
Teaching Urology to Undergraduates: A Prospective Survey of What General Practitioners Need to Know

 ,
,  ,
,  , , , , and
, , , , and
Abstract
:1. Background
2. Methods
3. Results
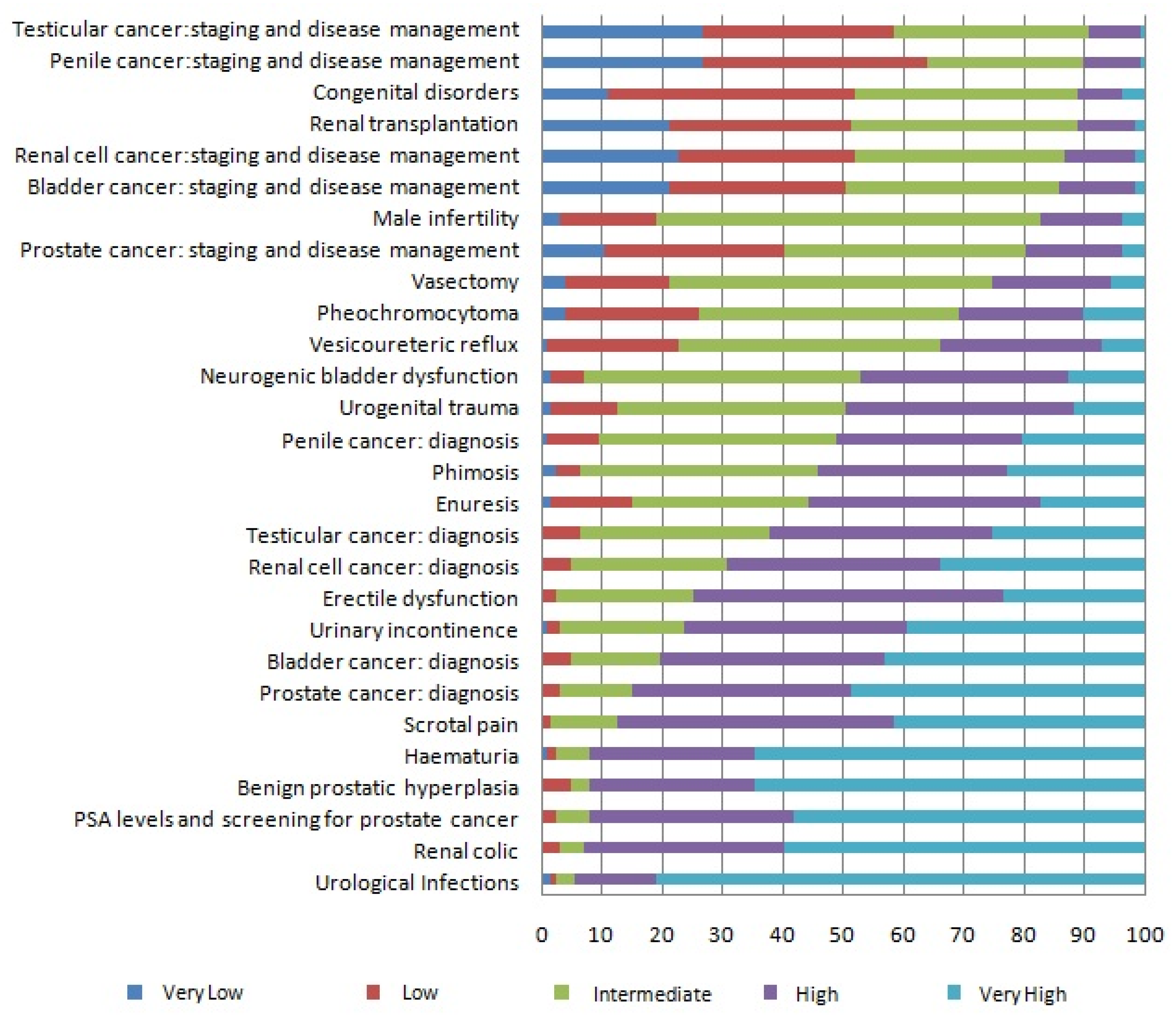
3.1. Evaluation of Urological KNOWLEDGE Needs
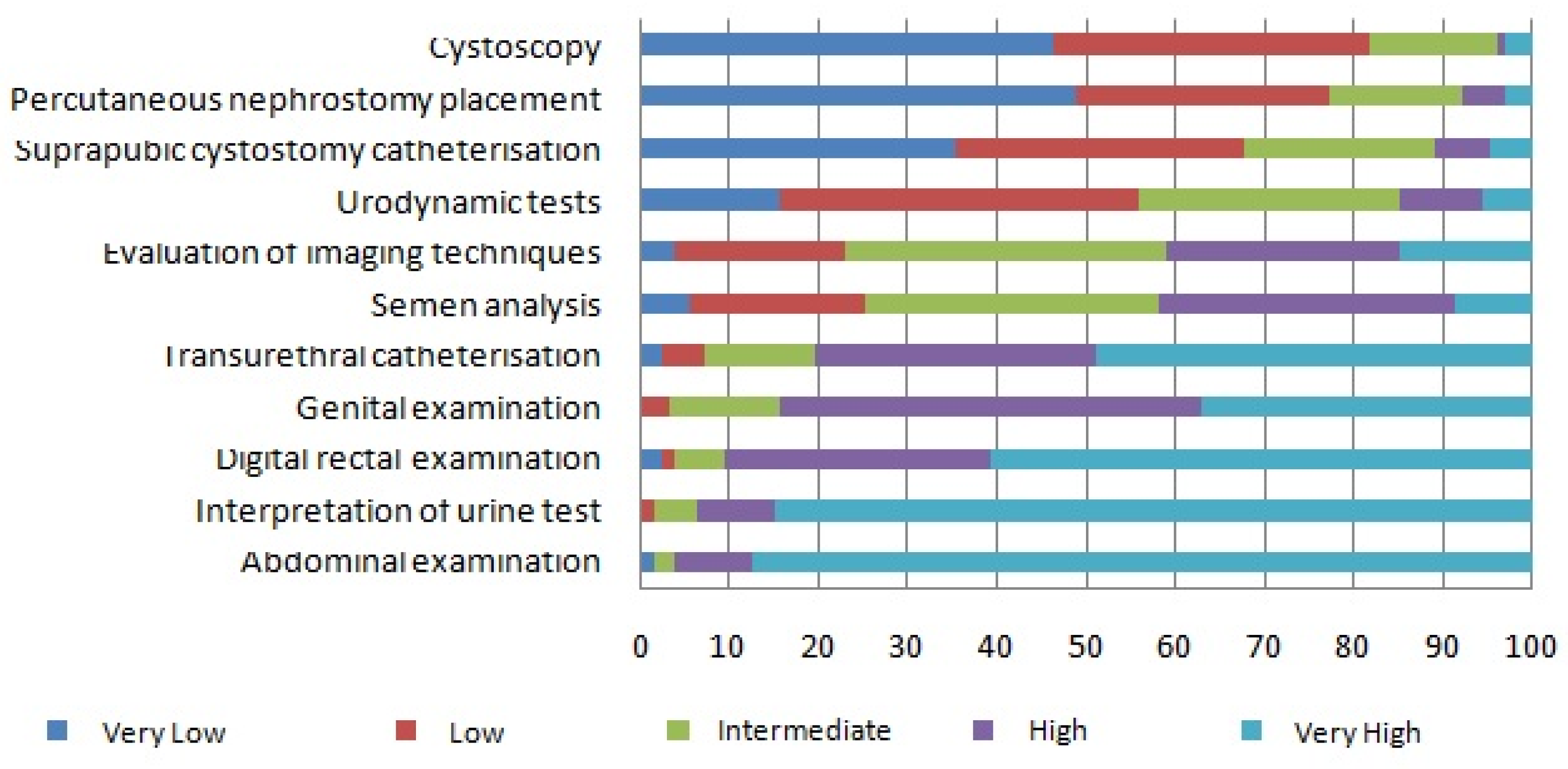
3.2. Evaluation of Urological SKILLS Needs
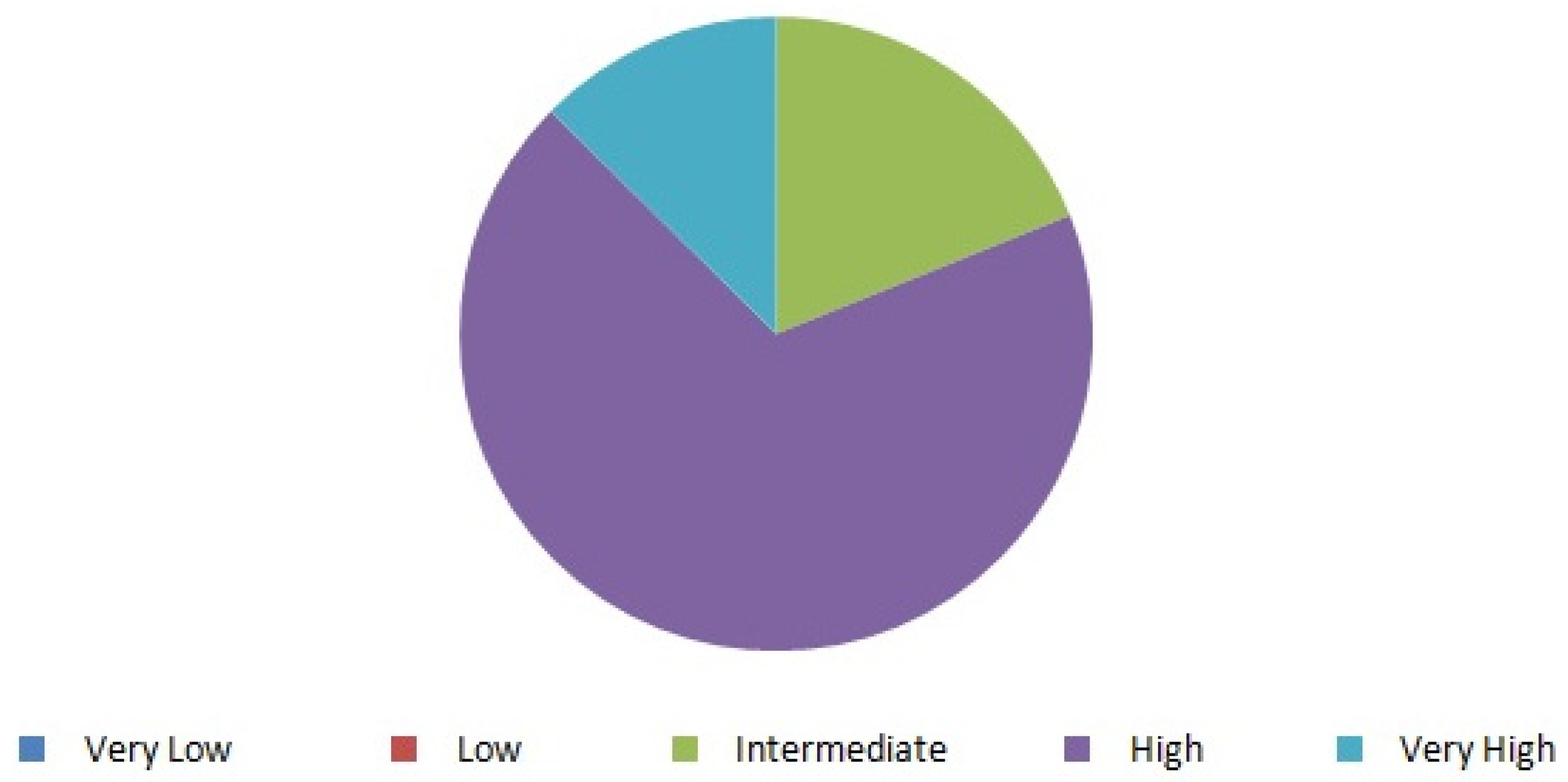
3.3. Evaluation of the RELEVANCE of Urological Pathology in Their Clinical Practice
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| GPs | General Practitioners |
| EHEA | European Higher Education Area |
| UTI | Urinary tract infections |
| BPH | Benign prostatic hyperplasia |
| DRE | Digital rectal examination |
