
Efficacy of Web-Based Supportive Interventions in Quality of Life in COPD Patients, a Systematic Review and Meta-Analysis

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Eligibility Criteria
2.2. Study Selection and Data Extraction
2.3. Assessment of Methodological Quality and Risk of Bias
2.4. Data Synthesis and Analysis
3. Results
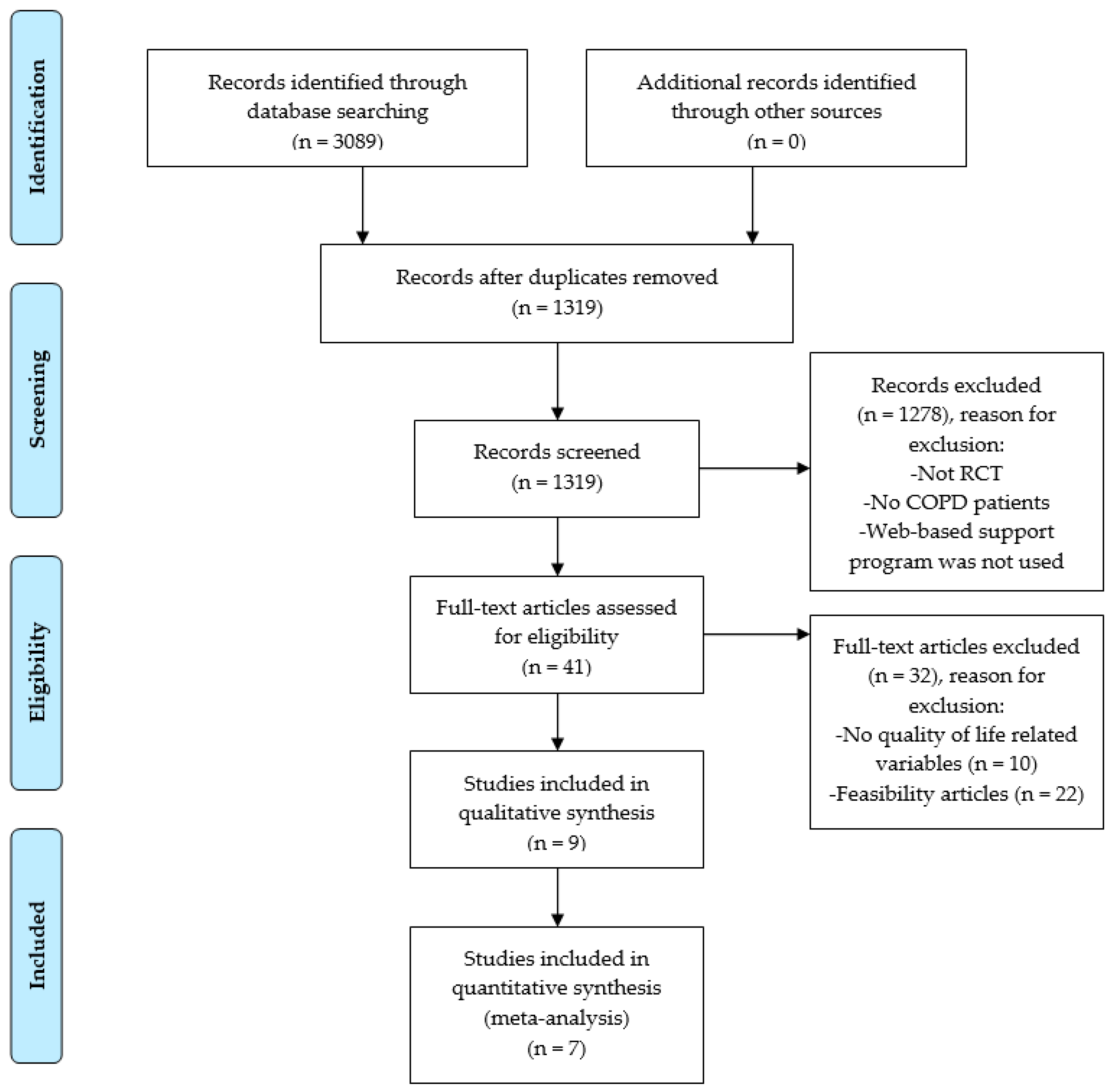
3.1. Study Selection
3.2. Study Characteristics
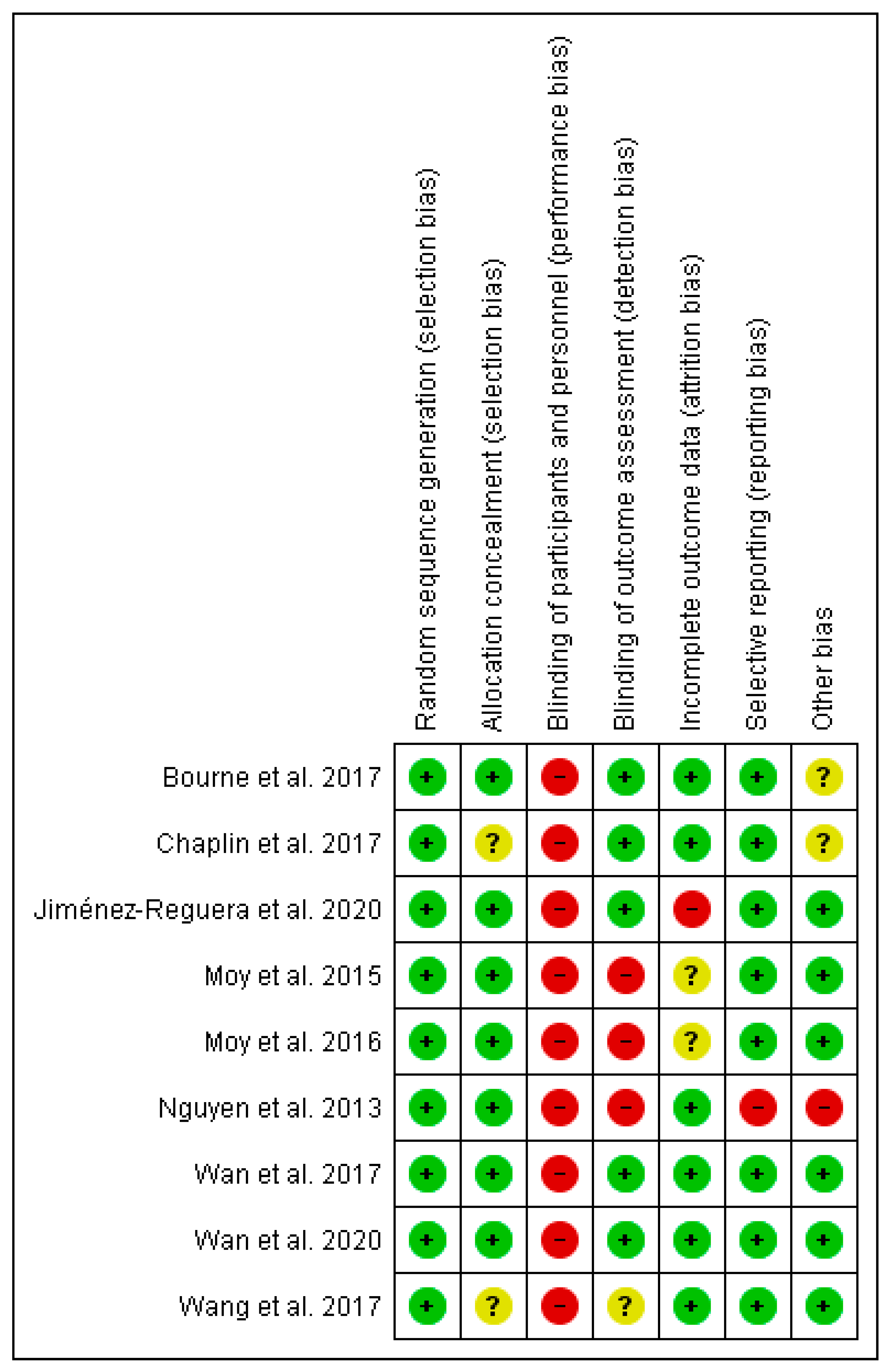
