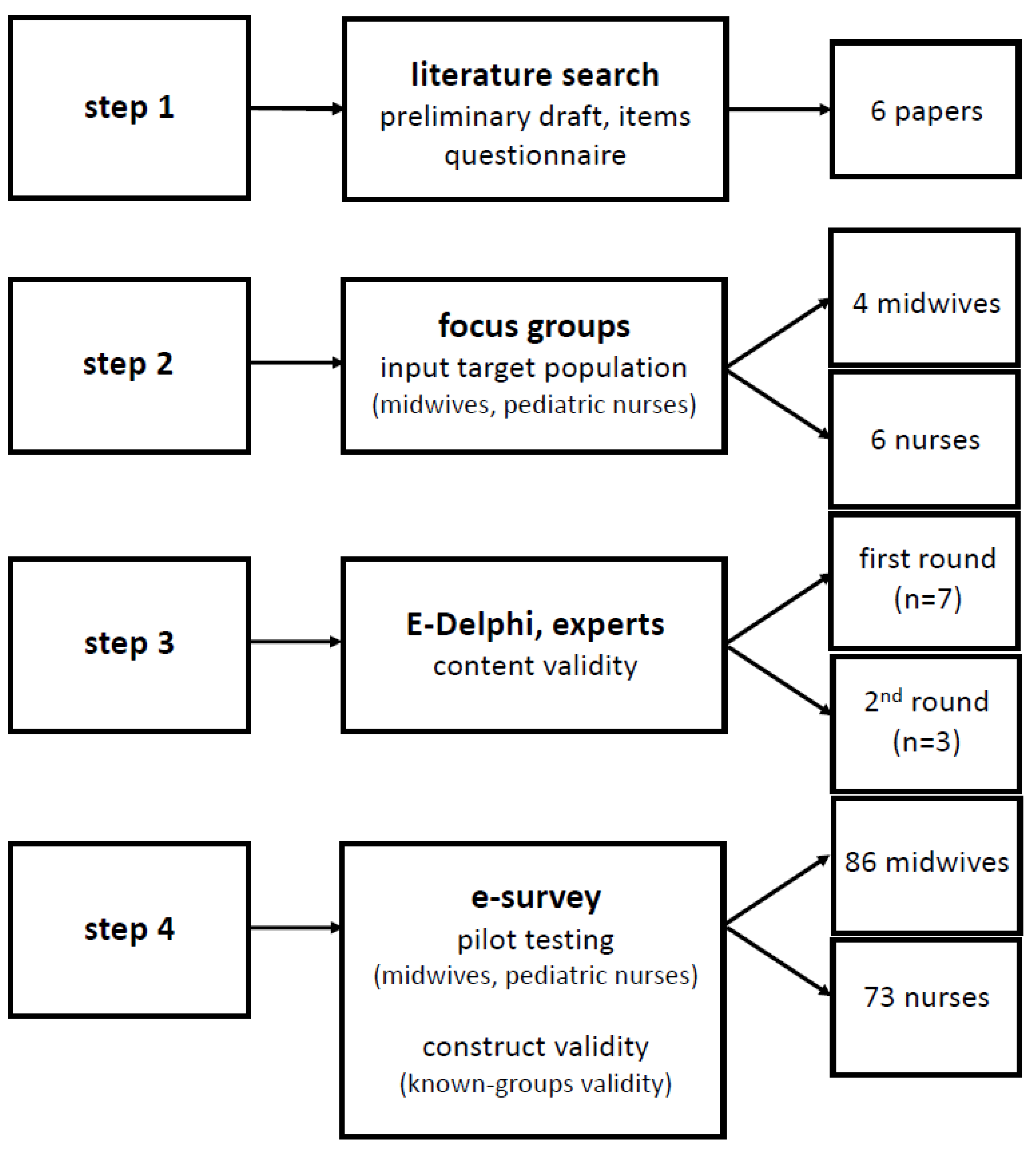
2.1. Development of the Instrument
2.2. Content Validation
2.3. Pilot Use of the Instrument
3. Results
3.1. Development of the Instrument
3.1.1. Step 1, Literature Screening
3.1.2. Step 2, Focus Groups
3.2. Content Validation of the Instrument
3.3. Pilot Use of the Instrument: Construct Validity Based on Known-Groups Validity
4. Discussion
4.1. Main Findings
4.2. Strenghts and Limitations
4.3. Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Available online: http://www.who.int/activities/promoting-baby-friendly-hospitals (accessed on 2 October 2021).
