
Spanish Questionnaires for the Assessment of Pelvic Floor Dysfunctions in Women: A Systematic Review of the Structural Characteristics and Psychometric Properties

 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Material and Method
2.1. Protocol
2.2. Sources and Search
2.3. Selection Criteria
2.4. Selection of Documents
2.5. Results Synthesis and Data Extraction
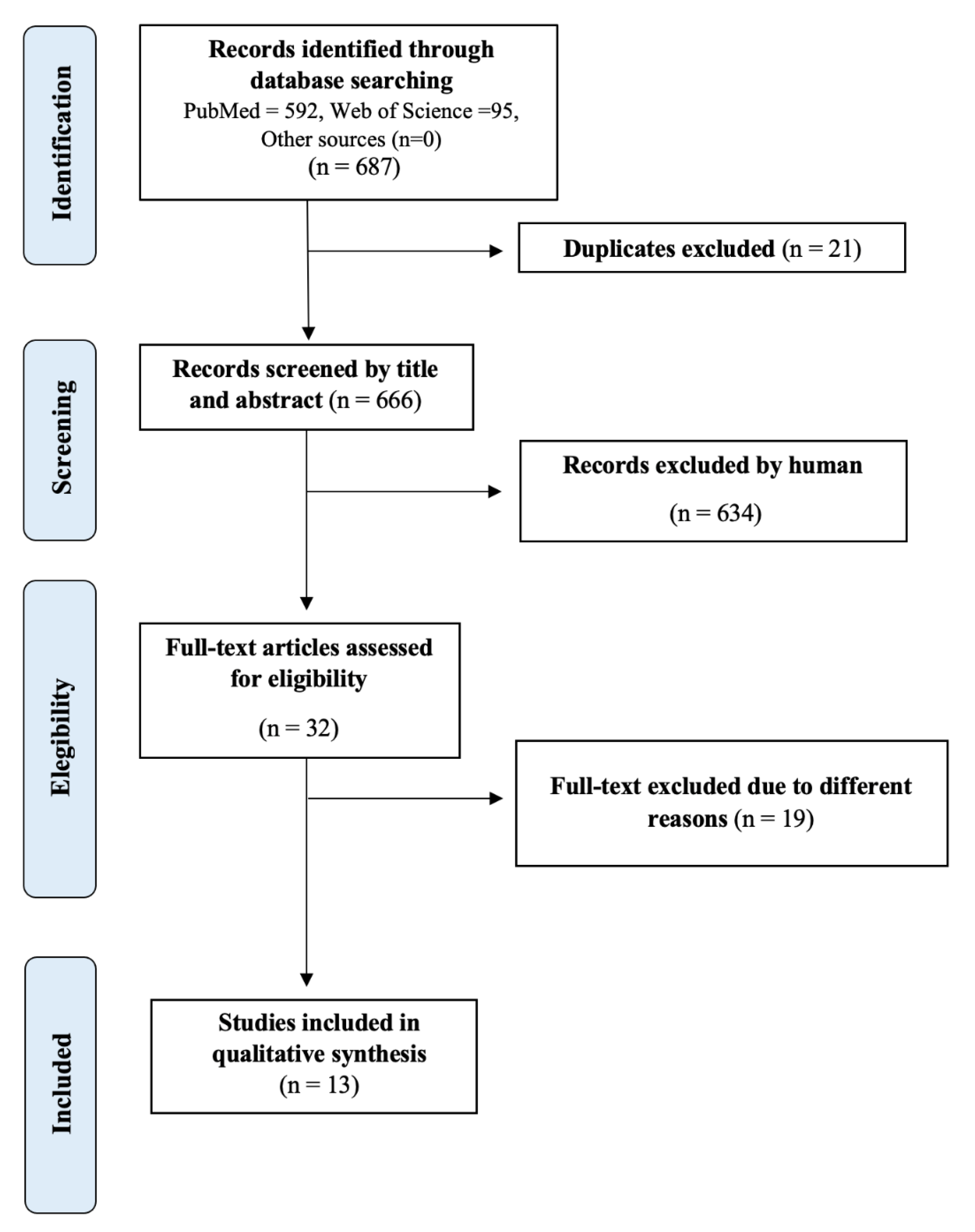
3. Results
4. Discussion
4.1. Selection and Use of Questionnaires in a Clinical and Research Setting
4.2. Psychometric Characteristics of the Questionnaires That Assess QoL
4.3. Psychometric Characteristics of the Questionnaires That Assess Sexual Function
4.4. Psychometric Characteristics of the Questionnaires That Evaluate POP
4.5. Psychometric Characteristics of the Questionnaires That Evaluate UI
4.6. Responsiveness
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grimes, W.; Stratton, M. Pelvic Floor Dysfunction; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Hoyte, L.; Damaser, M. Biomechanics of the Female Pelvic Floor; Elsevier: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Messelink, B.; Benson, T.; Berghmans, B.; Bø, K.; Corcos, J.; Fowler, C.; Laycock, J.; Lim, P.H.-C.; van Lunsen, R.; Nijeholt, G.L.Á.; et al. Standardization of terminology of pelvic floor muscle function and dysfunction: Report from the pelvic floor clinical assessment group of the International Continence Society. Neurourol. Urodyn. 2005, 24, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Petros, P.E.P.; Ulmsten, U.I. An integral theory of female urinary incontience: Experimental and clinical considerations. Acta Obstet. Gynecol. Scand. 1990, 69, 7–31. [Google Scholar] [CrossRef]
- Han, L.; Wang, L.; Wang, Q.; Li, H.; Zang, H. Association between pelvic organ prolapse and stress urinary incontinence with collagen. Exp. Ther. Med. 2014, 7, 1337–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, K.; Kumar, D. Pelvic floor dysfunction: A conceptual framework for collaborative patient-centred care. J. Adv. Nurs. 2003, 43, 555–568. [Google Scholar] [CrossRef] [PubMed]
- Weber, A.M.; Abrams, P.; Brubaker, L.; Cundiff, G.; Davis, G.; Dmochowski, R.R.; Fischer, J.; Hull, T.; Nygaard, I.; Weidner, A.C. The Standardization of Terminology for Researchers in Female Pelvic Floor Disorders. Int. Urogynecol. J. 2001, 12, 178–186. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Sánchez, B.; Torres-Lacomba, M.; Yuste-Sánchez, M.J.; Navarro-Brazález, B.; Pacheco-da-Costa, S.; Gutiérrez-Ortega, C.; Zapico-Goñi, Á. Cultural adaptation and validation of the Pelvic Floor Distress Inventory Short Form (PFDI-20) and Pelvic Floor Impact Questionnaire Short Form (PFIQ-7) Spanish versions. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 170, 281–285. [Google Scholar] [CrossRef]
- Engel, G.L. The Need for a New Medical Model: A Challenge for Biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Cruz, A.C.; Pedreira, M.D. Patient-and Family-Centered Care and Patient Safety: Reflections upon emerging proximity. Rev. Bras. Enferm. 2020, 73, e20190672. [Google Scholar] [CrossRef] [PubMed]
- Carrió, F.B. El modelo biopsicosocial en evolución. Med. Clín. 2002, 119, 175–179. [Google Scholar]
- Forget, N.; Higgins, J. Comparison of generic patient-reported outcome measures used with upper extremity musculoskeletal disorders: Linking process using the International Classification of Functioning, Disability, and Health (ICF). J. Rehabil. Med. 2014, 46, 327–334. [Google Scholar] [CrossRef] [Green Version]
- Barber, M.D. Questionnaires for women with pelvic floor disorders. Int. Urogynecol. J. 2007, 18, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Espuña Pons, M.; Fillol Crespo, M.; Pascual Amorós, M.A.; Rebollo Álvarez, P.; Prieto Soto, M. Spanish validation of the epidemiology of prolapse and incontinence questionnaire-EPIQ montserrat espuña pons. Actas Urol. Españolas 2009, 33, 646–653. [Google Scholar] [CrossRef]
