
The Relevance of Insomnia in the Diagnosis of Perinatal Depression: Validation of the Italian Version of the Insomnia Symptom Questionnaire


 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Setting
2.2. Participants
3. Procedure and Measures
- Perinatal Interview (PI) is a paper-and-pencil questionnaire to collect sociodemographic and clinical information, allowing us to investigate predictive and protective factors for the development of psychiatric disorders. Besides place and date of birth, nationality, educational level, job, and marital status, the PI investigates habits (i.e., eating, drinking, and weight control), voluptuary substance use (including coffee, tobacco, and alcohol), physiological rhythms (i.e., time to go to sleep, waking time, and sleeping hours), past surgery, past and current pharmacological treatment, gynecological and obstetric history, focusing on the current and past pregnancies, past and current personal and family psychiatric history and any psychiatric treatment, stressful life events, partner and family/friends’ support during pregnancy, and partner data.
- The Pittsburgh Sleep Quality Index (PSQI) [27,28] is a retrospective self-report questionnaire that measures sleep quality and disturbances over the previous month. The PSQI assesses seven clinically derived components of subjective sleep quality: 1. sleep quality, 2. sleep latency, 3. sleep duration, 4. habitual sleep efficiency, 5. sleep disturbance, 6. use of sleep medications, and 7. daytime dysfunction. The PSQI yields a global score that represents the sum of the seven component scores that are rated on a 4-point Likert scale ranging from 0 to 3, where 3 reflects the negative extreme of the Likert scale. A global score of 5 or higher is considered as an indicator of prominent sleep disturbance in at least two components or of moderate difficulties in more than three components, distinguishing between “good” and “bad” sleepers. In the Italian validation study [28], the PSQI showed high internal consistency with a Cronbach’s alpha of 0.84.
- The Edinburgh Postnatal Depression Scale (EPDS) [33] is a 10-item self-report questionnaire administered to screen for depressive symptoms in both the antenatal and postnatal periods [34,35]. We used the recommended score of 13 or more that indicates probable major depression in postnatal Italian-speaking women [36]. In the Italian validation study, the EPDS showed good internal consistency with a Cronbach’s alpha of 0.79.
- The Zung Self-Rating Anxiety Scale (SAS) [37] is a 20-item self-report assessment tool built to measure state anxiety levels. Raw scores range from 20 to 80. The initial cutoff was 50 [38], but the best cutoff was later proposed to be 40 for clinical settings and 36 for screening purposes [39]. The instrument is suited to investigate anxiety disorders and showed strong correlations with other similar instruments [40,41]. In this study, we used the Italian version [42].
- The Hypomania CheckList-32 (HCL-32) [43] is a 32-item self-rating questionnaire investigating the lifetime history of hypomanic symptoms. Individuals scoring ≥ 14 potentially have bipolar disorder/diathesis and should be carefully interviewed. The ideal cutoff point of the Italian version is 12, with a sensitivity of 0.85 and a specificity of 0.61 [44].
- The Temperament Evaluation of the Memphis, Pisa, Paris and San Diego-Autoquestionnaire (TEMPS-A) [45], is a 110 item yes-or-no self-report questionnaire designed to assess affective temperament in psychiatric and healthy subjects. It consists of five temperament traits, i.e., depressive (D), cyclothymic (C), hyperthymic (H), irritable (I), and anxious (A). The prevailing temperament is considered the one on which the completer obtains the higher score. We used the validated Italian version [46].
- Insomnia Symptom Questionnaire (ISQ) [31] is a 13-item self-report instrument designed to assess respondents’ perceptions about their daytime functioning, nighttime sleep, and identify insomnia. The ISQ items are based on DSM-IV criteria for primary insomnia [2] and are consistent with the American Academy of Sleep Medicine’s (AASM) Research Diagnostic Criteria (RDC) [47]. Items 1, 2, or 5 (example item: During the past month did you have difficulties falling asleep?) are used to determine the presence, frequency, and duration of sleep symptom criteria (example: How long did the symptom last?; example answer: # weeks/months/years) and are rated on a 6-point Likert scale, ranging from 0 (never) to 5 (always/5–7 times a week). Items 6–13 are used to identify significant daytime consequences of the sleep complaint (example item: During the past month have your sleep difficulties affected your work?) and are rated on a 5-point Likert scale, ranging from 0 (not at all) to 4 (extremely). The final outcome of the ISQ is obtained through a dichotomous response (yes/no) to the three sleep criteria (sleep symptom criterion items 1, 2, or 5; duration criterion items 1, 2, or 5; daytime impairment criterion items 6–13), which results in the “presence” (3 yes answer) or “absence” of insomnia. In the validation study [31], the ISQ obtained a Cronbach’s alpha of 0.89, indicating a high degree of internal consistency. In our sample, the ISQ obtained a Cronbach’s alpha of 0.92, showing comparable if not higher internal consistency.The Italian translation of the ISQ was carried out through a direct and reverse translation process [48]. Specifically, a bilingual Italian/English psychiatrist translated the ISQ from English to Italian. Subsequently, another bilingual Italian/English researcher back-translated the scale.
