
Contemporary Neuroprotection Strategies during Cardiac Surgery: State of the Art Review

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
3. Incidence and Prevalence of Neurological Deficit after Cardiac Surgery
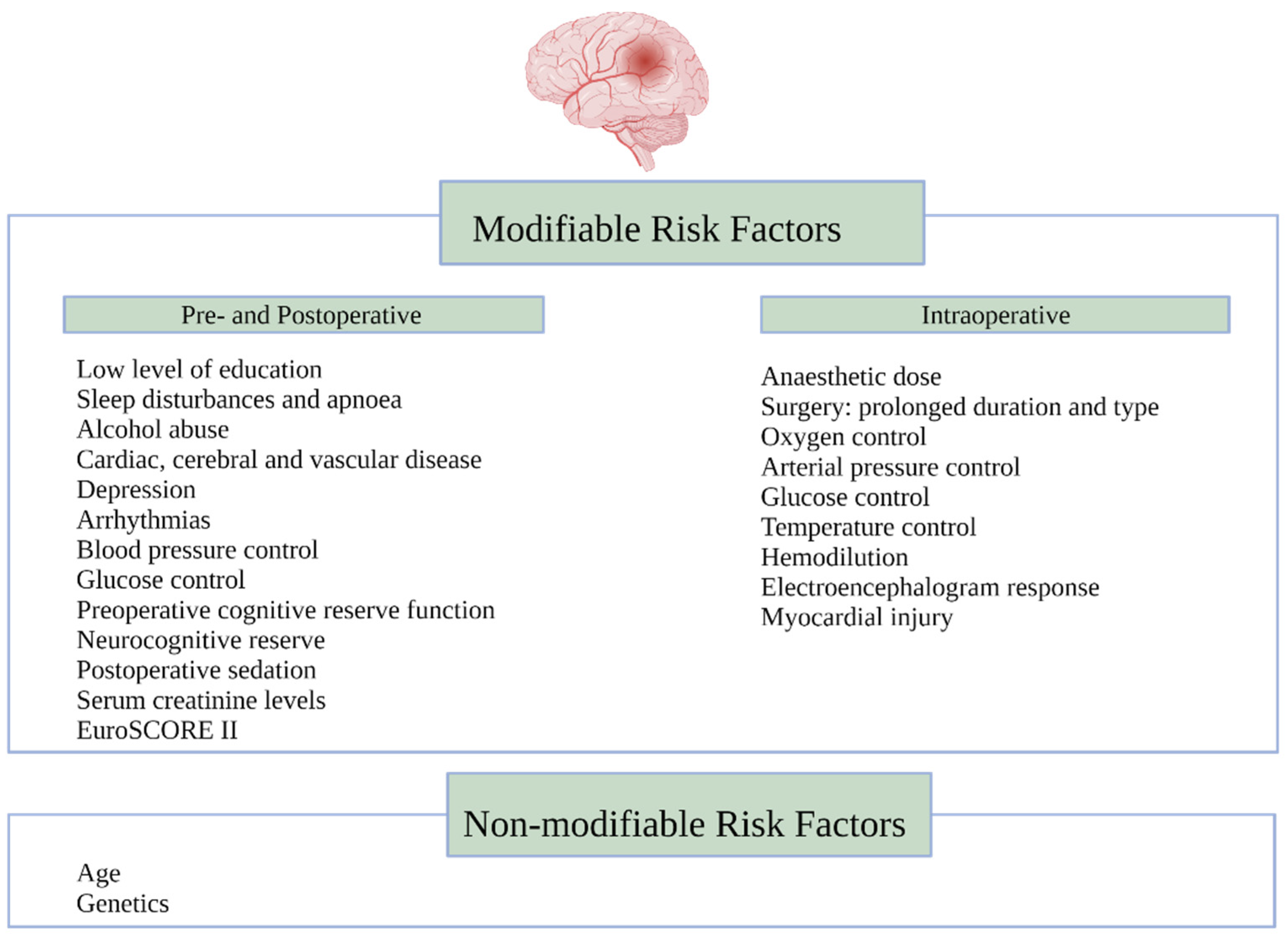
4. Risk Factors Associated with Neurological Decline
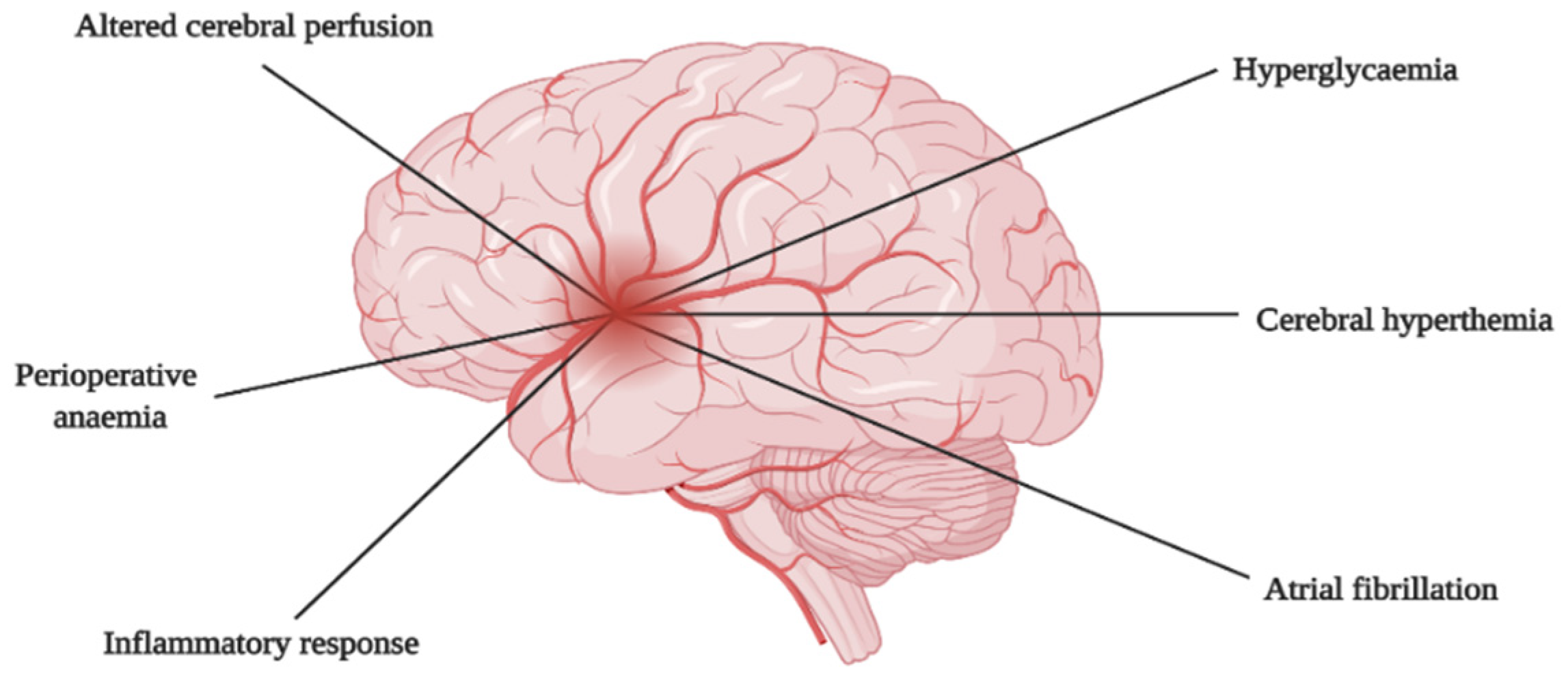
5. Mechanism of Brain Injury
5.1. Altered Cerebral Perfusion
5.2. Hypoxia Related Cerebral Injury
5.3. Reperfusion Related Cerebral Injury
5.4. Cerebral Macro- and Micro-Embolism
5.5. Inflammatory Response
5.6. Cerebral Hyperthermia
5.7. Hyperglycaemia
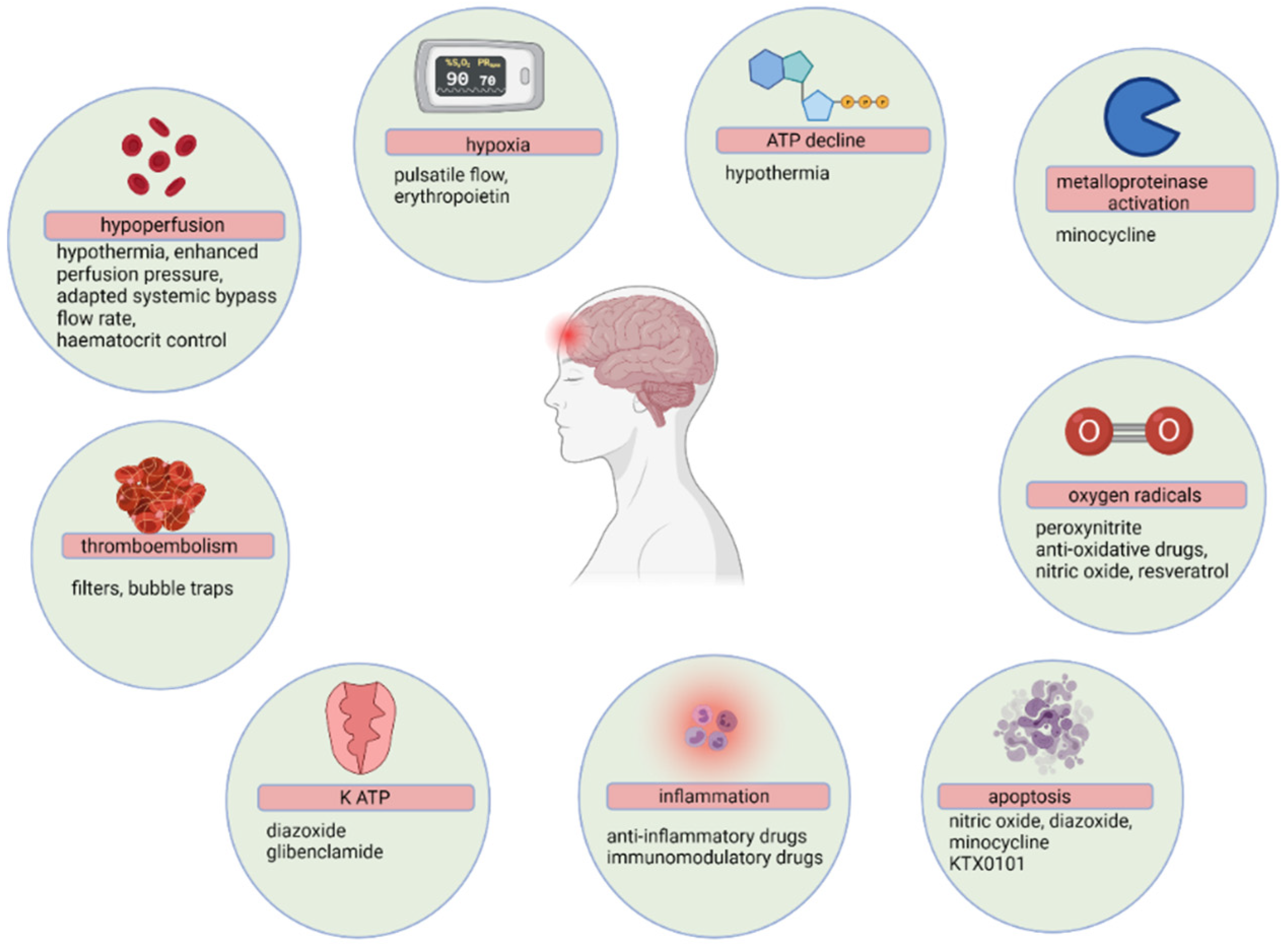
6. Neuroprotection Interventions
6.1. Preoperative Strategies
6.1.1. Corticosteroids
6.1.2. Erythromycin
6.1.3. Beta-Blockers, Statins and Angiotensin-Converting Enzyme Inhibitors
6.1.4. Recombinant Human Erythropoietin
6.2. Intraoperative Strategies
6.2.1. Pharmacological
Induction Agents
Inhalational Agents
Local Anaesthetic Agents
N-Methyl D-Aspartate (NMDA) Receptor Antagonists
Anti-Inflammatory Agents
Alpha-1 Adrenergic Receptor Agonists
Osmotic Agents
Anti-Oxidative Agents
6.2.2. Non-Pharmacological
On-Pump vs. Off-Pump
CPB Duration
Mean Arterial Pressure (MAP)
Degree of Hypothermia
Cerebral Perfusion
CPB Circuit
Glycaemic Control
Neuromonitoring
7. Assessing the Cause, Extent and Impact of Neuronal Injury
7.1. Computed Tomography
7.1.1. Non-enhanced Computed Tomography
7.1.2. Computed Tomography Angiography (CTA)
7.1.3. Computed Tomography Perfusion
7.2. Magnetic Resonance Imaging
7.3. Functional Nuclear Imaging
7.3.1. Single-Photon Emission Computed Tomography
7.3.2. Positron Emission Tomography
8. Neuroprotection Recommendations
9. Future Directions
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sultan, I.; Bianco, V.; Kilic, A.; Jovin, T.; Jadhav, A.; Jankowitz, B.; Aranda-Michel, E.; D’Angelo, M.P.; Navid, F.; Wang, Y.; et al. Predictors and Outcomes of Ischemic Stroke After Cardiac Surgery. Ann. Thorac. Surg. 2020, 110, 448–456. [Google Scholar] [CrossRef]
- Chen, F.; Duan, G.; Wu, Z.; Zuo, Z.; Li, H. Comparison of the cerebroprotective effect of inhalation anaesthesia and total intravenous anaesthesia in patients undergoing cardiac surgery with cardiopulmonary bypass: A systematic review and meta-analysis. BMJ Open 2017, 7, e014629. [Google Scholar] [CrossRef] [PubMed]
- Putzu, A.; Capelli, B.; Belletti, A.; Cassina, T.; Ferrari, E.; Gallo, M.; Casso, G.; Landoni, G. Perioperative statin therapy in cardiac surgery: A meta-analysis of randomized controlled trials. Crit. Care 2016, 20, 395. [Google Scholar] [CrossRef] [Green Version]
- Uysal, S.; Lin, H.-M.; Trinh, M.; Park, C.H.; Reich, D.L. Optimizing cerebral oxygenation in cardiac surgery: A randomized controlled trial examining neurocognitive and perioperative outcomes. J. Thorac. Cardiovasc. Surg. 2020, 159, 943–953.e3. [Google Scholar] [CrossRef]
- Habibi, M.R.; Habibi, V.; Habibi, A.; Soleimani, A. Lidocaine dose-response effect on postoperative cognitive deficit: Meta-analysis and meta-regression. Expert Rev. Clin. Pharmacol. 2018, 11, 361–371. [Google Scholar] [CrossRef]
- Pearce, A.; Lockwood, C.; Van Den Heuvel, C.; Pearce, J. The use of therapeutic magnesium for neuroprotection during global cerebral ischemia associated with cardiac arrest and cardiac surgery in adults: A systematic review. JBI Evid. Synth. 2017, 15, 86–118. [Google Scholar] [CrossRef]
- Momeni, M.; Khalifa, C.; Lemaire, G.; Watremez, C.; Tircoveanu, R.; Van Dyck, M.; Kahn, D.; Martins, M.R.; Mastrobuoni, S.; De Kerchove, L.; et al. Propofol plus low-dose dexmedetomidine infusion and postoperative delirium in older patients undergoing cardiac surgery. Br. J. Anaesth. 2021, 126, 665–673. [Google Scholar] [CrossRef]
