
Prevalence of Unmet Healthcare Needs in Adolescents and Associated Factors: Data from the Seventh Korea National Health and Nutrition Examination Survey (2016–2018)


Abstract
:1. Introduction
2. Materials and Methods
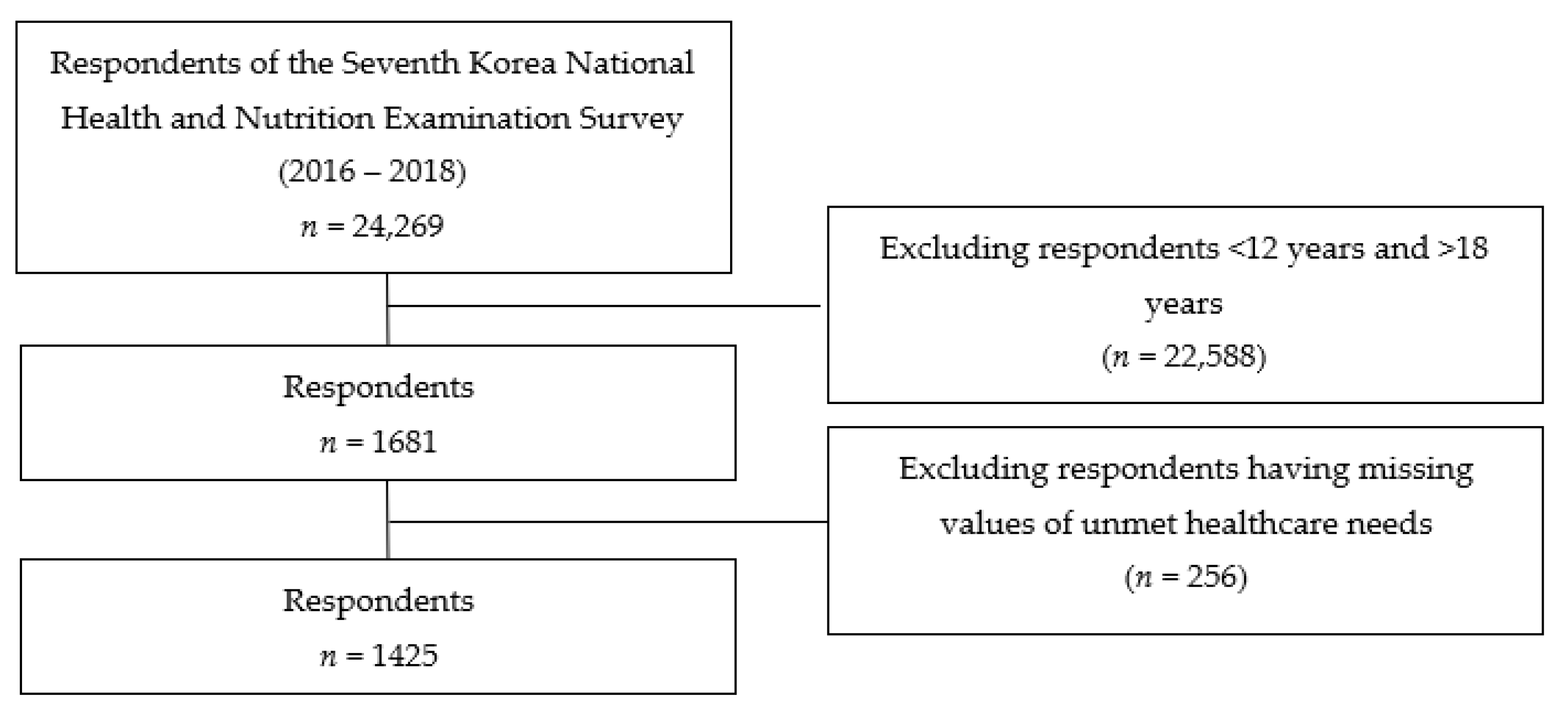
2.1. Study Design and Data Source
2.2. Variables
2.2.1. Dependent Variable
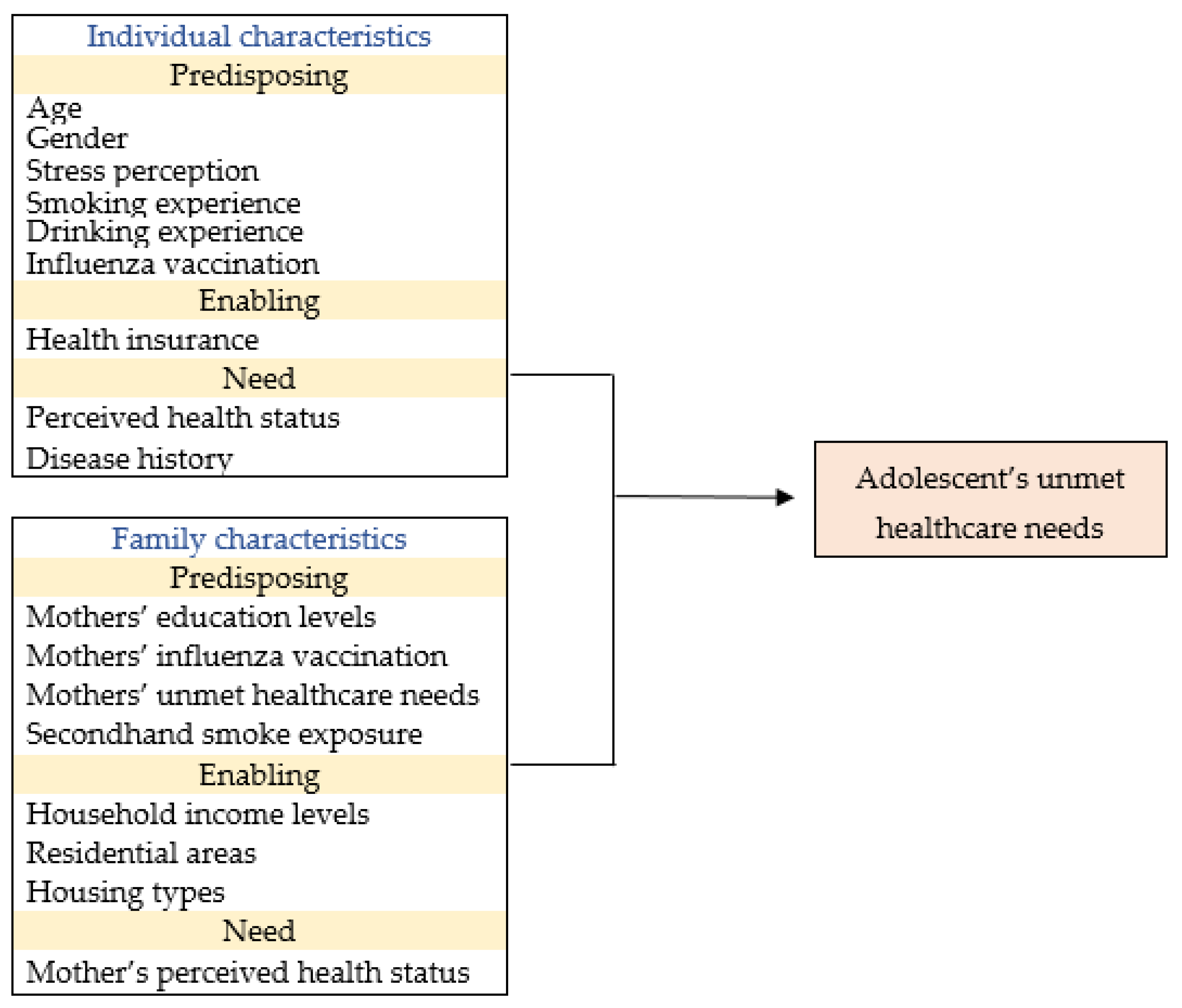
2.2.2. Independent Variable
2.3. Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jung, Y.H.; Byon, L.; Ko, S. Lifetime Distribution of Medical Cost in Korea. Health Soc. Welf. Rev. 2011, 31, 194–216. [Google Scholar] [CrossRef]
- Health and Nutrition Investigation Division of the Korea Disease Control and Prevention Agency. Major Results of the 12th Online Survey on Youth Health Behavior. 2016. Available online: http://www.mohw.go.kr/upload/viewer/skin/doc.html?fn=1478220716571_20161104095156.hwp&rs=/upload/viewer/result/202110/ (accessed on 28 August 2021).