- Byrne, J.J.; Spong, C.Y. “Is it safe?”—The many unanswered questions about medications and breast-feeding. N. Engl. J. Med. 2019, 380, 1296–1297. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.O. Drugs in lactation. Pharm. Res. 2018, 35, 45. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.O.; Pochop, S.L.; Manoguerra, A.S. Adverse drug reactions in breastfed infants: Less than imagined. Clin. Pediatr. 2003, 42, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Ito, S.; Blajchman, A.; Stephenson, M.; Eliopoulos, C.; Koren, G. Prospective follow-up of adverse reactions in breast-fed infants exposed to maternal medication. Am. J. Obstet. Gynecol. 1993, 168, 1393–1399. [Google Scholar] [CrossRef]
- Martin, E.; Vickers, B.; Landau, R.; Reece-Stremtan, S. ABM clinical protocol #28, peripartum analgesia and anesthesia for the breastfeeding mother. Breastfeed. Med. 2018, 13, 164–171. [Google Scholar] [PubMed]
- Wang, J.; Johnson, T.; Sahin, L.; Tassinari, M.S.; Anderson, P.O.; Baker, T.E.; Bucci-Rechtweg, C.; Burckart, G.J.; Chambers, C.D.; Hale, T.W.; et al. Evaluation of the safety of drugs and biological products used during lactation: Workshop summary. Clin. Pharmacol. Ther. 2017, 101, 736–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allegaert, K.; van den Anker, J.N. Maternal analgosedation and breastfeeding: Guidance for the pediatrician. J. Pediatr. Neonatal Individ. Med. 2015, 4, e040117. [Google Scholar]
- Mitchell, J.; Jones, W.; Winkley, E.; Kinsella, S.M. Guideline on anaesthesia and sedation in breastfeeding women 2020: Guideline from the association of anaesthetists. Anaesthesia 2020, 75, 1482–1493. [Google Scholar] [CrossRef]
- Ceulemans, M.; Van Calsteren, K.; Allegaert, K.; Foulon, V. Health products’ and substance use among pregnant women visiting a tertiary hospital in Belgium: A cross-sectional study. Pharmacoepidemiol. Drug Saf. 2019, 28, 1231–1238. [Google Scholar] [CrossRef]
- Stephens, A.; Brodribb, W.; McGuire, T.; Deckx, L. Breastfeeding questions to medicines call centres from the Australian public and health professionals. Austr. J. Prim. Health 2018, 24, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Saha, M.R.; Ryan, K.; Amir, L.H. Postpartum women’s use of medicines and breastfeeding practices: A systematic review. Int. Breastfeed. J. 2015, 10, 28. [Google Scholar] [CrossRef]
- Lupattelli, A.; Spigset, O.; Twigg, M.J.; Zagorodnikova, K.; Mårdby, A.C.; Moretti, M.E.; Drozd, M.; Panchaud, A.; Hämeen-Anttila, K.; Rieutord, A.; et al. Medication use in pregnancy: A cross-sectional, multinational web-based study. BMJ Open 2014, 4, e004365. [Google Scholar] [CrossRef] [Green Version]
- Davanzo, R.; Bua, J.; De Cunto, A.; Farina, M.L.; De Ponti, F.; Clavenna, A.; Mandrella, S.; Sagone, A.; Clementi, M. Advising mothers on the use of medications during breastfeeding: A need for a positive attitude. J. Hum. Lact. 2016, 32, 15–19. [Google Scholar] [CrossRef] [Green Version]
- Spiesser-Robelet, L.; Maurice, A.; Gagnayre, R. Understanding breastfeeding women’s behaviors toward medication: Healthcare professionals’ viewpoint. J. Hum. Lact. 2019, 35, 137–153. [Google Scholar] [CrossRef] [PubMed]
- Al-Sawalha, N.A.; Sawalha, A.; Tahaineh, L.; Almomani, B.; Al-Keilani, M. Healthcare providers’ attitude and knowledge regarding medication use in breastfeeding women: A Jordanian national questionnaire study. J. Obstet. Gynaecol. 2018, 38, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Polit, D.F.; Beck, C.T. Nursing Research: Generating and Assessing Evidence for Nursing Practice, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2017; pp. 1–784. [Google Scholar]
- Spiesser-Robelet, L.; Brunie, V.; de Andrade, V.; Gagnayre, R. Knowledge, representations, attitudes, and behaviors of women faced with taking medications while breastfeeding. J. Hum. Lact. 2017, 33, 98–114. [Google Scholar] [CrossRef]
- Colaceci, S.; Giusti, A.; De Angelis, A.; Della Barba, M.I.; De Vincenti, A.Y.; Vellone, E.; Alvaro, R. Medications, “natural” products, and pharmacovigilance during breastfeeding: A mixed-methods study on women’s opinions. J. Hum. Lact. 2016, 32, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Verstegen, R.H.J.; Ito, S. Drugs in lactation. J. Obstet. Gynaecol. Res. 2019, 45, 522–531. [Google Scholar] [CrossRef]
- Amundsen, S.; Øvrebø, T.G.; Amble, N.M.; Poole, A.C.; Nordeng, H. Risk perception, beliefs about medicines and medical adherence among pregnant and breastfeeding women with migraine: Findings from a cross-sectional study in Norway. BMJ Open 2019, 27, e026690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolgast, E.; Lindh-Åstrand, L.; Lilliecreutz, C. Women’s perceptions of medication use during pregnancy and breastfeeding—A Swedish cross-sectional questionnaire study. Acta Obstet. Gynecol. Scand. 2019, 98, 856–864. [Google Scholar] [CrossRef] [PubMed]
- Ngo, E.; Spigset, O.; Lupattelli, A.; Panchaud, A.; Annaert, P.; Allegaert, K.; Nordeng, H. Antihistamine use during breastfeeding with focus on breast milk transfer and safety in humans—A systematic literature review. Basic Clin. Pharmacol. Toxicol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Nörby, U.; Noël-Cuppers, B.; Hristoskova, S.; Desai, M.; Härmark, L.; Steel, M.; El-Haddad, C.; Douarin, L. Online information discrepancies regarding safety of medicine use during pregnancy and lactation: An IMI ConcePTION study. Expert Opin. Drug Saf. 2021, 20, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Ceulemans, M.; Fortuin, M.; Van Calsteren, K.; Allegaert, K.; Foulon, V. Prevalence and characteristics of pregnancy-and lactation-related calls to the National Poison Centre in Belgium: A retrospective analysis of calls from 2012 to 2017. J. Eval. Clin. Pract. 2020, 26, 911–917. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Methods | Main Findings |