- Hudetz, J.A.; Iqbal, Z.; Gandhi, S.D.; Patterson, K.M.; Byrne, A.J.; Hudetz, A.G.; Pagel, P.S.; Warltier, D.C. Ketamine attenuates post-operative cognitive dysfunction after cardiac surgery. Acta Anaesthesiol. Scand. 2009, 53, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Gamberini, M.; Bolliger, D.; Buse, G.A.L.; Burkhart, C.; Grapow, M.; Gagneux, A.; Filipovic, M.; Seeberger, M.; Pargger, H.; Siegemund, M.; et al. Rivastigmine for the prevention of postoperative delirium in elderly patients undergoing elective cardiac surgery—A randomized controlled trial. Crit. Care Med. 2009, 37, 1762–1768. [Google Scholar] [CrossRef]
- Kiabi, F.H.; Soleimani, A.; Habibi, M.R. Neuroprotective Effect of Low Mean Arterial Pressure on Postoperative Cognitive Deficit Attenuated by Prolonged Coronary Artery Bypass Time: A Meta-Analysis. Braz. J. Cardiovasc. Surg. 2019, 34, 739–748. [Google Scholar] [CrossRef] [PubMed]
- Sedrakyan, A.; Wu, A.W.; Parashar, A.; Bass, E.B.; Treasure, T. Off-pump surgery is associated with reduced occurrence of stroke and other morbidity as compared with traditional coronary artery bypass grafting: A meta-analysis of systematically reviewed trials. Stroke 2006, 37, 2759–2769. [Google Scholar] [CrossRef] [PubMed]
- Leshnower, B.G.; Rangaraju, S.; Allen, J.W.; Stringer, A.Y.; Gleason, T.G.; Chen, E.P. Deep Hypothermia with Retrograde Cerebral Perfusion Versus Moderate Hypothermia With Antegrade Cerebral Perfusion for Arch Surgery. Ann. Thorac. Surg. 2019, 107, 1104–1110. [Google Scholar] [CrossRef]
- Gasparovic, H.; Kopjar, T.; Rados, M.; Anticevic, A.; Rados, M.; Malojcic, B.; Ivancan, V.; Fabijanic, T.; Cikes, M.; Milicic, D.; et al. Impact of remote ischemic preconditioning preceding coronary artery bypass grafting on inducing neuroprotection. J. Thorac. Cardiovasc. Surg. 2019, 157, 1466–1476.e3. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Health Disorders, 5th ed.; American Psychiatric Association: Arlington, TX, USA, 2020; 90p. [Google Scholar]
- Berger, M.; Terrando, N.; Smith, S.K.; Browndyke, J.N.; Newman, M.F.; Mathew, J.P. Neurocognitive function after cardiac surgery: From phenotypes to mechanisms. Anesthesiology 2018, 129, 829–851. [Google Scholar] [CrossRef] [PubMed]
- Raffa, G.M.; Agnello, F.; Occhipinti, G.; Miraglia, R.; Re, V.L.; Marrone, G.; Tuzzolino, F.; Arcadipane, A.; Pilato, M.; Luca, A. Neurological complications after cardiac surgery: A retrospective case-control study of risk factors and outcome. J. Cardiothorac. Surg. 2019, 14, 23. [Google Scholar] [CrossRef] [PubMed]
- Leary, M.C.; Varade, P. Perioperative Stroke. Curr. Neurol. Neurosci. Rep. 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, M.; Rahouma, M.; Di Mauro, M.; Yanagawa, B.; Abouarab, A.; Demetres, M.; Di Franco, A.; Arisha, M.J.; Ibrahim, D.A.; Baudo, M.; et al. Early Versus Delayed Stroke After Cardiac Surgery: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2019, 8, e012447. [Google Scholar] [CrossRef] [PubMed]
- Sugimura, Y.; Sipahi, N.F.; Mehdiani, A.; Petrov, G.; Awe, M.; Minol, J.P.; Boeken, U.; Korbmacher, B.; Lichtenberg, A.; Dalyanoglu, H. Risk and Consequences of Postoperative Delirium in Cardiac Surgery. Thorac. Cardiovasc. Surg. 2020, 68, 417–424. [Google Scholar] [CrossRef]
- Reiche, S.; Mpanya, D.; Vanderdonck, K.; Mogaladi, S.; Motshabi-Chakane, P.; Tsabedze, N. Perioperative outcomes of coronary artery bypass graft surgery in Johannesburg, South Africa. J. Cardiothorac. Surg. 2021, 16, 1–8. [Google Scholar] [CrossRef]