- Case, A.; Fertig, A.; Paxson, C. The Lasting Impact of Childhood Health and Circumstance. J. Health Econ. 2005, 24, 365–389. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.P. The Impact of Childhood Health on Adult Labor Market Outcomes. Rev. Econ. Stat. 2009, 91, 478–489. [Google Scholar] [CrossRef] [Green Version]
- Huh, S.I. Changes in the Financial Burden of Health Expenditures by Income Level. Health Welf. Policy Forum 2009, 149, 48. [Google Scholar]
- Hargreaves, D.S.; Elliott, M.N.; Viner, R.M.; Richmond, T.K.; Schuster, M.A. Unmet Health Care Need in US Adolescents and Adult Health Outcomes. Pediatrics 2015, 136, 513–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.A.; Seo, Y.; Woo, K.S.; Shin, Y.-j. A Systematic Review of Studies on Current Status and Influencing Factors of Unmet Medical Needs in Korea. J. Crit. Soc. Welf. 2019, 62, 53–92. [Google Scholar] [CrossRef]
- Jung, S.; Paik, S.; Kim, J. Relationship between Medical Screening and Unmet Healthcare Needs: Using KNHANES(Korea National Health and Nutrition Examination Survey). Korean Soc. Hosp. Manag. 2019, 24, 1–12. Available online: https://kiss-kstudy-com-ssl.access.yonsei.ac.kr:8443/thesis/thesis-view.asp?key=3734952 (accessed on 17 May 2021).
- Marshall, E.G.P.D. Do Young Adults Have Unmet Healthcare Needs? J. Adolesc. Health 2011, 49, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Irvin, K.; Fahim, F.; Alshehri, S.; Kitsantas, P. Family Structure and Children’s Unmet Health-Care Needs. J. Child Health Care Prof. Work. Child. Hosp. Community 2018, 22, 57–67. [Google Scholar] [CrossRef] [Green Version]
- Mmari, K.; Marshall, B.; Hsu, T.; Shon, J.W.; Eguavoen, A. A Mixed Methods Study to Examine the Influence of the Neighborhood Social Context on Adolescent Health Service Utilization. BMC Health Serv. Res. 2016, 16, 433. [Google Scholar] [CrossRef] [Green Version]
- Choi, M.; Park, H.; Lee, B.; Jeong, S.; Park, J. The relationship between oral health behavior and dental services utilization in Korean adolescents. J. Korean Soc. Dent. Hyg. 2010, 10, 851–860. Available online: https://scienceon.kisti.re.kr/srch/selectPORSrchArticle.do?cn=JAKO201008237288429&SITE=CLICK (accessed on 17 May 2021).
