
Co-Design of a Neurodevelopment Assessment Scale: A Study Protocol

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
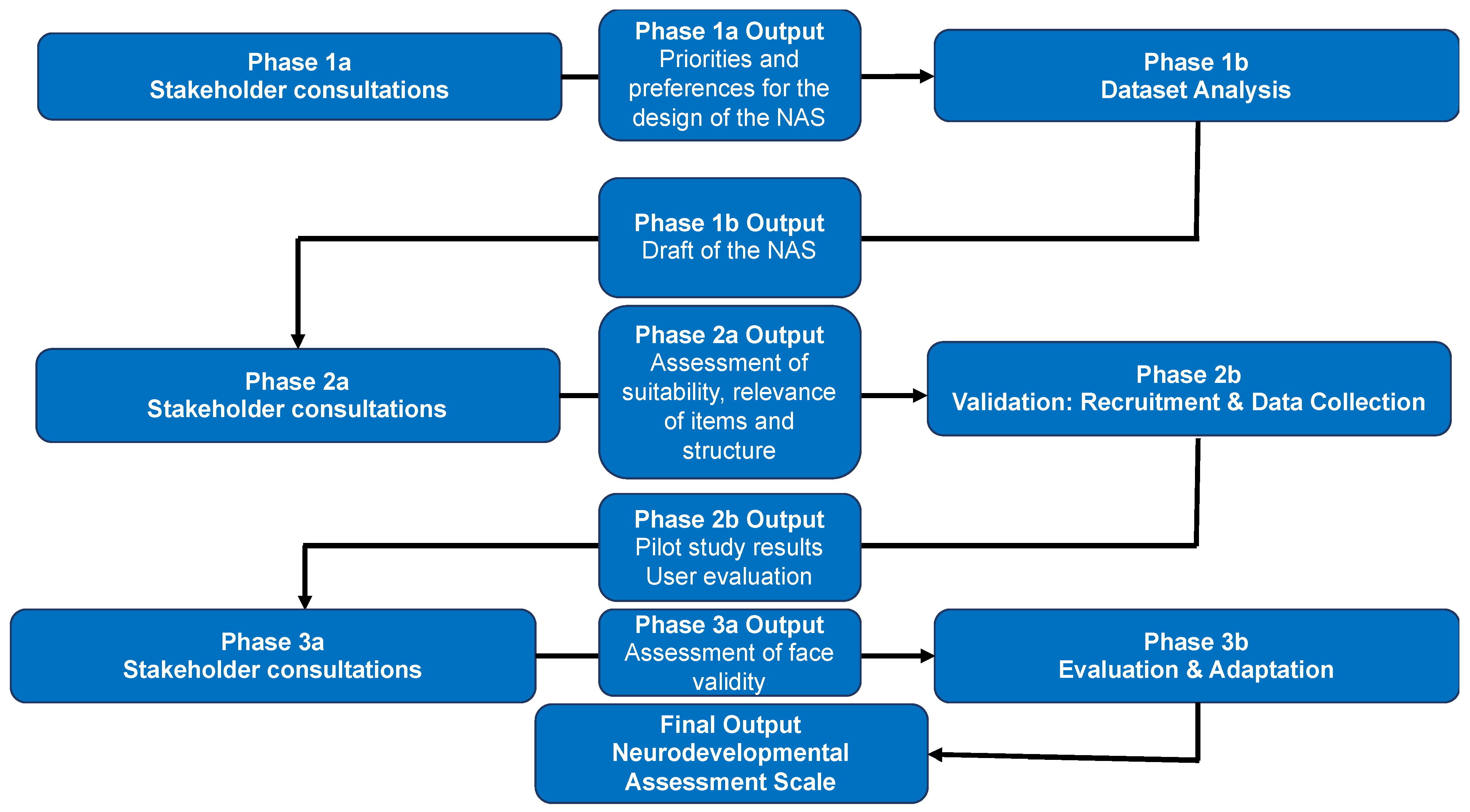
2.1. Study Design Overview
2.2. Study Setting, Population, and Duration
2.3. Study Procedures
2.3.1. Stakeholder/Community Consultations Phase 1a
2.3.2. NAS Development Phase 1b
2.3.3. Stakeholder/Community Consultations Phase 2a
2.3.4. NAS Development Phase 2b
2.3.5. Stakeholder/Community Consultations Phase 3a
2.3.6. NAS Development Phase 3b
3. Analysis Plan
3.1. Phase 1a: Stakeholder/Community Consultations
3.2. Phase 1b: Analysis of Existing Datasets
3.3. Phase 2a: Stakeholder/Community Consultations
3.4. Phase 2b: Validation: Recruitment and Data Collection
3.5. Phase 3a: Stakeholder/Community Consultations
3.6. Phase 3b: Evaluation and Adaptation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Olusanya, B.O.; Davis, A.C.; Wertlieb, D.; Boo, N.-Y.; Nair, M.K.; Halpern, R.; Kuper, H.; Breinbauer, C.; De Vries, P.J.; Gladstone, M.; et al. Developmental disabilities among children younger than 5 years in 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Glob. Health 2018, 6, e1100–e1121. [Google Scholar] [CrossRef] [Green Version]
- Dewey, D. What Is Comorbidity and Why Does It Matter in Neurodevelopmental Disorders? Curr. Dev. Disord. Rep. 2018, 5, 235–242. [Google Scholar] [CrossRef]
- Gillberg, C. The ESSENCE in child psychiatry: Early Symptomatic Syndromes Eliciting Neurodevelopmental Clinical Examinations. Res. Dev. Disabil. 2010, 31, 1543–1551. [Google Scholar] [CrossRef] [PubMed]
- Lahey, B.B.; Loeber, R.; Burke, J.; Rathouz, P.J.; McBurnett, K. Waxing and waning in concert: Dynamic comorbidity of conduct disorder with other disruptive and emotional problems over 7 years among clinic-referred boys. J. Abnorm. Psychol. 2002, 111, 556–567. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, B.J.; Dewey, D.M.; Crawford, S.G.; Wilson, B.N. The term comorbidity is of questionable value in reference to developmental disorders: Data and theory. J. Learn. Disabil. 2001, 34, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Chawarska, K.; Klin, A.; Paul, R.; Macari, S.; Volkmar, F. A prospective study of toddlers with ASD: Short-term diagnostic and cognitive outcomes. J. Child Psychol. Psychiatry Allied Discip. 2009, 50, 1235–1245. [Google Scholar] [CrossRef] [Green Version]