- Sánchez-Sánchez, B.; Navarro-Brazález, B.; Arranz-Martín, B.; Sánchez-Méndez, Ó.; de la Rosa-Díaz, I.; Torres-Lacomba, M. The female sexual function index: Transculturally adaptation and psychometric validation in Spanish women. Int. J. Environ. Res. Public Health 2020, 17, 994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patient Safety and Quality Improvement Service. Guide to Informed in Health Care; Patient Safety and Quality Improvement Service: Brisbane, QLD, Australia, 2017. [Google Scholar]
- Guerra, J.; Bagur, C.; Girabent, M. Adaptación al castellano y validación del cuestionario sobre práctica basada en la evidencia en fisioterapeutas. Fisioterapia 2012, 34, 65–72. [Google Scholar] [CrossRef]
- Instituto Cervantes. Los Hablantes de Español Han Aumentado un 30% en la Última Década. 2020. Available online: https://www.cervantes.es (accessed on 15 October 2021).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Rev. Española Cardiol. 2021, 74, 790–799. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Boers, M.; van der Vleuten, C.P.M.; Bouter, L.M.; Alonso, J.; Patrick, D.L.; de Vet, H.C.W.; Terwee, C.B. COSMIN Risk of Bias tool to assess the quality of studies on reliability or measurement error of outcome measurement instruments: A Delphi study. BMC Med. Res. Methodol. 2020, 20, 293. [Google Scholar] [CrossRef] [PubMed]
- Kyte, D.; Calvert, M.; van der Wees, P.; Hove, R.T.; Tolan, S.; Hill, J. An introduction to patient-reported outcome measures (PROMs) in physiotherapy. Physiotherapy 2015, 101, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espuña Pons, M.; Rebollo Álvarez, P.; Puig Clota, M. Validación de la versión española del International Consultation on Incontinence Questionnaire-Short Form. Un cuestionario para evaluar la incontinencia urinaria. Med. Clín. 2004, 122, 288–292. [Google Scholar] [CrossRef]
- Espuña Pons, M.; Puig Clota, M.; Rebollo Álvarez, P. Validación de la versión en español del “Cuestionario de Autoevaluación del Control de la Vejiga (CACV). Un nuevo instrumento para detectar pacientes con disfunción del tracto urinario inferior. Actas Urol. Españolas 2006, 30, 1017–1024. [Google Scholar] [CrossRef] [Green Version]
- Pons, M.E.; Clota, M.P.; Aguilón, M.G.; Zardain, P.C.; Álvarez, P.R. Cuestionario para evaluación de la función sexual en mujeres con prolapso genital y/o incontinencia. Validación de la versión española del ‘Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12). Actas Urol. Españolas 2008, 32, 211–219. [Google Scholar] [CrossRef] [Green Version]
- Viñaspre Hernández, R.R.; Tomás Aznar, C.; Rubio Aranda, E. Validación de la versión española de las formas cortas del Urogenital Distress Inventory (UDI-6) y del Incontinence Impact Questionnaire (IIQ-7) en mujeres embarazadas. Gac. Sanit. 2011, 25, 379–384. [Google Scholar] [CrossRef] [Green Version]
- Sánchez, E.M.M.; Serrano, C.M.S.; Almeida, M.D.L.C.; Mohedo, E.D.; Martínez, R.C. Spanish Version of the Broome Pelvic Muscle Self-Efficacy Scale: Validity and Reliability. Phys. Ther. 2013, 93, 1696–1706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mestre, M.; Lleberia, J.; Pubill, J.; Espuña-Pons, M. Spanish version of the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire IUGA-Revised (PISQ-IR): Transcultural validation. Int. Urogynecol. J. 2017, 20, 1865–1873. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Herrezuelo, I.; Hita-Contreras, F.; Martínez-Amat, A.; Aibar-Almazán, A.; Díaz, D.C.; Wangensteen, R.; Ochoa, A.A.; Díaz-Mohedo, E. The female sexual function index: Reliability and validity in Spanish postmenopausal women. Menopause 2019, 26, 401–408. [Google Scholar] [CrossRef]
