
Challenges of Using Instant Communication Technology in the Emergency Department during the COVID-19 Pandemic: A Focus Group Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
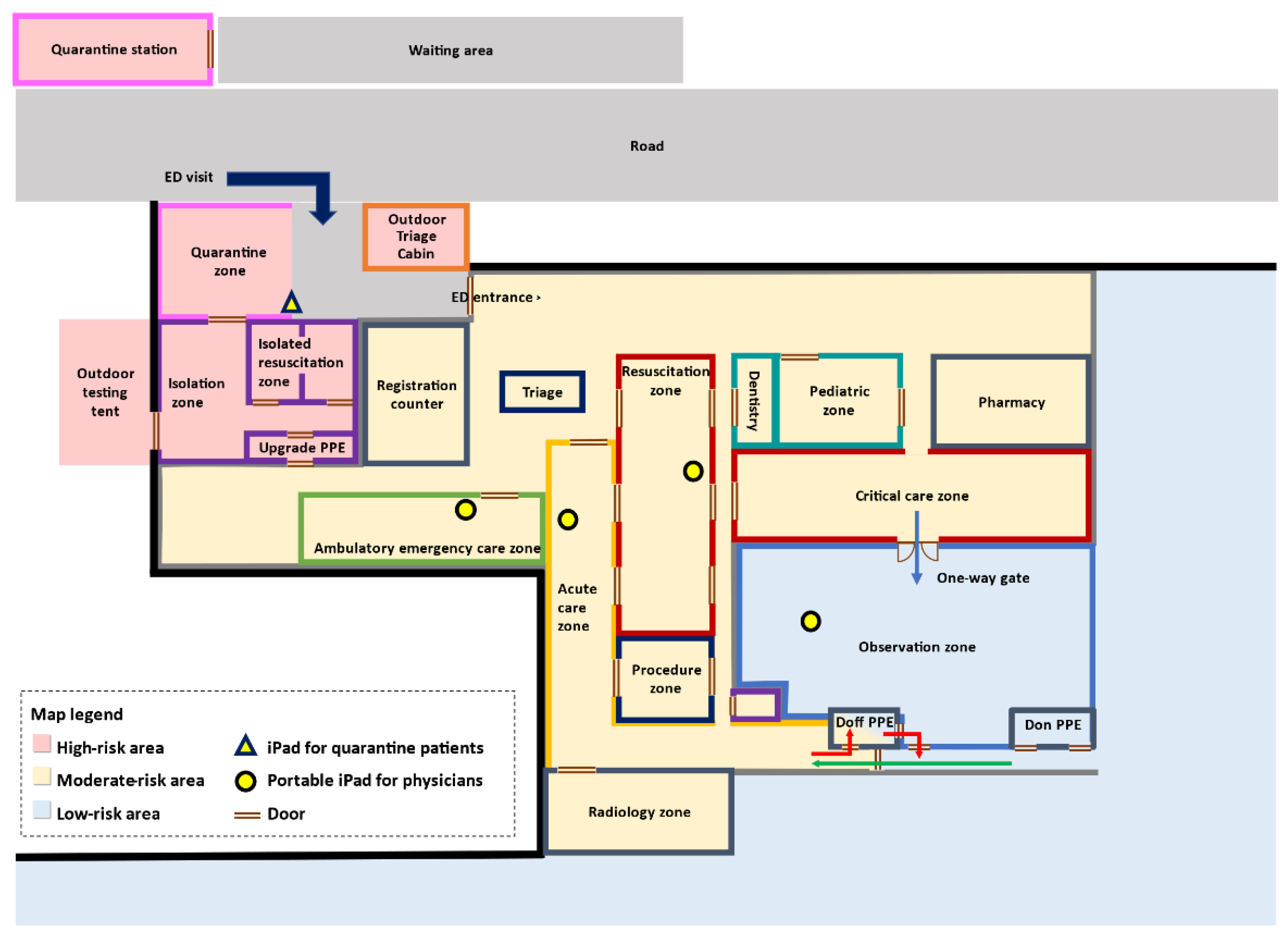
2.2. Regionalization within the ED
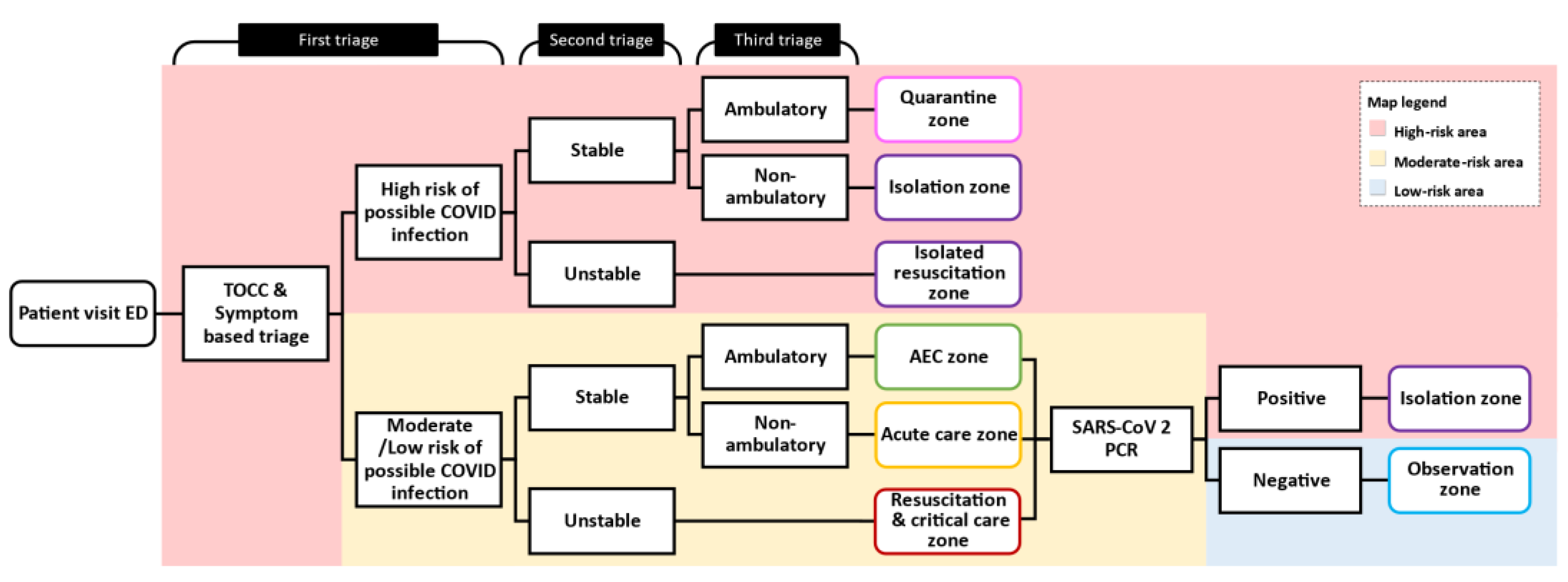
2.3. Patient Flow and the Diversion Protocol
2.4. The ICT Module
2.5. Focus Group Study
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ED | Emergency department |
| ICT | Instant communication technology |
| PCR | polymerase chain reaction |
| PPE | personal protection equipment |
| TOCC | travel, occupation, contact, and cluster |
Appendix A. The Interview Guide
- Do you have experience on using the ICT to communicate with other people?
- If yes, what are the obstacles on using the ICT?
- What are the major factors influencing the usage of the ICT?
- What are the software and hardware you will use with the ICT to facilitate communications?
- What are the factors that would influence your selection of these software and/or hardware?
- Do you have any experience on using the ICT to communicate with your patience in hospitals?
- If yes, what are the major factors contribute to the usage of the ICT in the field of Emergency Medicine (EM).
- If yes, what are the obstacles on using the ICT in the field of EM.
- If yes, what are the pros and cons of using the ICT in the field of EM during the COVID-19 pandemic?
- Anything you think should be improved to better using the ICT in the field of EM during this pandemic?
- From your perspectives, how does the ICT contribute to the communication between physicians and patients?