- Zarychta, K.; Mullan, B.; Luszczynska, A. It Doesn’t Matter What They Say, It Matters How They Behave: Parental Influences and Changes in Body Mass Among Overweight and Obese Adolescents. Appetite 2016, 96, 47–55. [Google Scholar] [CrossRef]
- Sanchez, A.; Norman, G.J.; Sallis, J.F.; Calfas, K.J.; Cella, J.; Patrock, K. Patterns and Correlates of Physical Activity and Nutrition Behaviors in Adolescents. Am. J. Prev. Med. 2007, 32, 124–130. [Google Scholar] [CrossRef] [Green Version]
- Kwon, S.; Kin, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Chio, S.; Chun, C.; Khang, Y.H.; Oh, K. Data Resource Profile: The Korea National Health and Nutrition Examination Survey(KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Andersen, R.; Newman, J.F. Societal and individual determinants of medical care utilization in the United States. Milbank MEMorial Fund Quarterly. Health Soc. 1973, 51, 95–124. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y. Factors of Long Term Care Service Use by the Elderly. Health Soc. Welf. Rev. 2009, 29, 182–200. [Google Scholar] [CrossRef]
- Andersen, R.; Newman, J.F. Societal and individual determinants of medical care utilization in the United States. The Milbank Qquarterly. 2005, 83, 1–28. [Google Scholar] [CrossRef]
- Statistics Canada. Unmet Health Care Needs. 2014. Available online: https://www150.statcan.gc.ca/n1/en/pub/82-625-x/2016001/article/14310-eng.pdf?st=ouLzMNz428 (accessed on 28 August 2021).
- European Commission. Children with Unmet Needs for Medical Examination or Treatment by Income Group, Household Composition and Degree of Urbanization. 2017. Available online: https://ec.europa.eu/eurostat/databrowser/view/ilc_hch14/default/table?lang=en (accessed on 28 August 2021).
- Parasuraman, S.R.; Anglin, T.M.; McLellan, S.E.; Riley, C.; Mann, M.Y. Health Care Utilization and Unmet Need Among Youth with Special Health Care Needs. J. Adolesc. Health 2018, 63, 435–444. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.; Huang, T.; Li, A.; Wang, Z. Does universal health insurance coverage reduce unmet healthcare needs in China? Evidence from the National Health Service Survey. Int. J. Equity Health 2021, 20, 43. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.; Wren, M. Unmet healthcare needs in Ireland: Analysis using the EU-SILC survey. Health Policy 2017, 121, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Scal, P. Are the Times A-Changing? Healthcare Coverage and Access for Adolescents and Young Adults Since the Affordable Care Act. J. Adolesc. Health 2018, 63, 381–382. [Google Scholar] [CrossRef]
- Griffith, K.N. Changes in Insurance Coverage and Access to Care for Young Adults in 2017. J. Adolesc. Health 2020, 66, 86–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, G.M.; Jin, S.; Moon, S.H. Exploratory Study on Factors of Unmet Medical Needs Using Data Mining Analysis. Korean Policy Stud. Rev. 2016, 25, 269–301. [Google Scholar]
- Hwang, J. Understanding reasons for unmet health care needs in Korea: What are health policy implications? BMC Health Serv. Res. 2018, 18, 557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Hou, F. Unmet needs for health care. Health Rep. 2002, 13, 23–34. [Google Scholar]