- Patel, A.; Berdunov, V.; Quayyum, Z.; King, D.; Knapp, M.; Wittenberg, R. Estimated societal costs of stroke in the UK based on a discrete event simulation. Age Ageing 2020, 49, 270–276. [Google Scholar] [CrossRef] [Green Version]
- Newman, M.F.; Mathew, J.P.; Grocott, H.P.; Mackensen, G.B.; Monk, T.; Welsh-Bohmer, K.A.; Blumenthal, J.A.; Laskowitz, D.T.; Mark, D. Central nervous system injury associated with cardiac surgery. Lancet 2006, 368, 694–703. [Google Scholar] [CrossRef]
- Krause, M.; Morabito, J.E.; Mackensen, G.B.; Perry, T.E.; Bartels, K. Current neurologic assessment and neuroprotective strategies in cardiac anesthesia: A Survey to the membership of the Society of Cardiovascular Anesthesiologists. Anesth. Analg 2020, 131, 518–526. [Google Scholar] [CrossRef]
- Indja, B.; Seco, M.; Seamark, R.; Kaplan, J.; Bannon, P.G.; Grieve, S.M.; Vallely, M.P. Neurocognitive and psychiatric issues post cardiac surgery. Heart Lung Circ. 2017, 26, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Minhas, J.; Chung, E. Risk Factors Associated with cognitive decline after cardiac surgery: A systematic review. Cardiovasc. Psychiatry Neurol. 2015, 2015, 370612. [Google Scholar] [CrossRef] [PubMed]
- Hogue, C.W.; Palin, C.A.; Arrowsmith, J.E. Cardiopulmonary bypass management and neurologic outcomes: An evidence-based appraisal of current practices. Anesth. Analg. 2006, 103, 21–37. [Google Scholar] [CrossRef] [Green Version]
- Hogue, C.W.; Gottesman, R.F.; Stearns, J. Mechanisms of cerebral injury from cardiac surgery. Crit. Care Clin. 2008, 24, 83–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salameh, A.; Dhein, S.; Dähnert, I.; Klein, N. Neuroprotective strategies during cardiac surgery with cardiopulmonary bypass. Int. J. Mol. Sci. 2016, 17, 1945. [Google Scholar] [CrossRef] [Green Version]
- Blauth, C.I. Macroemboli and microemboli during cardiopulmonary bypass. Ann. Thorac. Surg. 1995, 59, 1300–1303. [Google Scholar] [CrossRef]
- Stroobant, N.; Van Nooten, G.; Van Belleghem, Y.; Vingerhoets, G. The effect of CABG on neurocognitive functioning. Acta Cardiol. 2010, 65, 557–564. [Google Scholar] [CrossRef]
- Arrowsmith, J.E.; Grocott, H.P.; Reves, J.G.; Newman, M.F. Central nervous system complications of cardiac surgery. Br. J. Anaesth. 2000, 84, 378–393. [Google Scholar] [CrossRef] [Green Version]
- Barbut, D.; Yao, F.; Hager, D.; Kavanaugh, P.; Trifiletti, R.; Gold, J. Comparison of transcranial doppler ultrasonography and transesophageal echocardiography to monitor emboli during coronary artery bypass surgery. Stroke 1996, 27, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Pugsley, W.; Klinger, L.; Paschalis, C.; Treasure, T.; Harrison, M.; Newman, S. The impact of microemboli during cardiopulmonary bypass on neuropsychological functioning. Stroke 1994, 25, 1393–1399. [Google Scholar] [CrossRef] [Green Version]
- Stump, D.A.; Rogers, A.T.; Hammon, J.W.; Newman, S.P. Cerebral emboli and cognitive outcome after cardiac surgery. J. Cardiothorac. Vasc. Anesth. 1996, 10, 113–119. [Google Scholar] [CrossRef]
- Murphy, G.J.; Angelini, G.D. Side effects of cardiopulmonary bypass: What is the reality? J. Card. Surg. 2004, 19, 481–488. [Google Scholar] [CrossRef] [PubMed]
- White, M.G.; Luca, L.E.; Nonner, D.; Saleh, O.; Hu, B.; Barrett, E.F.; Barrett, J.N. Cellular mechanisms of neuronal damage from hyperthermia. Prog. Brain Res. 2007, 162, 347–371. [Google Scholar] [CrossRef]
- Giacco, F.; Brownlee, M. Oxidative stress and diabetic complications. Circ. Res. 2010, 107, 1058–1070. [Google Scholar] [CrossRef] [Green Version]
