
Building a Research Roadmap for Caregiver Innovation: Findings from a Multi-Stakeholder Consultation and Evaluation


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Description of Our Sample
3.1.1. Caregiver Demographics
3.1.2. Professionals Demographics
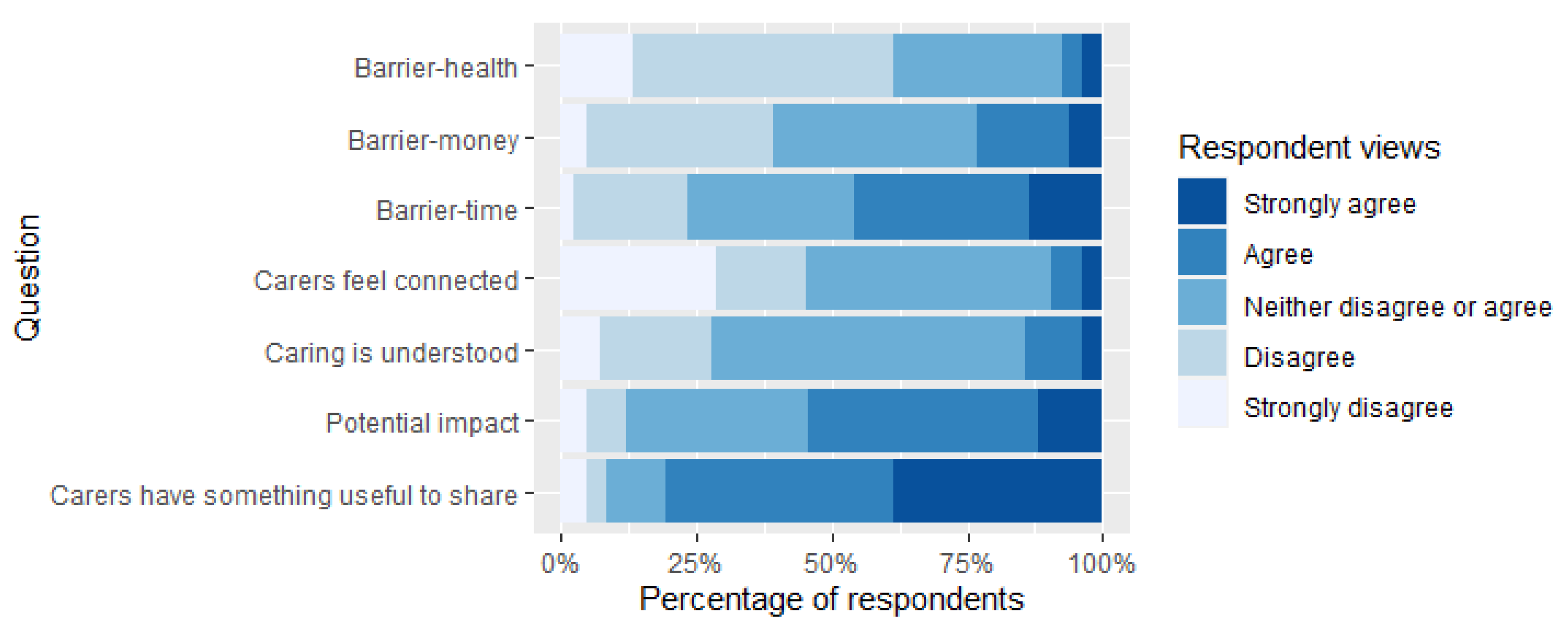
3.2. Views of Informal Caregivers
3.2.1. Previous Caregiver Research Participation
3.2.2. Future Research Participation
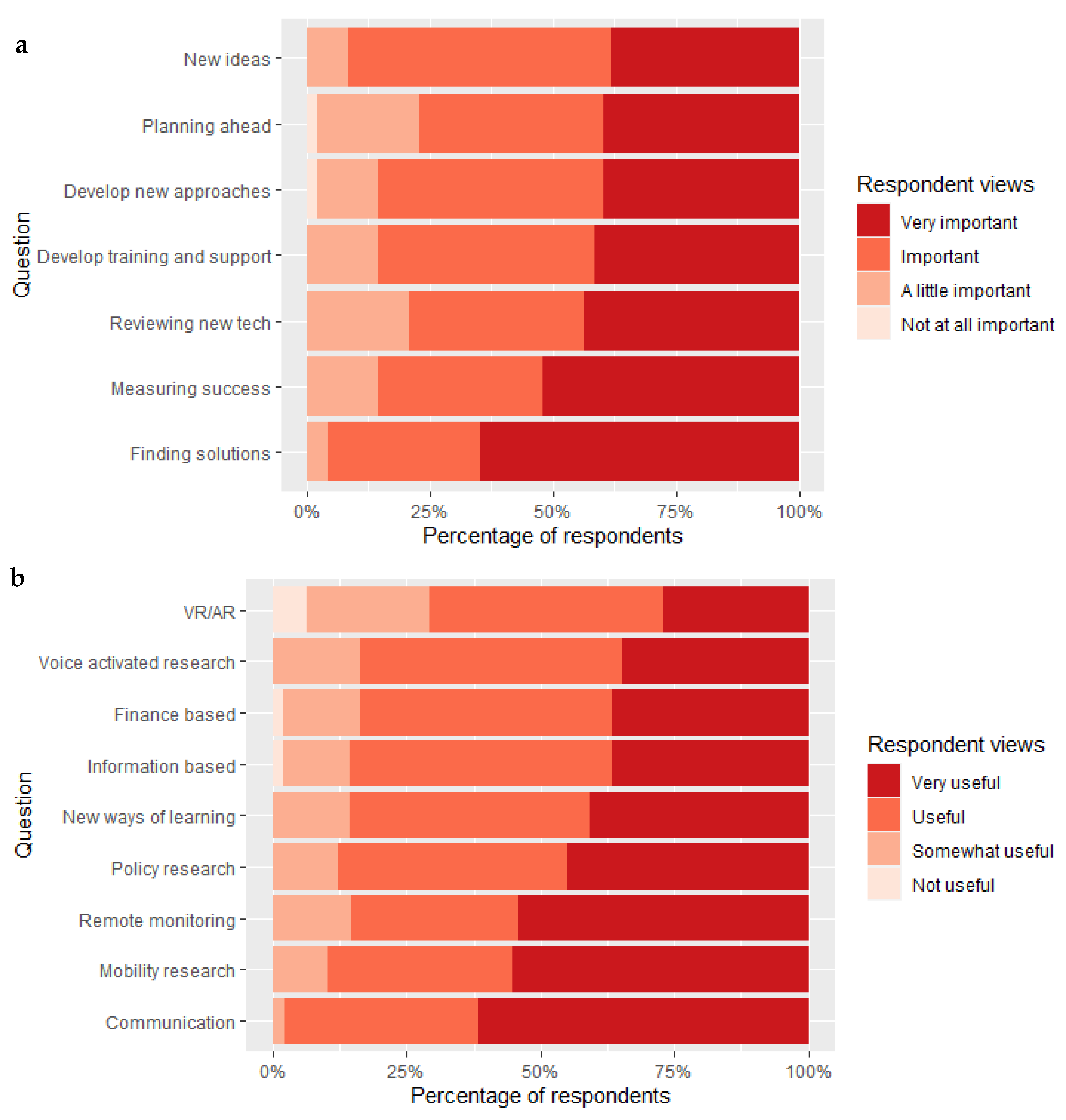
3.2.3. Future Research Aspirations
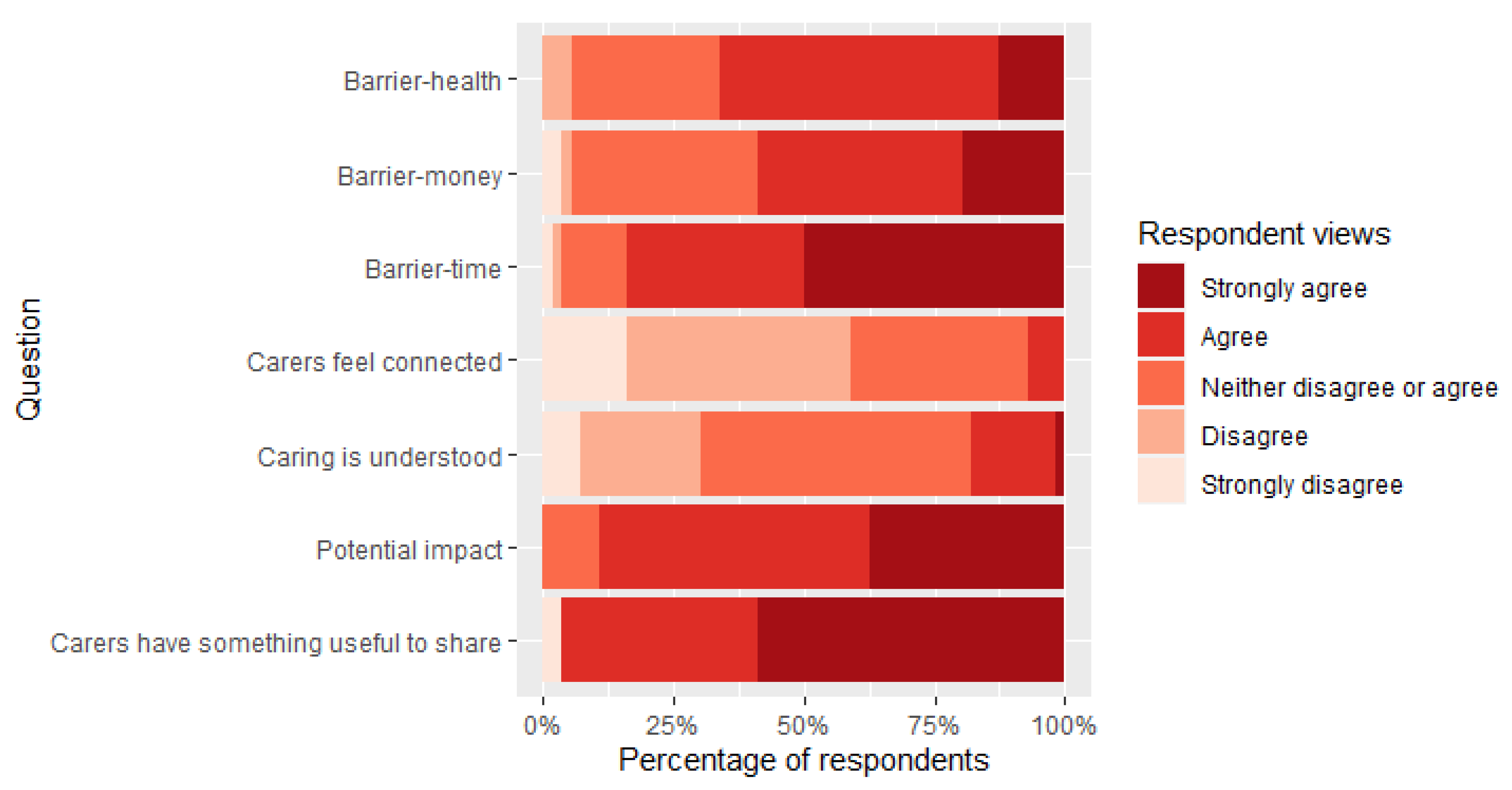
3.3. Professionals
3.3.1. Previous Research Participation
3.3.2. Future Research Participation
3.3.3. Future Research Aspirations
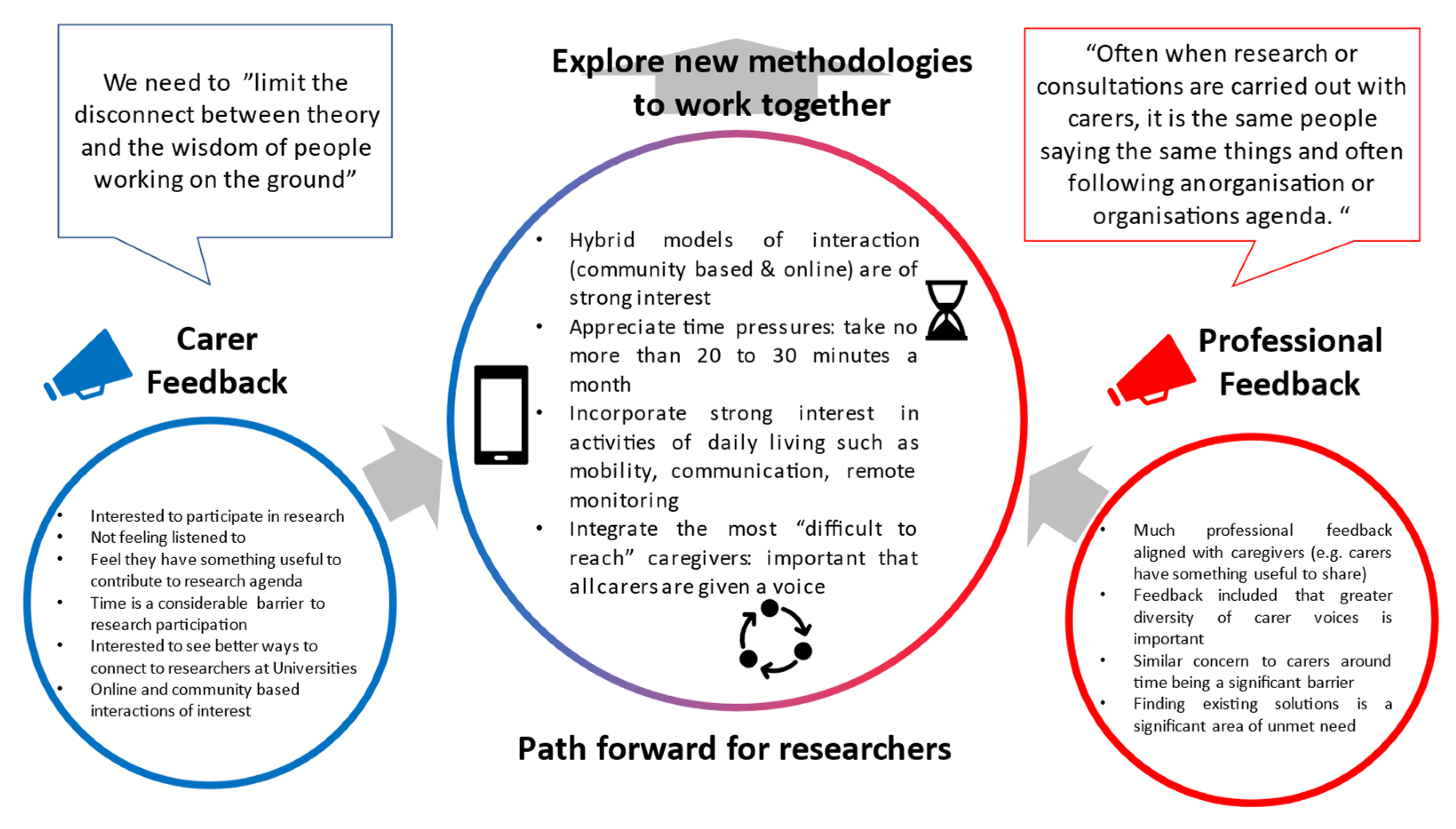
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- 18 to 24 (1)
- 25 to 34 (2)
- 35 to 44 (3)
- 45 to 54 (4)
- 55 to 64 (5)
- 65 to 74 (6)
- 75 to 84 (7)
- 85+ (8)
- Prefer not to say (9)
- Man/Male (including trans man) (1)
- Woman/Female (including trans woman) (2)
- I prefer not to answer (3)
- In another way (4)
- Degree or equivalent (1)
- Higher education (2)
- School qualifications (3)
- Other qualifications (4)
- No qualifications (5)
- Don’t know (6)
- White (1)
- Mixed/multiple ethnic groups (2)
- Asian/Asian British (3)
- Black/African/Caribbean/Black British (4)
- Other ethnic group (5)
- Prefer not to say (6)
- 1 year or less (1)
- Up to 2 years (2)
- Up to 4 years (3)
- Up to 10 years (4)
- 10 years or more (5)
- Yes, caregiving has not affected my working/studying hours (1)
- Yes, caregiving has caused me to reduce my working/studying hours (2)
- Caregiving has caused me to give up work/study (3)