References
- Binsaleh, S.; Al-Jasser, A.; Almannie, R.; Madbouly, K. Attitude and perception of urology by medical students at the end of their medical school: An appraisal from Saudi Arabia. Urol. Ann. 2015, 7, 211–220. [Google Scholar]
- Kerfoot, B.P.; Masser, B.A.; Dewolf, W.C. The continued decline of formal urological education of medical students in the United States: Does it matter? J. Urol. 2006, 175, 2243–2248. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/16697847 (accessed on 23 August 2021). [CrossRef]
- Hoag, N.A.; Hamidizadeh, R.; MacNeily, A.E. Undergraduate exposure to urology: Impact of the distributed model of medical education in British Columbia. J. Can. Urol. Assoc. 2013, 7, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Vela Navarrete, R.; Leduc, A.; Ackerman, R.; Ekman, P.; Leisinger, H. European Academy of Urology. Medical students’ exposure to urology in European medical schools: Historical review and current proposals. Eur. Urol. 2008, 54, 1214–1215. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/18814957 (accessed on 23 August 2021). [CrossRef]
- BOE. Orden SCB/925/2019, de 30 de Agosto, por la que se Aprueba la oferta de Plazas y la Convocatoria de Pruebas Selectivas 2019 para el Acceso en el año 2020, a Plazas de Formación Sanitaria Especializada para las Titulaciones Universitarias De grado/Licencia. 2019. Available online: http://www.boe.es (accessed on 23 August 2021).