- Sánchez-Sánchez, B.; Yuste-Sánchez, M.J.; Arranz-Martín, B.; Navarro-Brazález, B.; Romay-Barrero, H.; Torres-Lacomba, M. Quality of life in POP: Validity, Reliability and Responsiveness of the Prolapse Quality of Life Questionnaire (P-QoL) in Spanish Women. Int. J. Environ. Res. Public Health 2020, 17, 1690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Sánchez, B.; Arranz-Martín, B.; Navarro-Brazález, B.; Vergara-Pérez, F.; Bailón-Cerezo, J.; Torres-Lacomba, M. How Do We Assess Patient Skills in a Competence-Based Program? Assessment of Patient Competences Using the Spanish Version of the Prolapse and Incontinence Knowledge Questionnaire and Real Practical Cases in Women with Pelvic Floor Disorders. Int. J. Environ. Res. Public Health 2021, 18, 2377. [Google Scholar] [CrossRef] [PubMed]
- Ruiz de Viñaspre-Hernández, R.; Garrido-Santamaria, R.; Urra-Martínez, R.; Sáenz-Cabredo, P.; Martínez-Tofe, J.; Burgos-Esteban, A.; Gea-Caballero, V.; Antón-Solanas, I.; Santolalla-Arnedo, I.; Juárez-Vela, R. Transcultural adaptation and validation of the spanish version of the sexual satisfaction scale for women (SSS-W-E). Int. J. Environ. Res. Public Health 2021, 18, 9663. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Sánchez, B.; Torres-Lacomba, M.; Brazález, B.N.; Téllez, E.C.; Da Costa, S.P.; Ortega, C.G. Responsiveness of the Spanish Pelvic Floor Distress Inventory and Pelvic Floor Impact Questionnaires Short Forms (PFDI-20 and PFIQ-7) in women with pelvic floor disorders. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 190, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Teleman, P.; Stenzelius, K.; Iorizzo, L.; Jakobsson, U. Validation of the Swedish short forms of the Pelvic Floor Impact Questionnaire (PFIQ-7), Pelvic Floor Distress Inventory (PFDI-20) and Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12). Acta Obstet. Gynecol. Scand. 2011, 90, 483–487. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Xu, T.; Zhang, Y.; Mao, M.; Kang, J.; Zhu, L. Validation of the Chinese version of the Pelvic Floor Distress Inventory-20 (PFDI-20) according to the COSMIN checklist. Int. Urogynecol. J. 2019, 30, 1127–1139. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, P.B.; Sut, N.; Sut, H.K. Validation, cultural adaptation and responsiveness of two pelvic-floor-specific quality-of-life questionnaires, PFDI-20 and PFIQ-7, in a Turkish population. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 162, 229–233. [Google Scholar] [CrossRef]
- Henn, E.W.; Richter, B.W.; Marokane, M.M.P. Validation of the PFDI-20 and PFIQ-7 quality of life questionnaires in two African languages. Int. Urogynecol. J. 2017, 28, 1883–1890. [Google Scholar] [CrossRef]
- Barber, M.; Walters, M.; Bump, R. Short forms of two condition-specific quality-of-life questionnaires for women with pelvic floor disorders (PFDI-20 and PFIQ-7). Am. J. Obstet. Gynecol. 2005, 193, 103–113. [Google Scholar] [CrossRef]
- Takahashi, M.; Inokuchi, T.; Watanabe, C.; Saito, T.; Kai, I. The Female Sexual Function Index (FSFI): Development of a Japanese Version. J. Sex. Med. 2011, 8, 2246–2254. [Google Scholar] [CrossRef]
- Rosen, C.; Brown, J.; Heiman, S.; Leiblum, C.; Meston, R.; Shabsigh, D.; Ferguson, R.; D’Agostino, R. The female sexual function index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J. Sex. Marital Ther. 2000, 26, 191–205. [Google Scholar] [CrossRef]
- Babakhanian, M.; Ghazanfarpour, M.; Najafi, M.N.; Dizavandi, F.R.; Khadivzadeh, T.; Safaei, M.; Nooghabi, M.J. Psychometric properties of Persian language version of the Female Sexual Function Index (P-FSFI) among postmenopausal women. J. Turk. Ger. Gynecol. Assoc. 2018, 19, 187–192. [Google Scholar] [CrossRef]