3.3. Risk of Bias
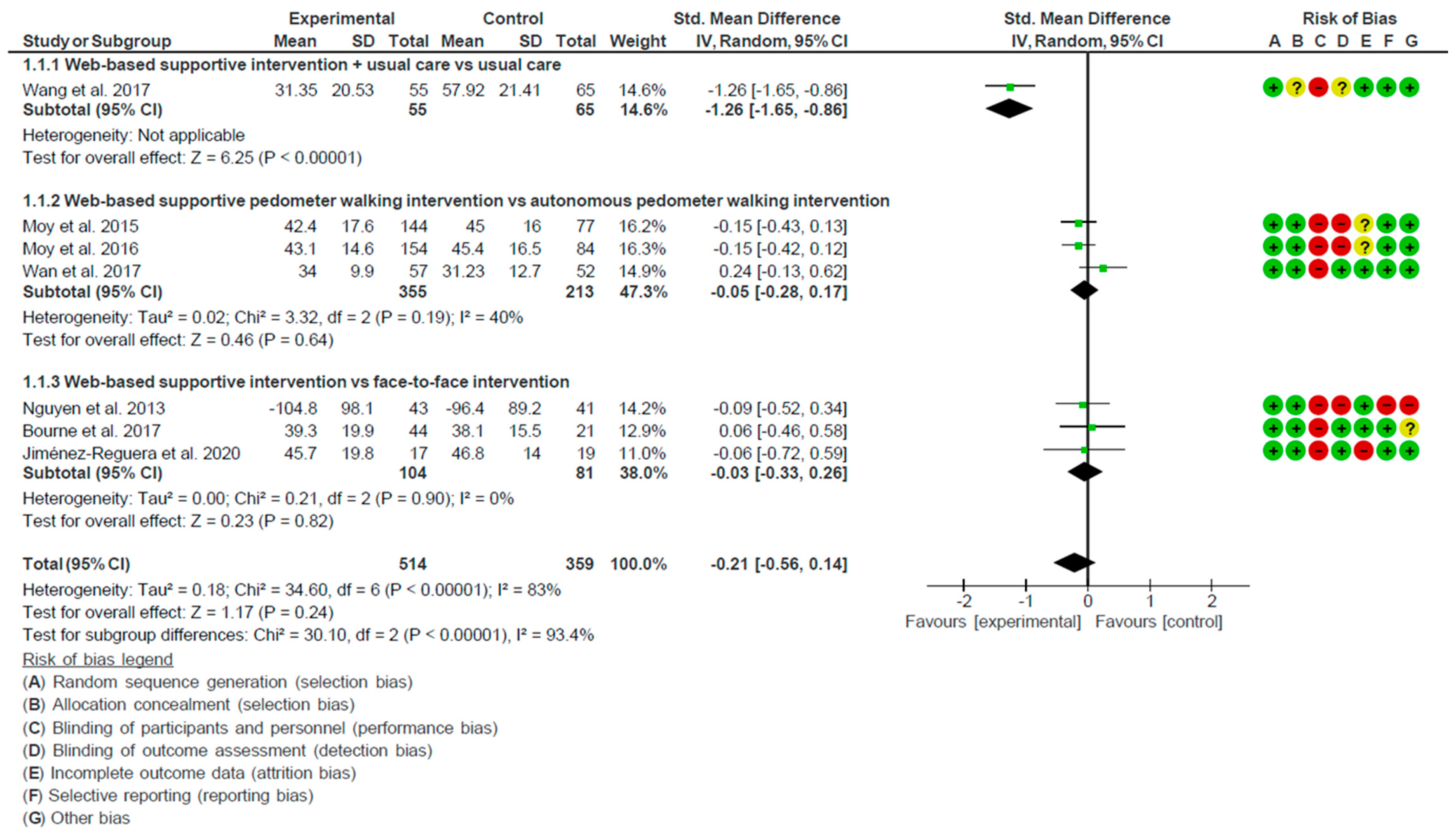
3.4. Results of Meta-Analysis
4. Discussion
Strengths and Limitations
5. Conclusions
Practical Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A
References
- Global Initiative for Chronic Obstructive Lung Disease. GOLD Report 2020. Available online: https://goldcopd.org/wp-content/uploads/2019/12/GOLD-2020-FINAL-ver1.2-03Dec19_WMV.pdf (accessed on 30 November 2021).