- I do not currently work/study and did not have to give up work/study due to caregiving (4)
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Title | Abbreviation (i.e., in Figure) |
|---|---|
| Question group: To what extent do you support the following statements | |
| I feel connected to researchers working at universities | I feel connected |
| I feel that researchers working in universities have a good understanding of the challenges of being a carer | Caring is understood |
| My experience (including as a carer) means that I have something useful to share with researchers working within universities | I have something useful to share |
| The work that researchers in universities do could make a significant impact on my health and wellness as a carer | Potential impact |
| Time is a significant barrier for me to become involved in research | Barrier—time |
| Money is a significant barrier for me to become involved in research | Barrier—money |
| My health is a significant barrier for me to become involved in research | Barrier—health |
| Question group: Where do you think your input as a carer is most important for researchers working in universities? | |
| Developing new ideas | New ideas |
| Reviewing new technology ideas in development (e.g., using a star rating) | Reviewing new tech |
| Developing new approaches to work together (e.g., improving the way researchers connect with carers) | Develop new approach |
| Developing training and support materials for development of new ideas | Develop training & support |
| Helping to decide how to measure the success of technologies (e.g., understanding what matters to you most) | Measure success |
| Making sure that other carers can find new solutions relevant to them | Finding solutions |
| Working with researchers in universities long term to plan ahead | Planning ahead |
| Other | Other |
| Question group: In your view, what areas of collaboration with universities would make the biggest impact on your own health and wellness? | |
| Information based technology research (e.g., research that shares key information around caring, your rights, entitlements etc.) | Information-based |
| Finance based research (e.g., innovations/applications that would help you manage any finance activities, including reminders or notifications) | Finance-based |
| Voice activated technology research (e.g., Alexa, Siri or other voice based technologies) | Voice activated research |
| Virtual reality/Augmented reality research (e.g., through the use of mobile phones or more specialised equipment) | VR/AR |
| Mobility research (e.g., any technologies that help within the home or getting out an about such as wheelchairs) | Mobility research |
| Research on technologies for remote monitoring (e.g., looking after someone at distance through self reported measures) | Remote monitoring |
| Communication technologies (e.g solutions to help you connect to other caregivers or professionals) | Communication |
| Policy related research (e.g., gathering evidence to help shape national agendas and priorities) | Policy research |
| Research into new/innovative ways of learning (e.g., online learning) | New ways of learning |
| Other | Other |
| To what extent do you support the following statements | |
| Carers are connected to researchers working at universities | I feel connected |