- Sibley, L.M.; Glazier, R.H. Reasons for Self-Reported Unmet Healthcare Needs in Canada: A Population-Based Provincial Comparison. Healthc. Policy 2009, 5, 87–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yun, J.; Kim, M.J.; Kim, J.-S. Parallel Multiple Mediating Effects of Academic Stress on the Relationship between Time Pressure and Subjective Well-Being of High School Students. Korean Educ. Inq. 2018, 36, 49–69. [Google Scholar] [CrossRef]
- Jang, J. Meausres to foster pediatrics to resolve medical blind spots. Res. Inst. Healthc. Policy 2015, 12, 58–64. [Google Scholar]
- Jang, M.; Cho, W.; Yoon, N.; Kwak, M.; Yoo, S. Identifying the Types of Collaboration in Community Health Promotion. Korean J. Health Educ. Promot. 2009, 26, 125–135. [Google Scholar]
- Oh, S.H. Presentation of the case of the Health Promotion Research School. In Proceedings of the Korea Public Health Association Comprehensive Academic Conference, Chungbuk, Korea, 14 October 2011; Publisher: Seoul, Korea, 2011; pp. 60–62. [Google Scholar]
- Green, C.; Jung, H.Y.; Wu, X.; Abramson, E.; Walkup, J.T.; Ford, J.S.; Grinspan, Z.M. Do Children with Special Health Care Needs with Anxiety have Unmet Health Care Needs? An Analysis of a National Survey. Matern. Child Health J. 2019, 23, 1220–1231. [Google Scholar] [CrossRef]
- Noh, E. Intergenerational Differences in Factors Affecting Unmet Health Care Needs in South Korea: Comparison of Middle-aged and Older Adults. J. Intergenerational Relatsh. 2021, 19, 144–162. [Google Scholar] [CrossRef]
- Kim, E.S.; Eun, S.J. Analysis of dental unmet needs medical research trends and influence factors: Using structural literature review. J. Korean Soc. Dent. Hyg. 2020, 20, 243–256. [Google Scholar] [CrossRef]
- Huh, S.I.; Lee, H.J. Unmet Health Care Needs and Attitudes towards Health Care System in Korea. Korean Health Econ. Rev. 2016, 22, 59–89. [Google Scholar]
- Ko, H. Unmet healthcare needs and health status: Panel evidence from Korea. Health Policy 2016, 120, 646–653. [Google Scholar] [CrossRef]
- Kress, H.G. Unmet needs in drug treatment of chronic severe pain-clinical evidence on current and future concepts. Eur. J. Pain Suppl. 2009, 3, 11–15. [Google Scholar] [CrossRef]
- Park, E.H.; Park, E.C.; Oh, D.H.; Cho, E. The Effect of Stress and Depression on Unmet Medical Needs. Korean J. Clin. Pharm. 2017, 27, 44–54. [Google Scholar] [CrossRef] [Green Version]
- Jung, B.; Ha, I.H. Determining the reasons for unmet healthcare needs in South Korea: A secondary data analysis. Health Qual. Life Outcomes 2021, 19, 99. [Google Scholar] [CrossRef]
- Jang, M.; Jung, Y.K. Research on the Brand Image of Apartment in Korea. J. Basic Des. Art 2003, 4, 344–353. [Google Scholar]
- Ministry of Land, Infrastructure and Transport. Occupation Type of Hosing by Region and Income Levels. 2019. Available online: http://stat.molit.go.kr/portal/cate/statView.do?hRsId=327&hFormId=5727&hSelectId=5727&hPoint=1&hAppr=1&hDivEng=&oFileName=&rFileName=&midpath=&month_yn=N&sFormId=5727&sStart=2019&sEnd=2019&sStyleNum=1&sDivEng=N&EXPORT= (accessed on 28 August 2021).
- Ministry of Land, Infrastructure and Transport. Housing Type by Administrative District. 2020. Available online: http://stat.molit.go.kr/portal/cate/statView.do?hRsId=327&hFormId=5403&hDivEng=&month_yn= (accessed on 28 August 2021).
