
An eCoach-Pain for Patients with Chronic Musculoskeletal Pain in Interdisciplinary Primary Care: A Feasibility Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Setting
2.2. The eCoach-Pain
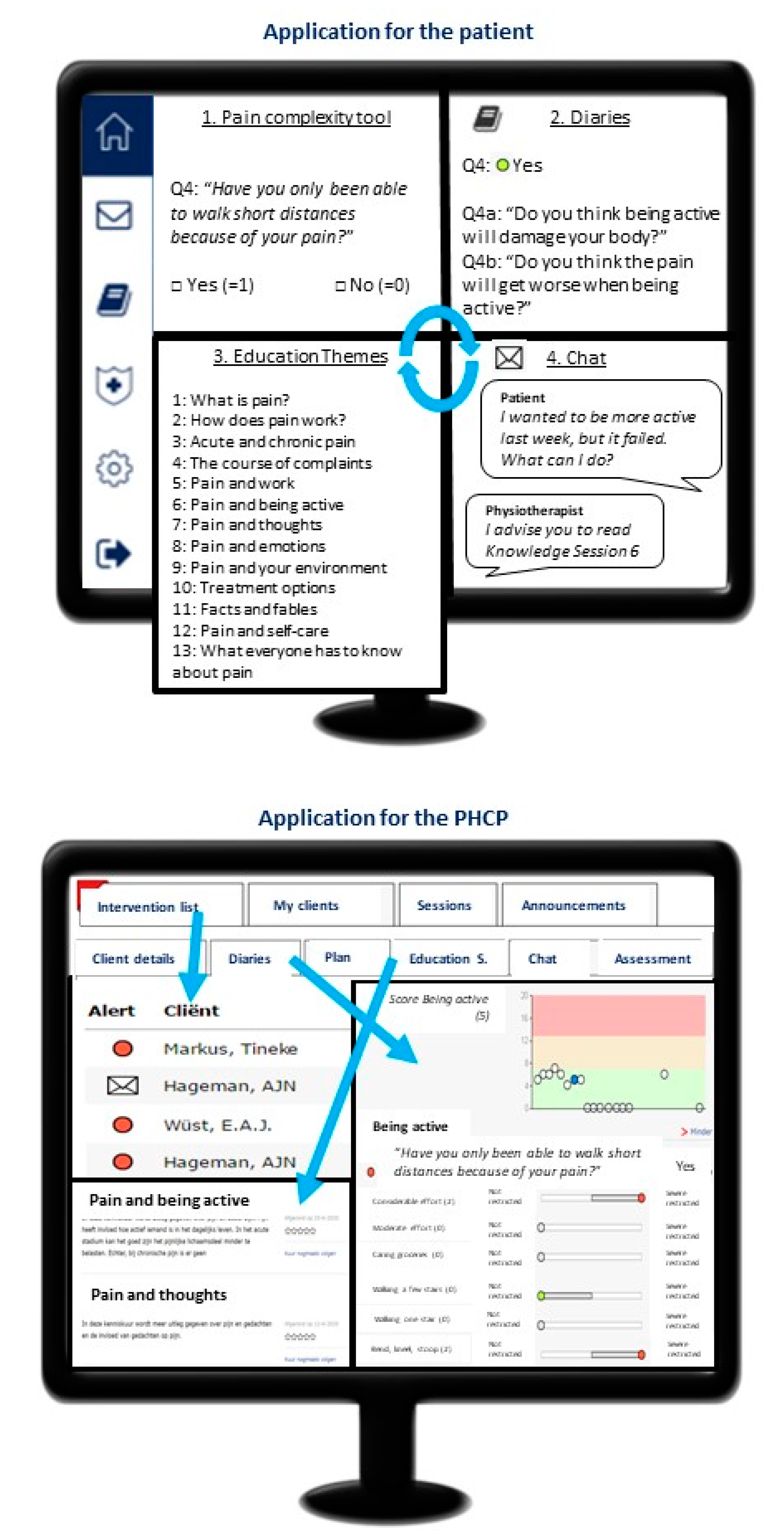
2.2.1. Application for the Patient
- 1.
