
The Blood Lead Levels of Children and the Loss of Ca2+ from Neurons Owing to Lead

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Participants
2.3. Animals
2.4. BLL Test
2.5. Follow-Up
2.6. Ca2+ Imaging
2.7. Statistical Analysis
3. Results
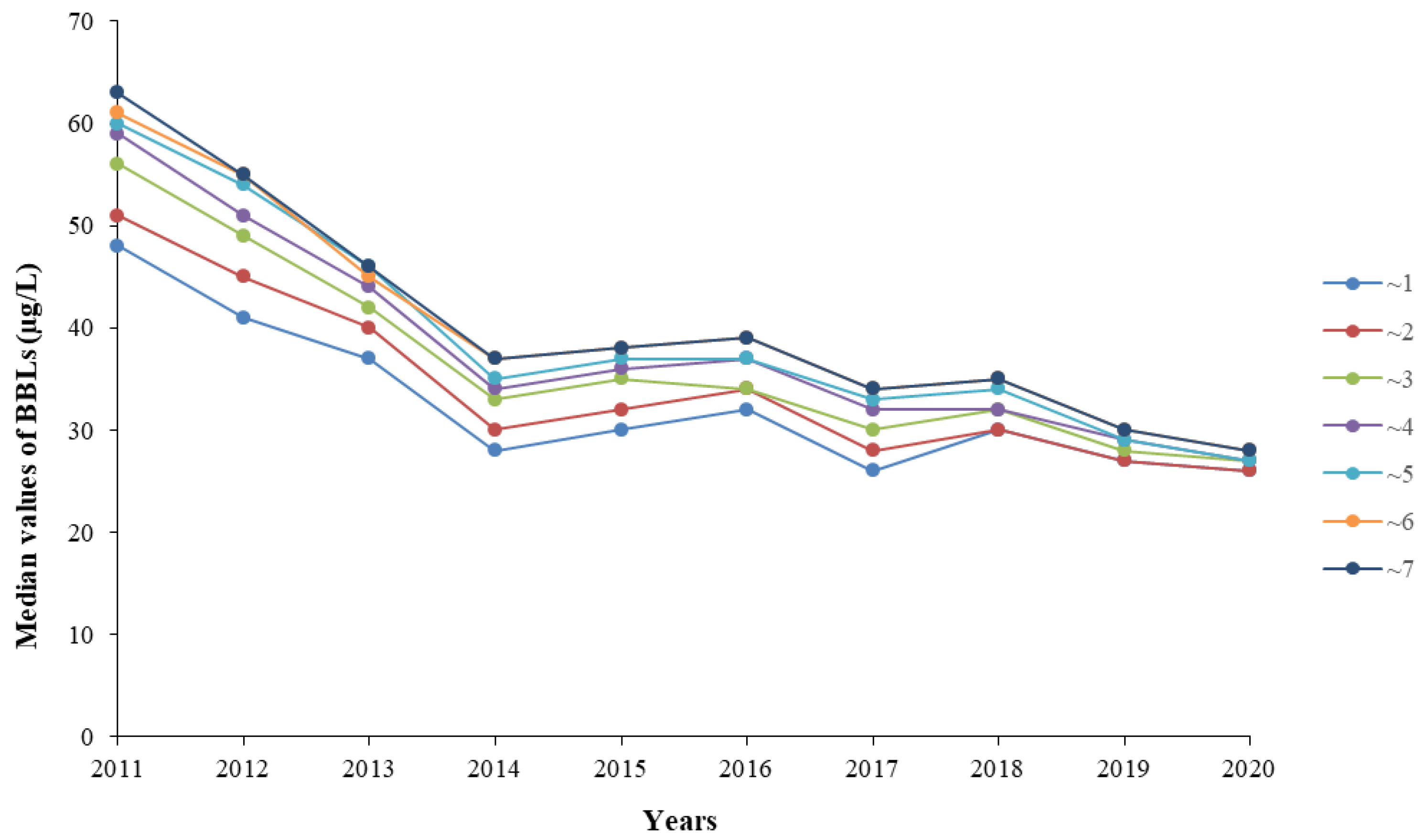
3.1. Median BLL
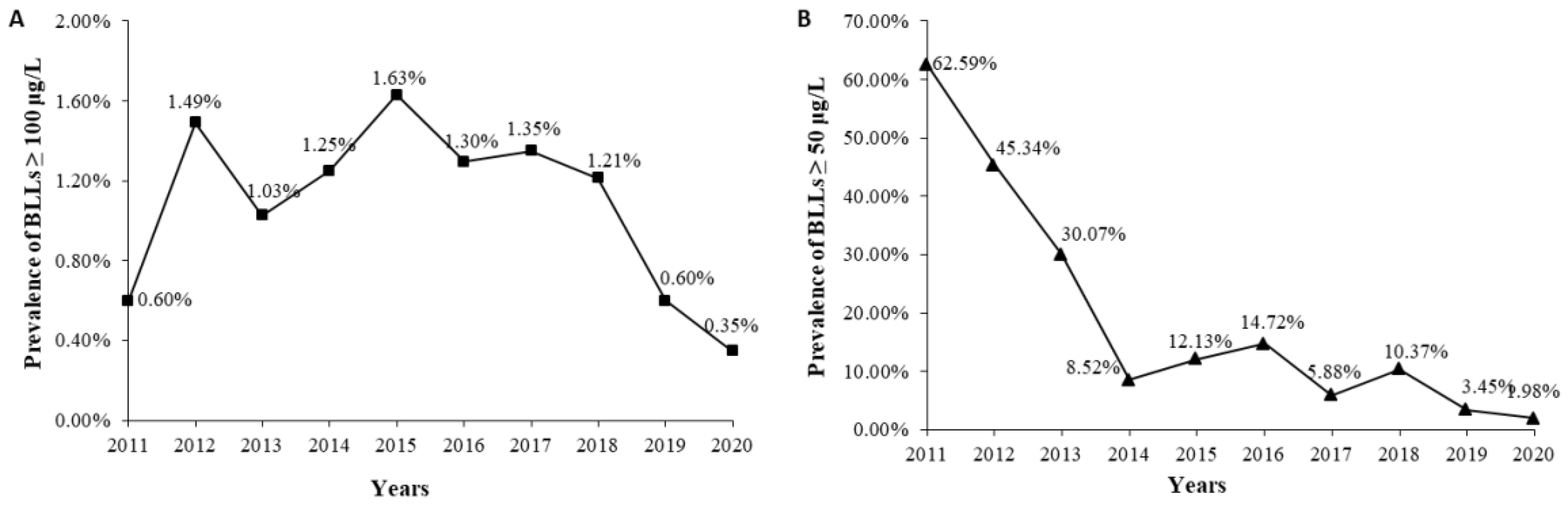
3.2. Elevated BLLs
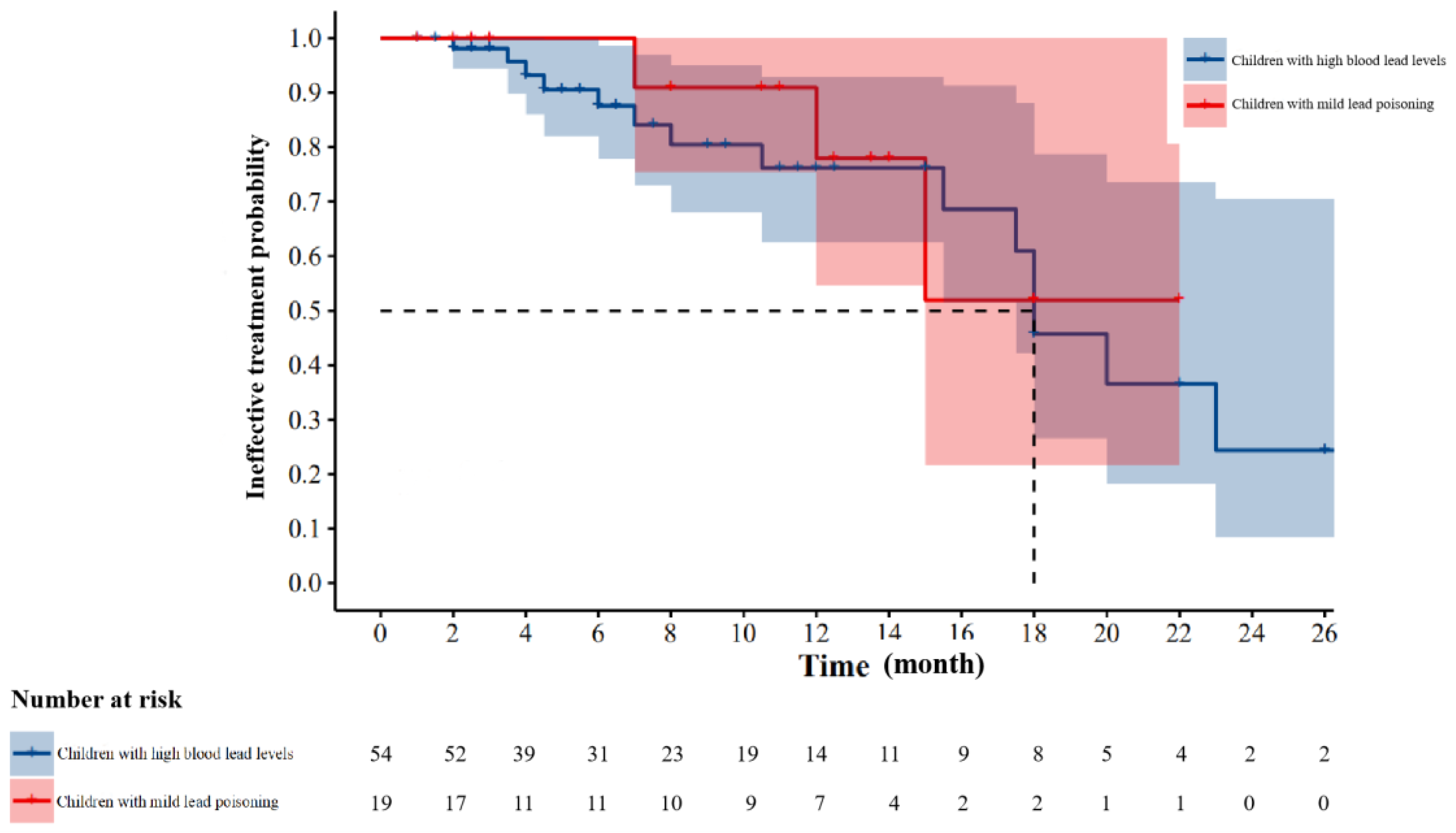
3.3. Treatment Efficiency
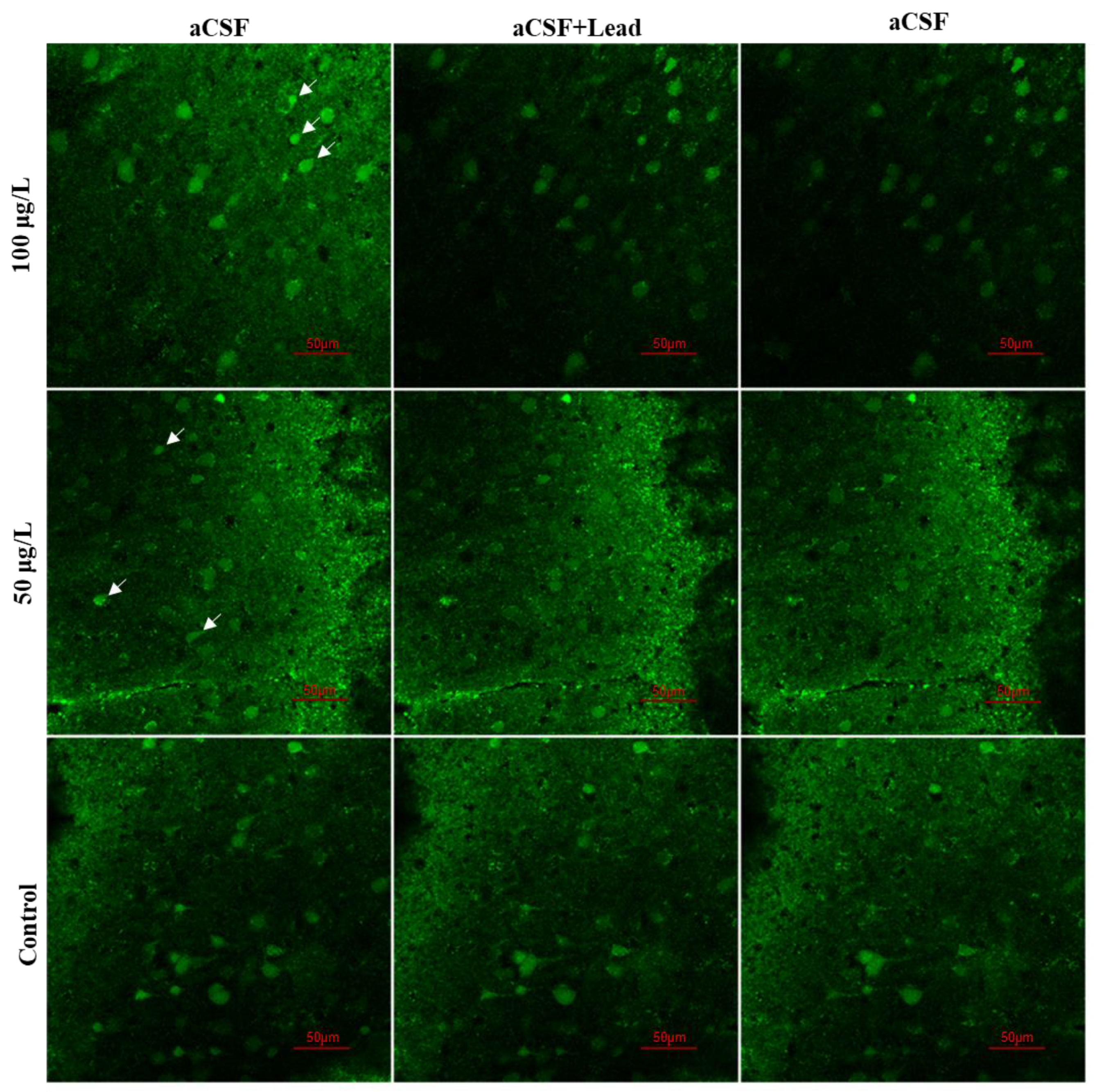
3.4. Lead Exposure Disrupted Ca2+ Signals in Developing Cortical Neurons
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Surkan, P.J.; Zhang, A.; Trachtenberg, F.; Daniel, D.B.; McKinlay, S.; Bellinger, D.C. Neuropsychological