- Gunasekaran, K.; Ahmad, M.; Rehman, S.; Thilagar, B.; Gopalratnam, K.; Ramalingam, S.; Paramasivam, V.; Arora, A.; Chandran, A. Impact of a Positive Viral Polymerase Chain Reaction on Outcomes of Chronic Obstructive Pulmonary Disease (COPD) Exacerbations. Int. J. Environ. Res. Public Health 2020, 17, 8072. [Google Scholar] [CrossRef]
- Lopez, A.D.; Shibuya, K.; Rao, C.; Mathers, C.D.; Hansell, A.; Held, L.S.; Schmid, V.; Buist, S. Chronic obstructive pulmonary disease: Current burden and future projections. Eur. Respir. J. 2006, 27, 397–412. [Google Scholar] [CrossRef] [Green Version]
- Disler, R.T.; Gallagher, R.D.; Davidson, P.M. Factors influencing self-management in chronic obstructive pulmonary disease: An integrative review. Int. J. Nurs. Stud. 2012, 49. [Google Scholar] [CrossRef] [PubMed]
- Ghobadi, H.; Ahari, S.S.; Kameli, A.; Lari, S.M. The Relationship between COPD Assessment Test (CAT) Scores and Severity of Airflow Obstruction in Stable COPD Patients. Tanaffos 2012, 11, 22–26. [Google Scholar]
- Izquierdo, J.L.; Morena, D.; Gonzalez-Moro, J.M.R.; Paredero, J.M.; Pérez, B.; Graziani, D.; Gutiérrez, M.; Rodríguez, J.M. Manejo clínico de la EPOC en situación de vida real. Análisis a partir de big data. Arch. Bronconeumol. 2021, 57, 94–100. [Google Scholar] [CrossRef]
- Kosteli, M.-C.; Heneghan, N.R.; Roskell, C.; Williams, S.; Adab, P.; Dickens, A.P.; Enocson, A.; Fitzmaurice, D.A.; Jolly, K.; Jordan, R.; et al. Barriers and enablers of physical activity engagement for patients with COPD in primary care. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 1019–1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stellefson, M.L.; Shuster, J.J.; Chaney, B.H.; Paige, S.R.; Alber, J.M.; Chaney, J.D.; Sriram, P.S. Web-based Health Information Seeking and eHealth Literacy among Patients Living with Chronic Obstructive Pulmonary Disease (COPD). Health Commun. 2017, 33, 1410–1424. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, S.; Brooks, D.; Stagg-Peterson, S.; Goldstein, R. Growing Awareness of the Importance of Health Literacy in Individuals with COPD. COPD: J. Chronic Obstr. Pulm. Dis. 2013, 10, 72–78. [Google Scholar] [CrossRef]
- Hernandez, P.; Balter, M.; Bourbeau, J.; Hodder, R. Living with chronic obstructive pulmonary disease: A survey of patients’ knowledge and attitudes. Respir. Med. 2009, 103, 1004–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, J.M.; Niikura, M.; Yang, C.W.T.; Sin, D.D. COVID-19 and COPD. Eur. Respir. J. 2020, 56, 2002108. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, S. Management Challenges in Chronic Obstructive Pulmonary Disease in the COVID-19 Pandemic: Telehealth and Virtual Reality. J. Clin. Med. 2021, 10, 1261. [Google Scholar] [CrossRef]
- Guerra-Paiva, S.; Dias, F.; Costaa, D.; Santos, V.; Santos, C. DPO2 Project: Telehealth to enhance the social role of physical activity in people living with COPD. Proc. Comput. Sci. 2021, 181, 869–875. [Google Scholar] [CrossRef]
- Jansen, F.; Van Uden-Kraan, C.F.; Van Zwieten, V.; Witte, B.I.; Leeuw, I.M.V.-D. Cancer survivors’ perceived need for supportive care and their attitude towards self-management and eHealth. Support. Care Cancer 2014, 23, 1679–1688. [Google Scholar] [CrossRef] [PubMed]
- Murray, E. Web-Based Interventions for Behavior Change and Self-Management: Potential, Pitfalls, and Progress. Medicine 2.0 2012, 1, e3. [Google Scholar] [CrossRef]
- Slev, V.N.; Mistiaen, P.; Pasman, H.R.W.; Leeuw, I.M.V.-D.; van Uden-Kraan, C.F.; Francke, A.L. Effects of eHealth for patients and informal caregivers confronted with cancer: A meta-review. Int. J. Med. Inform. 2016, 87, 54–67. [Google Scholar] [CrossRef] [Green Version]
- Gaveikaite, V.; Grundstrom, C.; Winter, S.; Chouvarda, I.; Maglaveras, N.; Priori, R. A systematic map and in-depth review of European telehealth interventions efficacy for chronic obstructive pulmonary disease. Respir. Med. 2019, 158, 78–88. [Google Scholar] [CrossRef]
- El-Gayar, O.; Timsina, P.; Nawar, N.; Eid, W. A systematic review of IT for diabetes self-management: Are we there yet? Int. J. Med. Inform. 2013, 82, 637–652. [Google Scholar] [CrossRef]
- Bonnevie, T.; Smondack, P.; Elkins, M.; Gouel, B.; Medrinal, C.; Combret, Y.; Muir, J.-F.; Cuvelier, A.; Prieur, G.; Gravier, F.-E. Advanced telehealth technology improves home-based exercise therapy for people with stable chronic obstructive pulmonary disease: A systematic review. J. Physiother. 2020, 67, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.K.; Stellefson, M.; Bernhardt, J. Healthy Aging 2.0: The Potential of New Media and Technology. Prev. Chronic Dis. 2012, 9. [Google Scholar] [CrossRef] [Green Version]
- Stellefson, M.; Chaney, B.; Barry, A.; Chavarria, E.; Tennant, B.; Walsh-Childers, K.; Sriram, P.; Zagora, J. Web 2.0 Chronic Disease Self-Management for Older Adults: A Systematic Review. J. Med. Internet Res. 2013, 15, e35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donner, C.F.; Raskin, J.; ZuWallack, R.; Nici, L.; Ambrosino, N.; Balbi, B.; Blackstock, F.; Casaburi, R.; Dreher, M.; Effing, T.; et al. Incorporating telemedicine into the integrated care of the COPD patient a summary of an inter-disciplinary workshop held in Stresa, Italy, 7–8 September 2017. Respir. Med. 2018, 143, 91–102. [Google Scholar] [CrossRef]