4. Data Analyses
5. Results
5.1. Descriptive Statistics
5.1.1. No-Insomnia Sample
5.1.2. Insomnia Sample
5.2. Criterion Validity of the ISQ
5.3. Reliability Statistic and Test–Retest Reliability
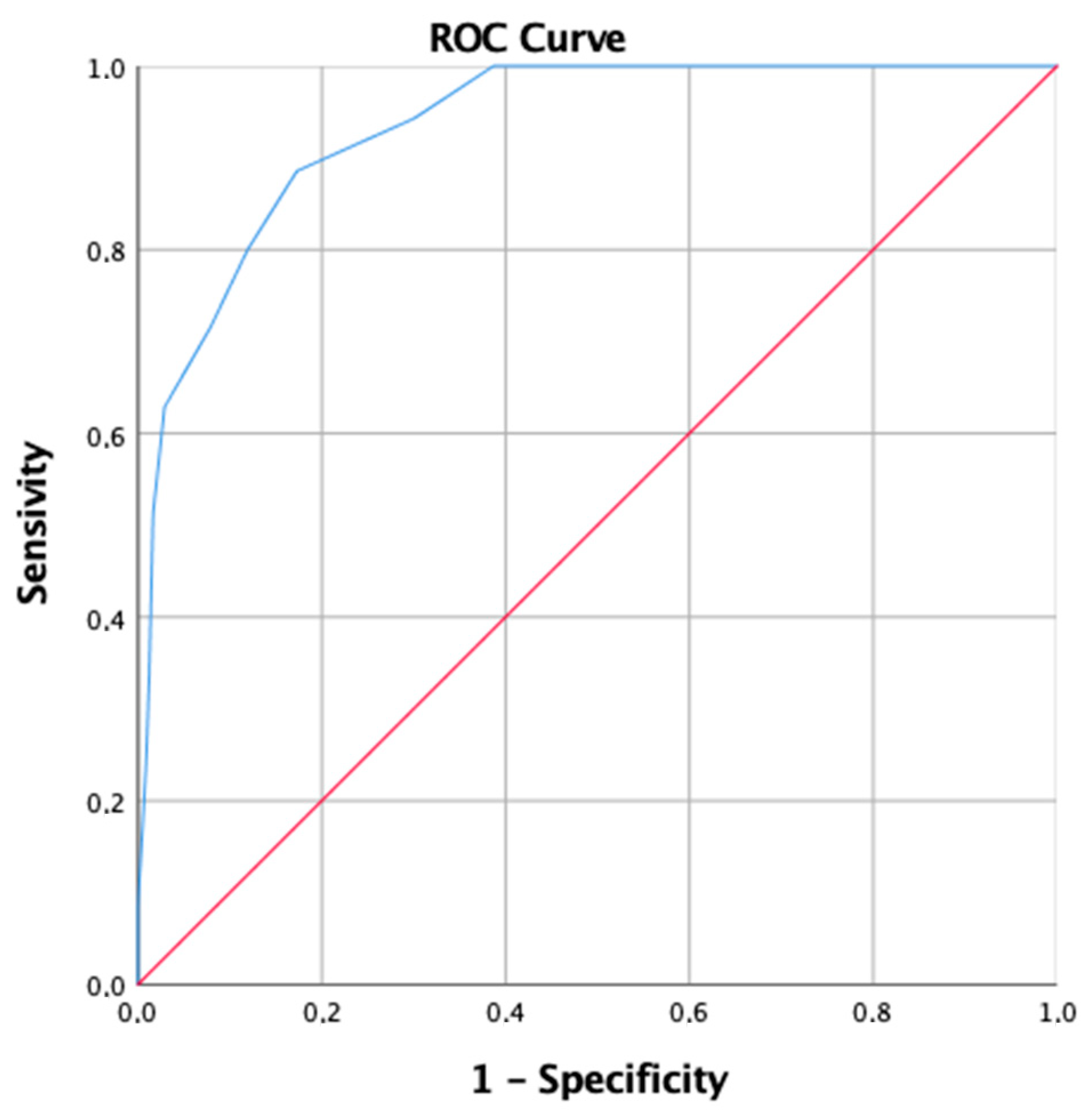
Screening Accuracy of the ISQ
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: Fifth Edition (DSM-5), 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR), 4th ed.; American Psychiatric Association: Arlington, VA, USA, 2000; Volume 1, ISBN 9780890423349. [Google Scholar]
- International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine (Ed.) American Academy of Sleep Medicine: Darien, IL, USA, 2014; ISBN 9780991543410. [Google Scholar]
- Lee, K.A. Alterations in sleep during pregnancy and postpartum: A review of 30 years of research. Sleep Med. Rev. 1998, 2, 231–242. [Google Scholar] [CrossRef]
- Mindell, J.A.; Cook, R.A.; Nikolovski, J. Sleep patterns and sleep disturbances across pregnancy. Sleep Med. 2015, 16, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Tomfohr, L.M.; Buliga, E.; Letourneau, N.L.; Campbell, T.S.; Giesbrecht, G.F. Trajectories of Sleep Quality and Associations with Mood during the Perinatal Period. Sleep 2015, 38, 1237–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plancoulaine, S.; Flori, S.; Bat-Pitault, F.; Patural, H.; Lin, J.-S.; Franco, P. Sleep Trajectories among Pregnant Women and the Impact on Outcomes: A Population-Based Cohort Study. Matern. Child Health J. 2017, 21, 1139–1146. [Google Scholar] [CrossRef] [Green Version]
- Sedov, I.D.; Cameron, E.E.; Madigan, S.; Tomfohr-Madsen, L.M. Sleep quality during pregnancy: A meta-analysis. Sleep Med. Rev. 2017, 38, 168–176. [Google Scholar] [CrossRef]
- Sedov, I.D.; Anderson, N.J.; Dhillon, A.K.; Tomfohr-Madsen, L.M. Insomnia symptoms during pregnancy: A meta-analysis. J. Sleep Res. 2020, 30, e13207. [Google Scholar] [CrossRef] [PubMed]
- Tochikubo, O.; Ikeda, A.; Miyajima, E.; Ishii, M. Effects of Insufficient Sleep on Blood Pressure Monitored by a New Multibiomedical Recorder. Hypertension 1996, 27, 1318–1324. [Google Scholar] [CrossRef] [PubMed]
- Otchet, F. General health and psychological symptom status in pregnancy and the puerperium: What is normal? Obstet. Gynecol. 1999, 94, 935–941. [Google Scholar] [CrossRef]
- Koukopoulos, A.; Mazza, C.; De Chiara, L.; Sani, G.; Simonetti, A.; Kotzalidis, G.D.; Armani, G.; Callovini, G.; Bonito, M.; Parmigiani, G.; et al. Psychometric Properties of the Perinatal Anxiety Screening Scale Administered to Italian Women in the Perinatal Period. Front. Psychiatry 2021, 12, 684579. [Google Scholar] [CrossRef]
- Kamysheva, E.; Skouteris, H.; Wertheim, E.H.; Paxton, S.J.; Milgrom, J. A prospective investigation of the relationships among sleep quality, physical symptoms, and depressive symptoms during pregnancy. J. Affect. Disord. 2010, 123, 317–320. [Google Scholar] [CrossRef]