References
- Lin, C.-H.; Hsieh, C.-C.; Chi, C.-H. Hospital Emergency Management of Emerging Infectious Disease using Instant Communication Technology. Prehospital Disaster Med. 2020, 35, 465–466. [Google Scholar] [CrossRef]
- Friedman, J.; Lame, M.; Clark, S.; Gogia, K.; Platt, S.L.; Kim, J.W. Telemedicine Medical Screening Evaluation Expedites the Initiation of Emergency Care for Children. Pediatr. Emerg. Care 2021, 37, e417–e420. [Google Scholar] [CrossRef]
- Fang, J.; Liu, Y.T.; Lee, E.Y.; Yadav, K. Telehealth Solutions for In-hospital Communication with Patients Under Isolation during COVID-19. West. J. Emerg. Med. 2020, 21, 801–806. [Google Scholar] [CrossRef]
- Li, J.-P.O.; Thomas, A.A.; Kilduff, C.L.; Logeswaran, A.; Ramessur, R.; Jaselsky, A.; Sim, D.A.; Hay, G.R.; Thomas, P.B. Safety of video-based telemedicine compared to in-person triage in emergency ophthalmology during COVID-19. EClinicalMedicine 2021, 34, 100818. [Google Scholar] [CrossRef] [PubMed]
- Wittbold, K.A.; Baugh, J.J.; Yun, B.J.; Raja, A.S.; White, B.A. iPad deployment for virtual evaluation in the emergency department during the COVID-19 pandemic. Am. J. Emerg. Med. 2020, 38, 2733–2734. [Google Scholar] [CrossRef]
- Lowe, J.; Shen, S. Off the Shelf: Rapid Deployment of an Emergency Department Telemedicine Platform Using Readily Available Consumer Products. J. Emerg. Med. 2020, 59, 726–729. [Google Scholar] [CrossRef]
- Sabırlı, R.; Karsli, E.; Canacik, O.; Ercin, D.; Çiftçi, H.; Sahin, L.; Dolanbay, T.; Tutuncu, E.E. Use of WhatsApp for Polyclinic Consultation of Suspected Patients With COVID-19: Retrospective Case Control Study. JMIR mHealth uHealth 2020, 8, e22874. [Google Scholar] [CrossRef] [PubMed]
- AlShaya, M.; Assery, M.K.; Pani, S.C. Reliability of mobile phone teledentistry in dental diagnosis and treatment planning in mixed dentition. J. Telemed. Telecare 2020, 26, 45–52. [Google Scholar] [CrossRef]
- Siddiqui, J.; Herchline, T.; Kahlon, S.; Moyer, K.J.; Scott, J.D.; Wood, B.R.; Young, J. Infectious Diseases Society of America Position Statement on Telehealth and Telemedicine as Applied to the Practice of Infectious Diseases. Clin. Infect. Dis. 2017, 64, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, N.R.; Steinberg, A.; Arnold, R.M.; Doshi, A.A.; White, D.B.; DeLair, W.; Nigra, K.; Elmer, J. Perspectives on Telephone and Video Communication in the Intensive Care Unit during COVID-19. Ann. Am. Thorac. Soc. 2021, 18, 838–847. [Google Scholar] [CrossRef]
- Candel, B.G.J.; Vaes, S.M.M.; van Bree, E.M.; Groenen, S.M.A.; Derkx, F.; Mignot, L.A.A.; de Groot, B. Telemedicine in the emergency department to decrease personal protective equipment use: A before-and-after study. Emerg. Med. J. 2021, 38, 224–228. [Google Scholar] [CrossRef]
- Domingues, R.B.; Mantese, C.E.; Aquino, E.D.S.; Fantini, F.G.M.M.; Prado, G.F.D.; Nitrini, R. Telemedicine in neurology: Current evidence. Arq. Neuro-Psiquiatr. 2020, 78, 818–826. [Google Scholar] [CrossRef]
- Makhni, M.C.; Riew, G.J.; Sumathipala, M.G. Telemedicine in Orthopaedic Surgery. J. Bone Jt. Surg. Am. Vol. 2020, 102, 1109–1115. [Google Scholar] [CrossRef]
- Chau, M.J.; Quintero, J.E.; Guiliani, A.; Hines, T.; Samaan, C.; Seybold, K.; Stowe, M.; Hanlon, D.; Gerhardth, G.A.; van Horne, C.G. Telehealth Sustainability in a Neurosurgery Department During the COVID-19 Pandemic. World Neurosurg. 2021, 152, e617–e624. [Google Scholar] [CrossRef] [PubMed]
- Villa, L.; Matz, O.; Dague, K.O.; Kluwig, D.; Rossaint, R.; Brokmann, J.C. The assessment of dermatological emergencies in the emergency department via telemedicine is safe: A prospective pilot study. Intern. Emerg. Med. 2020, 15, 1275–1279. [Google Scholar] [CrossRef] [PubMed]
- Flint, L.; Kotwal, A. The New Normal: Key Considerations for Effective Serious Illness Communication Over Video or Telephone During the Coronavirus Disease 2019 (COVID-19) Pandemic. Ann. Intern. Med. 2020, 173, 486–488. [Google Scholar] [CrossRef]
- Fenn, D.; Coppel, J.; Kearney, J.; Everson, L.; Braithwaite, S.; Chodhari, R. Walkie talkies to aid health care workers’ compliance with personal protective equipment in the fight against COVID-19. Crit. Care 2020, 24, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Alhajri, N.; Simsekler, M.C.E.; Alfalasi, B.; Alhashmi, M.; AlGhatrif, M.; Balalaa, N.; Al Ali, M.; Almaashari, R.; Al Memari, S.; Al Hosani, F.; et al. Physicians’ Attitudes Toward Telemedicine Consultations During the COVID-19 Pandemic: Cross-sectional Study. JMIR Med. Inform. 2021, 9, e29251. [Google Scholar] [CrossRef] [PubMed]