| Researchers working in universities have a good understanding of the challenges of being a carer | Caring is understood |
| Carer experience is something useful to share with researchers working within universities | Carers have something useful to share |
| The work that researchers in universities do could make a significant impact on carer health and wellness | Potential impact |
| Time is a significant barrier for carers to become involved in research | Barrier—time |
| Money is a significant barrier for carers to become involved in research | Barrier—money |
| Poor carer health is a significant barrier for carers to become involved in research | Barrier—health |
| Where do you think your input is most important for researchers working in universities to develop new ideas/solutions for carers? | |
| Developing new ideas | New ideas |
| Reviewing new technology ideas in development (e.g., using a star rating) | Reviewing new tech |
| Developing new approaches to work together (e.g., improving the way researchers connect with carers) | Develop new approach |
| Developing training and support materials for development of new ideas | Develop training & support |
| Helping to decide how to measure the success of technologies (e.g., understanding what matters to you most) | Measure success |
| Making sure that carers can find new solutions relevant to them | Finding solutions |
| Working with researchers in universities long term to plan ahead | Planning ahead |
| Other | Other |
| If you were to work with a carers in research on a regular basis, what technologies/innovations or areas of work do you think would make the biggest impact on carers own health and wellness? | |
| Information based technology research (e.g., research that shares key information around caring, your rights, entitlements etc.) | Information-based |
| Finance based research (e.g., innovations/applications that would help you manage any finance activities, including reminders or notifications) | Finance-based |
| Voice activated technology research (e.g., Alexa, Siri or other voice based technologies) | Voice activated research |
| Virtual reality/Augmented reality research (e.g., through the use of mobile phones or more specialised equipment) | VR/AR |
| Mobility research (e.g., any technologies that help within the home or getting out an about such as wheelchairs) | Mobility research |
| Research on technologies for remote monitoring (e.g., looking after someone at distance through self reported measures) | Remote monitoring |
| Communication technologies (e.g., solutions to help you connect to other caregivers or professionals) | Communication |
| Policy related research (e.g., gathering evidence to help shape national agendas and priorities) | Policy research |
| Research into new/innovative ways of learning (e.g., online learning) | New ways of learning |
| Other | Other |
References
- Carers UK. Missing out, the Identification Challenge. 2016. Available online: https://www.carersuk.org/for-professionals/policy/policy-library/missing-out-the-identification-challenge (accessed on 2 June 2021).
- Hoffmann, F.; Rodrigues, R. Informal Carers: Who Takes Care of Them? Policy Brief 4/2010. Vienna: European Centre for Social Welfare and Policy Research. 2010. Available online: https://www.euro.centre.org/publications/detail/387 (accessed on 2 June 2021).