- Hertenstein, E.; Feige, B.; Gmeiner, T.; Kienzler, C.; Spiegelhalder, K.; Johann, A.; Jansson-Fröjmark, M.; Palagini, L.; Rucker, G.; Riemann, D.; et al. Insomnia as a predictor of mental disorders: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 43, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Alvaro, P.K.; Roberts, R.; Harris, J.K. A Systematic Review Assessing Bidirectionality between Sleep Disturbances, Anxiety, and Depression. Sleep 2013, 36, 1059–1068. [Google Scholar] [CrossRef]
- Taylor, D.; Lichstein, K.L.; Durrence, H.H. Insomnia as a Health Risk Factor. Behav. Sleep Med. 2003, 1, 227–247. [Google Scholar] [CrossRef]
- Taylor, D.J.; Lichstein, K.L.; Durrence, H.H.; Reidel, B.W.; Bush, A.J. Epidemiology of Insomnia, Depression, and Anxiety. Sleep 2005, 28, 1457–1464. [Google Scholar] [CrossRef] [PubMed]
- Spoormaker, V.I.; Bout, J.V.D. Depression and anxiety complaints; relations with sleep disturbances. Eur. Psychiatry 2005, 20, 243–245. [Google Scholar] [CrossRef] [PubMed]
- Emamian, F.; Khazaie, H.; Okun, M.L.; Tahmasian, M.; Sepehry, A.A. Link between insomnia and perinatal depressive symptoms: A meta-analysis. J. Sleep Res. 2019, 28, e12858. [Google Scholar] [CrossRef]
- Okun, M.L. Sleep and postpartum depression. Curr. Opin. Psychiatry 2015, 28, 490–496. [Google Scholar] [CrossRef]
- Okun, M.L. Disturbed Sleep and Postpartum Depression. Curr. Psychiatry Rep. 2016, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lawson, A.; Murphy, K.E.; Sloan, E.; Uleryk, E.; Dalfen, A. The relationship between sleep and postpartum mental disorders: A systematic review. J. Affect. Disord. 2015, 176, 65–77. [Google Scholar] [CrossRef]
- González-Mesa, E.; Cuenca-Marín, C.; Suarez-Arana, M.; Tripiana-Serrano, B.; Ibrahim-Díez, N.; Gonzalez-Cazorla, A.; Blasco-Alonso, M. Poor sleep quality is associated with perinatal depression. A systematic review of last decade scientific literature and meta-analysis. J. Périnat. Med. 2019, 47, 689–703. [Google Scholar] [CrossRef]
- MacLean, J.V.; Faisal-Cury, A.; Chan, Y.-F.; Menezes, P.R.; Winters, A.; Joseph, R.; Huang, H. The relationship between sleep disturbance in pregnancy and persistent common mental disorder in the perinatal period (sleep disturbance and persistent CMD). J. Ment. Health 2015, 24, 375–378. [Google Scholar] [CrossRef]
- Harrison-Hohner, J.; Coste, S.; Dorato, V.; Curet, L.B.; McCarron, D.; Hatton, D. Prenatal calcium supplementation and postpartum depression: An ancillary study to a randomized trial of calcium for prevention of preeclampsia. Arch. Women’s Ment. Health 2001, 3, 141–146. [Google Scholar] [CrossRef]
- Reichner, C.A. Insomnia and sleep deficiency in pregnancy. Obstet. Med. 2015, 8, 168–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Curcio, G.G.; Tempesta, D.; Scarlata, S.; Marzano, C.; Moroni, F.; Rossini, P.M.; Ferrara, M.; De Gennaro, L. Validity of the Italian Version of the Pittsburgh Sleep Quality Index (PSQI). Neurol. Sci. 2012, 34, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Castronovo, V.; Galbiati, A.; Marelli, S.; Brombin, C.; Cugnata, F.; Giarolli, L.; Anelli, M.M.; Rinaldi, F.; Ferini-Strambi, L. Validation study of the Italian version of the Insomnia Severity Index (ISI). Neurol. Sci. 2016, 37, 1517–1524. [Google Scholar] [CrossRef]