- Wilhite, J.A.; Altshuler, L.; Fisher, H.; Gillespie, C.; Hanley, K.; Goldberg, E.; Wallach, A.; Zabar, S. The Telemedicine Takeover: Lessons Learned During an Emerging Pandemic. Telemed. e-Health 2021. [Google Scholar] [CrossRef]
- Hammersley, V.; Donaghy, E.; Parker, R.; McNeilly, H.; Atherton, H.; Bikker, A.; Campbell, J.; McKinstry, B. Comparing the content and quality of video, telephone, and face-to-face consultations: A non-randomised, quasi-experimental, exploratory study in UK primary care. Br. J. Gen. Pr. 2019, 69, e595–e604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boissin, C.; Blom, L.; Wallis, L.; Laflamme, L. Image-based teleconsultation using smartphones or tablets: Qualitative assessment of medical experts. Emerg. Med. J. 2017, 34, 95–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iyengar, K.; Upadhyaya, G.K.; Vaishya, R.; Jain, V. COVID-19 and applications of smartphone technology in the current pandemic. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 733–737. [Google Scholar] [CrossRef] [PubMed]
- Saleem, J.J.; Savoy, A.; Etherton, G.; Herout, J. Investigating the need for clinicians to use tablet computers with a newly envisioned electronic health record. Int. J. Med. Inform. 2018, 110, 25–30. [Google Scholar] [CrossRef] [Green Version]
- Horng, S.; Goss, F.R.; Chen, R.S.; Nathanson, L.A. Prospective pilot study of a tablet computer in an Emergency Department. Int. J. Med. Inform. 2012, 81, 314–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mickan, S.; Atherton, H.; Roberts, N.W.; Heneghan, C.; Tilson, J.K. Use of handheld computers in clinical practice: A systematic review. BMC Med. Inform. Decis. Mak. 2014, 14, 56. [Google Scholar] [CrossRef] [Green Version]
- Kaczmarek, B.F.; Trinh, Q.-D.; Menon, M.; Rogers, C.G. Tablet Telerounding. Urology 2012, 80, 1383–1388. [Google Scholar] [CrossRef]
- Hamm, J.M.; Greene, C.; Sweeney, M.; Mohammadie, S.; Thompson, L.B.; Wallace, E.; Schrading, W. Telemedicine in the emergency department in the era of COVID-19: Front-line experiences from 2 institutions. J. Am. Coll. Emerg. Physicians Open 2020, 1, 1630–1636. [Google Scholar] [CrossRef]
- Legler, S.; Diehl, M.; Hilliard, B.; Olson, A.; Markowitz, R.; Tignanelli, C.; Melton, G.B.; Broccard, A.; Kirsch, J.; Usher, M. Evaluation of an Intrahospital Telemedicine Program for Patients Admitted With COVID-19: Mixed Methods Study. J. Med. Internet Res. 2021, 23, e25987. [Google Scholar] [CrossRef]
- Berg, B.; Lune, H. Qualitative Research Methods for the Social Scientists; Pearson Education, Inc.: Hoboken, NJ, USA, 2012. [Google Scholar]
- Creswell, J.W.; Poth, C.N. Qualitative Inquiry and Research Design: Choosing Among Five Approaches; Sage Publications: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Patton, M.Q. Qualitative Research and Evaluation Methods, 3rd ed.; Sage Publications: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- Mansell, I.; Bennett, G.; Northway, R.; Mead, D.; Moseley, L. The learning curve: The advantages and disadvantages in the use of focus groups as a method of data collection. Nurse Res. 2004, 11, 79–88. [Google Scholar] [CrossRef]
- Grbich, C. Qualitative Data Analysis: An. Introduction, 2nd ed.; Sage Publication Ltd.: London, UK, 2013. [Google Scholar]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of healthcare interventions: An overview of reviews and development of a theoretical framework. BMC Health Serv. Res. 2017, 17, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Cynthia, S. Franklin PACMB. Reliability and validity in qualitative research. In The Handbook of Social Work Research Methods, 2nd ed.; Thyer, B.A., Ed.; Sage Publication Inc.: London, UK, 2010; pp. 355–374. [Google Scholar]
- Teter, C.M.; Whitted, K.; Vardaman, S.A. Reducing Hospital Visit Rates in Hospice Patients Using Telemedicine. CIN Comput. Inform. Nurs. 2021, 39, 682–688. [Google Scholar] [CrossRef]
- Flodgren, G.; Rachas, A.; Farmer, A.J.; Inzitari, M.; Shepperd, S. Interactive telemedicine: Effects on professional practice and health care outcomes. Cochrane Database Syst. Rev. 2015, 2015, CD002098. [Google Scholar] [CrossRef] [PubMed]