- Filocamo, M.T.; Serati, M.; Marzi, V.L.; Costantini, E.; Milanesi, M.; Pietropaolo, A.; Polledro, P.; Gentile, B.; Maruccia, S.; Fornia, S.; et al. The Female Sexual Function Index (FSFI): Linguistic Validation of the Italian Version. J. Sex. Med. 2014, 11, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Digesu, G.A.; Khullar, V.; Cardozo, L.; Robinson, D.; Salvatore, S. P-QOL: A validated questionnaire to assess the symptoms and quality of life of women with urogenital prolapse. Int. Urogynecol. J. 2004, 16, 176–181. [Google Scholar] [CrossRef]
- Brandt, C.; Van Rooyen, C.; Cronje, H. Validation of the prolapse quality of life questionnaire (P-QOL): An Afrikaans version in a South African population. South Afr. J. Obstet. Gynaecol. 2016, 22, 38. [Google Scholar] [CrossRef] [Green Version]
- Veit-Rubin, N.; Digesu, A.; Swift, S.; Khullar, V.; Gambirasio, I.K.; Dällenbach, P.; Boulvain, M. Validation of the French version of the P-QoL questionnaire. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 192, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Cam, C.; Sakalli, M.; Ay, P.; Aran, T.; Cam, M.; Karateke, A. Validation of the prolapse quality of life questionnaire (P-QOL) in a Turkish population. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 135, 132–135. [Google Scholar] [CrossRef]
- De Oliveira, M.S.; Tamanini, J.T.N.; de Aguiar Cavalcanti, G. Validation of the prolapse quality-of-life questionnaire (P-QoL) in Portuguese version in Brazilian women. Int. Urogynecol. J. 2009, 20, 1191–1202. [Google Scholar] [CrossRef] [PubMed]
- Claerhout, F.; Moons, P.; Ghesquiere, S.; Verguts, J.; De Ridder, D.; Deprest, J. Validity, reliability and responsiveness of a Dutch version of the prolapse quality-of-life (P-QoL) questionnaire. Int. Urogynecol. J. 2010, 21, 569–578. [Google Scholar] [CrossRef]
- Manchana, T.; Bunyavejchevin, S. Validation of the Prolapse Quality of Life (P-QOL) questionnaire in Thai version. Int. Urogynecol. J. 2010, 21, 985–993. [Google Scholar] [CrossRef] [PubMed]
- Svihrova, V.; Digesu, G.A.; Svihra, J.; Hudeckova, H.; Kliment, J.; Swift, S. Validation of the Slovakian version of the P-QOL questionnaire. Int. Urogynecol. J. 2009, 21, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Scarlato, A.; Souza, C.C.C.; Fonseca, E.S.M.; Sartori, M.G.F.; Girão, M.J.B.D.C.; Castro, R.A. Validation, reliability, and responsiveness of Prolapse Quality of Life Questionnaire (P-QOL) in a Brazilian population. Int. Urogynecol. J. 2011, 22, 751–755. [Google Scholar] [CrossRef] [PubMed]
- Chuang, F.-C.; Chu, L.-C.; Kung, F.-T.; Huang, K.-H. Validation of the traditional Chinese version of the prolapse quality of life questionnaire (P-QOL) in a Mandarin-speaking Taiwanese population. Taiwan. J. Obstet. Gynecol. 2016, 55, 680–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukacz, E.S.; Lawrence, J.; Buckwalter, J.G.; Burchette, R.J.; Nager, C.W.; Luber, K.M. Epidemiology of prolapse and incontinence questionnaire: Validation of a new epidemiologic survey. Int. Urogynecol. J. 2005, 16, 272–284. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.D.; Massagli, M.P.; Kohli, N.; Rajan, S.S.; Braaten, K.P.; Hoyte, L. A reliable, valid instrument to assess patient knowledge about urinary incontinence and pelvic organ prolapse. Int. Urogynecol. J. 2008, 19, 1283–1289. [Google Scholar] [CrossRef]
- Celenay, S.T.; Akbayrak, T.; Kaya, S.; Ekici, G.; Beksac, S.; Beksac, M. Validity and reliability of the Turkish version of the Pelvic Floor Distress Inventory-20. Int. Urogynecol. J. 2012, 23, 1123–1127. [Google Scholar] [CrossRef]