- Polisena, J.; Tran, K.; Cimon, K.; Hutton, B.; McGill, S.; Palmer, K.; Scott, R.E. Home telehealth for chronic obstructive pulmonary disease: A systematic review and meta-analysis. J. Telemed. Telecare 2010, 16, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Udsen, F.W.; Hejlesen, O.; Ehlers, L.H. A systematic review of the cost and cost-effectiveness of telehealth for patients suffering from chronic obstructive pulmonary disease. J. Telemed. Telecare 2014, 20, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Jiang, Y.; Xu, G.; Ding, Z. Effectiveness of Telemedicine Intervention for Chronic Obstructive Pulmonary Disease in China: A Systematic Review and Meta-Analysis. Telemed. e-Health 2020, 26, 1075–1092. [Google Scholar] [CrossRef]
- Alwashmi, M.; Hawboldt, J.; Davis, E.; Marra, C.; Gamble, J.-M.; Abu Ashour, W. The Effect of Smartphone Interventions on Patients with Chronic Obstructive Pulmonary Disease Exacerbations: A Systematic Review and Meta-Analysis. JMIR mHealth uHealth 2016, 4, e105. [Google Scholar] [CrossRef]
- Donner, C.; ZuWallack, R.; Nici, L. The Role of Telemedicine in Extending and Enhancing Medical Management of the Patient with Chronic Obstructive Pulmonary Disease. Medicina 2021, 57, 726. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.; Kim, Y.; Cho, W.-K. A Systematic Review and Meta-Analysis of Telemonitoring Interventions on Severe COPD Exacerbations. Int. J. Environ. Res. Public Health 2021, 18, 6757. [Google Scholar] [CrossRef]
- Snoswell, C.L.; Stringer, H.; Taylor, M.L.; Caffery, L.J.; Smith, A.C. An overview of the effect of telehealth on mortality: A systematic review of meta-analyses. J. Telemed. Telecare 2021. [Google Scholar] [CrossRef]
- Metting, E.; Dassen, L.; Aardoom, J.; Versluis, A.; Chavannes, N. Effectiveness of Telemonitoring for Respiratory and Systemic Symptoms of Asthma and COPD: A Narrative Review. Life 2021, 11, 1215. [Google Scholar] [CrossRef]
- Janjua, S.; Carter, D.; Threapleton, C.J.; Prigmore, S.; Disler, R.T. Telehealth interventions: Remote monitoring and consultations for people with chronic obstructive pulmonary disease (COPD). Cochrane Database Syst. Rev. 2021, 2021. [Google Scholar] [CrossRef]
- Shaw, G.; Whelan, M.E.; Armitage, L.C.; Roberts, N.; Farmer, A.J. Are COPD self-management mobile applica-tions effective? A systematic review and meta-analysis. NPJ Prim. Care Respir. Med. 2020, 30, 11. [Google Scholar] [CrossRef] [Green Version]
- Peters, G.M.; Kooij, L.; Lenferink, A.; van Harten, W.H.; Doggen, C.J.M. The Effect of Telehealth on Hospital Services Use: Systematic Review and Meta-analysis. J. Med. Internet Res. 2021, 23, e25195. [Google Scholar] [CrossRef]
- Deng, N.; Gu, T.; Zhao, Q.; Zhang, X.; Zhao, F.; He, H. Effects of telephone support on exercise capacity and quality of life in patients with chronic obstructive pulmonary disease: A meta-analysis. Psychol. Health Med. 2018, 23, 917–933. [Google Scholar] [CrossRef] [PubMed]
- Voncken-Brewster, V.; Tange, H.; de Vries, H.; Nagykaldi, Z.; Winkens, B.; van der Weijden, T. A randomized controlled trial evaluating the effectiveness of a web-based, computer-tailored self-management intervention for people with or at risk for COPD. Int. J. Chronic Obstr. Pulm. Dis. 2015, 10, 1061–1073. [Google Scholar] [CrossRef] [Green Version]
- Samoocha, D.; Bruinvels, D.J.; Elbers, N.A.; Anema, J.R.; van der Beek, A.J. Effectiveness of web-based inter-ventions on patient empowerment: A systematic review and meta-analysis. J. Med. Internet Res. 2010, 12, e23. [Google Scholar] [CrossRef]
- Pulman, A.; Lepping, P.; Paravastu, S.C.V.; Turner, J.; Billings, P.; Minchom, P. A patient centred framework for improving LTC quality of life through Web 2.0 technology. Health Inform. J. 2010, 16, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Murray, E.; Burns, J.; Tai, S.S.; Lai, R.; Nazareth, I. Interactive Health Communication Applications for people with chronic disease. Cochrane Database Syst. Rev. 2005, CD004274. [Google Scholar] [CrossRef]
- Bennett, G.G.; Glasgow, R.E. The delivery of public health interventions via the internet: Actualizing their po-tential. Annu. Rev. Public Health 2009, 30, 273–292. [Google Scholar] [CrossRef] [PubMed]
- Selzler, A.M.; Wald, J.; Sedeno, M.; Jourdain, T.; Janaudis-Ferreira, T.; Goldstein, R.; Bourbeau, J.; Stickland, M.K. Telehealth pulmonary rehabilitation: A review of the literature and an example of a nationwide initiative to im-prove the accessibility of pulmonary rehabilitation. Chron. Respir. Dis. 2018, 15, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Ambrosino, N.; Vagheggini, G.; Mazzoleni, S.; Vitacca, M. Telemedicine in chronic obstructive pulmonary disease. Breathe 2016, 12, 350–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Center for Reviews and Dissemination. Systematic Reviews—CRD’s Guidelines for Undertaking Reviews in Healthcare; Center for Reviews and Dissemination: York, UK, 2009. [Google Scholar]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeks, J.; Dinnes, J.; D’Amico, R.; Sowden, A.J.; Sakarovitch, C.; Song, F.; Petticrew, M.; Altman, D.G. Evaluating non-randomised intervention studies. Health Technol. Assess. 2003, 7, iii-173. [Google Scholar] [CrossRef] [Green Version]
- Saunders, L.D.; Soomro, G.M.; Buckingham, J.; Jamtvedt, G.; Raina, P. Assessing the Methodological Quality of Nonrandomized Intervention Studies. West. J. Nurs. Res. 2003, 25, 223–237. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.0 (Updated July 2019). Cochrane. 2019. Available online: www.training.cochrane.org/handbook (accessed on 30 November 2021).