- Avest, E.T.; Lambert, E.; De Coverly, R.; Tucker, H.; Griggs, J.; Wilson, M.H.; Ghorbangholi, A.; Williams, J.; Lyon, R.M. Live video footage from scene to aid helicopter emergency medical service dispatch: A feasibility study. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apple.com. How to Clean Your Apple Products. Available online: https://support.apple.com/en-us/HT204172 (accessed on 16 June 2021).
- Annaswamy, T.M.; Verduzco-Gutierrez, M.; Frieden, L. Telemedicine barriers and challenges for persons with disabilities: COVID-19 and beyond. Disabil. Health J. 2020, 13, 100973. [Google Scholar] [CrossRef]
- Foley, G.; Timonen, V. Using Grounded Theory Method to Capture and Analyze Health Care Experiences. Health Serv. Res. 2014, 50, 1195–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Theme: Setting | |
|---|---|
| Factors | Considerations |
| Patient evaluation | Patient identity should be verified through electronic, paper-based, or virtual registry systems. |
| Patients with mild symptoms are suitable for the use of instant communication technology (ICT) in the emergency department (ED). The door-to-patient-evaluation time and the length of ED stay could be reduced. | |
| ICT is useful in history taking and general appearance assessment. Emergency physicians were less comfortable performing physical examinations using ICT. Nevertheless, certain physical examinations could be omitted to avoid direct contact. | |
| Clinical information could be collected from patient families and caregivers who were restricted from entering the ED due to hospital policy. | |
| The use of ICT could be challenging for disabled patients or those who had language barriers. | |
| Consultation with subspecialty | ICT is acceptable for certain consultations with subspecialties, especially when the clinical judgment is largely based on verbal discussion, such as history taking or shared decision-making. |
| The interpretation of imaging studies is generally acceptable. | |
| The visual evaluation of skin lesions is acceptable sometimes. | |
| Patient privacy and comfortableness | Shelters or booths may be provided to protect patient privacy. |
| The surrounding light should be adjusted to achieve better visualization of the screen image. | |
| The environment should be well ventilated, with the temperature and moisture monitored. | |
| Sanitation | Non-contact- or motion-activated communication applications should be considered to lessen the risk of contact infection. |
| A disposable material for activation of applications on tablets with touch screens could be used. | |
| Most tablet computers can be sanitized using 70% isopropyl alcohol wipes. Aerosol sprays, bleaches, abrasives, or direct-spray cleaners are usually unacceptable. Moisture should be kept out of any opening. One of the simplest ways is to place the tablet into a sealed plastic bag and regularly sanitize the outer surface of the bag with medical alcohol. | |
| Cost | The potential costs included those for technology teams, hardware, software, Wi-Fi or internet connection, etc. To offset these, the cost of PPE could be significantly reduced. |
| The regulations on health insurance reimbursement should be clarified. | |
| Registration for and utilization of instant communication applications may have membership fees. | |
| Patient acceptability | Patient characteristics may be associated with patient acceptability of telemedicine evaluation. We observed that patients who were younger or were using smartphones were more comfortable receiving ICT evaluation. |
| We were unsure whether using instant communication applications, compared with traditional face-to-face interviews, would affect the physician-patient rapport. | |
| The familiarity of the ICT evaluation system among working personnel may have an impact on patient acceptability. | |
| Theme: Hardware | |
|---|---|
| Factors | Considerations |
| Wi-Fi/internet connection | A stable, low-cost, wide-bandwidth, high-quality internet connection is essential. |
| Using Wi-Fi, rather than a fixed internet connection mode, is more practical for the mobile setting of instant communication technology (ICT) evaluation. | |
| Power | The tablets should have a reasonable sustainable source of power for the high usage of instant communication applications. Power that will last for at least one workload shift (usually 12 h) is ideal. |
| Extra power-recharging devices should be available. | |
| Image and voice quality | Adequate color presentation, image resolution and size, and voice quality were paramount for patient assessment when using ICT. |
