
Spiritual Needs Assessment in Post-Secular Contexts: An Integrative Review of Questionnaires



Abstract
:1. Introduction
Spiritual Care from a Post-Secular Perspective
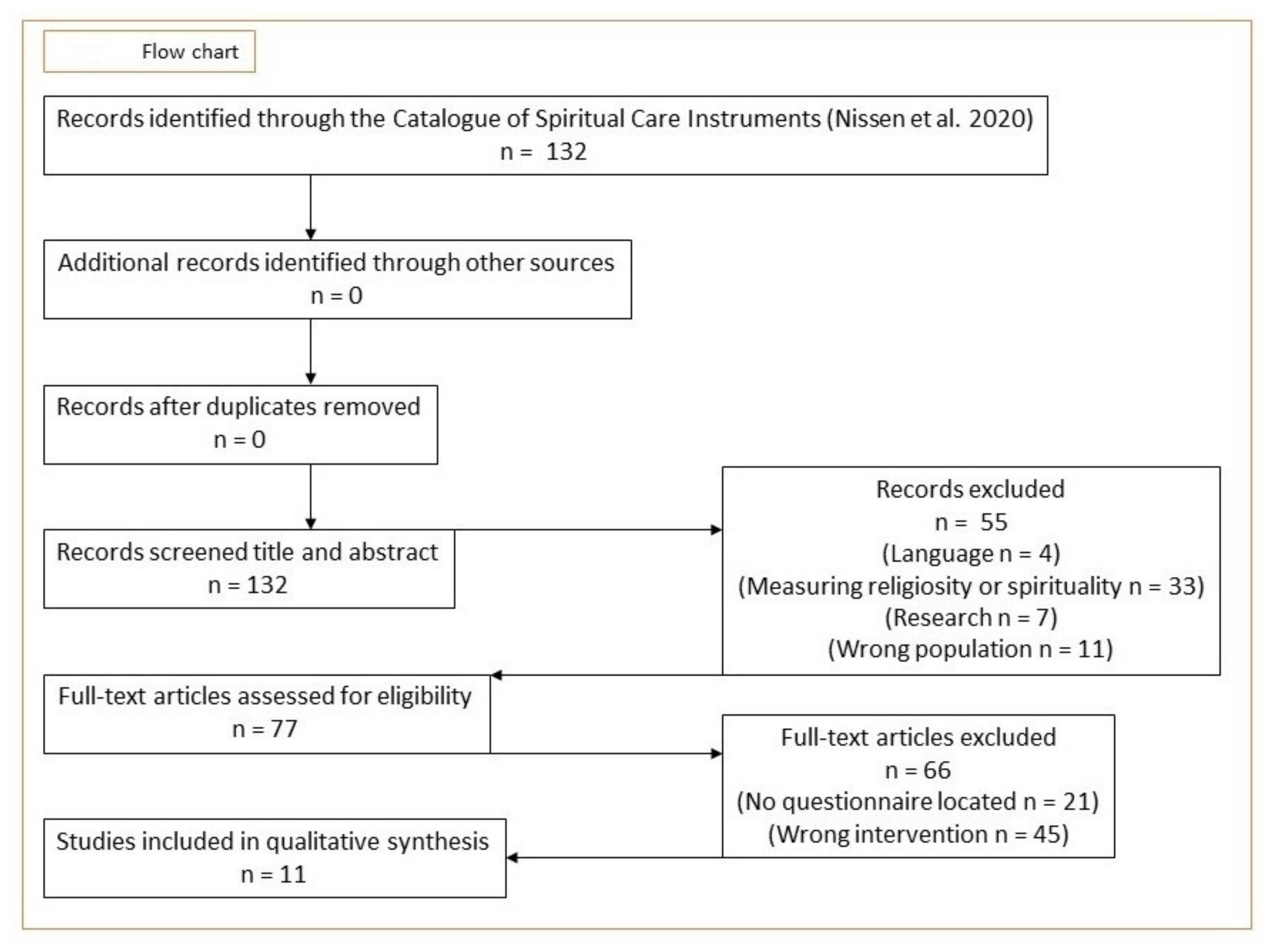
2. Method
3. Results
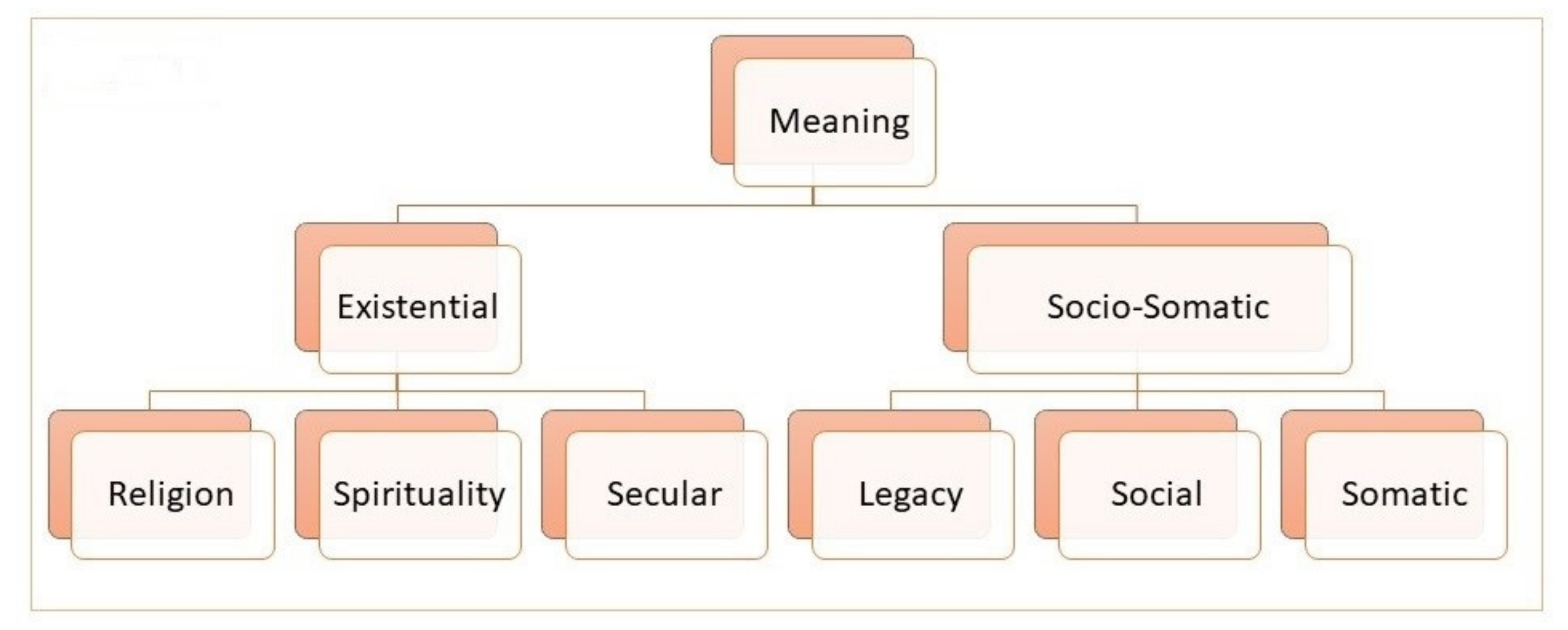
4. Inductive, Taxonomic Analysis, and Measurement Properties
5. Discussion: Evaluation of Applicability in a Post-Secular Context
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tan, H.; Rumbold, B.; Gardner, F.; Snowden, A.; Glenister, D.; Forest, A.; Bossie, C.; Wyles, L. Understanding the outcomes of spiritual care as experienced by patients. J. Health Care Chaplain. 2020, 10, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Lin, Y.; Yan, J.; Wu, Y.; Hu, R. The effects of spiritual care on quality of life and spiritual well-being among patients with terminal illness: A systematic review. Palliat. Med. 2018, 32, 1167–1179. [Google Scholar] [CrossRef] [PubMed]
- Vallurupalli, M.; Lauderdale, K.; Balboni, M.J.; Phelps, A.C.; Block, S.D.; Ng, A.K.; Kachnic, L.A.; VanderWeele, T.J.; Balboni, T.A. The Role of Spirituality and Religious Coping in the Quality of Life of Patients with Advanced Cancer Receiving Palliative Radiation Therapy. J. Support. Oncol. 2012, 10, 81–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balboni, T.A.; Paulk, M.E.; Balboni, M.J.; Phelps, A.C.; Loggers, E.T.; Wright, A.A.; Block, S.D.; Lewis, E.F.; Peteet, J.R.; Prigerson, H.G. Provision of Spiritual Care to Patients with Advanced Cancer: Associations with Medical Care and Quality of Life Near Death. J. Clin. Oncol. 2010, 28, 445–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Büssing, A. (Ed.) Spiritual Needs in Research and Practice; Palgrave Macmillan: Cham, Switzerland, 2021. [Google Scholar] [CrossRef]
- Andersen, A.H.; Hvidt, E.A.; Hvidt, N.C.; Roessler, K.K. ‘Maybe we are losing sight of the human dimension’–physicians’ approaches to existential, spiritual, and religious needs among patients with chronic pain or multiple sclerosis. A qualitative interview-study. Health Psychol. Behav. Med. 2020, 8, 248–269. [Google Scholar] [CrossRef]
- Best, M.; Butow, P.; Olver, I. Why do We Find It so Hard to Discuss Spirituality? A Qualitative Exploration of Attitudinal Barriers. J. Clin. Med. 2016, 5, 77. [Google Scholar] [CrossRef]
- Nissen, R.D.; Gildberg, F.A.; Hvidt, N.C. Approaching the religious psychiatric patient in a secular country: Does “subalternalizing” religious patients mean they do not exist? Arch. Psychol. Relig. 2019, 41, 123–140. [Google Scholar] [CrossRef]
- Jones, K.F.; Paal, P.; Symons, X.; Best, M.C. The Content, Teaching Methods and Effectiveness of Spiritual Care Training for Healthcare Professionals: A Mixed-Methods Systematic Review. J. Pain Symptom Manag. 2021, 62, e261–e278. [Google Scholar] [CrossRef]