- The pain complexity tool:
- (A)
- The STarT MSK Tool assessing the complexity of the pain problem for referral within primary care. The patient’s first action in the eCoach-Pain is completing this questionnaire. The Dutch version of the STarT MSKTool is translated and validated [30,31]. The STarT MSK Tool exists of nine Yes (=1) or No (=0) questions regarding activity level, anxiety, depression, and thoughts about CMP and one Visual Analogue Scale (0–10) to assess pain intensity (0–4 = 0 points, 5–6 = 1 point, 7–8 = 2 points, 9–10 = 3 points). All scores are summed, and a total score of 0–4 indicated a low risk, a total score from 5–8 indicated a moderate risk, and a total score from 9–12 indicated a high risk of developing CMP.
- (B)
- To further differentiate within the range of primary, secondary and tertiary rehabilitation care an additional set of questions about the biopsychosocial complaints and background of the patient was added to be filled in by the PHCP. After completion of both parts of the complexity tool, the eCoach-Pain calculates the score and assigns the best-fitting referral option to assist the PHCP. The PHCP discusses the results with the patient and refers him/her to the most appropriate treatment via shared decision making.
- 2.
- Diaries:
- 3.
- Education sessions:
- 4.
- Chat function:
2.2.2. Application for the PHCPs
2.3. Data Collection and Analysis
2.3.1. Learnability, Usability, and Desirability
2.3.2. Adherence to the Application
2.3.3. Experiences of Patients
2.3.4. Experiences of PHCPs
3. Results
3.1. Learnability, Usability, and Desirability
3.2. Adherence to the Application
3.3. Experiences of Patients and PHCPs
3.3.1. Overall Opinion and Usage
R16: “Basically, I think it is a good app. However, the questions appear too frequent, too standard.”
PT2: “I like the idea that every week new educational sessions about pain are open for the patient. And, that I can see what the patient answered, which information they have read, and that I can use that during the treatment session. This causes more structure in my treatments.”
GP2: “The eCoach-Pain is an extra treatment option above the existing options. As a GP, it is important to know the content of the treatment options when referring to a PT, and it is great that we can offer something extra.”
3.3.2. Pain Complexity Tool and Diaries
R02: “I thought that I had to fill in some questions a few times. However, the questions came every day or week for two or three months. And this was not explained to me beforehand.”
GP1: “When using the paper-version, you have more freedom in the choice of the treatment. As you can overrule the score of the patient easier. In the eCoach-Pain, the treatment options are more limited based on the answers of the patients. Which is a strength of the eCoach-Pain.”
3.3.3. Educational Sessions
R10: “It was a revelation for me, because through the information in the educational sessions, in addition with information on the same topic given by my PHCP, I understand how my brain controls the pain”.
R13: “I have read all sessions and the total overview was good for me. But at the same time it was also confronting, maybe that was good, as well.”
3.3.4. Chat Function and Communication with PHCP
GP1: “Because of our work-flow, it is the easiest way that the PT communicates with the patient and has a prominent role in the follow-up.”
3.3.5. Technical Issues
3.3.6. Future Usage and Recommendations of the eCoach-Pain
R16: “I would recommend it to people who get acquainted with pain complaints, or who have not so much knowledge yet, for them it is useful to get to know more about pain. But for people who have complaints for years, like me, I would not recommend it.”