- Okun, M.L.; Kravitz, H.M.; Sowers, M.F.; Moul, D.E.; Buysse, D.J.; Hall, M. Psychometric Evaluation of the Insomnia Symptom Questionnaire: A Self-report Measure to Identify Chronic Insomnia. J. Clin. Sleep Med. 2009, 5, 41–51. [Google Scholar] [CrossRef] [Green Version]
- Sheehan, D.V. Mini International Neuropsychiatric Interview Version 7.0.2 for DSM-5; Harm Research Institute: Tampa, FL, USA, 2016. [Google Scholar]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of Postnatal Depression. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [Green Version]
- Murray, D.; Cox, J.L. Screening for depression during pregnancy with the edinburgh depression scale (EDDS). J. Reprod. Infant Psychol. 1990, 8, 99–107. [Google Scholar] [CrossRef]
- McBride, H.L.; Wiens, R.M.; McDonald, M.J.; Cox, D.W.; Chan, E.K.H. The Edinburgh Postnatal De-pression Scale (EPDS): A rievew of the reported validity evidence. In Validity and Validation in Social, Behavioral, and Health Sciences; Zumbo, B.D., Ed.; Springer: New York, NY, USA, 2014; pp. 157–174. [Google Scholar]
- Benvenuti, P. The Edinburgh Postnatal Depression Scale: Validation for an Italian sample. J. Affect. Disord. 1999, 53, 137–141. [Google Scholar] [CrossRef]
- Zung, W.W. A Rating Instrument For Anxiety Disorders. Psychosomatics 1971, 12, 371–379. [Google Scholar] [CrossRef]
- Zung, W.W.K. The Measurement of Affects: Depression and Anxiety. In Modern Trends in Pharma-Copsychiatry; Pichot, P., Olivier-Martin, R., Eds.; Karger Publishers AG: Basilea, Switzerland, 1974; Volume 7, pp. 170–188. ISBN 9783805516303. [Google Scholar]
- Dunstan, D.A.; Scott, N. Norms for Zung’s Self-rating Anxiety Scale. BMC Psychiatry 2020, 20, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunstan, D.A.; Scott, N.; Todd, A.K. Screening for anxiety and depression: Reassessing the utility of the Zung scales. BMC Psychiatry 2017, 17, 329. [Google Scholar] [CrossRef] [PubMed]
- Tanaka-Matsumi, J.; Kameoka, V.A. Reliabilities and concurrent validities of popular self-report measures of depression, anxiety, and social desirability. J. Consult. Clin. Psychol. 1986, 54, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Conti, L. The Zung Self-Rating Anxiety Scale (SAS). In Repertorio Delle Scale di Valutazione in Psichiatria, Vol.1; Conti, L., Ed.; SEE: Firenze, Italy, 1999; pp. 561–563. [Google Scholar]
- Angst, J.; Adolfsson, R.; Benazzi, F.; Gamma, A.; Hantouche, E.; Meyer, T.D.; Skeppar, P.; Vieta, E.; Scott, J. The HCL-32: Towards a self-assessment tool for hypomanic symptoms in outpatients. J. Affect. Disord. 2005, 88, 217–233. [Google Scholar] [CrossRef]
- Carta, M.G.; Hardoy, M.C.; Cadeddu, M.; Murru, A.; Campus, A.; Morosini, P.L.; Gamma, A.; Angst, J. The accuracy of the Italian version of the Hypomania Checklist (HCL-32) for the screening of bipolar disorders and comparison with the Mood Disorder Questionnaire (MDQ) in a clinical sample. Clin. Pract. Epidemiol. Ment. Health 2006, 2, 2. [Google Scholar] [CrossRef] [Green Version]