- Rzepka, J.; Zalewski, K.; Stefanowicz, A.; Khullar, V.; Swift, S.; Digesu, G.A. Validation of the Polish version of P-QoL questionnaire. Ginekol. Pol. 2016, 87, 477–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flores-Espinoza, C.; Araya, A.X.; Pizarro-Berdichevsky, J.; Santos, V.; Ferrer, M.; Garin, O.; Swift, S.; Digesu, A.G. Validation of the Spanish-language version of the Prolapse Quality of Life Questionnaire in Chilean women. Int. Urogynecol. J. 2014, 26, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Nunes-Tamanini, J.T.; Dambros, M.; D’Ancona, C.A.; Paulo César, R.P.; Netto, R., Jr. Validation of the International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF) for Portuguese. Rev. Bras. Ginecol. E Obs. 2010, 32, 273–278. [Google Scholar]
- Broome, B. Psychometric analysis of the Broome Pelvic Muscle Self-Efficacy Scale in African-American women with incontinence. Urol. Nurs. 2001, 21, 289–297. [Google Scholar]


{kind=link}
| Questionnaire | Acronym | Nº Items | Population | Purpose | Dimensions | Subscale | Punctuation |
|---|---|---|---|---|---|---|---|
| International Consultation on Incontinence Questionnaire-Short Form [23] | ICIQ-SF | 3 + 8 | 500 women 59.4 ± 13.2 years (Mean ± SD) | Detect UI in any healthcare setting | - | - | Sum of the first 3 items (from 0 to 21 points) |
| Bladder control Self-Assessment Questionnaire [24] | B-SAQ | 8 | 133 women 57.5 ± 15.5 years (Mean ± SD) | Identify overactive bladder problems | - | 2: Discomfort and symptoms | Likert scale: from 0 to 3. The scores of each subscale are added separately |
| Pelvic Organ Prolapse/ Urinary Incontinence SexualQuestionnaire [25] | PISQ-12 | 12 | 49 women 47.9 ± 9.8 years (Mean ± SD) | Assess sexual function in women with prolapse genital and/or urinary incontinence. | - | - | Sum of the scores for each item, (from 0 = always to 4 = never), reversing this score for items 1, 2, 3, and 4. |
| Epidemiology of Prolapse and Incontinence Questionnaire [14] | EPIQ | 53 (22 scoring) | 120 women | Evaluates the symptoms of POP and UI, and the QoL in women who suffer from them | 7: Overactive bladder, SUI, QoL, POP, FI, pain and difficulty in emptying and defecatory dysfunction | - | Each item from 0 to 10 |
| Urogenital Distress Inventory [26] | UDI-6 | 6 | 181 pregnant women 33 years (Median) | Measure the parameters presence, severity, symptoms associated urogenital and type of urinary incontinence. | - | 3: Irritative symptoms, stress symptoms and symptoms of obstruction/pain related to urination | Likert scale: From 0 to 4 |
| Incontinence Impact Questionnaire [26] | IIQ-7 | 7 | 181 pregnant women 33 years (Median) | Measure the QoL in women with urinary incontinence | Seven components: ability to do household chores, physical activity, recreational activity, ability to travel, social activities, emotional state, and frustration | - | Likert scale: From 0 to 3 |
| Pelvic Floor Distress Inventory Short Form [8] | PFDI-20 | 20 | 114 women 56 ± 11 years (Mean ± SD) | Measures QoL with health or perceived health in people with PFD and symptom scale | 3: POPDI, CRADI, UDI | - | POPDI: 0–100 CRADI: 0–100 UDI: 0–100 Maximum score 300. |
| Pelvic Floor Impact Questionnaire Short Form [8] | PFIQ-7 | 21, 7 items for each dimension | 114 women 56 ± 11 years (Mean ± SD) | Measures the impact of PFD | 3: UIQ, CRAIQ, POPIQ | - | UIQ: 0–100 CRAIQ:0–100 POPIQ:0–100 Maximun score 300. |
| Broome Pelvic Muscle Self- Efficacy Scale [27] | - | 23 | 119 women 53.5 ± 19.8 years (Mean ± SD) | Measures the expectations of self-efficacy and results perceived by women with UI who perform pelvic floor exercises | 2: Expectation of self-efficacy, expectation of result | - | Each item 0–100 |
| Pelvic Organ Prolapse/ Urinary Incontinence Sexual Questionnaire [28] | PISQ-IR | 20 | 268 women: 118 NSA 64.9 ± 10.8 years 150 SA 54.7 ± 10 years (Mean ± SD) | Assess female sexual function in women with pelvic floor disorders (sexually active and inactive women) | - | 2: NSA, SA | NR |