- Holroyd-Leduc, J.M.; Helewa, A.; Walker, J.M. Critical Evaluation of Research in Physical Rehabilitation: Towards Evidence-Based Practice. Philadelphia: WB Saunders Company, 2000. Evid. Based Med. 2002, 7, 135. [Google Scholar] [CrossRef] [Green Version]
- Newham, J.J.; Presseau, J.; Heslop-Marshall, K.; Russell, S.; Ogunbayo, O.J.; Netts, P.; Hanratty, B.; Kaner, E. Features of self-management interventions for people with COPD associated with improved health-related quality of life and reduced emergency department visits: A systematic review and meta-analysis. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 1705–1720. [Google Scholar] [CrossRef] [Green Version]
- Blakemore, A.; Dickens, C.; Guthrie, E.; Bower, P.; Kontopantelis, E.; Afzal, C.; Coventry, P. Depression and anxiety predict health-related quality of life in chronic obstructive pulmonary disease: Systematic review and meta-analysis. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 501–512. [Google Scholar] [CrossRef] [Green Version]
- Cannon, D.; Buys, N.; Sriram, K.B.; Sharma, S.; Morris, N.; Sun, J. The effects of chronic obstructive pulmonary disease self-management interventions on improvement of quality of life in COPD patients: A meta-analysis. Respir. Med. 2016, 121, 81–90. [Google Scholar] [CrossRef] [Green Version]
- Chaplin, E.; Hewitt, S.; Apps, L.; Bankart, J.; Pulikottil-Jacob, R.; Boyce, S.; Morgan, M.; Williams, J.; Singh, S. Interactive web-based pulmonary rehabilitation programme: A randomised controlled feasibility trial. BMJ Open 2017, 7, e013682. [Google Scholar] [CrossRef]
- Wang, L.; He, L.; Tao, Y.; Sun, L.; Zheng, H.; Zheng, Y.; Shen, Y.; Liu, S.; Zhao, Y.; Wang, Y.; et al. Evaluating a Web-Based Coaching Program Using Electronic Health Records for Patients with Chronic Obstructive Pulmonary Disease in China: Randomized Controlled Trial. J. Med. Internet Res. 2017, 19, e264. [Google Scholar] [CrossRef]
- Nguyen, H.Q.; Donesky, D.; Reinke, L.F.; Wolpin, S.; Chyall, L.; Benditt, J.O.; Paul, S.M.; Carrieri-Kohlman, V. Internet-Based Dyspnea Self-Management Support for Patients with Chronic Obstructive Pulmonary Disease. J. Pain Symptom Manag. 2012, 46, 43–55. [Google Scholar] [CrossRef]
- Moy, M.L.; Collins, R.; Martinez, C.H.; Kadri, R.; Roman, P.; Holleman, R.G.; Kim, H.M.; Nguyen, H.Q.; Cohen, M.D.; Goodrich, D.; et al. An Internet-Mediated Pedometer-Based Program Improves Health-Related Quality-of-Life Domains and Daily Step Counts in COPD. Chest 2015, 148, 128–137. [Google Scholar] [CrossRef] [Green Version]
- Moy, M.L.; Martinez, C.H.; Kadri, R.; Roman, P.; Holleman, R.G.; Kim, H.M.; Nguyen, H.Q.; Cohen, M.D.; Goodrich, D.E.; Giardino, N.D.; et al. Long-Term Effects of an Internet-Mediated Pedometer-Based Walking Program for Chronic Obstructive Pulmonary Disease: Randomized Controlled Trial. J. Med. Internet Res. 2016, 18, e215. [Google Scholar] [CrossRef] [Green Version]
- Wan, E.S.; Kantorowski, A.; Homsy, D.; Teylan, M.; Kadri, R.; Richardson, C.R.; Gagnon, D.R.; Garshick, E.; Moy, M.L. Promoting physical activity in COPD: Insights from a randomized trial of a web-based intervention and pedometer use. Respir. Med. 2017, 130, 102–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, E.S.; Kantorowski, A.; Polak, M.; Kadri, R.; Richardson, C.R.; Gagnon, D.R.; Garshick, E.; Moy, M.L. Long-term effects of web-based pedometer-mediated intervention on COPD exacerbations. Respir. Med. 2020, 162, 105878. [Google Scholar] [CrossRef] [PubMed]
- Bourne, S.; Devos, R.; North, M.; Chauhan, A.; Green, B.; Brown, T.; Cornelius, V.; Wilkinson, T. Online versus face-to-face pulmonary rehabilitation for patients with chronic obstructive pulmonary disease: Randomised controlled trial. BMJ Open 2017, 7, e014580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiménez-Reguera, B.; López, E.M.; Fitch, S.; Juarros-Monteagudo, L.; Sánchez-Cortés, M.; Rodríguez-Hermosa, J.L.; Calle-Rubio, M.; Hernández-Criado, M.T.; López-Martín, M.; Angulo, S.; et al. Development and Preliminary Evaluation of the Effects of an mHealth Web-Based Platform (HappyAir) on Adherence to a Maintenance Program After Pulmonary Rehabilitation in Patients with Chronic Obstructive Pulmonary Disease: Randomized Controlled Trial (Preprint). JMIR mHealth uHealth 2020, 8, e18465. [Google Scholar] [CrossRef]
- Barak, A.; Klein, B.; Proudfoot, J.G. Defining Internet-Supported Therapeutic Interventions. Ann. Behav. Med. 2009, 38, 4–17. [Google Scholar] [CrossRef] [PubMed]
- Kuijpers, W.; Groen, W.G.; Aaronson, N.K.; Van Harten, W.H. A Systematic Review of Web-Based Interventions for Patient Empowerment and Physical Activity in Chronic Diseases: Relevance for Cancer Survivors. J. Med. Internet Res. 2013, 15, e37. [Google Scholar] [CrossRef] [Green Version]
- Gregersen, T.L.; Green, A.; Frausing, E.; Ringbæk, T.; Brøndum, E.; Ulrik, C.S. Do telemedical interventions im-prove quality of life in patients with COPD? A systematic review. Int. J. COPD 2016, 11, 809–822. [Google Scholar]
- Janjua, S.; Banchoff, E.; Threapleton, C.J.D.; Prigmore, S.; Fletcher, J.; Disler, R.T. Digital interventions for the management of chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2021, 4, CD013246. [Google Scholar] [CrossRef] [PubMed]