- Balboni, M.J.; Sullivan, A.; Enzinger, A.C.; Epstein-Peterson, Z.D.; Tseng, Y.D.; Mitchell, C.; Niska, J.; Zollfrank, A.; VanderWeele, T.J.; Balboni, T.A. Nurse and Physician Barriers to Spiritual Care Provision at the End of Life. J. Pain Symptom Manag. 2014, 48, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Bar-Sela, G.; Schultz, M.J.; Elshamy, K.; Rassouli, M.; Ben-Arye, E.; Doumit, M.; Gafer, N.; Albashayreh, A.; Ghrayeb, I.; Turker, I.; et al. Training for awareness of one’s own spirituality: A key factor in overcoming barriers to the provision of spiritual care to advanced cancer patients by doctors and nurses. Palliat. Support. Care 2019, 17, 345–352. [Google Scholar] [CrossRef]
- Berger, P.L. The Many Altars of Modernity; De Gruyter: Berlin, Germany, 2014. [Google Scholar]
- Nissen, R.D.; Viftrup, D.T.; Hvidt, N.C. The Process of Spiritual Care. Front. Psychol. 2021, 12, 674453. [Google Scholar] [CrossRef]
- Habermas, J. Notes on Post-Secular Society. New Perspect. Q. 2008, 25, 17–29. [Google Scholar] [CrossRef]
- Gorski, P.; Kim, D.K.; Torpey, J.; VanAntwerpen, J. The Post-Secular in Question: Religion in Contemporary Society; NYU Press: New York, NY, USA, 2012. [Google Scholar]
- Nynäs, P.; Lassander, M.; Utriainen, T. (Eds.) Post-Secular Society, 1st ed.; Transaction Publishers: New Brunswick, NJ, USA, 2012. [Google Scholar] [CrossRef]
- Berger, P.L. The Hospital: On the Interface between Secularity and Religion. Society 2015, 52, 410–412. [Google Scholar] [CrossRef]
- Puchalski, C.; Ferrell, B.; Virani, R.; Otis-Green, S.; Baird, P.; Bull, J.; Chochinov, H.; Handzo, G.; Nelson-Becker, H.; Prince-Paul, M.; et al. Improving the quality of spiritual care as a dimension of palliative care: The report of the Consensus Conference. J. Palliat. Med. 2009, 12, 885–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Strengthening of Palliative Care as a Component of Integrated Treatment throughout the Life Course. J. Pain Palliat. Care Pharmacother. 2014, 28, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Gijsberts, M.H.E.; van der Steen, J.T.; Hertogh, C.; Deliens, L. Spiritual care provided by nursing home physicians: A nationwide survey. BMJ Support. Palliat. Care 2019, 10, e42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrad, R.; Cosentino, C.; Keasley, R.; Sulla, F. Spiritual care in nursing: An overview of the measures used to assess spiritual care provision and related factors amongst nurses. Acta Biomed. 2019, 90, 44–55. [Google Scholar]
- Drummond, D.A.; Carey, L.B. Assessing Spiritual Well-Being in Residential Aged Care: An Exploratory Review. J. Relig. Health 2018, 58, 372–390. [Google Scholar] [CrossRef]