- Copeland, W.E.; Adair, C.E.; Smetanin, P.; Stiff, D.; Briante, C.; Colman, I.; Fergusson, D.; Horwood, L.; Poulton, R.; Costello, E.J.; et al. Diagnostic transitions from childhood to adolescence to early adulthood. J. Child Psychol. Psychiatry 2013, 54, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, P.; Carlström, E.; Råstam, M.; Gillberg, C.; Anckarsäter, H. The genetics of autism spectrum disorders and related neuropsychiatric disorders in childhood. Am. J. Psychiatry 2010, 167, 1357–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Loo, K.M.J.; Martens, G.J.M. Genetic and environmental factors in complex neurodevelopmental disorders. Curr. Genom. 2007, 8, 429–444. [Google Scholar]
- Anckarsäter, H.; Larson, T.; Hansson, S.L.; Carlström, E.; Ståhlberg, O.; Gillberg, C.; Råstam, M.; Gillberg, C.; Lichtenstein, P. Child neurodevelopmental and behavioural problems are intercorrelated and dimensionally distributed in the general population. Open Psychiatry J. 2008, 2, 5–11. [Google Scholar] [CrossRef]
- Eapen, V. Neurodevelopmental genes have not read the DSM criteria: Or, have they? Front. Psychiatry 2012, 3, 75. [Google Scholar] [CrossRef] [Green Version]
- Lundström, S.; Reichenberg, A.; Anckarsäter, H.; Lichtenstein, P.; Gillberg, C. Autism phenotype versus registered diagnosis in Swedish children: Prevalence trends over 10 years in general population samples. BMJ 2015, 350, h1961. [Google Scholar] [CrossRef] [Green Version]
- Whitehouse, A.J.; Cooper, M.N.; Bebbington, K.; Alvares, G.; Lin, A.; Wray, J.; Glasson, E.J. Evidence of a reduction over time in the behavioral severity of autistic disorder diagnoses. Autism Res. 2017, 10, 179–187. [Google Scholar] [CrossRef] [Green Version]
- Bishop, D.V.; Whitehouse, A.J.; Watt, H.J.; Line, E.A. Autism and diagnostic substitution: Evidence from a study of adults with a history of developmental language disorder. Dev. Med. Child. Neurol. 2008, 50, 341–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shattuck, P.T. The contribution of diagnostic substitution to the growing administrative prevalence of autism in US special education. Pediatrics 2006, 117, 1028–1037. [Google Scholar] [CrossRef] [PubMed]
- Påhlman, M.; Gillberg, C.; Himmelmann, K. One-third of school-aged children with cerebral palsy have neuropsychiatric impairments in a population-based study. Acta Paediatr. 2019, 108, 2048–2055. [Google Scholar] [CrossRef] [PubMed]
- Strnadová, I.; Dowse, L.; Watfern, C. Doing Research Inclusively: Guidelines for Co-Producing Research with People with Disability. Available online: https://apo.org.au/node/310904 (accessed on 11 February 2021).