- Akiskal, H.S.; Akiskal, K.K.; Haykal, R.F.; Manning, J.S.; Connor, P.D. TEMPS-A: Progress towards validation of a self-rated clinical version of the Temperament Evaluation of the Memphis, Pisa, Paris, and San Diego Autoquestionnaire. J. Affect. Disord. 2005, 85, 3–16. [Google Scholar] [CrossRef]
- Pompili, M.; Girardi, P.; Tatarelli, R.; Iliceto, P.; De Pisa, E.; Tondo, L.; Akiskal, K.K.; Akiskal, H.S. TEMPS-A (Rome): Psychometric validation of affective temperaments in clinically well subjects in mid- and south Italy. J. Affect. Disord. 2008, 107, 63–75. [Google Scholar] [CrossRef]
- Edinger, J.D.; Bonnet, M.H.; Bootzin, R.R.; Doghramji, K.; Dorsey, C.M.; Espie, C.A.; Jamieson, A.O.; McCall, W.; Morin, C.M.; Stepanski, E.J. Derivation of Research Diagnostic Criteria for Insomnia: Report of an American Academy of Sleep Medicine Work Group. Sleep 2004, 27, 1567–1596. [Google Scholar] [CrossRef] [PubMed]
- Behling, O.; Law, K. Translating Questionnaires and Other Research Instruments; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2000; ISBN 9780761918240. [Google Scholar]
- Youden, W.J. Index for Rating Diagnostic Tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Hannigan, L.J.; Eilertsen, E.M.; Gjerde, L.C.; Reichborn-Kjennerud, T.; Eley, T.C.; Rijsdijk, F.; Ystrom, E.; A McAdams, T. Maternal prenatal depressive symptoms and risk for early-life psychopathology in offspring: Genetic analyses in the Norwegian Mother and Child Birth Cohort Study. Lancet Psychiatry 2018, 5, 808–815. [Google Scholar] [CrossRef] [Green Version]
- Parsons, C.; Young, K.; Rochat, T.; Kringelbach, M.; Stein, A. Postnatal depression and its effects on child development: A review of evidence from low- and middle-income countries. Br. Med Bull. 2011, 101, 57–79. [Google Scholar] [CrossRef]
- Lindahl, V.; Pearson, J.L.; Colpe, L. Prevalence of suicidality during pregnancy and the postpartum. Arch. Women’s Ment. Health 2005, 8, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Coble, P.A.; Reynolds, C.F.; Kupfer, D.J.; Houck, P.R.; Day, N.L.; Giles, D.E. Childbearing in women with and without a history of affective disorder. II. Electroencephalographic sleep. Compr. Psychiatry 1994, 35, 215–224. [Google Scholar] [CrossRef]
- Wolfson, A.R.; Crowley, S.J.; Anwer, U.; Bassett, J.L. Changes in Sleep Patterns and Depressive Symptoms in First-Time Mothers: Last Trimester to 1-Year Postpartum. Behav. Sleep Med. 2003, 1, 54–67. [Google Scholar] [CrossRef]
- Osnes, R.S.; Roaldset, J.O.; Follestad, T.; Eberhard-Gran, M. Insomnia late in pregnancy is associated with perinatal anxiety: A longitudinal cohort study. J. Affect. Disord. 2019, 248, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Osnes, R.S.; Eberhard-Gran, M.; Follestad, T.; Kallestad, H.; Morken, G.; Roaldset, J.O. Mid-pregnancy insomnia is associated with concurrent and postpartum maternal anxiety and obsessive-compulsive symptoms: A prospective cohort study. J. Affect. Disord. 2020, 266, 319–326. [Google Scholar] [CrossRef]