- Seddigh, R.; Keshavarz-Akhlaghi, A.-A.; Azarnik, S. Questionnaires Measuring Patients’ Spiritual Needs: A Narrative Literature Review. Iran J. Psychiatry Behav. Sci. 2016, 10, e4011. [Google Scholar] [CrossRef] [Green Version]
- Lucchetti, G.; Bassi, R.M.; Lucchetti, A.L.G. Taking Spiritual History in Clinical Practice: A Systematic Review of Instruments. Explore 2013, 9, 159–170. [Google Scholar] [CrossRef]
- Ghorbani, M.; Mohammadi, E.; Aghabozorgi, R.; Ramezani, M. Spiritual care interventions in nursing: An integrative literature review. Support. Care Cancer 2021, 29, 1165–1181. [Google Scholar] [CrossRef] [PubMed]
- Büssing, A. The Spiritual Needs Questionnaire in Research and Clinical Application: A Summary of Findings. J. Relig. Health 2021, 60, 3732–3748. [Google Scholar] [CrossRef] [PubMed]
- Damberg Nissen, R.; Falkø, E.; Toudal Viftrup, D.; Assing Hvidt, E.; Søndergaard, J.; Büssing, A.; Wallin, J.A.; Hvidt, N.C. The Catalogue of Spiritual Care Instruments: A Scoping Review. Religions 2020, 11, 252. [Google Scholar] [CrossRef]
- Büssing, A.; Janko, A.; Baumann, K.; Hvidt, N.C.; Kopf, A. Spiritual Needs among Patients with Chronic Pain Diseases and Cancer Living in a Secular Society. Pain Med. 2013, 14, 1362–1373. [Google Scholar] [CrossRef] [PubMed]
- Casanova, J. Are We Still Secular? Explorations on the Secular and the Post-Secular. In Post-Secular Society; Nynäs, P., Lassander, M., Utriainen, T., Eds.; Transaction Publishers: Piscataway, NJ, USA, 2012. [Google Scholar]
- Beaumont, J.; Eder, K.; Mendieta, E. Reflexive secularization? Concepts, processes and antagonisms of postsecularity. Eur. J. Soc. Theory 2018, 23, 291–309. [Google Scholar] [CrossRef]
- Casanova, J.; van den Breemer, R.; Wyller, T. Secular and Sacred: The Scandinavian Case of Religion in Human Rights, Law and Public Space; Vandenhoeck and Ruprecht: Göttingen, Germany, 2014. [Google Scholar]
- La Cour, P.; Hvidt, N.C. Research on meaning-making and health in secular society: Secular, spiritual and religious existential orientations. Soc. Sci. Med. 2010, 71, 1292–1299. [Google Scholar] [CrossRef] [PubMed]
- Hvidt, N.C.; Assing Hvidt, E.; la Cour, P. Meanings of “the existential” in a Secular Country: A Survey Study. J. Relig. Health 2021. [Google Scholar] [CrossRef] [PubMed]
- Nissen, R.D.; Andersen, A. Addressing Religion in Secular Healthcare: Existential communication and the post-secular negotiation. Religions 2021, in press. [Google Scholar]
- Nolan, S.; Saltmarsh, P.; Leget, C.J.W. Spiritual care in palliative care—Working towards an EAPC Task Force. Eur. J. Palliat. Care 2021, 18, 86–89. [Google Scholar]