- Maynard, A. Shrinking the state: The fate of the NHS and social care. J. R. Soc. Med. 2017, 110, 49–51. [Google Scholar] [CrossRef] [Green Version]
- Pristavec, T. The burden and benefits of caregiving: A latent class analysis. Gerontologist 2019, 59, 1078–1091. [Google Scholar] [CrossRef] [PubMed]
- Stansfeld, S.; Smuk, M.; Onwumere, J.; Clark, C.; Pike, C.; McManus, S.; Harris, J.; Bebbington, P. Stressors and common mental disorder in informal carers—An analysis of the English Adult Psychiatric Morbidity Survey 2007. Soc. Sci. Med. 2014, 120, 190–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metzelthin, S.F.; Verbakel, E.; Veenstra, M.Y.; van Exel, J.; Ambergen, A.W.; Kempen, G.I.J.M. Positive and negative outcomes of informal caregiving at home and in institutionalised long-term care: A cross-sectional study. BMC Geriatr. 2017, 17, 232. [Google Scholar] [CrossRef]
- del-Pino-Casado, R.; Priego-Cubero, E.; López-Martínez, C.; Orgeta, V. Subjective caregiver burden and anxiety in informal caregivers: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0247143. [Google Scholar] [CrossRef] [PubMed]
- Egan, K. Digital technology, health and wellbeing and the COVID-19 pandemic: It′s time to call forward informal carers from the back of the queue. Semin. Oncol. Nurs. 2020, 36, 151088. [Google Scholar] [CrossRef]
- Ewing, G.; Austin, L.; Jones, D.; Grande, G. Who cares for the carers at hospital discharge at the end of life? A qualitative study of current practice in discharge planning and the potential value of using The Carer Support Needs Assessment Tool (CSNAT) Approach. Palliat. Med. 2018, 32, 939–949. [Google Scholar] [CrossRef] [Green Version]
- Egan, K.J.; Pinto-Bruno, Á.C.; Bighelli, I.; Berg-Weger, M.; van Straten, A.; Albanese, E.; Pot, A.M. Online training and support programs designed to improve mental health and reduce burden among caregivers of people with dementia: A systematic review. J. Am. Med. Dir. Assoc. 2018, 19, 200–206.e201. [Google Scholar] [CrossRef]
- Shin, J.Y.; Choi, S.W. Online interventions geared toward increasing resilience and reducing distress in family caregivers. Curr. Opin. Supportive Palliat. Care 2020, 14, 60–66. [Google Scholar] [CrossRef]
- Pot, A.M.; Gallagher-Thompson, D.; Xiao, L.D.; Willemse, B.M.; Rosier, I.; Mehta, K.M.; Zandi, D.; Dua, T.; iSupport Development Team. iSupport: A WHO global online intervention for informal caregivers of people with dementia. World Psychiatry 2019, 18, 365–366. [Google Scholar] [CrossRef] [Green Version]
- Pham, Q.; El-Dassouki, N.; Lohani, R.; Jebanesan, A.; Young, K. The future of virtual care for older ethnic adults beyond COVID-19. arXiv 2021. preprint. [Google Scholar]
- James, T.; Mukadam, N.; Sommerlad, A.; Guerra Ceballos, S.; Livingston, G. Culturally tailored therapeutic interventions for people affected by dementia: A systematic review and new conceptual model. Lancet Healthy Longev. 2021, 2, e171–e179. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Wherton, J.; Papoutsi, C.; Lynch, J.; Hughes, G.; A′Court, C.; Hinder, S.; Fahy, N.; Procter, R.; Shaw, S. Beyond adoption: A new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. J. Med. Internet Res. 2017, 19, e367. [Google Scholar] [CrossRef] [Green Version]
- WHO. Global Strategy on Digital Health 2020–2025; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Lindeman, D.A.; Kim, K.K.; Gladstone, C.; Apesoa-Varano, E.C. Technology and caregiving: Emerging interventions and directions for research. Gerontologist 2020, 60 (Suppl. 1), S41–S49. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Decade of Healthy Ageing: Baseline Report; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- NHS Digital. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/personal-social-services-survey-of-adult-carers/england-2018-19 (accessed on 19 August 2021).