GP1: “Because of the high work-load in primary care, it would be of added value when someone as a PNMH can get a more prominent role in follow-up of patients. They will also be able to keep track of the eCoach-Pain activities. We as GPs have not enough time to do this properly.”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef] [PubMed]
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study. Lancet 2020, 396, 2006–2017. [Google Scholar] [CrossRef]
- Fayaz, A.; Croft, P.; Langford, R.M.; Donaldson, L.J.; Jones, G.T. Prevalence of chronic pain in the UK: A systematic review and meta-analysis of population studies. BMJ Open 2016, 6, e010364. [Google Scholar] [CrossRef] [PubMed]
- Bekkering, G.E.; Bala, M.M.; Reid, K.; Kellen, E.; Harker, J.; Riemsma, R.; Huygen, F.J.; Kleijnen, J. Epidemiology of chronic pain and its treatment in The Netherlands. Neth J. Med. 2011, 69, 141–153. [Google Scholar] [PubMed]
- Breivik, H.; Eisenberg, E.; O’Brien, T.; Openminds. The individual and societal burden of chronic pain in Europe: The case for strategic prioritisation and action to improve knowledge and availability of appropriate care. BMC Public Health 2013, 13, 1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaskin, D.J.; Richard, P. The economic costs of pain in the United States. J. Pain 2012, 13, 715–724. [Google Scholar] [CrossRef]
- World Health Organization. Rehabilitation in Health Systems; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Roberts, A.; Philip, L.; Currie, M.; Mort, A. Striking a balance between in-person care and the use of eHealth to support the older rural population with chronic pain. Int. J. Qual Stud. Health Well-Being 2015, 10, 27536. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Observatory for eHealth. Building Foundations for eHealth: Progress of Member States: Report of the Global Observatory for eHealth; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Eysenbach, G. What is e-health? J. Med. Internet Res. 2001, 3, E20. [Google Scholar] [CrossRef] [PubMed]
- Özden, F.; Sarı, Z.; Karaman, Ö.N.; Aydoğmuş, H. The effect of video exercise-based telerehabilitation on clinical outcomes, expectation, satisfaction, and motivation in patients with chronic low back pain. Ir. J. Med. Sci. 2021, 1–11. [Google Scholar] [CrossRef]
- van de Graaf, D.L.; Trompetter, H.R.; Smeets, T.; Mols, F. Online Acceptance and Commitment Therapy (ACT) interventions for chronic pain: A systematic literature review. Internet Interv. 2021, 26, 100465. [Google Scholar] [CrossRef]
- McGuire, B.E.; Henderson, E.M.; McGrath, P.J. Translating e-pain research into patient care. Pain 2017, 158, 190–193. [Google Scholar] [CrossRef]
- Dutch Pain Society en het Samenwerkingsverband Pijnpatiënten. Zorgstandaard Chronische Pijn. Available online: https://www.zorginzicht.nl/kwaliteitsinstrumenten/chronische-pijn (accessed on 1 November 2021).
- World Health Organization. Digital Health Investements should be Coordinated to Support Continuity of Care; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Niv, D.; Devor, M.; European Federation of, I.C. Position paper of the European Federation of IASP Chapters (EFIC) on the subject of pain management. Eur J. Pain 2007, 11, 487–489. [Google Scholar] [CrossRef]
- Committee on Education of the EFIC (European Federation of IASP Chapters). The Pain Management Core Curriculum for European Medical Schools; European Federation of IASP: Washington, DC, USA, 2013; p. 33. [Google Scholar]
- Domenech, J.; Sanchez-Zuriaga, D.; Segura-Orti, E.; Espejo-Tort, B.; Lison, J.F. Impact of biomedical and biopsychosocial training sessions on the attitudes, beliefs, and recommendations of health care providers about low back pain: A randomised clinical trial. Pain 2011, 152, 2557–2563. [Google Scholar] [CrossRef]
- Bronstein, L.R. A Model for Interdisciplinary Collaboration. Soc. Work 2003, 48, 297–306. [Google Scholar] [CrossRef]
- Puntillo, F.; Giglio, M.; Brienza, N.; Viswanath, O.; Urits, I.; Kaye, A.D.; Pergolizzi, J.; Paladini, A.; Varrassi, G. Impact of COVID-19 pandemic on chronic pain management: Looking for the best way to deliver care. Best Pract. Res. Clin. Anaesthesiol. 2020, 34, 529–537. [Google Scholar] [CrossRef]