- Hvidt, N.C.; Nielsen, K.T.; Kørup, A.K.; Prinds, C.; Hansen, D.G.; Viftrup, D.T.; Hvidt, E.A.; Hammer, E.R.; Falkø, E.; Locher, F.; et al. What is spiritual care? Professional perspectives on the concept of spiritual care identified through group concept mapping. BMJ Open 2020, 10, e042142. [Google Scholar] [CrossRef]
- Ramezani, M.; Ahmadi, F.; Mohammadi, E.; Kazemnejad, A. Spiritual care in nursing: A concept analysis. Int. Nurs. Rev. 2014, 61, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Descola, P. Beyond Nature and Culture; University of Chicago Press: Chicago, IL, USA, 2014. [Google Scholar]
- Koenig, H.G. Concerns about Measuring “Spirituality” in Research. J. Nerv. Ment. Dis. 2008, 196, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Grabenweger, R.; Paal, P. Spiritualität in der psychiatrischen Pflege—Begriffsanalyse und Vorschlag einer Arbeitsdefinition. Spirit. Care 2021, 10, 53–62. [Google Scholar] [CrossRef]
- Saad, M.; de Medeiros, R. Spirituality and Healthcare—Common Grounds for the Secular and Religious Worlds and Its Clinical Implications. Religions 2021, 12, 22. [Google Scholar] [CrossRef]
- Zinnbauer, B.J.; Pargament, K.I.; Cole, B.; Rye, M.S.; Butter, E.M.; Belavich, T.G.; Hipp, K.M.; Scott, A.B.; Kadar, J.L. Religion and Spirituality: Unfuzzying the Fuzzy. J. Sci. Study Relig. 1997, 36, 549. [Google Scholar] [CrossRef]
- Huguelet, P.; Koenig, H.G. Religion and Spirituality in Psychiatry; Cambridge University Press: Cambridge, UK, 2009. [Google Scholar] [CrossRef]
- Bash, A. Spirituality: The emperor’s new clothes? J. Clin. Nurs. 2004, 13, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef] [PubMed]
- De Souza, M.T.; Da Silva, M.D.; De Carvalho, R. Integrative review: What is it? How to do it? Einstein 2010, 8, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.R. A general inductive approach for analyzing qualitative evaluation data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Gildberg, F.A.; Bradley, S.K.; Tingleff, E.B.; Hounsgaard, L. Empirically Testing Thematic Analysis (ETTA): Methodological implications in textual analysis coding system. Nordisk Sygeplejeforskning 2015, 5, 193–207. [Google Scholar] [CrossRef]
- Charmaz, K. Constructing Grounded Theory; A Practical Guide Through Qualitative Analysis; Sage Publications: London, UK, 2006. [Google Scholar]
- Lo, C.; Panday, T.; Zeppieri, J.; Rydall, A.; Murphy-Kane, P.; Zimmermann, C.; Rodin, G. Preliminary psychometrics of the Existential Distress Scale in patients with advanced cancer. Eur. J. Cancer Care 2017, 26, e12597. [Google Scholar] [CrossRef]
- Pinto, S.M.O.; Berenguer, S.M.A.C.; Martins, J.C.A.; Kolcaba, K. Cultural adaptation and validation of the Portuguese End of Life Spiritual Comfort Questionnaire in Palliative Care patients. Porto Biomed. J. 2016, 1, 147–152. [Google Scholar] [CrossRef] [Green Version]