- Gorst, S.L.; Armitage, C.J.; Brownsell, S.; Hawley, M.S. Home Telehealth Uptake and Continued Use Among Heart Failure and Chronic Obstructive Pulmonary Disease Patients: A Systematic Review. Ann. Behav. Med. 2014, 48, 323–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sul, A.R.; Lyu, D.-H.; Park, D.-A. Effectiveness of telemonitoring versus usual care for chronic obstructive pulmonary disease: A systematic review and meta-analysis. J. Telemed. Telecare 2018, 26, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Yohannes, A.M. Telehealthcare management for patients with chronic obstructive pulmonary disease. Expert Rev. Respir. Med. 2012, 6, 239–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelders, S.M.; Kok, R.; Ossebaard, H.C.; Van Gemert-Pijnen, J.E. Persuasive System Design Does Matter: A Systematic Review of Adherence to Web-based Interventions. J. Med. Internet Res. 2012, 14, e152. [Google Scholar] [CrossRef]
- Sobnath, D.D.; Philip, N.; Kayyali, R.; Nabhani-Gebara, S.; Pierscionek, B.; Vaes, A.W.; A Spruit, M.; Kaimakamis, E.; Mehring, M.; Ryan, D.; et al. Features of a Mobile Support App for Patients with Chronic Obstructive Pulmonary Disease: Literature Review and Current Applications. JMIR mHealth uHealth 2017, 5, e17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mcdowell, J.E.; McClean, S.; FitzGibbon, F.; Tate, S. A randomised clinical trial of the effectiveness of home-based health care with telemonitoring in patients with COPD. J. Telemed. Telecare 2015, 21, 80–87. [Google Scholar] [CrossRef]
- Fridriksdottir, N.; Gunnarsdottir, S.; Zoëga, S.; Ingadottir, B.; Hafsteinsdottir, E.J.G. Effects of web-based inter-ventions on cancer patients’ symptoms: Review of randomized trials. Support. Care Cancer 2018, 26, 337–351. [Google Scholar] [CrossRef]
- Triberti, S.; Savioni, L.; Sebri, V.; Pravettoni, G. eHealth for improving quality of life in breast cancer patients: A systematic review. Cancer Treat. Rev. 2019, 74, 1–14. [Google Scholar] [CrossRef]
- Brunton, L.; Bower, P.; Sanders, C. The Contradictions of Telehealth User Experience in Chronic Obstructive Pulmonary Disease (COPD): A Qualitative Meta-Synthesis. PLoS ONE 2015, 10, e0139561. [Google Scholar] [CrossRef]
- Ruland, C.M.; Maffei, R.M.; Børøsund, E.; Krahn, A.; Andersen, T.; Grimsbø, G.H. Evaluation of different features of an eHealth application for personalized illness management support: Cancer patients’ use and appraisal of usefulness. Int. J. Med. Inform. 2013, 82, 593–603. [Google Scholar] [CrossRef] [PubMed]
- McCabe, C.; McCann, M.; Brady, A.M. Computer and mobile technology interventions for self-management in chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2017, 5, CD011425. [Google Scholar] [CrossRef]
- Lundell, S.; Holmner, Å.; Rehn, B.; Nyberg, A.; Wadell, K. Telehealthcare in COPD: A systematic review and meta-analysis on physical outcomes and dyspnea. Respir. Med. 2015, 109, 11–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eysenbach, G.; Kummervold, P.E.; Ritterband, L. “Is Cybermedicine Killing You?”—The Story of a Cochrane Disaster. J. Med. Internet Res. 2005, 7, e21. [Google Scholar] [CrossRef]
- Welling, J.B.A.; Hartman, J.; Hacken, N.H.T.; Klooster, K.; Slebos, D.-J. The minimal important difference for the St George’s Respiratory Questionnaire in patients with severe COPD. Eur. Respir. J. 2015, 46, 1598–1604. [Google Scholar] [CrossRef] [PubMed]
- Baumeister, R.F.; Vohs, K.D.; Nathan DeWall, C.; Zhang, L. How Emotion Shapes Behavior: Feedback, Anticipation, and Reflection, Rather Than Direct Causation. Pers. Soc. Psychol. Rev. 2007, 11, 167–203. [Google Scholar] [CrossRef]
- De La Torre-Díez, I.; López-Coronado, M.; Vaca, C.; Aguado, J.S.; de Castro, C. Cost-utility and cost-effectiveness studies of telemedicine, electronic, and mobile health systems in the literature: A systematic review. Telemed. e-Health 2015, 21, 81–85. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, M.T.; Sousa, C.S.; Morais-Almeida, M.; Simões, M.J.; Mendes, P. Telemedicine in COPD: An Overview by Topics. COPD J. Chronic Obstr. Pulm. Dis. 2020, 17, 601–617. [Google Scholar] [CrossRef]
- Kamei, T.; Yamamoto, Y.; Kajii, F.; Nakayama, Y.; Kawakami, C. Systematic review and meta-analysis of studies involving telehome monitoring-based telenursing for patients with chronic obstructive pulmonary disease. Jpn. J. Nurs. Sci. 2012, 10, 180–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz, J.; Brooks, D.; Marques, A. Home telemonitoring effectiveness in COPD: A systematic review. Int. J. Clin. Pract. 2014, 68, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.; Lee, S.H. Effectiveness of tele-monitoring by patient severity and intervention type in chronic obstruc-tive pulmonary disease patients: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2019, 92, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Wantland, D.J.; Portillo, C.J.; Holzemer, W.L.; Slaughter, R.; McGhee, E.M. The Effectiveness of Web-Based vs. Non-Web-Based Interventions: A Meta-Analysis of Behavioral Change Outcomes. J. Med. Internet Res. 2004, 6, e40. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. The law of attrition. J. Med. Internet Res. 2005, 7, e11. [Google Scholar] [CrossRef]
- Bennett, A.V.; Jensen, R.E.; Basch, E. Electronic patient-reported outcome systems in oncology clinical practice. CA A Cancer J. Clin. 2012, 62, 336–347. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Sample Size, Distribution and Sample Age n (% Men): (Mean ± SD) | Treatment Status | Severity | Downs and Black (Risk of Bias) |
|---|---|---|---|---|
| Nguyen et al. (2013) [55] | 125 (54%) allocated randomly into: EG: 68.5 ± 11.0 CG1: 68.2 ± 9.9 CG2: 69.3 ± 8.0 | Clinically stable | Mild to very severe | 22 (Poor quality) |
| Moy et al. (2015) [56] | 238 (93.7%) allocated randomly into: EG: 67.0 ± 8.6 CG: 66.4 ± 9.2 | Clinically stable | Mild to very severe | 22 (Poor quality) |