- Yerneni, K.K.; Bai, W.; Khan, B.V.; Medford, R.M.; Natarajan, R. Hyperglycemia-induced activation of nuclear transcription factor kappaB in vascular smooth muscle cells. Diabetes 1999, 48, 855–864. [Google Scholar] [CrossRef]
- González-Moreno, E.I.; Cámara-Lemarroy, C.R.; González-González, J.G.; Góngora-Rivera, F. Glycemic variability and acute ischemic stroke: The missing link? Transl. Stroke Res. 2014, 5, 638–646. [Google Scholar] [CrossRef]
- Klamt, J.G.; Vicente, W.V.; Garcia, L.V.; Carmona, F.; Abrão, J.; Menardi, A.C.; Manso, P.H. Neuroprotective Anesthesia Regime and Intensive Management for Pediatric Cardiac Surgery with Cardiopulmonary Bypass: A Review and Initial Experience. Braz. J. Vardiovasc Surg. 2017, 32, 523–529. [Google Scholar]
- Lanier, W.L. The prevention and treatment of cerebral ischemia. Can. J. Anesth. 1999, 46 Pt 2, R46–R56. [Google Scholar] [CrossRef] [Green Version]
- Brambrink, A.M.; Koerner, I.P.; Diehl, K.; Strobel, G.; Noppens, R.; Kempski, O. The antibiotic erythromycin induces tolerance against transient global cerebral ischemia in rats (pharmacologic preconditioning). Anesthesiology 2006, 104, 1208–1215. [Google Scholar] [CrossRef] [PubMed]
- Katayama, Y.; Inaba, T.; Nito, C.; Ueda, M. Neuroprotective effects of erythromycin on ischemic injury following permanent focal cerebral ischemia in rats. Neurol. Res. 2016, 38, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Thomaidou, E.; Argiriadou, H.; Vretzakis, G.; Megari, K.; Taskos, N.; Chatzigeorgiou, G.; Anastasiadis, K. Perioperative use of erythromycin reduces cognitive decline after coronary artery bypass grafting surgery: A pilot study. Clin. Neuropharmacol. 2017, 40, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Koutsogiannidis, C.-P.C.; Johnson, E.O. Pharmacological neuroprotection in cardiac surgery: Effectiveness of pharmacologic-preconditioning with erythromycin. Curr. Vasc. Pharmacol. 2018, 16, 329–335. [Google Scholar] [CrossRef]
- Sykora, M.; Siarnik, P.; Diedler, J.; Lees, K.R.; Alexandrov, A.; Bath, P.M.; Bluhmki, E.; Bornstein, N.; Claesson, L.; Davis, S.M.; et al. β-Blockers, Pneumonia, and Outcome After Ischemic Stroke. Stroke 2015, 46, 1269–1274. [Google Scholar] [CrossRef] [Green Version]
- Padma, M.V. Angiotensin-converting enzyme inhibitors will help in improving stroke outcome if given immediately after stroke. Ann. Indian Acad. Neurol. 2010, 13, 156–159. [Google Scholar] [CrossRef]
- Lakič, N.; Mrak, M.; Šušteršič, M.; Rakovec, P.; Bunc, M. Perioperative erythropoietin protects the CNS against ischemic lesions in patients after open heart surgery. Wien. Klin. Wochenschr. 2016, 128, 875–881. [Google Scholar] [CrossRef]
- Koerner, I.P.; Brambrink, A.M. Brain protection by anesthetic agents. Curr. Opin. Anaesthesiol. 2006, 19, 481–486. [Google Scholar] [CrossRef]
- Jovin, D.; Katlaps, K.G.; Ellis, B.K.; Dharmaraj, B. Neuroprotection against stroke and encephalopathy after cardiac surgery. Interv. Med. Appl. Sci. 2019, 11, 27–37. [Google Scholar] [CrossRef]
- Rath, G.; Dash, H.; Suri, A.; Chandra, P.; Mahajan, A.; Mahajan, C.; Chouhan, R. Effect of intraoperative brain protection with propofol on postoperative cognition in patients undergoing temporary clipping during intracranial aneurysm surgery. Neurol. India 2014, 62, 262–268. [Google Scholar] [CrossRef]
- Matchett, G.A.; Allard, M.W.; Martin, R.D.; Zhang, J.H. Neuroprotective effect of volatile anesthetic agents: Molecular mechanisms. Neurol. Res. 2009, 31, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Zorrilla-Vaca, A.; Núñez-Patiño, R.A.; Torres, V.; Salazar-Gomez, Y. The Impact of Volatile Anesthetic Choice on Postoperative Outcomes of Cardiac Surgery: A Meta-Analysis. BioMed Res. Int. 2017, 2017, 7073401. [Google Scholar] [CrossRef] [Green Version]