- Sharma, V.; Mazmanian, D. Sleep loss and postpartum psychosis. Bipolar Disord. 2003, 5, 98–105. [Google Scholar] [CrossRef]
- Ottoni, G.L.; Lorenzi, T.M.; Lara, D.R. Association of temperament with subjective sleep patterns. J. Affect. Disord. 2011, 128, 120–127. [Google Scholar] [CrossRef]
- Oniszczenko, W.; Rzeszutek, M.; Stanisławiak, E. Affective Temperaments, Mood, and Insomnia Symptoms in a Nonclinical Sample. Behav. Sleep Med. 2017, 17, 355–363. [Google Scholar] [CrossRef]
- Goldstein, C.A.; Lanham, M.S.; Smith, Y.R.; O’Brien, L.M. Sleep in women undergoing in vitro fertilization: A pilot study. Sleep Med. 2016, 32, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Backhaus, J.; Junghanns, K.; Broocks, A.; Riemann, D.; Hohagen, F. Test–retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. Psychosomatics 2002, 53, 737–740. [Google Scholar] [CrossRef]
- Violani, C.; Devoto, A.; Lucidi, F.; Lombardo, C.; Russo, P.M. Validity of a Short Insomnia Questionnaire: The SDQ. Brain Res. Bull. 2004, 63, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Darvishi, N.; Khaledi-Paveh, B.; Vaisi-Raygani, A.; Jalali, R.; Daneshkhah, A.; Bartina, Y.; Mohammadi, M. A systematic review and meta-analysis of prevalence of insomnia in the third trimester of pregnancy. BMC Pregnancy Childbirth 2021, 21, 284. [Google Scholar] [CrossRef] [PubMed]
- Krystal, A.D.; Edinger, J.D. Measuring sleep quality. Sleep Med. 2008, 9, S10–S17. [Google Scholar] [CrossRef]
- Adler, I.; Weidner, K.; Eberhard-Gran, M.; Garthus-Niegel, S. The Impact of Maternal Symptoms of Perinatal Insomnia on Social-emotional Child Development: A Population-based, 2-year Follow-up Study. Behav. Sleep Med. 2020, 19, 303–317. [Google Scholar] [CrossRef]


{kind=link}
| No-Insomnia Sample N (%) | Insomnia Sample N (%) | df | p | ||
|---|---|---|---|---|---|
| Continuous Variables | F | ||||
| Age | |||||
| M(SD) | 33.13 (5.11) | 34.10 (4.60) | 1.254 | 1/289 | 0.264 |
| Min-Max | 19–46 | 22–42 | |||
| BMI Early Pregnancy | |||||
| M(SD) | 22.59 (3.81) | 22.92 (3.02) | 0.197 | 1/245 | 0.658 |
| Min-Max | 15.63–42.52 | 17.44–28.98 | |||
| TEMPS-A Depressive | |||||
| M(SD) | 5.49 (2.38) | 8.70 (4.06) | 41.855 | 1/248 | <0.001 |
| TEMPS-A Cyclothymic | |||||
| M(SD) | 3.07 (2.94) | 5.64 (3.66) | 20.226 | 1/248 | <0.001 |
| TEMPS-A Hyperthymic | |||||
| M(SD) | 10.73 (3.76) | 9.73 (4.80) | 1.889 | 1/245 | 0.171 |
| TEMPS-A Irritable | |||||
| M(SD) | 1.88 (2.21) | 4.15 (3.29) | 26.140 | 1/242 | <0.001 |
| TEMPS-A Anxious | |||||
| M(SD) | 5.01 (4.04) | 10.27 (5.35) | 43.933 | 1/242 | <0.001 |
| EPDS | |||||
| M(SD) | 5.26 (3.77) | 10.46 (2.61) | 52.439 | 1/289 | <0.001 |
| SAS | |||||
| M(SD) | 33.51 (6.52) | 39.94 (5.69) | 31.315 | 1/271 | <0.001 |
| HCL-32 | |||||
| M(SD) | 11.68 (6.56) | 15.43 (6.58) | 8.674 | 1/254 | 0.004 |