| The device should have high-resolution cameras to provide video and image quality. Tablets with built-in front and back cameras were preferred, to enable switching between users. | |
| The loudness of the voice should be adjustable to provide adequate audio ability and patient privacy. | |
| Public/personal modes | Some health providers may be unwilling to use personal devices as tools for the ICT assessment of emergency patients. A disrupted boundary of professional and personal lives was the major concern. |
| Portable/fixed modes | When the zoning or regionalization of the emergency department is well set up, a fixed model of patient assessment using ICT is generally feasible. |
| Portable devices may be suitable for discussions for shared decision-making, especially when the emergency department is overcrowded. However, portable devices may require more maintenance since they are vulnerable to frequent usage. | |
| Maintenance | The cost and resources needed for maintenance should be preplanned. |
| Theme: Software | |
|---|---|
| Factors | Considerations |
| Platform choices | Instant communication applications work on certain platforms; for example, FaceTime is generally for iOS, while LINE is cross-platform. The choice of applications and platforms should be based on the overall design of the telemedicine system that will use instant communication technology (ICT). |
| Security | Cybersecurity is important for patient evaluation, so the utilization of ICTs and internet connections should be carefully examined. The risks of personal information breaches were a concern. |
| The security upgrades and updates of ICT should be checked regularly. | |
| End-to-end encryption may provide better protection of conversations between devices. The content of calls may be retrieved and stored on the servers of ICT applications, so the policies of the ICT software should be clarified. | |
| ICT accounts | A single account of emergency department, rather than personal accounts, for each device was preferable. |
| Each device may need an individual account for identification. | |
| Interview modes | Instant communication applications that support both one-on-one interviews and chat rooms are preferred. Group chatting is useful for consultations that involve multiple subspecialists, team resource management, or patient family meetings for clinical decision-making. |
| Video/voice recording | Health insurance reimbursement may require video/voice recording of the patient assessment. |
| The recording materials may play an important role when conflicts are encountered, especially medical-legal issues. The accessibility and security control of the storage material should be strictly regulated. | |
| The storage of video/voice recording requires significant storage space and cost. | |
| Time limitation | Instant communication applications may have time limitations for each call. Extension of the call duration may require additional cost to upgrade the application. |
| Time limitations may facilitate the efficiency of patient assessment but should be well communicated between the physician and the patient in advance. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, Y.-S.; Lu, C.-H.; Chiu, P.-W.; Chang, H.-C.; Lin, Y.-Y.; Huang, S.-P.; Wang, P.-Y.; Chen, C.-J.; Lin, I.-C.; Tang, J.-S.; et al. Challenges of Using Instant Communication Technology in the Emergency Department during the COVID-19 Pandemic: A Focus Group Study. Int. J. Environ. Res. Public Health 2021, 18, 12463. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312463
Kuo Y-S, Lu C-H, Chiu P-W, Chang H-C, Lin Y-Y, Huang S-P, Wang P-Y, Chen C-J, Lin I-C, Tang J-S, et al. Challenges of Using Instant Communication Technology in the Emergency Department during the COVID-19 Pandemic: A Focus Group Study. International Journal of Environmental Research and Public Health. 2021; 18(23):12463. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312463
Chicago/Turabian StyleKuo, Yuh-Shin, Chien-Hsin Lu, Po-Wei Chiu, Hung-Chieh Chang, Yu-Yuan Lin, Shao-Peng Huang, Pei-Yu Wang, Cheng-Jen Chen, I-Chen Lin, Jing-Shia Tang, and et al. 2021. "Challenges of Using Instant Communication Technology in the Emergency Department during the COVID-19 Pandemic: A Focus Group Study" International Journal of Environmental Research and Public Health 18, no. 23: 12463. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312463