- Peterman, A.H.; Fitchett, G.; Brady, M.J.; Hernandez, L.; Cella, D. Measuring spiritual well-being in people with cancer: The functional assessment of chronic illness therapy—Spiritual well-being scale (FACIT-Sp). Ann. Behav. Med. 2002, 24, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.W.; Wong, F.K.Y.; Yeung, S.M.; Sum, F. Holistic Health Status Questionnaire: Developing a measure from a Hong Kong Chinese population. Health Qual. Life Outcomes 2016, 14, 28. [Google Scholar] [CrossRef] [Green Version]
- Jim, H.S.; Purnell, J.; Richardson, S.A.; Golden-Kreutz, D.; Andersen, B.L. Measuring meaning in life following cancer. Qual. Life Res. 2006, 15, 1355–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chochinov, H.M.; Hassard, T.; McClement, S.; Hack, T.; Kristjanson, L.J.; Harlos, M.; Sinclair, S.; Murray, A. The Patient Dignity Inventory: A Novel Way of Measuring Dignity-Related Distress in Palliative Care. J. Pain Symptom Manag. 2008, 36, 559–571. [Google Scholar] [CrossRef] [PubMed]
- Galek, K.; Flannelly, K.J.; Vane, A.; Galek, R.M. Assessing a Patient’s Spiritual Needs: A comprehensive instrument. Holist. Nurs. Pract. 2005, 19, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Faull, K.; Hills, M.D. A spiritually-based measure of holistic health for those with disabilities: Development, preliminary reliability and validity assessment. Disabil. Rehabil. 2007, 29, 999–1010. [Google Scholar] [CrossRef] [PubMed]
- Vivat, B.; Young, T.; Winstanley, J.; Arraras, J.; Black, K.; Boyle, F.; Bredart, A.; Costantini, A.; Guo, J.; Irarrazaval, M.; et al. The international phase 4 validation study of the EORTC QLQ-SWB32: A stand-alone measure of spiritual well-being for people receiving palliative care for cancer. Eur. J. Cancer Care 2017, 26, e12697. [Google Scholar] [CrossRef]
- Vilalta, A.; Valls, J.; Porta, J.; Viñas, J. Evaluation of Spiritual Needs of Patients with Advanced Cancer in a Palliative Care Unit. J. Palliat. Med. 2014, 17, 592–600. [Google Scholar] [CrossRef] [Green Version]
- Büssing, A.; Balzat, H.-J.; Heusser, P. Spiritual needs of patients with chronic pain diseases and cancer—Validation of the spiritual needs questionnaire. Eur. J. Med Res. 2010, 15, 266–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokkink, L.B.; De Vet, H.C.W.; Prinsen, C.A.C.; Patrick, D.L.; Alonso, J.; Bouter, L.; Terwee, C.B. COSMIN Risk of Bias checklist for systematic reviews of Patient-Reported Outcome Measures. Qual. Life Res. 2018, 27, 1171–1179. [Google Scholar] [CrossRef] [Green Version]