- Slattery, B.W.; Haugh, S.; O’Connor, L.; Francis, K.; Dwyer, C.P.; O’Higgins, S.; Egan, J.; McGuire, B.E. An Evaluation of the Effectiveness of the Modalities Used to Deliver Electronic Health Interventions for Chronic Pain: Systematic Review With Network Meta-Analysis. J. Med. Internet Res. 2019, 21, e11086. [Google Scholar] [CrossRef] [Green Version]
- Lindberg, B.; Nilsson, C.; Zotterman, D.; Söderberg, S.; Skär, L. Using Information and Communication Technology in Home Care for Communication between Patients, Family Members, and Healthcare Professionals: A Systematic Review. Int. J. Telemed. Appl. 2013, 2013, 461829. [Google Scholar] [CrossRef] [Green Version]
- Moseley, G.L.; Nicholas, M.K.; Hodges, P.W. A randomized controlled trial of intensive neurophysiology education in chronic low back pain. Clin. J. Pain 2004, 20, 324–330. [Google Scholar] [CrossRef]
- Malfliet, A.; Kregel, J.; Meeus, M.; Roussel, N.; Danneels, L.; Cagnie, B.; Dolphens, M.; Nijs, J. Blended-Learning Pain Neuroscience Education for People With Chronic Spinal Pain: Randomized Controlled Multicenter Trial. Phys. Ther. 2017, 98, 357–368. [Google Scholar] [CrossRef]
- Ekman, I.; Swedberg, K.; Taft, C.; Lindseth, A.; Norberg, A.; Brink, E.; Carlsson, J.; Dahlin-Ivanoff, S.; Johansson, I.-L.; Kjellgren, K.; et al. Person-Centered Care—Ready for Prime Time. Eur. J. Cardiovasc. Nurs. 2011, 10, 248–251. [Google Scholar] [CrossRef]
- Koppenaal, T.; Arensman, R.M.; van Dongen, J.M.; Ostelo, R.W.J.G.; Veenhof, C.; Kloek, C.J.J.; Pisters, M.F. Effectiveness and cost-effectiveness of stratified blended physiotherapy in patients with non-specific low back pain: Study protocol of a cluster randomized controlled trial. BMC Musculoskelet. Dis. 2020, 21, 265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keogh, E.; Rosser, B.A.; Eccleston, C. e-Health and chronic pain management: Current status and developments. Pain 2010, 151, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Cynthia, L.; Ivan, P.J.H.; Mariëlle, E.A.L.K.; Albère, J.K.; Gijs, B.; Dirk, R.; Jeanine, A.V. Exploring the feasibility of a network of organizations for pain rehabilitation: What are the lessons learned? Res. Square 2021. [Google Scholar] [CrossRef]
- Sananet Care BV. Sananet: Specialist in eHealth. Available online: https://www.sananet.nl/ (accessed on 27 August 2021).
- Dunn, K.; Campbell, P.; Afolabi, E.; Lewis, M.; van der Windt, D.; Hill, J.; Mallen, C.; Protheroe, J.; Hay, E.; Foster, N. Refinement and validation of the keele start msk tool for musculoskeletal pain in primary care. Rheumatology 2017, 56. [Google Scholar] [CrossRef] [Green Version]
- van den Broek, A.G.; Kloek, C.J.J.; Pisters, M.F.; Veenhof, C. Construct validity and test-retest reliability of the Dutch STarT MSK tool in patients with musculoskeletal pain in primary care physiotherapy. PLoS ONE 2021, 16, e0248616. [Google Scholar] [CrossRef]
- de Jong, M.J.; van der Meulen-de Jong, A.E.; Romberg-Camps, M.J.; Becx, M.C.; Maljaars, J.P.; Cilissen, M.; van Bodegraven, A.A.; Mahmmod, N.; Markus, T.; Hameeteman, W.M.; et al. Telemedicine for management of inflammatory bowel disease (myIBDcoach): A pragmatic, multicentre, randomised controlled trial. Lancet 2017, 390, 959–968. [Google Scholar] [CrossRef]
- Amin, H.; Weerts, J.; Brunner-La Rocca, H.P.; Knackstedt, C.; Sanders-van Wijk, S. Future perspective of heart failure care: Benefits and bottlenecks of artificial intelligence and eHealth. Future Cardiol. 2021, 17, 917–921. [Google Scholar] [CrossRef]
- Hochstenbach, L.M.; Zwakhalen, S.M.; Courtens, A.M.; van Kleef, M.; de Witte, L.P. Feasibility of a mobile and web-based intervention to support self-management in outpatients with cancer pain. Eur. J. Oncol. Nurs. 2016, 23, 97–105. [Google Scholar] [CrossRef] [Green Version]
- QSR International Pty Ltd. (2018) NVivo (Version 12). Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 4 November 2021).