- Mullan, C.; Catalano, M.; Manetta, F. Neuroprotective Strategies in Repair and Replacement of the Aortic Arch. Int. J. Angiol. 2018, 27, 098–109. [Google Scholar] [CrossRef]
- Mathew, J.P.; Mackensen, G.B.; Phillips-Bute, B.; Grocott, H.P.; Glower, D.D.; Laskowitz, D.T.; Blumenthal, J.A.; Newman, M.F. Randomized, double-blinded, placebo controlled study of neuroprotection with lidocaine in cardiac surgery. Stroke 2009, 40, 880–887. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Foo, I. Is intravenous lidocaine protective against myocardial ischaemia and reperfusion injury after cardiac surgery? Ann. Med. Surg. 2020, 59, 72–75. [Google Scholar] [CrossRef]
- Avidan, M.S.; Maybrier, H.R.; Ben Abdallah, A.; Jacobsohn, E.; Vlisides, P.E.; Pryor, K.; Veselis, R.A.; Grocott, H.P.; Emmert, D.A.; Rogers, E.M.; et al. Intraoperative ketamine for prevention of postoperative delirium or pain after major surgery in older adults: An international, multicentre, double-blind, randomised clinical trial. Lancet 2017, 390, 267–275. [Google Scholar] [CrossRef]
- Grocott, H.P.; Nussmeier, N.A. Neuroprotection in cardiac surgery. Anesthesiol. Clin. N. Am. 2003, 21, 487–509. [Google Scholar] [CrossRef]
- Durgut, K.; Hosgor, K.; Gormus, N.; Ozergin, U.; Solak, H. The cerebroprotective effects of pentoxifylline and aprotinin during cardiopulmonary bypass in dogs. Perfusion 2004, 19, 101–106. [Google Scholar] [CrossRef]
- Wang, Y.; Han, R.; Zuo, Z. Dexmedetomidine–induced neuroprotection: Is it translational? Transl. Perioper. Pain Med. 2016, 1, 15–19. [Google Scholar]
- Choi, S.; Jerath, A.; Jones, P.; Avramescu, S.; Djaiani, G.; Syed, S.; Saha, T.; Kaustov, L.; Kiss, A.; D’Aragon, F.; et al. Cognitive Outcomes after DEXmedetomidine sedation in cardiac surgery: CODEX randomised controlled trial protocol. BMJ Open 2021, 11, e046851. [Google Scholar] [CrossRef]
- Bhudia, S.; Cosgrove, D.M.; Naugle, R.I.; Rajeswaran, J.; Lam, B.-K.; Walton, E.; Petrich, J.; Palumbo, R.C.; Gillinov, A.M.; Apperson-Hansen, C.; et al. Magnesium as a neuroprotectant in cardiac surgery: A randomized clinical trial. J. Thorac. Cardiovasc. Surg. 2006, 131, 853–861.e7. [Google Scholar] [CrossRef] [Green Version]
- Checchia, P.A.; Bronicki, R.A.; Muenzer, J.T.; Dixon, D.; Raithel, S.; Gandhi, S.; Huddleston, C.B. Nitric oxide delivery during cardiopulmonary bypass reduces postoperative morbidity in children—A randomized trial. J. Thorac. Cardiovasc. Surg. 2013, 146, 530–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dȩbska, G.; May, R.; Kicinska, A.; Szewczyk, A.; Elger, C.E.; Kunz, W. Potassium channel openers depolarize hippocampal mitochondria. Brain Res. 2001, 892, 42–50. [Google Scholar] [CrossRef]
- Simard, J.M.; Chen, M.; Tarasov, K.; Bhatta, S.; Ivanova, S.; Melnitchenko, L.; Tsymbalyuk, N.; West, G.A.; Gerzanich, V. Newly expressed SUR1-regulated NCCa-ATP channel mediates cerebral edema after ischemic stroke. Nat. Med. 2006, 12, 433–440. [Google Scholar] [CrossRef]
- Hong, J.-H.; Lee, H.; Lee, S.-R. Protective effect of resveratrol against neuronal damage following transient global cerebral ischemia in mice. J. Nutr. Biochem. 2016, 27, 146–152. [Google Scholar] [CrossRef]