function in children with blood lead levels <10 microg/dL. Neurotoxicology 2007, 28, 1170–1177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glenn, B.S.; Bandeen-Roche, K.; Lee, B.K.; Weaver, V.M.; Todd, A.C.; Schwartz, B.S. Changes in systolic blood pressure associated with lead in blood and bone. Epidemiology 2006, 17, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Cleveland, L.M.; Minter, M.L.; Cobb, K.A.; Scott, A.A.; German, V.F. Lead hazards for pregnant women and children: Part 1: Immigrants and the poor shoulder most of the burden of lead exposure in this country. Part 1 of a two-part article details how exposure happens, whom it affects, and the harm it can do. Am. J. Nurs. 2008, 108, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Abadin, H.; Ashizawa, A.; Stevens, Y.W.; Llados, F.; Diamond, G.; Sage, G.; Citra, M.; Quinones, A.; Bosch, S.J.; Swarts, S.G. Agency for Toxic Substances and Disease Registry (ATSDR) Toxicological Profiles. In Toxicological Profile for Lead; Agency for Toxic Substances and Disease Registry (US): Atlanta, GA, USA, 2007. [Google Scholar]
- Bellinger, D.C. Lead neurotoxicity in children: Decomposing the variability in dose-effect relationships. Am. J. Ind. Med. 2007, 50, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Müller, Y.M.; Rivero, L.B.; Carvalho, M.C.; Kobus, K.; Farina, M.; Nazari, E.M. Behavioral impairments related to lead-induced developmental neurotoxicity in chicks. Arch. Toxicol. 2008, 82, 445–451. [Google Scholar] [CrossRef] [PubMed]
- National Health Commission of the People’s Republic of China. The Children Lead Acidosis and Lead Poisoning Prevention Guide and Children’s Blood Lead and Lead Poisoning Classification Principles. Available online: http://www.nhc.gov.cn/wjw/gfxwj/201304/a02eab3564bd46ae8c75645631aafa6d.shtml (accessed on 23 September 2021).
- Centers for Disease Control and Prevention. What Do Parents Need to Know to Protect Their Children? Available online: http://www.cdc.gov/nceh/lead/ACCLPP/blood_lead_levels.htm (accessed on 23 September 2021).