- Kim, J.; Kim, Y.; Jang, H.; Cho, M.; Lee, M.; Kim, J.; Lee, H. Living labs for health: An integrative literature review. Eur. J. Public Health 2019, 30, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Archibald, M.M.; Wittmeier, K.; Gale, M.; Ricci, F.; Russell, K.; Woodgate, R.L. Living labs for patient engagement and knowledge exchange: An exploratory sequential mixed methods study to develop a living lab in paediatric rehabilitation. BMJ Open 2021, 11, e041530. [Google Scholar] [CrossRef]
- Verbeek, H.; Zwakhalen, S.M.G.; Schols, J.; Kempen, G.; Hamers, J.P.H. The living lab in ageing and long-term care: A sustainable model for translational research improving quality of life, quality of care and quality of work. J. Nutr. Health Aging 2020, 24, 43–47. [Google Scholar] [CrossRef] [Green Version]
- van den Kieboom, R.C.; Bongers, I.M.; Mark, R.E.; Snaphaan, L.J. User-driven living lab for assistive technology to support people with dementia living at home: Protocol for developing co-creation-based innovations. JMIR Res. Protoc. 2019, 8, e10952. [Google Scholar] [CrossRef]
- Okop, K.J.; Murphy, K.; Lambert, E.V.; Kedir, K.; Getachew, H.; Howe, R.; Niyibizi, J.B.; Ntawuyirushintege, S.; Bavuma, C.; Rulisa, S.; et al. Community-driven citizen science approach to explore cardiovascular disease risk perception, and develop prevention advocacy strategies in sub-Saharan Africa: A programme protocol. Res. Involv. Engagem. 2021, 7, 11. [Google Scholar] [CrossRef]
- Sanders, E.B.N.; Stappers, P.J. Co-creation and the new landscapes of design. CoDesign 2008, 4, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Interaction Design Website. Making Your UX Life Easier with the MoSCoW. Available online: https://www.interaction-design.org/literature/article/making-your-ux-life-easier-with-the-moscow (accessed on 19 August 2021).
- Staniszewska, S.; Brett, J.; Simera, I.; Seers, K.; Mockford, C.; Goodlad, S.; Altman, D.G.; Moher, D.; Barber, R.; Denegri, S.; et al. GRIPP2 reporting checklists: Tools to improve reporting of patient and public involvement in research. BMJ 2017, 358, j3453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egan, K.J. A national U.K. survey to understand current needs and future expectations of informal caregivers for technology to support health and wellbeing. JMIR Aging 2021, in press. [Google Scholar] [CrossRef]
- Graffigna, G.; Gheduzzi, E.; Morelli, N.; Barello, S.; Corbo, M.; Ginex, V.; Ferrari, R.; Lascioli, A.; Feriti, C.; Masella, C. Place4Carers: A multi-method participatory study to co-design, piloting, and transferring a novel psycho-social service for engaging family caregivers in remote rural settings. BMC Health Serv. Res. 2021, 21, 591. [Google Scholar] [CrossRef] [PubMed]
- Enzenbach, C.; Wicklein, B.; Wirkner, K.; Loeffler, M. Evaluating selection bias in a population-based cohort study with low baseline participation: The life-adult-study. BMC Med Res. Methodol. 2019, 19, 135. [Google Scholar] [CrossRef]
- Veselkov, K.; Gonzalez, G.; Aljifri, S.; Galea, D.; Mirnezami, R.; Youssef, J.; Bronstein, M.; Laponogov, I. HyperFoods: Machine intelligent mapping of cancer-beating molecules in foods. Sci. Rep. 2019, 9, 9237. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- O′Connor, S.; Bouamrane, M.M.; O′Donnell, C.A.; Mair, F.S. Barriers to co-designing mobile technology with persons with dementia and their carers. Stud. Health Technol. Inform. 2016, 225, 1028–1029. [Google Scholar]





| Variable | Group | Caregivers (n= 112, [%]) | Professionals (n = 62 *, [%]) |
|---|---|---|---|
| Age Group | 18 to 24 | 0 [0%] | 0 [0%] |
| 25 to 34 | 4 [3.6%] | 16 [26%] | |
| 35 to 44 | 21 [18.8%] | 13 [21%] | |
| 45 to 54 | 47 [42%] | 22 [35%] | |
| 55 to 64 | 30 [26.8%] | 11 [18%] | |
| 65 to 74 | 7 [6.3%] | 0 [0%] | |
| 75 to 84 | 2 [1.8%] | 0 [0%] | |
| Prefer not to say | 1 [0.9%] | 0 [0%] | |
| Gender | Man/Male (including trans man) | 12 [10.7%] | 13 [21%] |
| Woman/Female (including trans woman) | 96 [85.7%] | 48 [79%] | |
| In another way | 2 [1.8%] | 0 [0%] | |
| I prefer not to answer | 2 [1.8%] | 0 [0%] | |
| Ethnicity | White | 111 [99.1%] | 58 [94%] |
| Asian/Asian British | 0 | 2 [3%] | |
| Other ethnic group | 0 | 2 [3%] | |
| Mixed/multiple ethnic groups | 1 [0.9%] | 0 [0%] | |
| Education level | Degree or equivalent | 68 [60.7%] | 46 [74%] |
| Higher education | 27 [24.1%] | 10 [16%] | |
| Other qualifications | 5 [4.5%] | 5 [8%] | |
| School qualifications | 10 [8.9%] | 1 [2%] | |
| No qualifications | 2 [1.8%] | 0 [0%] |