| Moy et al. (2016) [57] | 238 (93.7%) allocated randomly into: EG: 67.0 ± 8.6 CG: 66.4 ± 9.2 | Clinically stable | Mild to very severe | 23 (Poor quality) |
| Wang et al. (2017) [54] | 120 (47.5%) allocated randomly into: EG: 69.3 ± 7.8 CG: 71.9 ± 8.1 | After discharge | Moderate to very severe | 20 (Fair quality) |
| Wan et al. (2017) [58] | 109 (98,2%) allocated randomly into: EG: 68.4 ± 8.7 CG: 68.8 ± 7.9 | Clinically stable | Mild to very severe | 23 (Fair quality) |
| Bourne et al. (2017) [60] | 90 (65.56%) allocated randomly into: EG: 69.1 ± 7.9 CG: 71.4 ± 8.6 | Clinically stable | Moderate to very severe | 22 (Fair quality) |
| Chaplin et al. (2017) [53] | 103 (68.93%) allocated randomly into: EG: 66.4 ± 10.1 CG: 66.1 ± 8.1 | Clinically stable | Moderate to very severe | 22 (Fair quality) |
| Wan et al. (2020) [59] | 109 (98.17%) allocated randomly into: EG: 68.4 ± 8.7 CG: 68.7 ± 7.9 | Clinically stable | Mild to very severe | 23 (Fair quality) |
| Jiménez-Reguera et al. (2020) [61] | 36 (61.11%) allocated randomly into: EG: 68.1 ± 6.6 CG: 68.1 ± 7.0 | After discharge | Moderate to very severe | 18 (Poor quality) |
| Study | Interventions | Web Content Elements | Experimental Intervention Content | Intervention Duration | Outcomes Measures | Main Results | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nguyen et al. (2013) [55] | EG: internet-based dyspnea self-management program. CG1: face-to-face dyspnea self-management program. CG2: general health education. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 9 | Intervention included a personalized education program, dyspnea self-management training, exacerbation guidelines, personalized exercise with biweekly feedback and support, personal symptom and exercise log, real-time follow up, convenient access to information and support materials. | 12 months | Quality of life measure(s): CRQ, SF-36. Other outcomes (measure(s)): self-efficacy (validated question); functional capacity (6MWT, ITT); dyspnea with activities (CRQ-D); arm endurance; adherence; satisfaction. | Quality of life results: No significant differences were found between groups in quality of life. EG participants had significant improvement in quality of life compared with baseline. Other outcomes results: Self-efficacy for managing dyspnea improved for the EG and CG1 compared with CG2. No significant differences were found in dyspnea and functional capacity between groups. EG participants had significant improvement in dyspnea and functional capacity compared with the baseline. | |
| Moy et al. (2015) [56] | EG: web-based pedometer walking intervention. CG: pedometer walking intervention. | 1 | 2 | 3 | 4 | 5 | 6 | Step counting allowed for patient self-monitoring, new personalized weekly objectives were established, educational and motivational content to improve patient self-management, social support through an online forum. | 4 months | Quality of life measure(s): SGRQ. Other outcomes (measure(s)): physical activity (pedometer); adherence; safety. | Quality of life results: No significant differences were found between groups in SGRQ total score. EG had significant improvement on symptoms and impact subscales compared to the CG. EG participants had significant improvement in SGRQ total score, symptoms, and impact compared with the baseline. Other outcomes results: EG had significant improvement on physical activity compared to the CG. | |||
| Moy et al. (2016) [57] | EG: web-based pedometer walking intervention. CG: pedometer walking intervention. | 2 | 3 | 4 | 5 | 6 | Step counting allowed for patient self-monitoring, new personalized weekly objectives were established, motivational content to improve patient self-management, social support through an online forum. | 12 months | Quality of life measure(s): SGRQ. Other outcomes (measure(s)): physical activity (pedometer); adherence; safety. | Quality of life results: No significant differences were found between groups in quality of life. EG participants had significant improvement in SGRQ total score, symptoms, and impact compared with the baseline. Other outcomes results: Significant differences were found in physical activity between groups at month 4, but not in months 8 and 12. | ||||
| Wang et al. (2017) [54] | EG: web based coaching program + routine care CG: routine care | 1 | 4 | 5 | These were used to manage patients’ clinical and demographic variables and enabled communication between health care providers and patients. The patient was able to access disease information, pulmonary rehabilitation instructions, and particular management of the participant was determined according to the evolution of the disease. | 12 months | Quality of life measure(s): SGRQ. Other outcomes (measure(s)): functional capacity (6MWT); dyspnea (MRC); lung function (spirometry). | Quality of life results: EG had significant improvement in the SGRQ total score, SGRQ symptoms, SGRQ activity and SGRQ impact compared to the CG. Other outcomes results: EG had significant improvement of lung function, functional capacity, and degree of dyspnea compared to CG. | ||||||