- Bridges, C.C.; Zalups, R.K. Molecular and ionic mimicry and the transport of toxic metals. Toxicol. Appl. Pharmacol. 2005, 204, 274–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouton, C.M.; Frelin, L.P.; Forde, C.E.; Arnold Godwin, H.; Pevsner, J. Synaptotagmin I is a molecular target for lead. J. Neurochem. 2001, 76, 1724–1735. [Google Scholar] [CrossRef] [Green Version]
- Kern, M.; Wisniewski, M.; Cabell, L.; Audesirk, G. Inorganic lead and calcium interact positively in activation of calmodulin. Neurotoxicology 2000, 21, 353–363. [Google Scholar]
- Westerink, R.H.; Klompmakers, A.A.; Westenberg, H.G.; Vijverberg, H.P. Signaling pathways involved in Ca2+- and Pb2+-induced vesicular catecholamine release from rat PC12 cells. Brain Res. 2002, 957, 25–36. [Google Scholar] [CrossRef]
- Sun, Z.; Südhof, T.C. A simple Ca(2+)-imaging approach to neural network analyses in cultured neurons. J. Neurosci. Methods 2021, 349, 109041. [Google Scholar] [CrossRef] [PubMed]
- Garza, A.; Vega, R.; Soto, E. Cellular mechanisms of lead neurotoxicity. Med. Sci. Monit. 2006, 12, Ra57–Ra65. [Google Scholar] [PubMed]
- Raciti, M.; Ceccatelli, S. Epigenetic mechanisms in developmental neurotoxicity. Neurotoxicol. Teratol. 2018, 66, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Green, D.; Sullivan, M.; Cooper, N.; Dean, A.; Marquez, C. A Pilot Study of Children’s Blood Lead Levels in Mount Isa, Queensland. Int. J. Environ. Res. Public Health 2017, 14, 1567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Ding, N.; Tucker, K.L.; Weisskopf, M.G.; Sparrow, D.; Hu, H.; Park, S.K. A Western Diet Pattern Is Associated with Higher Concentrations of Blood and Bone Lead among Middle-Aged and Elderly Men. J. Nutr. 2017, 147, 1374–1383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Wu, S.; Xiang, Y.; Liang, X. An investigation of outpatient children’s blood lead level in Wuhan China. PLoS ONE 2014, 9, e95284. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, A.S.; Leonard, M.L.; Mason, J. CDC’s Lead Poisoning Prevention Program: A Long-standing Responsibility and Commitment to Protect Children From Lead Exposure. J. Public Health Manag. Pract. 2019, 25 (Suppl. S1), S5–S12. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Second Report on Human Biomonitoring of Environmental Chemicals in Canada. Available online: https://www.canada.ca/en/health-canada/services/environmental-workplace-health/reports-publications/environmental-contaminants/second-report-human-biomonitoring-environmental-chemicals-canada-health-canada-2013.html (accessed on 23 September 2021).
- Mathec, A.; Schirnding, Y.V.; Montgomery, M.; Röllin, H. Lead Poisoning in South African Children: The Hazard is at Horne. Rev. Environ. Health 2021, 19, 347–362. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Jiang, Y.M.; Li, J.Y.; Liu, F.; Wang, H.; Yu, F.; Yang, H. Environmental lead exposure among children in Chengdu, China, 2007–2009. Biol. Trace Elem. Res. 2011, 143, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Zhang, J.; Xu, Y. Epigenetic Basis of Lead-Induced Neurological Disorders. Int. J. Environ. Res. Public Health 2020, 17, 4878. [Google Scholar] [CrossRef] [PubMed]
- Florea, A.-M.; Taban, J.; Varghese, E.; Alost, B.T.; Moreno, S.; Büsselberg, D. Lead (Pb2+) neurotoxicity: Ion-mimicry with calcium (Ca2+) impairs synaptic transmission. A review with animated illustrations of the pre- and post-synaptic effects of lead. J. Local Glob. Health Sci. 2013, 2013, 4. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Years | Boy | Girl | p-Value | ||