- Brintz, C.E.; Birnbaum-Weitzman, O.; Merz, E.L.; Penedo, F.J.; Daviglus, M.L.; Fortmann, A.L.; Gallo, L.C.; Gonzalez, P.; Johnson, T.P.; Navas-Nacher, E.L.; et al. Validation of the Functional Assessment of Chronic Illness Therapy-Spiritual Well-Being-expanded (FACIT-Sp-Ex) across English and Spanish-speaking Hispanics/Latinos: Results from the Hispanic Community Health Study/Study of Latinos Sociocultural Ancillary Study. Psychol. Relig. Spirit. 2017, 9, 337–347. [Google Scholar] [CrossRef]
- Fuente-Cobo, C.; Carabante-Muntada, J.M. Media and Religion in Spain: A Review of Major Trends. J. Relig. Media Digit. Cult. 2018, 7, 175–202. [Google Scholar] [CrossRef]
- Administration USNAaR. National Archives. 2021. Available online: https://www.archives.gov/founding-docs (accessed on 21 October 2021).
- Holbraad, M.; Pedersen, M.A. The Ontological Turn: An Anthropological Exposition; Cambridge University Press: Cambridge, UK, 2017. [Google Scholar] [CrossRef]
- Nelson-Becker, H.; Moeke-Maxwell, T. Spiritual Diversity, Spiritual Assessment, and Māori End-of-Life Perspectives: Attaining Ka Ea. Religions 2020, 11, 536. [Google Scholar] [CrossRef]
- Bandini, J.; Thiel, M.; Meyer, E.; Paasche-Orlow, S.; Zhang, Q.; Cadge, W. Interprofessional spiritual care training for geriatric care providers. Innov. Aging 2018, 2, 963. [Google Scholar] [CrossRef]
- Puchalski, C.; Jafari, N.; Buller, H.; Haythorn, T.; Jacobs, C.; Ferrell, B. Interprofessional Spiritual Care Education Curriculum: A Milestone toward the Provision of Spiritual Care. J. Palliat. Med. 2020, 23, 777–784. [Google Scholar] [CrossRef]
- Attard, J.; Baldacchino, D.R.; Camilleri, L. Nurses’ and midwives’ acquisition of competency in spiritual care: A focus on education. Nurse Educ. Today 2014, 34, 1460–1466. [Google Scholar] [CrossRef] [PubMed]
- Viftrup, D.T.; Laursen, K.; Hvidt, N.C. Developing an Educational Course in Spiritual Care: An Action Research Study at Two Danish Hospices. Religions 2021, 12, 827. [Google Scholar] [CrossRef]
- Moestrup, L.; Hvidt, N.C. Where is God in my dying? A qualitative investigation of faith reflections among hospice patients in a secularized society. Death Stud. 2016, 40, 618–629. [Google Scholar] [CrossRef]
- Austin, P.; Macdonald, J.; MacLeod, R. Measuring Spirituality and Religiosity in Clinical Settings: A Scoping Review of Available Instruments. Religions 2018, 9, 70. [Google Scholar] [CrossRef] [Green Version]
- Timmins, F.; Murphy, M.; Caldeira, S.; Ging, E.; King, C.; Brady, V.; Whelan, J.; O’Boyle, C.; Kelly, J.; Neill, F.; et al. Developing Agreed and Accepted Understandings of Spirituality and Spiritual Care Concepts among Members of an Innovative Spirituality Interest Group in the Republic of Ireland. Religions 2016, 7, 30. [Google Scholar] [CrossRef] [Green Version]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willis, G.B. Cognitive Interviewing: A Tool for Improving Questionnaire Design; SAGE Publications: London, UK, 2005; ISBN 978-0761928041. [Google Scholar]