| Female Sexual Function Index [29] | FSFI | 19 | 152 postmenopausal women 63.91 ± 6.99 years (Mean ± SD) | Assess the key dimensions of sexual function in women | - | 6: Sexual desire, arousal, lubrication, orgasm, satisfaction and pain. | The subscales range from 0 (or 1) to 5 (higher scores indicate better sexual function). |
| Female Sexual Function Index [15] | FSFI | 19 | 323 women: 167 FSD group 48 ± 8 years 156 control group 40 ± 11 years (Mean ± SD) | Evaluates sexual health in the female population | - | 6: Sexual desire, arousal, lubrication, orgasm, satisfaction and pain. | The subscales range from 0 (or 1) to 5 (higher scores indicate better sexual function). |
| Prolapse Quality of Life Questionnaire [30] | P-QoL | 20 | 200 women: 100 symptomatic 52 ± 13.4 years 100 asymptomatic 40 ± 11.1 years | Evaluates the impact of POP on the QoL of women | - | 9: General health, POP impact, role limitation, physical limitation, social limitation, personal relationships, emotions, sleep/energy, severity measures | Each subscale from 0 to 100 |
| Prolapse and Incontinence Knowledge Questionnaire [31] | PIKQ | 24 | 147 women 38.57 ± 8.21 years (Mean ± SD) | Assess women’s knowledge of UI and POP | 2: UI and POP sections | Score range: 0 to 1. In each scale, the minimum score is 0 and the maximum is 12. | |
| Sexual Satisfaction Scale for Women (SSS-W-E) [32] | SSS-W-E | 30 | 316 women | Measure sexual satisfaction of women | 5: Satisfaction, communication, compatibility, concern for the relationship and personal concerns. | Likert scale: From 1 = strongly disagree to 5 = strongly agree. |
| Study | Questionnaire | Test–Retest Reliability | Internal Consistency | Content Validity | KMO | Construct Validity | SRM |
|---|---|---|---|---|---|---|---|
| Espuña-Pons et al., 2004 [23] | ICIQ-SF | - | Cronbach’s α = 0.89 | - | - | NR | |
| Espuña-Pons et al., 2006 [24] | B-SAQ | - | Cronbach’s α symptoms = 0.722 Cronbach’s α discomfort = 0.889 | - | ICIQ-UI SF: 0.65 | NR | |
| Espuña-Pons et al., 2008 [25] | PISQ-12 | ICC: 0.22–0.76 | Cronbach’s α = 0.829 | Three Factors | - | FSM: r = 0.71 FMS_DR = 0.504 ICIQ-UI-SF: r = −0.038 CACVSimptoms: r = −0.30 CACVannoyance: r = −0.40 | NR |
| Espuña-Pons et al., 2009 [14] | EPIQ | ICC = 0.49–0.91 | Cronbach’s α Total: 0.94 QoL: 0.96 Overactive bladder: 0.91 Anal incontinence: 0.63 Pain and Difficulty emptying: 0.72 Defecatory dysfunction: 0.75 Stress Urinary Incontinence: 0.61 Pelvic prolapse = Not Calculated | Seven Factors: QoL Overactive bladder Anal incontinence Pain and Difficulty emptying Defecatory dysfunction Stress Urinary Incontinence Pelvic prolapse | - | - | NR |
| Ruiz de Viñaspre et al., 2011 [26] | UDI-6 | ICC = 0.812–0.902 | Cronbach’s α = 0.667 | - | ICIQ: r = 0.497 | NR | |
| IIQ-7 | ICC = 0.954 | Cronbach’s α = 0.910 | ICIQ: r = 0.472 | NR | |||
| Sánchez-Sánchez et al., 2013 [8] ; Sánchez-Sánchez, B. et al., 2015 [33] | PFDI-20 | ICC= TOTAL= 0.644 POPDI = 0.711 CRADI = 0.771 UDI = 0.428 | Cronbach’s α TOTAL= 0.837 POPDI = 0.787 CRADI = 0.630 UDI = 0.699 | - | PFIQ-7: r = 0.220–0.468 PFIQ-7(UIQ): r = 0.181–0.489 PFIQ-7(CRAIQ): r = 0.212–0.397 PFIQ-7(POPIQ): r = 0.222–0.453 SF-12 (PCS) r = 0.215–0.415 SF-12 (MCS) r = 0.010–0.188 ICIQ-SF: r = 0.207–0.589 EPIQ (US) r = 0.346–0.625 EPIC (POP) r = 0.264–0.641 EPIC (QoL) r = 0.249–0.594 EPIC (CRS) r = 0.112–0.449 | Total: 084 POPDI: 0.78 CRADI: 0.50 UDI: 0.67 | |
| PFIQ-7 | ICC = 0.786 | Cronbach’s α ≥ 0.967 | - | PFDI-20 r = 0.220–0.468 PFDI-20 (POPDI): r = 0.212–0.453 PFDI-20 (CRADI): r = 0.181–0.397 PFDI-20 (UDI): r = 0.343–0.489 SF-12 (PCS) r = 0.293–0.480 SF-12 (MCS) r = 0.173–0.352 ICIQ-SF: r = 0.427–0.567 EPIQ (US) r = 0.427–0.567 EPIC (POP) r = 0.219–0.451 EPIC (QoL) r = 0.456–0.694 EPIC (CRS) r = 0.005–0.314 | Total: 0.57 UIQ: 0.61 CRAIQ: 0.39 POPIQ: 0.47 | ||