| Wan et al. (2017) [58] | EG: web-based pedometer walking intervention. CG: pedometer walking intervention. | 1 | 2 | 3 | 4 | 5 | 6 | Step counting allowed for patient self-monitoring, new personalized weekly objectives were established, educational and motivational content to improve patient self-management, social support through an online forum. | 3 months | Quality of life measure(s): SGRQ. Other outcomes (measure(s)): self-efficacy (Ex-SRES); functional capacity (6MWT); physical activity (pedometer); dyspnea (MRC); depression (BDI-II); COPD knowledge (BCKQ); social support (MOS-SSS); motivation and confidence to exercise; adherence. | Quality of life results: No significant differences were found between groups in quality of life. Other outcomes results: EG had significant improvement of daily step count compared to CG. No significant differences were found between groups in functional capacity, self-efficacy, dyspnea, depression, COPD knowledge, social support motivation, and confidence to exercise. | |||
| Bourne et al. (2017) [60] | EG: online supportive pulmonary rehabilitation. CG: face-to-face- supportive pulmonary rehabilitation. | 1 | 3 | 4 | 5 | 9 | Intervention included pulmonary online rehabilitation and educational videos to promote self-management. | 6 weeks | Quality of life measure(s): SGRQ, CAT. Other outcomes (measure(s)): functional capacity (6MWT); dyspnea (MRC); anxiety and depression (HADS); adherence; safety. | Quality of life results: No significant differences were found between groups in quality of life. Other outcomes results: No significant differences were found between groups in exercise capacity, anxiety, and depression. | ||||
| Chaplin et al. (2017) [53] | EG: web based pulmonary rehabilitation program. CG: face-to-face pulmonary rehabilitation program. | 1 | 2 | 4 | 5 | 6 | 7 | 9 | Intervention included education content, exacerbation guidelines, a home exercise program and goal setting, record of the progress, motivational interviewing techniques, and convenient access to information and support. | 6–8 weeks | Quality of life measure(s): CRQ, CAT, EQ-5D. Other outcomes (measure(s)): self-efficacy (PRAISE); exercise capacity (ISWT, ESWT); anxiety and depression (HADS); COPD Knowledge (BCKQ). | Quality of life results: No significant differences were found between groups in quality of life. EG and CG participants had significant improvement in quality of life compared with the baseline. Other outcomes results: No significant differences were found between groups in any other outcome. EG and CG participants had significant improvement in functional capacity compared with the baseline. | ||
| Wan et al. (2020) [59] | EG: web-based pedometer walking intervention. CG: pedometer walking intervention. | 1 | 2 | 3 | 4 | 5 | 6 | Step counting allowed for patient self-monitoring, new personalized weekly objectives were established, educational and motivational content provided to improve patient self-management, social support through an online forum. | 15 months | Quality of life measure(s): SGRQ. Other outcomes (measure(s)): self-efficacy (Ex-SRES); physical activity (pedometer); acute exacerbations. | Quality of life results: No significant differences were found between groups in quality of life. CG participants had a significant worsening of quality of life compared with the baseline. There was no significant change in EG group, indicating no significant decline. Other outcomes results: No significant differences were found between groups in daily step count and self-efficacy. EG participants had significant improvement of acute exacerbations compared with baseline. EG participants had a minor decline that CG participants in daily step count compared with baseline. | |||
| Jiménez-Reguera et al. (2020) [61] | EG: web-based follow-up program. CG: face-to-face follow-up program. | 1 | 2 | Intervention included an educational program and data collection related to disease and physical activity, daily reminders of daily exercise, record of medication intake, daily mood, and level of tiredness. | 10 months | Quality of life measure(s): SGRQ, CAT, EQ- 5D. Other outcomes (measure(s)): functional capacity (6MWT); lung function (spirometry); adherence (CAP FISIO); adherence to physical activity (Morisky–Green Test). | Quality of life results: No significant differences were found between groups in quality of life. EG participants had a significant improvement of quality of life in compared with the baseline. Other outcomes results: No significant differences between the two groups were observed in functional capacity and lung function. EG participants had significant improvement of functional capacity in compared with baseline. EG participants had a significant improvement of adherence to the program and adherence to physical activity in compared with CG. | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calvache-Mateo, A.; López-López, L.; Heredia-Ciuró, A.; Martín-Núñez, J.; Rodríguez-Torres, J.; Ortiz-Rubio, A.; Valenza, M.C. Efficacy of Web-Based Supportive Interventions in Quality of Life in COPD Patients, a Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12692. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312692
Calvache-Mateo A, López-López L, Heredia-Ciuró A, Martín-Núñez J, Rodríguez-Torres J, Ortiz-Rubio A, Valenza MC. Efficacy of Web-Based Supportive Interventions in Quality of Life in COPD Patients, a Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(23):12692. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312692
Chicago/Turabian StyleCalvache-Mateo, Andrés, Laura López-López, Alejandro Heredia-Ciuró, Javier Martín-Núñez, Janet Rodríguez-Torres, Araceli Ortiz-Rubio, and Marie Carmen Valenza. 2021. "Efficacy of Web-Based Supportive Interventions in Quality of Life in COPD Patients, a Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 23: 12692. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312692