| PSQI Global Score | |||||
| M(SD) | 5.75 (3.02) | 12. 29 (2.89) | 144.850 | 1/276 | <0.001 |
| Categorical Variables | Chi-squared test | ||||
| Level of Education | 0.691 | 2 | 0.708 | ||
| Middle school | 14 (5.6) | 1 (2.6) | |||
| High school | 101 (40.1) | 17 (43.6) | |||
| University/Postgraduate | 137 (54.4) | 21 (53.8) | |||
| N/A | 1 | - | |||
| Occupation | 1.512 | 1 | 0.219 | ||
| Unemployed | 55 (21.8) | 5 (13.2) | |||
| Employed | 197 (78.2) | 33 (86.8) | |||
| N/A | 1 | 1 | |||
| Partner | 0.474 | 1 | 0.491 | ||
| No | 3 (1.2) | 0 (0) | |||
| Yes | 240 (98.8) | 38 (100) | |||
| N/A | 10 | 1 | |||
| BMI cutoff | 2.533 | 3 | 0.469 | ||
| Underweight | 20 (9.1) | 2 (7.4) | |||
| Normal weight | 152 (69.1) | 17 (63.0) | |||
| Overweight | 41 (18.6) | 8 (29.6) | |||
| Obese | 7 (3.2) | 0 (0) | |||
| N/A | 33 | 12 | |||
| BMI—Range Weight Gain | 0.389 | 2 | 0.823 | ||
| Under range | 91 (44.0) | 9 (39.1) | |||
| Normal | 81 (39.1) | 9 (39.1) | |||
| Above range | 35 (16.9) | 5 (21.7) | |||
| N/A | 46 | 16 | |||
| Medical Conditions | 0.020 | 1 | 0.888 | ||
| No | 192 (75.9) | 30 (76.9) | |||
| Yes | 61 (24.1) | 9 (23.1) | |||
| Psychiatric History | 3.068 | 1 | 0.080 | ||
| No | 205 (81.3) | 27 (69.2) | |||
| Yes | 47 (18.7) | 12 (30.8) | |||
| N/A | 1 | - | |||
| Previous Psychopharmacological Therapy | 16.772 | 1 | <0.001 | ||
| No | 238 (94.1) | 29 (74.4) | |||
| Yes | 15 (5.9) | 10 (25.6) | |||
| Current Psychopharmacological Therapy | 0.058 | 1 | 0.810 | ||
| No | 248 (98.0) | 38 (97.4) | |||
| Yes | 5 (2.0) | 1 (2.6) | |||
| Psychiatric Family History | 10.287 | 1 | 0.001 | ||
| No | 192 (75.9) | 20 (51.3) | |||
| Yes | 61 (24.1) | 19 (48.7) | |||
| Menstrual Cycle Regularity | 0.446 | 1 | 0.504 | ||
| No | 49 (19.6) | 9 (24.3) | |||
| Yes | 201 (80.4) | 28 (75.7) | |||
| N/A | 4 | 2 | |||
| Premenstrual Syndrome | 3.199 | 1 | 0.074 | ||
| No | 137 (55.0) | 15 (39.5) | |||
| Yes | 112 (45.0) | 23 (60.5) | |||
| N/A | 4 | 1 | |||
| Others Completed Pregnancies | 0.118 | 1 | 0.731 | ||
| No | 156 (62.4) | 22 (59.5) | |||
| Yes | 94 (37.6) | 15 (40.5) | |||
| N/A | 3 | 2 | |||
| Abortions | 1.746 | 1 | 0.186 | ||
| No | 181 (72.7) | 23 (62.2) | |||
| Yes | 68 (27.3) | 14 (37.8) | |||
| N/A | 4 | 2 | |||
| Caffeine | 1.576 | 1 | 0.209 | ||
| No | 126 (50.4) | 15 (39.5) | |||
| Yes | 124 (49.6) | 23 (60.5) | |||
| N/A | 3 | 1 | |||
| Tobacco | 0.053 | 1 | 0.818 | ||
| No | 221 (90.2) | 32 (91.4) | |||
| Yes | 24 (8.6) | 3 (8.6) | |||
| N/A | 8 | 4 | |||
| Alcohol | 0.202 | 1 | 0.653 | ||
| No | 245 (98.4) | 37 (97.4) | |||
| Yes | 4 (1.6) | 1 (2.6) | |||
| N/A | 4 | 1 | |||
| Narcotic Substances | 1.073 | 1 | 0.300 | ||
| No | 248 (99.2) | 37 (97.4) | |||
| Yes | 2 (0.8) | 1 (2.6) | |||
| N/A | 3 | 1 | |||
| Assisted Fertilization | 4.683 | 1 | 0.030 | ||
| No | 209 (83.9) | 36 (97.3) | |||
| Yes | 40 (16.1) | 1 (2.7) | |||
| N/A | 4 | 2 | |||
| Past Perinatal Psychiatric Disorders | 9.882 | 1 | 0.002 | ||
| No | 236 (93.7) | 29 (78.4) | |||