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef]
- Kiger, M.E.; Varpio, L. Thematic analysis of qualitative data: AMEE Guide No. Med. Teach. 2020, 42, 846–854. [Google Scholar] [CrossRef]
- Yuan, E.S. Zoom; Zoom Video Communications, Inc.: San Jose, CA, USA, 2011. [Google Scholar]
- Bair, M.J.; Robinson, R.L.; Katon, W.; Kroenke, K. Depression and pain comorbidity: A literature review. Arch. Intern. Med. 2003, 163, 2433–2445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsang, A.; Von Korff, M.; Lee, S.; Alonso, J.; Karam, E.; Angermeyer, M.C.; Borges, G.L.; Bromet, E.J.; Demytteneare, K.; de Girolamo, G.; et al. Common chronic pain conditions in developed and developing countries: Gender and age differences and comorbidity with depression-anxiety disorders. J. Pain 2008, 9, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.P.; Arnold, J.B.; Evans, A.M.; Yaxley, A.; Damarell, R.A.; Shanahan, E.M. The association between body fat and musculoskeletal pain: A systematic review and meta-analysis. BMC Musculoskelet. Dis. 2018, 19, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, A.; Kamper, S.J.; Wiggers, J.H.; O’Brien, K.M.; Lee, H.; Wolfenden, L.; Yoong, S.L.; Robson, E.; McAuley, J.H.; Hartvigsen, J.; et al. Musculoskeletal conditions may increase the risk of chronic disease: A systematic review and meta-analysis of cohort studies. BMC Med. 2018, 16, 167. [Google Scholar] [CrossRef]
- Rijken, M.; Korevaar, J. Goede Zorg Voor Mensen met Multimorbiditeit: Handvatten Voor de Ontwikkeling en Evaluatie van Zorg Voor Mensen met Meerdere Chronische Aandoeningen; Nivel: Utrecht, The Netherlands, 2021. [Google Scholar]
- Smeets, R.G.M.; Kroese, M.; Ruwaard, D.; Hameleers, N.; Elissen, A.M.J. Person-centred and efficient care delivery for high-need, high-cost patients: Primary care professionals’ experiences. BMC Fam. Pract. 2020, 21, 106. [Google Scholar] [CrossRef]
- Nijs, J.; Roussel, N.; Paul van Wilgen, C.; Köke, A.; Smeets, R. Thinking beyond muscles and joints: Therapists’ and patients’ attitudes and beliefs regarding chronic musculoskeletal pain are key to applying effective treatment. Man. Ther. 2013, 18, 96–102. [Google Scholar] [CrossRef]
- Pietila Holmner, E.; Stalnacke, B.M.; Enthoven, P.; Stenberg, G. “The acceptance” of living with chronic pain—an ongoing process: A qualitative study of patient experiences of multimodal rehabilitation in primary care. Pain Med. 2018, 50, 73–79. [Google Scholar]
- van der Meer, H.A.; de Pijper, L.; van Bruxvoort, T.; Visscher, C.M.; Nijhuis-van der Sanden, M.W.G.; Engelbert, R.H.H.; Speksnijder, C.M. Using e-Health in the physical therapeutic care process for patients with temporomandibular disorders: A qualitative study on the perspective of physical therapists and patients. Disabil. Rehabil. 2020, 1–8. [Google Scholar] [CrossRef]
- Orlando, J.F.; Beard, M.; Kumar, S. Systematic review of patient and caregivers’ satisfaction with telehealth videoconferencing as a mode of service delivery in managing patients’ health. PLoS ONE 2019, 14, e0221848. [Google Scholar] [CrossRef] [Green Version]
- van Tilburg, M.L.; Kloek, C.J.J.; Staal, J.B.; Bossen, D.; Veenhof, C. Feasibility of a stratified blended physiotherapy intervention for patients with non-specific low back pain: A mixed methods study. Physiother. Theory Pract. 2020, 1–13. [Google Scholar] [CrossRef]
- Zorgimpuls. e-Health in de Eerste Lijn, Wat Kunnen We Ermee? Available online: https://www.zorgimpuls.nl/upload/files/Artikelen%20ZorgImpuls/ZorgImpuls%20whitepaper%20e-health%20totaal_feb%202018.pdf (accessed on 1 November 2021).