|---|---|---|---|---|---|
| N | Median (P25–P75) | N | Median (P25–P75) | ||
| 2011 | 4797 | 56 (45–68) | 3525 | 53 (43–65) | <0.001 |
| 2012 | 5818 | 49 (38–61) | 4236 | 46 (36–58) | <0.001 |
| 2013 | 4818 | 42 (34–54) | 3655 | 40 (32–51) | <0.001 |
| 2014 | 4899 | 33 (27–39) | 3661 | 32 (27–38) | <0.001 |
| 2015 | 5031 | 35 (29–42) | 3861 | 34 (28–40) | <0.001 |
| 2016 | 4286 | 36 (30–45) | 3114 | 35 (29–42) | <0.001 |
| 2017 | 4106 | 31 (26–36) | 3000 | 30 (26–36) | <0.001 |
| 2018 | 2800 | 33 (26–40) | 2139 | 32 (26–40) | 0.01 |
| 2019 | 2890 | 29 (25–35) | 1957 | 28 (25–34) | 0.009 |
| 2020 | 4548 | 27 (24–32) | 3221 | 26 (23–31) | <0.001 |
| Total | 43,993 | 36 (28–48) | 32,369 | 35 (28–46) | <0.001 |
| Years | ~1 | ~2 | ~3 | ~4 | ~5 | ~6 | ~7 | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Median (P25–P75) | N | Median (P25–P75) | N | Median (P25–P75) | N | Median (P25–P75) | N | Median (P25–P75) | N | Median (P25–P75) | N | Median (P25–P75) | ||
| 2011 | 1575 | 48 (38–57) | 1726 | 51 (42–62) | 2220 | 56 (45–67) | 901 | 59 (48–70) | 663 | 60 (48–73) | 658 | 61 (50–73) | 579 | 63 (52–76) | <0.001 |
| 2012 | 2210 | 41 (33–51) | 2265 | 45 (36–56) | 2323 | 49 (38–61) | 1065 | 51 (41–64) | 835 | 54 (43–66) | 710 | 55 (44–68) | 646 | 55 (43–68) | <0.001 |
| 2013 | 1834 | 37 (30–46) | 2051 | 40 (31–50) | 1940 | 42 (34–53) | 801 | 44 (35–57) | 686 | 46 (38–57) | 632 | 45 (38–57) | 529 | 46 (39–58) | <0.001 |
| 2014 | 1572 | 28 (24–34) | 1983 | 30 (25–37) | 2173 | 33 (28–39) | 786 | 34 (30–40) | 710 | 35 (31–41) | 732 | 37 (33–42) | 604 | 37 (33–42) | <0.001 |
| 2015 | 1797 | 30 (25–37) | 1918 | 32 (27–39) | 2318 | 35 (29–42) | 884 | 36 (32–44) | 741 | 37 (33–44) | 576 | 38 (33–46) | 658 | 38 (35–47) | <0.001 |
| 2016 | 1275 | 32 (26–39) | 1652 | 34 (28–42) | 2002 | 34 (29–43) | 850 | 37 (31–44) | 588 | 37 (33–47) | 525 | 39 (34–48) | 508 | 39 (34–48) | <0.001 |
| 2017 | 1311 | 26 (23–32) | 1220 | 28 (25–34) | 1767 | 30 (26–36) | 811 | 32 (28–37) | 729 | 33 (29–38) | 673 | 34 (30–39) | 595 | 34 (30–38) | <0.001 |
| 2018 | 740 | 30 (24–37) | 924 | 30 (25–39) | 1260 | 32 (26–39) | 606 | 32 (27–41) | 534 | 34 (28–42) | 464 | 35 (29–43) | 411 | 35 (29–43) | <0.001 |
| 2019 | 592 | 27 (23–32) | 689 | 27 (24–33) | 1131 | 28 (25–34) | 593 | 29 (25–36) | 600 | 29 (26–35) | 600 | 30 (27–36) | 642 | 30 (27–36) | <0.001 |
| 2020 | 1176 | 26 (23–30) | 1119 | 26 (23–30) | 1608 | 27 (24–31) | 915 | 27 (24–32) | 980 | 27 (24–31) | 989 | 28 (25–32) | 982 | 28 (24–33) | <0.001 |
| Total | 14,082 | 32 (26–43) | 15,547 | 34 (27–46) | 18,742 | 36 (28–48) | 8212 | 37 (30–50) | 7066 | 37 (30–49) | 6559 | 38 (30–50) | 6154 | 37 (31–50) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duan, Y.; Shi, H.; Jiang, Y. The Blood Lead Levels of Children and the Loss of Ca2+ from Neurons Owing to Lead. Int. J. Environ. Res. Public Health 2021, 18, 12051. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212051
Duan Y, Shi H, Jiang Y. The Blood Lead Levels of Children and the Loss of Ca2+ from Neurons Owing to Lead. International Journal of Environmental Research and Public Health. 2021; 18(22):12051. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212051
Chicago/Turabian StyleDuan, Yifei, Hua Shi, and Yongmei Jiang. 2021. "The Blood Lead Levels of Children and the Loss of Ca2+ from Neurons Owing to Lead" International Journal of Environmental Research and Public Health 18, no. 22: 12051. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212051