| Yes | 16 (6.3) | 8 (21.6) | |||
| N/A | 1 | 2 | |||
| Pregnancy Complications | 0.052 | 1 | 0.819 | ||
| No | 183 (73.2) | 27 (75.0) | |||
| Yes | 67 (26.8) | 9 (25.0) | |||
| N/A | 3 | 3 | |||
| Rest period | 0.003 | 1 | 0.955 | ||
| No | 191 (76.1) | 28 (75.7) | |||
| Yes | 60 (23.9) | 9 (24.3) | |||
| N/A | 2 | 12 | |||
| Hospitalization During Pregnancy | 0.767 | 1 | 0.381 | ||
| No | 237 (93.7) | 36 (97.3) | |||
| Yes | 16 (6.3) | 1 (2.7) | |||
| N/A | - | 2 | |||
| Partner’s Support | 1.526 | 1 | 0.217 | ||
| No | 14 (5.6) | 4 (10.8) | |||
| Yes | 238 (94.4) | 33 (89.2) | |||
| N/A | 1 | 2 | |||
| Family’s Support | 2.604 | 1 | 0.107 | ||
| No | 52 (20.6) | 12 (32.4) | |||
| Yes | 200 (79.4) | 25 (67.6) | |||
| N/A | 1 | 2 | |||
| Stressful Events | 0.065 | 1 | 0.799 | ||
| No | 136 (54.8) | 20 (52.6) | |||
| Yes | 112 (45.2) | 18 (47.4) | |||
| N/A | 5 | 1 | |||
| ISQ—T0 | 145.953 | 1 | <0.001 | ||
| No | 240 (94.9) | 8 (20.5) | |||
| Yes | 13 (5.1) | 31 (70.5) | |||
| ISQ—T1 | 7.528 | 1 | 0.006 | ||
| No | 42 (93.3) | 2 (50.0) | |||
| Yes | 3 (6.7) | 2 (50.0) |
| PSQI Global Score | PSQI Global Score | Total | |||
|---|---|---|---|---|---|
| ≤5 | >5 | ≤10 | >10 | ||
| ISQ | |||||
| No-Insomnia | 124 | 122 | 216 | 20 | 236 |
| Insomnia | 0 | 42 | 18 | 24 | 42 |
| Score (Yes or No) | 124 | 154 | 234 | 44 | 278 |
| ISQ | PSQI | SAS | EPDS | HCL-32 | ||
|---|---|---|---|---|---|---|
| ISQ | rpb | - | 0.519 | 0.352 | 0.366 | 0.167 |
| p | <0.001 | <0.001 | <0.001 | 0.007 | ||
| N | 292 | 278 | 273 | 291 | 256 |
| DSM-5 Diagnosis | Total | ||
|---|---|---|---|
| Insomnia | No-Insomnia | ||
| ISQ | |||
| Insomnia | 31 | 13 | 44 |
| No-Insomnia | 8 | 240 | 248 |
| Total | 39 | 253 | 292 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Chiara, L.; Mazza, C.; Ricci, E.; Koukopoulos, A.E.; Kotzalidis, G.D.; Bonito, M.; Callovini, T.; Roma, P.; Angeletti, G. The Relevance of Insomnia in the Diagnosis of Perinatal Depression: Validation of the Italian Version of the Insomnia Symptom Questionnaire. Int. J. Environ. Res. Public Health 2021, 18, 12507. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312507
De Chiara L, Mazza C, Ricci E, Koukopoulos AE, Kotzalidis GD, Bonito M, Callovini T, Roma P, Angeletti G. The Relevance of Insomnia in the Diagnosis of Perinatal Depression: Validation of the Italian Version of the Insomnia Symptom Questionnaire. International Journal of Environmental Research and Public Health. 2021; 18(23):12507. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312507
Chicago/Turabian StyleDe Chiara, Lavinia, Cristina Mazza, Eleonora Ricci, Alexia Emilia Koukopoulos, Georgios D. Kotzalidis, Marco Bonito, Tommaso Callovini, Paolo Roma, and Gloria Angeletti. 2021. "The Relevance of Insomnia in the Diagnosis of Perinatal Depression: Validation of the Italian Version of the Insomnia Symptom Questionnaire" International Journal of Environmental Research and Public Health 18, no. 23: 12507. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312507