- Yuen, C.-M.; Sun, C.-K.; Lin, Y.-C.; Chang, L.-T.; Kao, Y.-H.; Yen, C.-H.; Chen, Y.-L.; Tsai, T.-H.; Chua, S.; Shao, P.-L.; et al. Combination of cyclosporine and erythropoietin improves brain infarct size and neurological function in rats after ischemic stroke. J. Transl. Med. 2011, 9, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dijk, D.; Spoor, M.; Hijman, R.; Nathoe, H.M.; Borst, C.; Jansen, E.W.L.; Grobbee, D.E.; De Jaegere, P.P.T.; Kalkman, C.; Octopus Study Group. Cognitive and cardiac outcomes 5 years after off-pump vs on-pump coronary artery bypass graft surgery. JAMA 2007, 297, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Murphy, G.S.; Hessel, E.A.; Groom, R.C. Optimal perfusion during cardiopulmonary bypass: An evidence-based approach. Anesth. Analg. 2009, 108, 1394–1417. [Google Scholar] [CrossRef]
- Schell, R.M.; Kern, F.H.; Greeley, W.J.; Schulman, S.R.; Frasco, P.E.; Croughwell, N.D.; Newman, M.; Reves, J.G. Cerebral blood flow and metabolism during cardiopulmonary bypass. Anesth. Analg. 1993, 76, 849–865. [Google Scholar] [CrossRef] [PubMed]
- Tarakji, K.G. Temporal onset, risk factors, and outcomes associated with stroke after coronary artery bypass grafting. JAMA 2011, 305, 381–390. [Google Scholar] [CrossRef]
- Poon, S.S.; Estrera, A.; Oo, A.; Field, M. Is moderate hypothermic circulatory arrest with selective antegrade cerebral perfusion superior to deep hypothermic circulatory arrest in elective aortic arch surgery? Interact. Cardiovasc. Thorac. Surg. 2016, 23, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, W.A. Neuroprotection in cardiac surgery. Ann. Thorac. Surg. 2005, 79, S2254–S2256. [Google Scholar] [CrossRef]
- Stein, L.H.; Elefteriades, J.A. Protecting the brain during aortic surgery: An enduring debate with unanswered questions. J. Cardiothorac. Vasc. Anesth. 2010, 24, 316–321. [Google Scholar] [CrossRef]
- Angeloni, E.; Benedetto, U.; Takkenberg, J.; Stigliano, I.; Roscitano, A.; Melina, G.; Sinatra, R. Unilateral versus bilateral antegrade cerebral protection during circulatory arrest in aortic surgery: A meta-analysis of 5100 patients. J. Thorac. Cardiovasc. Surg. 2014, 147, 60–67. [Google Scholar] [CrossRef] [Green Version]
- Yan, T.D.; Bannon, P.G.; Bavaria, J.; Coselli, J.S.; Elefteriades, J.A.; Griepp, R.B.; Hughes, G.C.; Lemaire, S.A.; Kazui, T.; Kouchoukos, N.T.; et al. Consensus on hypothermia in aortic arch surgery. Ann. Cardiothorac. Surg. 2013, 2, 163–168. [Google Scholar] [CrossRef]
- Etz, C.D.; Plestis, K.A.; Kari, F.A.; Silovitz, D.; Bodian, C.A.; Spielvogel, D.; Griepp, R.B. Axillary cannulation significantly improves survival and neurologic outcome after atherosclerotic aneurysm repair of the aortic root and ascending aorta. Ann. Thorac. Surg. 2008, 86, 441–447. [Google Scholar] [CrossRef]
- Das, S. Can epiaortic ultrasound reduce the incidence of intraoperative stroke during cardiac surgery? Interact. Cardiovasc. Thorac. Surg. 2004, 3, 71–75. [Google Scholar] [CrossRef] [Green Version]
- Day, J.; Taylor, K. The systemic inflammatory response syndrome and cardiopulmonary bypass. Int. J. Surg. 2005, 3, 129–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrokhi, F.; Smiley, D.; Umpierrez, G.E. Glycemic control in non-diabetic critically ill patients. Best Pr. Res. Clin. Endocrinol. Metab. 2011, 25, 813–824. [Google Scholar] [CrossRef] [Green Version]
- McCowen, K.C.; Malhotra, A.; Bistrian, B.R. Stress-induced hyperglycemia. Crit. Care Clin. 2001, 17, 107–124. [Google Scholar] [CrossRef]
- Reves, J.G.; Karp, R.B.; Buttner, E.E.; Tosone, S.; Smith, L.R.; Samuelson, P.N.; Kreusch, G.R.; Oparil, S. Neuronal and adrenomedullary catecholamine release in response to cardiopulmonary bypass in man. Circulation 1982, 66, 49–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grocott, H.P.; Yoshitani, K. Neuroprotection during cardiac surgery. J. Anesth. 2007, 21, 367–377. [Google Scholar] [CrossRef] [PubMed]