- Daniels, N.E.M.; Hochstenbach, L.M.J.; van Bokhoven, M.A.; Beurskens, A.; Delespaul, P. Implementing Experience Sampling Technology for Functional Analysis in Family Medicine—A Design Thinking Approach. Front. Psychol. 2019, 10, 2782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joosten, E.A.; DeFuentes-Merillas, L.; de Weert, G.H.; Sensky, T.; van der Staak, C.P.; de Jong, C.A. Systematic review of the effects of shared decision-making on patient satisfaction, treatment adherence and health status. Psychother. Psychosom. 2008, 77, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Nederlands Huisartsen Genootschap. NHG-Standpunt: E-Health Voor Huisarts en Patiënt. Available online: https://www.nhg.org/nhg-e-health (accessed on 31 March 2021).
- Higgins, K.S.; Tutelman, P.R.; Chambers, C.T.; Witteman, H.O.; Barwick, M.; Corkum, P.; Grant, D.; Stinson, J.N.; Lalloo, C.; Robins, S.; et al. Availability of researcher-led eHealth tools for pain assessment and management: Barriers, facilitators, costs, and design. PAIN Rep. 2018, 3, e686. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Registration via | Primary Care Practice | Data Available | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Participant Number | Sex (%) | Age (y) (Median, IQR) | Days Active in the Coach Till Export (Median, IQR) | First Contact Person | PHCP (n, %) | Webpage (n, %) | 1 (n, %) | 2 (n, %) | Questionnaire (n, %) September 2020 | Export (n, %) October 2020 | Interview (n, %) September + December 2020 |
| R01 | M | 41 | 103 | GP | X | X | X | X | |||
| R02 | M | 61 | 86 | GP | X | X | X | X | X | ||
| R03 | M | 36 | 124 | GP | X | X | X | X | |||
| R04 | F | 69 | 109 | PT | X | X | X | X | |||
| R05 | M | 70 | 54 | GP | X | X | X | X | |||
| R06 | M | 71 | 115 | GP | X | X | X | X | X | ||
| R07 | F | 67 | 133 | PT | X | X | X | X | X | ||
| R08 | M | 70 | 61 | GP | X | X | X | ||||
| R09 | F | 43 | 150 | PT | X | X | X | X | |||
| R10 | F | 65 | 7 | PT | X | X | X | X | X | ||
| R11 | F | 66 | 112 | GP | X | X | X | X | |||
| R12 | F | 47 | 68 | PT | X | X | X | X | |||
| R13 | F | 46 | 117 | PT | X | X | X | X | |||
| R14 | F | 60 | 92 | GP | X | X | X | X | |||
| R15 | M | 62 | 117 | GP | X | X | X | X | |||
| R16 | F | 32 | 83 | GP | X | X | X | X | |||
| R17 | F | 50 | n.a. | PNMH | X | X | X | ||||
| R18 | F | 41 | n.a. | PT | X | X | X | ||||
| R19 | F | 45 | n.a. | PT | X | X | X | ||||
| R20 | M | 50 | 65 | PT | X | X | X | ||||
| R21 | F | 57 | 98 | GP | X | X | X | ||||
| R22 | F | 35 | 56 | PT | X | X | X | ||||
| R23 | F | 44 | 105 | GP | X | X | X | ||||
| R24 | F | 24 | 127 | GP | X | X | X | ||||
| R25 | F | 29 | 118 | PNMH | X | X | X | ||||
| R26 | F | 64 | 115 | GP | X | X | X | ||||
| R27 | F | 40 | 59 | PT | X | X | X | ||||
| R28 | F | 38 | 144 | PT | X | X | X | ||||
| R29 | F | 65 | 127 | PT | X | X | X | ||||
| Total: | F:21 72% | 50.0—24.0 | 107.0—46.0 | GP: 14, PT: 13, PNMH: 2 | 13 45% | 16 55% | 8 28% | 21 72% | 11 38% | 26 90% | 11 38% |
| Subscribed by | |||
|---|---|---|---|
| GP and PT (n = 11) | GP (n = 6) | PT (n = 5) | |