| Medrano-Sánchezet al., 2013 [27] | Broome Pelvic Muscle Self- Efficacy Scale (BPMSES) | NO | Cronbach’s α BPMSES = 0.91 Expectations of self-efficacy) = 0.84 Expectations of results = 0.94 | Six Factors | 0.721 | - | NR |
| Mestre et al., 2017 [28] | PISQ-IR | NO | Cronbach’s α NSA = 0.79 SA = 0.91 Subscales = 0.54–0.91 | 4 factors NSA condition-specific NSA partner-related NSA global quality NSA condition impact | - | POPQ: r = 0.012–0.145 Pelvic Floor Tone: r = 0.084–0.11 Oxford Scale: r = 0.01–0.141 ISI: r = 0.158–0.346 PFDI-20: r = 0.167–0.363 EPIC: r = 0.014–0.241 FSFIdesire: r = 0.528–0.871 FSFIarousal: r = 0.363–0.742 FSFIlubrication: r = 0.552 FSFIorgasm: r = 0.694 FSFIsatisfaction: r = 0.334–0.785 FSFIpain: r = 0.028–0.416 FSFItotal: r = 0.271–0.809 | NR |
| Pérez-Herrezuelo et al., 2019 [29] | FSFIpostmenopausal | ICC Total: 0.901 Dimension 1: 0.791–0.936 Dimension 2: 0.839–0.930 Dimension 3: 0.817–0.844 | Cronbach’s α Total: 0.964 Dimension 1: 0.961 Dimension 2: 0.911 Dimension 3: 0.679 | Three factors | 0.921 | VAS: r = 0.556–0.868 HADSanxiety: r = 0.007–0.060 HADSdepression: r = 0.004–0.061 | NR |
| Sánchez-Sánchez et al., 2020 [15] | FSFI | ICC FSFI total = 0.96 FSFI desire = 0.943 FSFI arousal = 0.907 FSFI lubrication = 0.939 FSFI orgasm = 0.916 FSFI satisfaction = 0.931 FSFI pain = 0.930 | Cronbach’s α FSFI total= 0.850 FSFI desire = 0.760 FSFI arousal = 0.745 FSFI lubrication= 0.756 FSFI orgasm = 0.753 FSFI satisfaction = 0.753 FSFI pain = 0.765 | Six Factors | 0.861 | - | Desire: 0.58 Arousal: 0.82 Lubrication: 0.85 Orgasm: 0.84 Satisfaction: 0.82 Pain: 1.01 Total FSFI: 1.11 In all cases p < 0.001 |
| Sánchez-Sánchez et al., 2020 [30] | P-QoL | ICC General Health Perceptions: 0.791 Prolapse Impact: 0.862 Role Limitations: 0.863 Physical Limitations: 0.908 Social Limitations: 0.864 Personal Limitations: 0.725 Emotions: 0.849 Sleep/Energy: 0.938 Severity Measures: 0.857 | Cronbach’s α Role Limitations: 0.848 Physical Limitations: 0.768 Social Limitations: 0.751 Personal Limitations: 0.806 Emotions: 0.877 Sleep/Energy: 0.621 Severity Measures: 0.550 | - | PFIQ-7 UIQ: r = 0.316–0.505 CRAIQ: r = 0.204–0.411 POPIQ: r = 0.305–0.555 PFDI-20 Total: r = 0.265–0.468 POPDI: r = 0.266–0.444 CRADI: r = 0.131–0.396 UDI: r = 0.235–0.513 | General health: 0.29 POP impact: 0.73 * Role limitation: 0.50 Physical limitation: 0.62 * Social limitation: 0.61 * Personal relationships: 0.57 * Emotions: 0.63 * Sleep/energy: 0.65 * Severity measures: 0.73 * (* p < 0.001) | |
| Sánchez-Sánchez et al., 2021 [31] | PIKQ | ICC: PIKQ-IU: 0.995 PIKQ-POP: 0.977 | Cronbach’s α PIKQ-IU: 0.745 PIKQ-POP: 0.758 | - | - | PIKQ-IU: 1.16 (1.01–1.32) PIKQ-POP: 1.15 (0.99–1.33) (95%CI) | |
| Ruiz de Viñaspre-Hernández et al., 2021 [32] | SSS-W-E | - | Cronbach’s α Total = 0.93 Contentment = 0.86 Communication = 0.70 Compatibility = 0.81 Relational Concern = 0.90 Personal Concern = 0.93 | Five Factors | Total: 0.92 Dimensions: 0.76 – 0.88 | - | NR |
| Study | Conclusions |
|---|---|
| Espuña-Pons et al., 2004 [23] | High sensitivity values and positive predictive values are indicators of the quality of the questionnaire as an instrument diagnosis of UI. |
| Espuña-Pons et al., 2006 [24] | This questionnaire will be very useful both in clinical practice and in research, allowing epidemiological studies of the prevalence of disease evaluated from the point of view of the patient to be carried out. |
| Espuña-Pons et al., 2008 [25] | The Spanish version of the PISQ-12 complies with the psychometric properties of feasibility, validity and reliability, to be used in our country, both in clinical practice and in research. |
| Espuña-Pons et al., 2009 [14] | The Spanish version of the EPIQ is feasible, valid and reliable to be used in clinical practice as a screening instrument for pelvic floor pathology. |