- Kim, S.H.; Seo, G. A study on the resetting of vulnerable areas in emergency medical care using real-time traffic information big data. Mag. Korean Soc. Agric. Eng. 2021, 63, 27–34. [Google Scholar]
- Kwon, H.Y.; Jeong, H.J.; Lee, A.; Kim, J.H. External Medical Service Use among Children Living in Seoul. Seoul Stud. 2014, 15, 61–77. [Google Scholar]



{kind=link}
{kind=link}
| Adolescents’ Unmet Healthcare Needs | ||||||||
|---|---|---|---|---|---|---|---|---|
| Variables | n (%) | Yes | No | t/χ2 | p-Value | |||
| n (%) | n (%) | |||||||
| Total | 1425 (100.0) | 78 (5.5) | 1347 (94.5) | |||||
| Individual characteristics | ||||||||
| Predisposing factors | ||||||||
| Age (years): mean (SD) | 15.1 (2.1) | 14.9 (2.0) | −0.818 | 0.414 | ||||
| Gender | ||||||||
| Male | 738 (51.8) | 36 (46.2) | 702 (52.1) | 1.050 | 0.306 | |||
| Female | 687 (48.2) | 42 (53.8) | 645 (47.9) | |||||
| Stress perception (n = 1424) | ||||||||
| Low | 1020 (71.6) | 41 (52.6) | 979 (72.7) | 14.760 | <0.001 | |||
| High | 404 (28.4) | 37 (47.4) | 367 (27.3) | |||||
| Smoking experience (n = 1424) | ||||||||
| No | 1280 (89.9) | 65 (83.3) | 1215 (90.3) | 3.900 | 0.048 | |||
| Yes | 144 (10.1) | 13 (16.7) | 131 (9.7) | |||||
| Drinking experience (n = 1424) | ||||||||
| No | 1115 (78.3) | 53 (67.9) | 1062 (78.9) | 5.205 | 0.023 | |||
| Yes | 309 (21.7) | 25 (32.1) | 284 (21.1) | |||||
| Influenza vaccination (n = 1423) | ||||||||
| No | 1006 (70.7) | 64 (82.1) | 942 (70.0) | 5.137 | 0.023 | |||
| Yes | 417 (29.3) | 14 (17.9) | 403 (30.0) | |||||
| Enabling factors | ||||||||
| Health insurance | ||||||||
| None | 13 (0.9) | 2 (2.6) | 11 (0.8) | |||||
| National health Insurance | 1357 (95.2) | 73 (93.6) | 1284 (95.3) | 2.764 | 0.256 b | |||
| National Medicaid | 55 (3.9) | 3 (3.8) | 52 (3.9) | |||||
| Need factors | ||||||||
| Perceived health status | ||||||||
| Good | 1347 (94.5) | 65 (83.3) | 1282 (95.2) | - | <0.001 a | |||
| Poor | 78 (5.5) | 13 (16.7) | 65 (4.8) | |||||
| Disease history b (n = 1424) | ||||||||
| No | 678 (47.6) | 45 (57.7) | 633 (47.0) | 3.361 | 0.067 | |||
| Yes | 746 (52.4) | 33 (42.3) | 713 (53.0) | |||||
| Family characteristics | ||||||||
| Predisposing factors | ||||||||
| Mothers’ education level (n = 1230) | ||||||||
| ≤Middle school | 56 (4.6) | 4 (5.8) | 52 (4.5) | |||||
| high school | 528 (42.9) | 33 (47.8) | 495 (42.6) | 1.183 | 0.554 | |||
| ≥college | 646 (52.5) | 32 (46.4) | 614 (52.9) | |||||
| Mothers’ influenza vaccination (n = 1230) | ||||||||
| No | 956 (77.7) | 61 (88.4) | 895 (77.1) | 4.818 | 0.028 | |||
| Yes | 274 (22.3) | 8 (11.6) | 266 (22.9) | |||||
| Mothers’ unmet healthcare needs (n = 1199) | ||||||||
| No | 1116 (93.1) | 61 (92.4) | 1055 (93.1) | - | 0.802 a | |||
| Yes | 83 (6.9) | 5 (7.6) | 78 (6.9) | |||||
| Secondhand smoke exposure at home (n = 1423) | Secondhand smoke exposure at home (n = 1423) | |||||||
| No | 1274 (89.5) | 63 (80.8) | 1211 (90.0) | 6.755 | 0.009 | |||
| Yes | 149 (10.5) | 15 (19.2) | 134 (10.0) | |||||
| Enabling factors | ||||||||
| Household income level (n = 1423) | ||||||||
| Low | 193 (13.6) | 15 (19.5) | 178 (13.2) | 2.432 | 0.119 | |||
| High | 1230 (86.4) | 62 (80.5) | 1168 (86.8) | |||||
| Residential area | ||||||||