- Forsyth, B.H.; Kudela, M.S.; Levin, K.; Lawrence, D.; Willis, G.B. Methods for Translating an English-Language Survey Questionnaire on Tobacco Use into Mandarin, Cantonese, Korean, and Vietnamese. Field Methods 2007, 19, 264–283. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Inclusion: The Instrument Had to Be (Listed Alphabetically) |
|---|
| A spiritual needs assessment questionnaire or applicable as such |
| Applicable as a self-report questionnaire |
| Any of the following target groups: chronic disease patients, life-threatening illness, or terminal patients (end-of-life) |
| Deemed applicable in a post-secular context, by initial face validation |
| Published in a peer-review journal |
| Written in English |
| Instrument Name Abbreviation | Author, Origin Year | Health Field | Likert Scale | Number of Questions |
|---|---|---|---|---|
|
Existential Distress Scale EDS | Lo et al. Canada 2017 [50] | Cancer | 5 | 10 |
|
(Portuguese) End of Life Spiritual Comfort Questionnaire EOLSCQ | Pinto et al. Portugal 2016 [51] | EOL/PC | 6 | 28 |
|
Functional Assessment of Chronic Illness Therapy —Spiritual Well-Being Scale FACIT-Sp-12 | Peterman et al. USA 2002 [52] | Cancer—Chronic illness | 5 | 12 |
|
Holistic Health Status Questionnaire HHSQ | Chan et al. Hong Kong 2016 [53] | Chronic illness | 4 | 45 |
|
Meaning in Life Scale MiLS | Jim et al. USA 2006 [54] | Cancer | 6/4 | 21 |
|
Patient Dignity Inventory PDI | Chochinov et al. Canada 2008 [55] | EOL/PC | 5 | 25 |
|
Patient Spiritual Needs Assessment Scale PSNAS | Galek et al. USA 2005 [56] | EOL/PC | 6 | 29 |
|
QE Health Scale QEHS | Faull & Hill, New Zealand 2007 [57] | Chronic physical disabilities | 5 | 28 |
|
Quality of Life Questionnaire—Spiritual Wellbeing—32 QLQ-SWB–32 | Vivat et al. EU 2017 [58] | EOL/PC | 4/8 | 32 |
|
Spiritual Needs Questionnaire for Palliative Care SNQPC | Vilalta et al. Spain 2014 [59] | Cancer/PC | 5 | 28 |
|
Spiritual Needs Questionnaire SpNQ | Büssing et al. Germany 2010 [60] | Cancer—Chronic illness | Y/N/3 | 27 |
| RS Word | N | RS Word | N | RS Word | N | RS Word | N |
|---|---|---|---|---|---|---|---|
| Angel | 1 | Fate | 1 | Pastor | 1 | Religion | 11 |
| Allah | 1 | God | 8 | Pilgrimage | 1 | Ritual | 1 |
| Christian resurrection | 1 | Heaven | 1 | Power outside yourself | 1 | Sacrament | 1 |
| Divine intervention | 1 | Higher presence | 1 | Pray | 7 | Saint | 1 |
| Divine punishment | 1 | Karma | 1 | Predestined | 1 | Spirituality | 24 |
| Faith | 9 | Life after death | 1 | Reincarnation | 1 |
| Existential | Socio-Somatic | Total | ||||||
|---|---|---|---|---|---|---|---|---|
| Instrument | R | S | RS | SEC | L | SOC | SOM | |
| EDS | 0 | 0 | 0 | 6 | 1 | 3 | 0 | 10 |
| EOLSCQ | 1 | 0 | 0 | 13 | 0 | 4 | 10 | 28 |