| Key Theme | Sub-Theme | Example Quote (s) |
|---|---|---|
| 1. Previous research participation | 1.1. Experience and connection to research/ers | The research facilitated access to [a] psychologist and assessment whilst [I was] awaiting CAHMS appointments |
| 1.2. Barriers | I always found great difficulty finding the time with all other responsibilities, however, feel it would have been good opportunity, but struggle with other commitments to find time | |
| 2. Future research participation | 2.1. Value of the input from caregivers | It is important to have your voice heard to give an accurate picture of caring and carers |
| 2.2. Methods of participation | Face-to-face is always preferred to build meaningful relationship. Online is next best thing and personally I would be reluctant for the final two options [telephone and post] as [it’s] difficult to engage | |
| 2.3. Time available for participation | There needs to be a balance between the time commitment and the formation of a relationship between the carer and the researcher | |
| 3. Future research aspirations | 3.1. Innovative technology | The use of remote technology so that carers don’t worry or have to be with the person as much |
| 3.2. Improved support for carers | Give carers a voice and some real support, there are many of us who are unpaid and dedicate ourselves to our person whilst struggling with life ourselves Please help us be less invisible in our communities. Please help us help the person we love and care for to be less invisible in our communities. | |
| 3.3. Impact on policy | Shaping government agenda is probably where change is mostly required |
| Key Theme | Sub-Theme | Example Quote |
|---|---|---|
| 1. Previous research participation | 1.1. Experience and connection to Research/ers | I feel obligated to take part since we need more attention on the work we do as carers. |
| 1.2. Interest in research | Think it is really important to gather information from all walks of life and people who are doing the work at ground level and not people sitting in offices that are not meeting clients and families on a daily basis. | |
| 1.3. Barriers | Time is my main commodity. | |
| 2. Future research participation | 2.1. Methods of participation | Carers have little time for themselves, so it would make sense to provide ways in which they could contribute with their experiences at a convenient time. They are exhausted day by day so asking them to go somewhere or receiving people at home is uncomfortable and burdensome for them. |
| 2.2. Involving hard to reach stakeholders | Often when research or consultations are carried out with carers, it is the same people saying the same things and often following an organisation or organisation’s agenda. Would suggest there is value in speaking with carers who haven’t been supported by carer organisations. | |
| 3. Future research aspirations | 3.1. Innovative technology | Technology for monitoring care for persons when they have memory issues that can give the carer peace of mind…Having a life outside of caring, maybe tracking what the carer is doing and encouraging them to take a break where possible. |
| 3.2. Training and support for Carers | Training and peer support is currently a massive challenge and services are currently looking to move as much as possible onto online platforms. To find the best possible solutions to help people manage their own well-being as carers, which will impact on those they care for. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Egan, K.J.; McMillan, K.A.; Lennon, M.; McCann, L.; Maguire, R. Building a Research Roadmap for Caregiver Innovation: Findings from a Multi-Stakeholder Consultation and Evaluation. Int. J. Environ. Res. Public Health 2021, 18, 12291. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312291
Egan KJ, McMillan KA, Lennon M, McCann L, Maguire R. Building a Research Roadmap for Caregiver Innovation: Findings from a Multi-Stakeholder Consultation and Evaluation. International Journal of Environmental Research and Public Health. 2021; 18(23):12291. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312291
Chicago/Turabian StyleEgan, Kieren J., Kathryn A. McMillan, Marilyn Lennon, Lisa McCann, and Roma Maguire. 2021. "Building a Research Roadmap for Caregiver Innovation: Findings from a Multi-Stakeholder Consultation and Evaluation" International Journal of Environmental Research and Public Health 18, no. 23: 12291. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312291