|---|---|---|
| Al-Sawalha et al. [16] | After a pilot study (n = 10), a self-constructed (approach not described) questionnaire was distributed to HCPs (nurses, pharmacists, physicians) in Jordan. This questionnaire had 23 questions (on demographics, attitudes on medicine use during lactation and knowledge) related to the most commonly used medicines during lactation. | 904 responses, 44% nurses (no sub-specialties mentioned). 27% advised to always stop or interrupt breastfeeding whenever a lactating mother took any medicine. Awareness on recommendations was lower in nurses (OR 0.21) compared to physicians. 80% of HCPs considered themselves as having a low level of knowledge, even lower in nurses (OR 0.10). A request to add this topic to curricula and professional continuing education. |
| Spiesser-Robelet et al. [18] | Scoping review on literature sources on breastfeeding mothers’ knowledge, representations, attitudes and behaviors about medicines resulted in 18 papers and 15 studies. Questionnaire development was not assessed, nor discussed. | Most (12/15) studies were quantitative, with HCPs as the target audience and questionnaires were commonly (8/15) used. The studies reflect an almost systematic conflict for the mothers between taking medicines and breastfeeding. Studies describe safety behaviors of breastfeeding women taking medicines, but do not allow them to understand how breastfeeding mothers’ behaviors were constructed. Items were maternal knowledge (n = 2), social representations (n = 4), attitudes (n = 1) and behaviors (incidence, acceptability, or consequence of medicine use during lactation, measures to reduce infant exposure). |
| Colaceci et al. [19] | State-of-the-art development of a questionnaire, using a mixed methods study, with the construction of the questionnaire based on four categories (experience, medicines versus natural products, access to information and adverse reactions), subsequently administered to 248 pregnant women or mothers. | Women showed three attitudes: discontinue breastfeeding in order to take the medicine, “endure the pain” or use ‘natural products’ as these are perceived to be safer. Information sources for lactation management were pediatricians (46%), midwives (24%) and prescribers (10%), reflecting the relevance of HCPs. |
| Verstegen et al. [20] | Narrative review, with a focus on the clinical pharmacology of lactation related medicine exposure and methods to assess exposure and effects. | Specific section on the lactation compatibility of analgesics, anesthetics and sedatives. Acetaminophen and non-steroidal, anti-inflammatory drugs are safe. Opioids can be used safely for short-term pain management, with the need for more intense monitoring (lethargy, respiratory depression) when longer treatment duration is needed. |
| Amundsen et al. [21] | Cross-sectional questionnaire among 401 women with migraine, either pregnant or in postpartum (<18 months). The development of the questionnaire has not been described, but a pilot (n = 6) was done, with only minor adaptations afterwards. | The majority severely overestimated the risk associated with migraine medicines during pregnancy or lactation. Women who reported medicine use were more positive and overestimated lesser the risks of such medicines compared with their counterparts. |
| Wolgast et al. [22] | Questionnaire on the use, perceptions towards the use and perceptions about pregnancy outcomes in association with medicines during pregnancy and lactation. In total, 850 women participated. Its development was based on two questions from a former questionnaire. | The majority (58%) perceived medicines during lactation as (probably) harmful and perceived herbal medicines as less harmful (21%). Women had great confidence in advice form a physician (84%) or midwife (77%). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janssens, I.; Van Hauwe, M.; Ceulemans, M.; Allegaert, K. Development and Pilot Use of a Questionnaire to Assess the Knowledge of Midwives and Pediatric Nurses on Maternal Use of Analgesics during Lactation. Int. J. Environ. Res. Public Health 2021, 18, 11555. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111555
Janssens I, Van Hauwe M, Ceulemans M, Allegaert K. Development and Pilot Use of a Questionnaire to Assess the Knowledge of Midwives and Pediatric Nurses on Maternal Use of Analgesics during Lactation. International Journal of Environmental Research and Public Health. 2021; 18(21):11555. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111555
Chicago/Turabian StyleJanssens, Ine, Margot Van Hauwe, Michael Ceulemans, and Karel Allegaert. 2021. "Development and Pilot Use of a Questionnaire to Assess the Knowledge of Midwives and Pediatric Nurses on Maternal Use of Analgesics during Lactation" International Journal of Environmental Research and Public Health 18, no. 21: 11555. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111555