| FACIT-Sp-12 | 0 | 0 | 3 | 8 | 1 | 0 | 0 | 12 |
| HHSQ | 5 | 1 | 0 | 18 | 1 | 7 | 13 | 45 |
| MiLS | 0 | 0 | 3 | 18 | 0 | 0 | 0 | 21 |
| PDI | 0 | 1 | 0 | 13 | 2 | 4 | 5 | 25 |
| PSNAS | 1 | 1 | 3 | 15 | 2 | 4 | 3 | 29 |
| QEHS | 0 | 2 | 1 | 19 | 0 | 4 | 2 | 28 |
| QLQ-SWB-32 | 2 | 1 | 7 | 16 | 1 | 5 | 0 | 32 |
| SNQPC | 6 | 1 | 0 | 8 | 5 | 4 | 4 | 28 |
| SpNQ | 6 | 0 | 1 | 8 | 3 | 9 | 0 | 27 |
| Instrument | Items Selected Based on Interviews | Content Validity | Construct Validity | Reliability | Internal Consistency | Measurement Error | Responsiveness |
|---|---|---|---|---|---|---|---|
| EDS | + | + | + | - | + | - | - |
| EOLSCQ | - | + | + | - | + | - | - |
| FACIT-Sp-12 | + | + | + | + | + | - | - |
| HHSQ | + | + | + | + | + | - | - |
| MiLS | - | + | + | + | + | - | - |
| PDI | + | + | + | + | + | - | - |
| PSNAS | - | - | - | - | - | - | - |
| QEHS | + | + | + | + | + | - | - |
| QLQ-SWB-32 | + | + | + | + | + | - | - |
| SNQPC | + | + | - | - | - | - | - |
| SpNQ | + | + | + | - | + | - | - |
| Instrument | RS Wording | N of Questions with RS Wording | Neutral |
|---|---|---|---|
| EDS | 0 | 0 | Yes |
| EOLSCQ | Faith | 1 | Yes |
| FACIT-Sp-12 | Faith, Spiritual | 2 | Yes |
| HHSQ | Divine intervention, Fate, God, Heavens, Karma, Pray, Predestined, Religion | 6 | No |
| MiLS | Faith, Spiritual | 2 | Yes |
| PDI | Spiritual | 1 | Yes |
| PSNAS | Power outside yourself, Pray, Ritual, Religious, Spiritual | 5 | Yes |
| QEHS | Faith, God, Spiritual | 3 | No |
| QLQ-SWB-32 | God, Life after death, Meditation, Pray, Spiritual | 10 | No |
| SNQPC | Christian resurrection, Divine punishment, Faith, God, Pilgrimage, Reincarnation, Religious, Sacrament | 7 | No |
| SpNQ | Allah, Angels, God, Higher presence, Life after death, Pastor, Pray, Religious, Saints, Spiritual | 7 | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nissen, R.D.; Falkø, E.; Stripp, T.K.; Hvidt, N.C. Spiritual Needs Assessment in Post-Secular Contexts: An Integrative Review of Questionnaires. Int. J. Environ. Res. Public Health 2021, 18, 12898. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182412898
Nissen RD, Falkø E, Stripp TK, Hvidt NC. Spiritual Needs Assessment in Post-Secular Contexts: An Integrative Review of Questionnaires. International Journal of Environmental Research and Public Health. 2021; 18(24):12898. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182412898
Chicago/Turabian StyleNissen, Ricko D., Erik Falkø, Tobias K. Stripp, and Niels Christian Hvidt. 2021. "Spiritual Needs Assessment in Post-Secular Contexts: An Integrative Review of Questionnaires" International Journal of Environmental Research and Public Health 18, no. 24: 12898. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182412898