| Learnability | 5.0 (1.0) | 5.0 (0.0) | 5.0 (1.0) |
| It was easy to learn how to use the application. | 5.0 (0.5) | 5.0 (0.0) | 5.0 (1.0) |
| I think the application was very complicated. a | 5.0 (0.5) | 5.0 (0.5) | 5.0 (1.0) |
| I needed a lot of help to learn using the application. a | 5.0 (0.5) | 5.0 (0.0) | 5.0 (3.0) |
| I quickly caught on how I could use the application. | 5.0 (1.0) | 5.0 (0.8) | 4.0 (1.0) |
| I am confident that I used the application in the right way. | 5.0 (1.5) | 5.0 (0.8) | 4.0 (0.8) |
| Usability | 5.0 (1.5) | 5.0 (1.0) | 5.0 (2.0) |
| I could easily login into the application. | 5.0 (1.0) | 5.0 (0.8) | 4.0 (2.0) |
| I could easily report my pain, activities, feelings, thoughts, and emotions. | 5.0 (1.5) | 5.0 (0.8) | 5.0 (3.0) |
| I understood the information in the educational sessions about my pain, activities, feelings, thoughts, and emotions. | 5.0 (1.0) | 5.0 (0.8) | 5.0 (2.0) |
| I could easily search for information about pain with the application. | 5.0 (2.0) | 5.0 (1.5) | 4.0 (2.0) |
| I could easily leave a message for the PHCP via the application. | 5.0 (1.5) | 4.5 (1.8) | 5.0 (0.0) |
| Desirability | 4.0 (2.0) (n = 10) | 4.5 (2.0) | 4.0 (1.0) (n = 4) |
| I liked using the application. | 4.0 (1.0) | 5.0 (1.5) | 4.0 (1.8) |
| I liked using the pain diary for reporting my pain, activities, feelings, thoughts, and emotions. | 4.0 (1.0) | 5.0 (0.8) | 4.0 (1.3) |
| I liked using the educational sessions. | 4.0 (1.8) | 4.5 (2.0) | 3.5 (1.0) |
| I liked using the chat function. | 3.0 (1.8) | 3.5 (1.8) | 3.0 (1.0) |
| I liked the idea that my PHCP monitors my pain, activities, feelings, thoughts, and emotions. | 4.5 (1.0) | 4.5 (1.0) | 4.5 (1.5) |
| I liked the idea that my PHCP could adjust my treatment based on my answers in the eCoach-Pain. | 4.0 (2.0) | 4.0 (1.8) | 4.0 (2.3) |
| I would like to recommend the application to other patients. | 4.0 (2.0) | 4.5 (1.8) | 3.5 (1.0) |
| Total overall score (0–10) | 7.0 (2.8) | 8.5 (2.3) | 6.5 (0.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamper, C.; Huijnen, I.; de Mooij, M.; Köke, A.; Verbunt, J.; Kroese, M. An eCoach-Pain for Patients with Chronic Musculoskeletal Pain in Interdisciplinary Primary Care: A Feasibility Study. Int. J. Environ. Res. Public Health 2021, 18, 11661. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111661
Lamper C, Huijnen I, de Mooij M, Köke A, Verbunt J, Kroese M. An eCoach-Pain for Patients with Chronic Musculoskeletal Pain in Interdisciplinary Primary Care: A Feasibility Study. International Journal of Environmental Research and Public Health. 2021; 18(21):11661. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111661
Chicago/Turabian StyleLamper, Cynthia, Ivan Huijnen, Maria de Mooij, Albère Köke, Jeanine Verbunt, and Mariëlle Kroese. 2021. "An eCoach-Pain for Patients with Chronic Musculoskeletal Pain in Interdisciplinary Primary Care: A Feasibility Study" International Journal of Environmental Research and Public Health 18, no. 21: 11661. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111661