- Mair, G.; Wardlaw, J.M. Imaging of acute stroke prior to treatment: Current practice and evolving techniques. Br. J. Radiol. 2014, 87, 20140216. [Google Scholar] [CrossRef] [Green Version]
- Kloska, S.P.; Nabavi, D.G.; Gaus, C.; Nam, E.-M.; Klotz, E.; Ringelstein, E.B.; Heindel, W. Acute stroke assessment with CT: Do we need multimodal evaluation? Radiology 2004, 233, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Potter, C.A.; Vagal, A.S.; Goyal, M.; Nunez, D.B.; Leslie-Mazwi, T.M.; Lev, M.H. CT for Treatment Selection in Acute Ischemic Stroke: A Code Stroke Primer. Radiographics 2019, 39, 1717–1738. [Google Scholar] [CrossRef]
- Wannamaker, R.; Buck, B.; Butcher, K. Multimodal CT in Acute Stroke. Curr. Neurol. Neurosci. Rep. 2019, 19, 63. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.J.; Wintermark, M. Perfusion Computed Tomography for the Evaluation of Acute Ischemic Stroke. Stroke 2016, 47, 1153–1158. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.J.; Kang, H.G.; Kim, H.-J.; Ahn, S.-H.; Kim, N.Y.; Warach, S.; Kang, D.-W. Magnetic resonance imaging in acute ischemic stroke treatment. J. Stroke 2014, 16, 131–145. [Google Scholar] [CrossRef] [Green Version]
- Ospel, J.M.; Menon, B.K.; Qiu, W.; Kashani, N.; Mayank, A.; Singh, N.; Cimflova, P.; Marko, M.; Nogueira, R.G.; McTaggart, R.A.; et al. A Detailed Analysis of Infarct Patterns and Volumes at 24-h Noncontrast CT and Diffusion-weighted MRI in Acute Ischemic Stroke Due to Large Vessel Occlusion: Results from the ESCAPE-NA1 Trial. Radiology 2021, 300, 152–159. [Google Scholar] [CrossRef]
- Heiss, W.-D. Radionuclide imaging in ischemic stroke. J. Nucl. Med. 2014, 55, 1831–1841. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Author & Publication Year | Intervention | Placebo/Standard Care | Outcome | Results |
|---|---|---|---|---|
| Habibi et al. [5], 2018 | Lidocaine* n = 340 | Normal saline infusion n = 348 | Development of POCD (decline of >1 SD postoperatively when compared to preoperative baseline)
| POCD: 29% for the lidocaine group and 39% for the control. Lidocaine use reduced POCD. Better outcomes were in younger patients, male gender, more prolonged CPB, and higher concentrations of lidocaine. |
| Pearce et al. [6], 2017 | Magnesium* n = 582 | Normal saline n = 582 | Functional neurological assessment
| The measurement of neurological outcomes varied in the different studies. Use of different doses at induction of anaesthesia, up to 48 h post-surgery. Methodological heterogeneity existed in these studies. There were improved functional neurological outcomes in the magnesium group for patients with global ischaemia, but magnesium does not improve long-term cognitive function. |
Neurophysiological assessment
| ||||
Neuropsychological assessment
| ||||
| Chen et al. [2], 2017 | Inhalational/Volatile agents
| TIVA techniques
| Serum protein S100B levels were the primary outcome measure. | Levels of S100B protein were lower in the Inhalational group when compared to the TIVA group. MMSE scores were higher in the inhalational agents’ group. No significance between inhalational and TIVA group in SjVO2, D (a-v)O2 and O2ER |
Secondary outcomes:
| ||||
| Momeni et al. [7], 2021 | Propofol plus dexmedetomidine infusion n = 204 | Propofol plus standard saline infusion n = 207 | Incidence of POD:
| POD occurred in 18% of dexmedetomidine and in 19% of the placebo group. These results did not show any statistical significance. |
| Hudetz et al. [8], 2009 | Ketamine bolus at induction n = 26 | Normal saline n = 26 Non-surgical group n = 26 | Neurocognitive and neurological testing:
| A decrease in cognitive function by at least 2 standard deviations in the placebo group vs. ketamine group when compared to non-surgical controls was observed. |