| Ruiz de Viñaspre et al., 2011 [26] | The results of the study show that both questionnaires constitute a reliable, consistent and valid instrument to evaluate urogenital symptoms and their impact on the QoL of pregnant women. |
| Sánchez-Sánchez et al., 2013 [8] ; Sánchez-Sánchez, B., 2015 [33] | The Spanish versions of the PFDI-20 and PFIQ-7 are equivalent in content, semantics, conceptually and idiomatically with the original versions, in addition to being reliable, valid and feasible and responsive to evaluate the symptoms and QoL in Spanish women with PFD. |
| Medrano-Sánchez et al., 2013 [27] | The Spanish version of the Broome questionnaire for self-efficacy is a useful measurement tool for a relevant psychometric and clinical estimation of women in performing pelvic floor exercises. |
| Mestre et al., 2017 [28] | The Spanish version of the PISQ-IR meets the criteria of feasibility, validity and reliability for use in clinical practice. |
| Pérez-Herrezuelo et al., 2019 [29] | The Spanish version of the FSFI shows good internal consistency and test–retest reliability, and also good construct, concurrent, and divergent validity for a population of postmenopausal women, shows satisfactory general psychometric properties and is able to discriminate between women with and without sexual dysfunctions among a population of Spanish postmenopausal women. |
| Sánchez-Sánchez et al., 2020 [15] | The Spanish version of the FSFI can be used as a reliable, valid, responsive and feasible instrument to assess sexual function in women. |
| Sánchez-Sánchez et al., 2020 [30] | The Spanish version of the P-QoL has sufficient validity, reliability, responsiveness, and feasibility for assessing the severity of symptoms and their impact on the QoL of Spanish women with POP. |
| Sánchez-Sánchez et al., 2021 [31] | The Spanish PIKQ is a comprehensible, valid, reliable, feasible, and responsive-to-change tool for assessing patient knowledge about UI and POP conditions in the Spanish language, as well as the effect of educational treatment strategies on them, both in research and clinical interventions. |
| Ruiz de Viñaspre-Hernández et al., 2021 [32] | The Spanish version has good overall reliability and validity. The findings are largely compatible with the initial hypothesis, which make the SSS-W-E a useful tool for the evaluation of women’s sexual satisfaction in clinical practice and research, in Spain. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guallar-Bouloc, M.; Gómez-Bueno, P.; Gonzalez-Sanchez, M.; Molina-Torres, G.; Lomas-Vega, R.; Galán-Mercant, A. Spanish Questionnaires for the Assessment of Pelvic Floor Dysfunctions in Women: A Systematic Review of the Structural Characteristics and Psychometric Properties. Int. J. Environ. Res. Public Health 2021, 18, 12858. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312858
Guallar-Bouloc M, Gómez-Bueno P, Gonzalez-Sanchez M, Molina-Torres G, Lomas-Vega R, Galán-Mercant A. Spanish Questionnaires for the Assessment of Pelvic Floor Dysfunctions in Women: A Systematic Review of the Structural Characteristics and Psychometric Properties. International Journal of Environmental Research and Public Health. 2021; 18(23):12858. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312858
Chicago/Turabian StyleGuallar-Bouloc, Marina, Paloma Gómez-Bueno, Manuel Gonzalez-Sanchez, Guadalupe Molina-Torres, Rafael Lomas-Vega, and Alejandro Galán-Mercant. 2021. "Spanish Questionnaires for the Assessment of Pelvic Floor Dysfunctions in Women: A Systematic Review of the Structural Characteristics and Psychometric Properties" International Journal of Environmental Research and Public Health 18, no. 23: 12858. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312858