| Metropolitan city | 633 (44.4) | 36 (46.2) | 597 (44.3) | 0.100 | 0.751 | |||
| Regional area | 792 (55.6) | 42 (53.8) | 750 (55.7) | |||||
| Housing type (n = 1424) | ||||||||
| Apartment | 1027 (72.1) | 42 (53.8) | 985 (73.2) | |||||
| Detached house | 252 (17.7) | 26 (33.3) | 226 (16.8) | 15.787 | <0.001 | |||
| Multi-unit house and others | 145 (10.2) | 10 (12.8) | 135 (10.0) | |||||
| Need factors | ||||||||
| Mothers’ perceived health status (n = 1233) | ||||||||
| Good | 422 (34.2) | 24 (34.8) | 398 (34.2) | 0.010 | 0.920 | |||
| Poor | 811 (65.8) | 45 (65.2) | 766 (65.8) | |||||
| Adolescents’ Unmet Healthcare Needs | ||
|---|---|---|
| OR (95% CI) | p-Value | |
| Age | 0.843 (0.722–0.986) | 0.032 |
| Gender (ref = male) | ||
| female | 1.184 (0.695–2.016) | 0.534 |
| Stress perception (ref = low) | ||
| high | 2.054 (1.189–3.546) | 0.010 |
| Smoking experience (ref = no) | ||
| yes | 1.586 (0.662–3.799) | 0.300 |
| Drinking experience for a year (ref = no) | ||
| yes | 1.695 (0.820–3.507) | 0.154 |
| Influenza vaccination (ref = no) | ||
| yes | 0.636 (0.295–1.371) | 0.248 |
| Perceived health status (ref = good) | ||
| poor | 3.778 (1.734–8.229) | 0.001 |
| Disease history a (ref = no) | ||
| yes | 0.599 (0.349–1.027) | 0.063 |
| Mothers’ education level (ref = ≤middle school) | ||
| high school | 1.244 (0.396–3.907) | 0.708 |
| ≥college | 1.481(0.456–4.808) | 0.513 |
| Mother’s influenza vaccination (ref = no) | ||
| yes | 0.634(0.263–1.529) | 0.311 |
| Mothers’ unmet healthcare needs (ref = no) | ||
| yes | 0.864(0.293–2.550) | 0.791 |
| Secondhand smoke exposure at home (ref = no) | ||
| yes | 1.718(0.831–3.553) | 0.144 |
| Household income level (ref = low) | ||
| high | 0.785(0.365–1.686) | 0.534 |
| Residential area (ref = metropolitan city) | ||
| Regional area | 0.997(0.584–1.700) | 0.990 |
| Housing type (ref = apartment) | ||
| detached house | 2.916(1.592–5.341) | 0.001 |
| multi-unit house and others | 1.356(0.586–3.137) | 0.477 |
| Mothers’ perceived health status (ref = good) | ||
| poor | 0.913(0.525–1.588) | 0.748 |
| Reasons for Unmet Healthcare Needs | n | % |
|---|---|---|
| Not enough time to visit the hospital | 48 | 61.5 |
| Less severe symptoms | 25 | 32.1 |
| Financial problem Etc. a | 2 3 | 2.6 3.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.; Park, J. Prevalence of Unmet Healthcare Needs in Adolescents and Associated Factors: Data from the Seventh Korea National Health and Nutrition Examination Survey (2016–2018). Int. J. Environ. Res. Public Health 2021, 18, 12781. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312781
Park H, Park J. Prevalence of Unmet Healthcare Needs in Adolescents and Associated Factors: Data from the Seventh Korea National Health and Nutrition Examination Survey (2016–2018). International Journal of Environmental Research and Public Health. 2021; 18(23):12781. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312781
Chicago/Turabian StylePark, Hyeran, and Jeongok Park. 2021. "Prevalence of Unmet Healthcare Needs in Adolescents and Associated Factors: Data from the Seventh Korea National Health and Nutrition Examination Survey (2016–2018)" International Journal of Environmental Research and Public Health 18, no. 23: 12781. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312781