- Safeer, R.S.; Keenan, J. Health literacy: The gap between physicians and patients. Am. Fam. Phys. 2005, 72, 463–468. [Google Scholar]
- Foster, S.L.; Mash, E.J. Assessing social validity in clinical treatment research: Issues and procedures. J. Consult Clin. Psychol. 1999, 67, 308–319. [Google Scholar] [CrossRef]
- Morgan, D.L. Successful Focus Groups: Advancing the State of the Art; Sage Publications: Thousand Oaks, CA, USA, 1993. [Google Scholar]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Alvares, G.A.; Dawson, P.A.; Dissanayake, C.; Eapen, V.; Gratten, J.; Grove, R.; Henders, A.; Heussler, H.; Lawson, L.; Masi, A.; et al. Study protocol for the Australian autism biobank: An international resource to advance autism discovery research. BMC Pediatrics 2018, 18, 284. [Google Scholar] [CrossRef]
- Masi, A.; Dissanayake, C.; Alach, T.; Cameron, K.; Fordyce, K.; Frost, G.; Grove, R.; Heussler, H.; Silove, N.; Sulek, R.; et al. Clinical outcomes and associated predictors of early intervention in autism spectrum disorder: A study protocol. BMJ Open 2021, 11, e047290. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.sydney.edu.au/brain-mind/our-clinics/child-behaviour-research-clinic.html (accessed on 11 February 2021).
- Johnson, S.; Barrett, P.M.; Dadds, M.R.; Fox, T.; Shortt, A. The diagnostic interview schedule for children, adolescents, and parents: Initial reliability and validity data. Behav. Chang. 1999, 16, 155–164. [Google Scholar] [CrossRef]
- Corbin, J.; Strauss, A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory; Sage Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Huberman, A.M.; Miles, M.B. Data management and analysis methods. In Handbook of Qualitative Research; Sage Publications Inc.: Thousand Oaks, CA, USA, 1994; pp. 428–444. [Google Scholar]
- QSR International Pty Ltd. NVivo (released in March 2020). Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 11 February 2021).
- Dadds, M.R.; Frick, P.J. Toward a transdiagnostic model of common and unique processes leading to the major disorders of childhood: The REAL model of attention, responsiveness and learning. Behav. Res. Ther. 2019, 119, 103410. [Google Scholar] [CrossRef] [PubMed]
- Eapen, V.; Crncec, R.; Walter, A.; Tay, K.P. Conceptualisation and Development of a Quality of Life Measure for Parents of Children with Autism Spectrum Disorder. Autism Res. Treat. 2014, 2014, 160783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saville, D.J. Multiple Comparison Procedures: The Practical Solution. Am. Statist. 1990, 44, 174–180. [Google Scholar]
- Lombardo, M.V.; Lai, M.-C.; Baron-Cohen, S. Big data approaches to decomposing heterogeneity across the autism spectrum. Mol. Psychiatry 2019, 24, 1435–1450. [Google Scholar] [CrossRef] [Green Version]
- Hadders-Algra, M.; Tacke, U.; Pietz, J.; Rupp, A.; Philippi, H. Reliability and predictive validity of the Standardized Infant NeuroDevelopmental Assessment neurological scale. Dev. Med. Child Neurol. 2019, 61, 654–660. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Stakeholder/Community Consultations | NAS Development | |
|---|---|---|
| Phase 1 | Initial consultation conducted separately with the following groups:
| Cluster analysis of existing databases containing diagnostic and functional assessments of NDDs analysed to ascertain clinical and theoretical subscales on the NAS. Items will have a readability level of grade 8 or lower [18]. |
| Phase 2 | Consultation with stakeholders from Phase 1 to review outcomes from dataset analyses (Phase 1b) to identify clinically meaningful items for NAS along with subscales. Parents/caregivers will be asked whether they feel each item should be included in the NAS and to provide their opinion about areas for improvement in the NAS. | Validation: recruitment and data collection in a pilot study of the NAS with a sample of parents/carers of children with NDDs who are preschool aged (ages 2–6), or are attending primary (ages 5–13), or secondary school (ages 13–18). |
| Phase 3 | Consultation with stakeholders from Phases 1 and 2 to assess face validity and user experience/friendliness (i.e., ‘social validity’). Social validity is defined as a measure of the overall acceptability of a measure, tool, or intervention beyond its effectiveness as perceived by the people who are implementing, receiving, and consenting to it [19]. | Data analysis: NAS validation. Evaluation and adaptation to finalise the NAS. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masi, A.; Azim, S.I.; Lam-Cassettari, C.; Dadds, M.; Mendoza Diaz, A.; Henry, G.; Karlov, L.; Lin, P.-I.; Mallitt, K.-A.; Montgomery, A.; et al. Co-Design of a Neurodevelopment Assessment Scale: A Study Protocol. Int. J. Environ. Res. Public Health 2021, 18, 12837. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312837
Masi A, Azim SI, Lam-Cassettari C, Dadds M, Mendoza Diaz A, Henry G, Karlov L, Lin P-I, Mallitt K-A, Montgomery A, et al. Co-Design of a Neurodevelopment Assessment Scale: A Study Protocol. International Journal of Environmental Research and Public Health. 2021; 18(23):12837. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312837
Chicago/Turabian StyleMasi, Anne, Syeda Ishra Azim, Christa Lam-Cassettari, Mark Dadds, Antonio Mendoza Diaz, Georgina Henry, Lisa Karlov, Ping-I Lin, Kylie-Ann Mallitt, Alicia Montgomery, and et al. 2021. "Co-Design of a Neurodevelopment Assessment Scale: A Study Protocol" International Journal of Environmental Research and Public Health 18, no. 23: 12837. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312837