- Vela-Navarrete, R.; Carballido, J.; Gonzalez-Enguita, C.; Olivier Gómez, C.; Rodríguez De Betancourt, F. Urology at the European university: Adaptations to the Bologna Plan. The model of the Autonomous University of Madrid. Actas Urol. Esp. 2015, 39, 399–404. [Google Scholar] [CrossRef]
- Navarrete, R.V.; Le Duc, A.; Ackermann, R.; Boccon-Gibod, L.; Debruyne, F.; Ekman, P.; Jonas, U.; Abrahamsson, P.A.; Artibani, W.; Chapple, C.; et al. Medical students’ exposure to urology in European schools: The European association of urology proposals for a convergence programme. Eur. Urol. 2010, 58, 528–531. [Google Scholar] [CrossRef]
- Shah, J.; Manson, J.; Boyd, J. Recruitment in urology: A national survey in the UK. Ann. R. Coll. Surg. Engl. 2004, 86, 186–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miah, S.; Mangera, A.; Venugopal, S.; Luk, A.; Mcdermid, R.; Rosario, D. The clinical need for undergraduate urology. Clin. Teach. 2015, 12, 353–355. [Google Scholar] [CrossRef] [PubMed]
- Loughlin, K.R. The Current Status of Medical Student Urological Education in the United States. J. Urol. 2008, 179, 1087–1091. [Google Scholar] [CrossRef] [PubMed]
- Malde, S.; Shrotri, N. Undergraduate urology in the UK: Does it prepare doctors adequately? Br. J. Med. Surg. Urol. 2012, 5, 20–27. Available online: http://0-journals-sagepub-com.brum.beds.ac.uk/doi/10.1016/j.bjmsu.2011.09.001 (accessed on 23 August 2021). [CrossRef]
- Shah, J.; Billington, R.; Manson, J.; Vale, J. Undergraduate urology: A survey of current provisions and guidelines for a core curriculum. BJU Int. 2002, 89, 327–330. [Google Scholar] [CrossRef]
- Mishail, A.; Shahsavari, M.; Kim, J.; Welliver, R.C.; Vemulapalli, P.; Adler, H.L. Deficits in Urological Knowledge Among Medical Students and Primary Care Providers: Potential for Impact on Urological Care. J. Urol. 2008, 180, 2140–2147. [Google Scholar] [CrossRef] [PubMed]
- Nieder, A.M.; Manoharan, M.; Vyas, S.; Soloway, M.S. 1082: Evaluation and Work-up of Hematuria among Primary Care Physicians in Miami-Dade County: An Anonymous Questionnaire-Based Survey. J. Urol. 2007, 177, 357. [Google Scholar] [CrossRef]
- Bogado, S.J.; Bogado, C.M.; Lopez, C.I.; Rosselot, J.E. The effects of a new model of hospital management on undergraduate teaching of urology. Rev. Med. Chile 2010, 138, 437–443. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/20668791 (accessed on 23 August 2021).