Depression:
| ||||
Vascular dementia:
| ||||
| Gamberini et al. [9], 2009 | Rivastigmine* n = 57 | Placebo n = 56 | Delirium screening:
| There was no difference between the rivastigmine and placebo groups. Delirium occurred in 17 patients (30%) of the placebo group and 18 patients (32%) of the rivastigmine group. |
Cognitive assessment:
| ||||
| Kiabi et al. [10], 2019 | MAP < 80 mmHg | MAP 80 ≥ mmHg | Incidence of POCD:
| POCD occurred in 6.4% of all cases. The maintenance of low MAP was not associated with a decline in POCD. A shorter duration of CPB was associated with a reduction in POCD regardless of the groups (lower MAP vs. standard of care). |
| Sedrakyan et al. [11], 2006 | Off-pump CABG | On-pump CABG | Postoperative strokes | Off-pump was associated with the least occurrences of strokes. |
| Leshnower et al. [12], 2019 | Deep hypothermic circulatory arrest (DHCA) with retrograde cerebral perfusion (RCP) * n = 11 | Moderate hypothermic circulatory arrest (MHCA) with antegrade cerebral perfusion (ACP) -cooled to nasopharyngeal temperatures of 20 °C to 28 °C n = 9 | Neurological examination and classification:
| There was no clinically significant neurological injury present in both groups. Clinical parameters and S-100 levels were very similar; however, MRI DWI lesions that are consistent with acute cerebral infarction were present in 45% of the DHCA + RCP compared to 100% of MHCA + ACP |
National Institute of Health stroke scale (NIHSS)
| ||||
| Serum levels of S-100 MRI examination with diffusion-weighted imaging (DWI) | ||||
| Gasparovic et al. [13], 2019 | Remote ischaemic preconditioning (RIPC)* n = 33 | Standard care n = 33 | Structural and functional cerebral changes:
| No statistically significant difference between the two groups. New brain ischaemia occurred in 9 patients (27%) of the RIPC group versus eight patients (24%) of the control group. |
Neurocognitive testing:
| ||||
| Uysal et al. [4], 2020 | Cerebral oxygenation monitoring* n = 59 | Control group: Cerebral oxygenation information was hidden from investigators No intervention protocol n = 66 | Cognitive testing: Cognitive Stability Index HeadMinder battery (HeadMinder, Inc, New York, NY, USA)
| No significant differences in cognition existed between the intervention and control group at T2. The mean memory score at T3 was better in the intervention group. |
| Preoperative Strategies |
| |
| Intraoperative Strategies | Non-pharmacological
| Pharmacological
|
| Postoperative Strategies |
| |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Motshabi-Chakane, P.; Mogane, P.; Moutlana, J.; Leballo-Mothibi, G.; Dingezweni, S.; Mpanya, D.; Tsabedze, N. Contemporary Neuroprotection Strategies during Cardiac Surgery: State of the Art Review. Int. J. Environ. Res. Public Health 2021, 18, 12747. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312747
Motshabi-Chakane P, Mogane P, Moutlana J, Leballo-Mothibi G, Dingezweni S, Mpanya D, Tsabedze N. Contemporary Neuroprotection Strategies during Cardiac Surgery: State of the Art Review. International Journal of Environmental Research and Public Health. 2021; 18(23):12747. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312747
Chicago/Turabian StyleMotshabi-Chakane, Palesa, Palesa Mogane, Jacob Moutlana, Gontse Leballo-Mothibi, Sithandiwe Dingezweni, Dineo Mpanya, and Nqoba Tsabedze. 2021. "Contemporary Neuroprotection Strategies during Cardiac Surgery: State of the Art Review" International Journal of Environmental Research and Public Health 18, no. 23: 12747. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312747