- Thomas, P.A.; Kern, D.E.; Hughes, M.T.; Chen, B.Y. Curriculum Development for Medical Education: A Six-Step Approach. Curriculum Development for Medical Education: A Six-Step Approach, 3rd ed.; JHU Press: Baltimore, MD, USA, 2015. [Google Scholar]
- Kramer, M.; Usher, A. Work-Integrated Learning and Career-Ready Students: Examining the Evidence; Higher Education Strategy Associates: Toronto, ON, Canada, 2011. [Google Scholar]
- Teichman, J.M.; Weiss, B.D.; Solomon, D. Urological needs assessment for primary care practice: Implications for undergraduate medical education. J. Urol. 1999, 161, 1282–1285. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/10081891 (accessed on 23 August 2021). [CrossRef]
- Kerfoot, B.P.; Turek, P.J. What every graduating medical student should know about urology: The stakeholder viewpoint. Urology 2008, 71, 549–553. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/18387383 (accessed on 23 August 2021). [CrossRef]
- Borque Fernando, A.; Romero Fernández, F.J.; Esteban Escaño, L.M.; Sanz Saiz, G.; Gil Sanz, M.J. Moodle_Unizar y el desarrollo de la Asignatura Urología. In Buenas Prácticas en la Docencia Universitaria con Apoyo del TIC: Experiencias en 2013; Alejandre Marco, J.L., Ed.; Prensas de la Universidad de Zaragoza: Zaragoza, Spain, 2013; pp. 177–188. [Google Scholar]
- Fernando, Á.B.; Arellano, Á.A.; Santos, J.M.G.; Dena, F.L.; Aladrén, M.M.; Vera, M.P.G.; María, A.; Corisco, H.; Caballero, M.B.; Boudet, J.M.F.; et al. Una clase accesible para los estudiantes de Ciencias de la Salud. In Buenas Prácticas en la Docencia Universitaria con Apoyo del TIC: Experiencias en 2015; Alejandre Marco, J.L., Ed.; Prensas de la Universidad de Zaragoza: Zaragoza, Spain, 2015; pp. 85–93. [Google Scholar]
- Kerfoot, B.P.; Baker, H.; Volkan, K.; Church, P.A.; Federman, D.D.; Masser, B.A.; DeWOLF, W.C. Development and initial evaluation of a novel urology curriculum for medical students. J. Urol. 2004, 172, 278–281. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/15201794 (accessed on 23 August 2021). [CrossRef]
- Teichman, J.M.; Richards, J. Multimedia to teach urology to medical students. Urology 1999, 53, 267–270. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/9933037 (accessed on 23 August 2021). [CrossRef]
- Elves, A.W.; Ahmed, M.; Abrams, P. Computer-assisted learning; experience at the Bristol Urological Institute in the teaching of urology. Br. J. Urol. 1997, 80 (Suppl. S3), 59–62. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/9415087 (accessed on 23 August 2021).
- Kerfoot, B.P. Interactive spaced education versus web based modules for teaching urology to medical students: A randomized controlled trial. J. Urol. 2008, 179, 2351–2357. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/18423715 (accessed on 23 August 2021). [CrossRef] [PubMed]
- Preece, R. The current role of simulation in urological training. Central Eur. J. Urol. 2015, 68, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Gohil, R.; Khan, R.S.; Ahmed, K.; Kumar, P.; Challacombe, B.; Khan, M.S.; Dasgupta, P. Urology training: Past, present and future. BJU Int. 2012, 109, 1444–1448. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Years of Professional Practice | |
|---|---|
| Mean (CI 95%) | 22.6 years (20.9–24.2 years) |
| Median (P25-P75) | 23 years (15.25–31 years) |
| Min-Max | 3–38 years |
| Sex | |
| Men/Women | 46.5%/53.5% |
| Workspace | |
| Rural/Urban | 28.3%/71.7% |
| Primary Care/Emergency | 85%/15% |
| Associate Professor of Health Sciences | |
| Yes/No | 23.6%/76.4% |
| Theoretical Lessons |
|
| Practical Workshops |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borque-Fernando, Á.; Redondo-Redondo, C.; Orna-Montesinos, C.; Esteban, L.M.; Denizón-Arranz, S.; Tejero-Sánchez, A.; García-Ruiz, R.; Sanchez-Zalabardo, J.M.; Gracia-Romero, J.; Monreal-Híjar, A.; et al. Teaching Urology to Undergraduates: A Prospective Survey of What General Practitioners Need to Know. Int. J. Environ. Res. Public Health 2021, 18, 11687. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111687
Borque-Fernando Á, Redondo-Redondo C, Orna-Montesinos C, Esteban LM, Denizón-Arranz S, Tejero-Sánchez A, García-Ruiz R, Sanchez-Zalabardo JM, Gracia-Romero J, Monreal-Híjar A, et al. Teaching Urology to Undergraduates: A Prospective Survey of What General Practitioners Need to Know. International Journal of Environmental Research and Public Health. 2021; 18(21):11687. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111687
Chicago/Turabian StyleBorque-Fernando, Ángel, Cristina Redondo-Redondo, Concepción Orna-Montesinos, Luis Mariano Esteban, Sophia Denizón-Arranz, Arlanza Tejero-Sánchez, Ramiro García-Ruiz, José Manuel Sanchez-Zalabardo, Jesús Gracia-Romero, Antonio Monreal-Híjar, and et al. 2021. "Teaching Urology to Undergraduates: A Prospective Survey of What General Practitioners Need to Know" International Journal of Environmental Research and Public Health 18, no. 21: 11687. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111687