
Prevalence of Asthma and Its Associating Environmental Factors among 6–12-Year-Old Schoolchildren in a Metropolitan Environment—A Cross-Sectional, Questionnaire-Based Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Study Design
2.3. The Questionnaire
2.4. Statistical Analysis and Data Visualization
3. Results
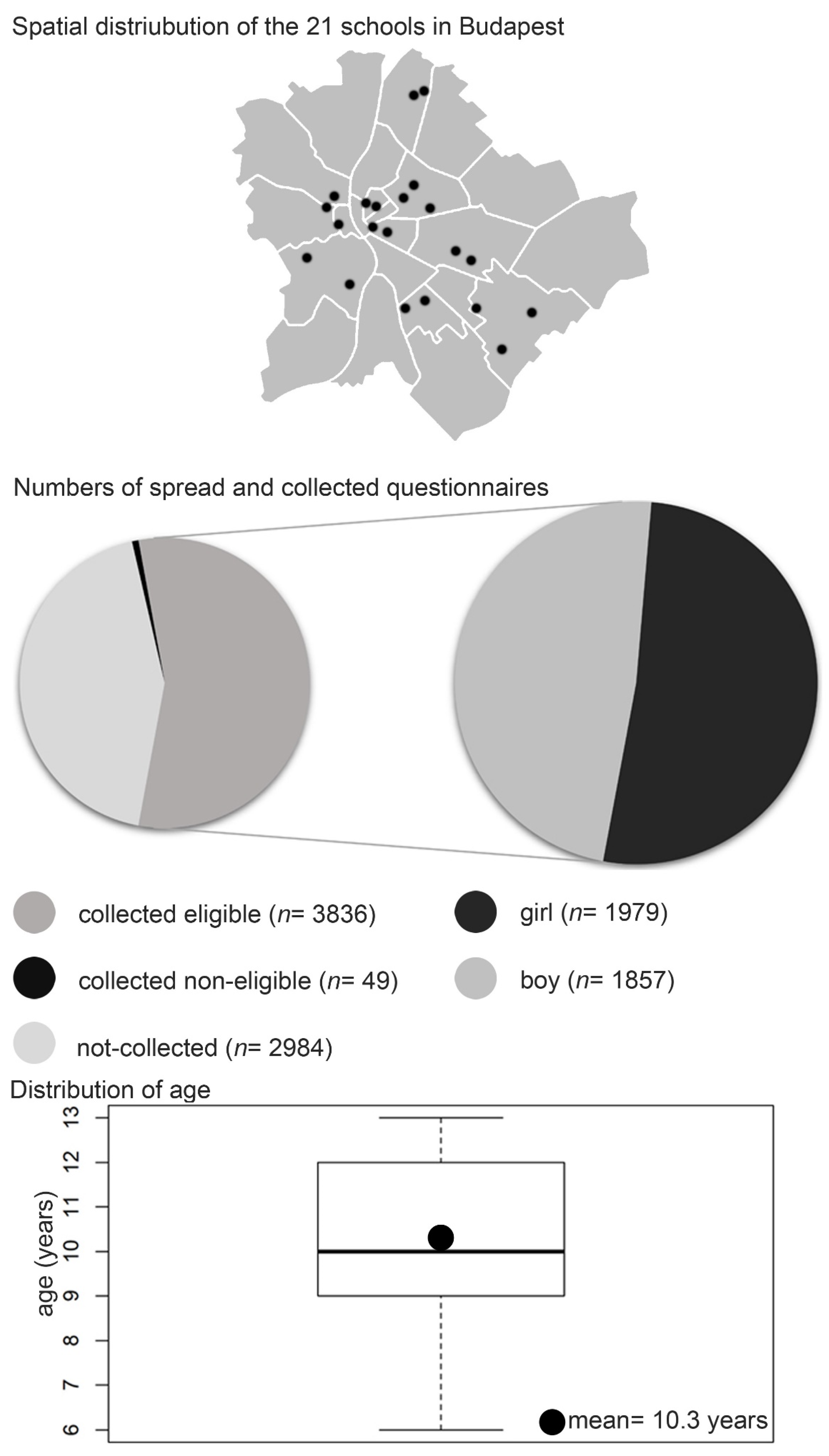
3.1. Data Acquisition, Refinement and Demographic Parameters of the Study Group
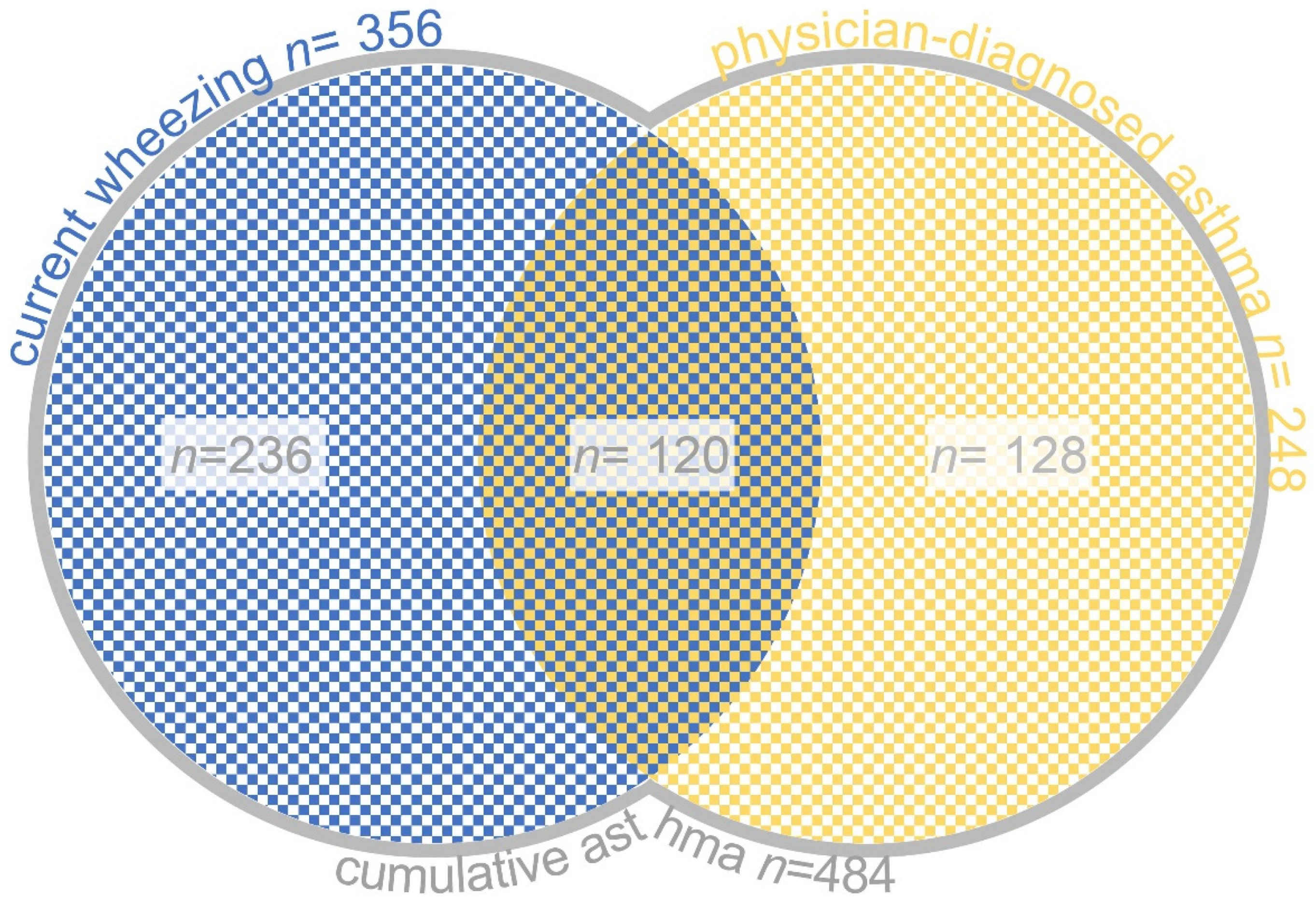
3.2. Prevalence of Asthma
3.3. The Severity of Asthma and Associating Atopic Diseases
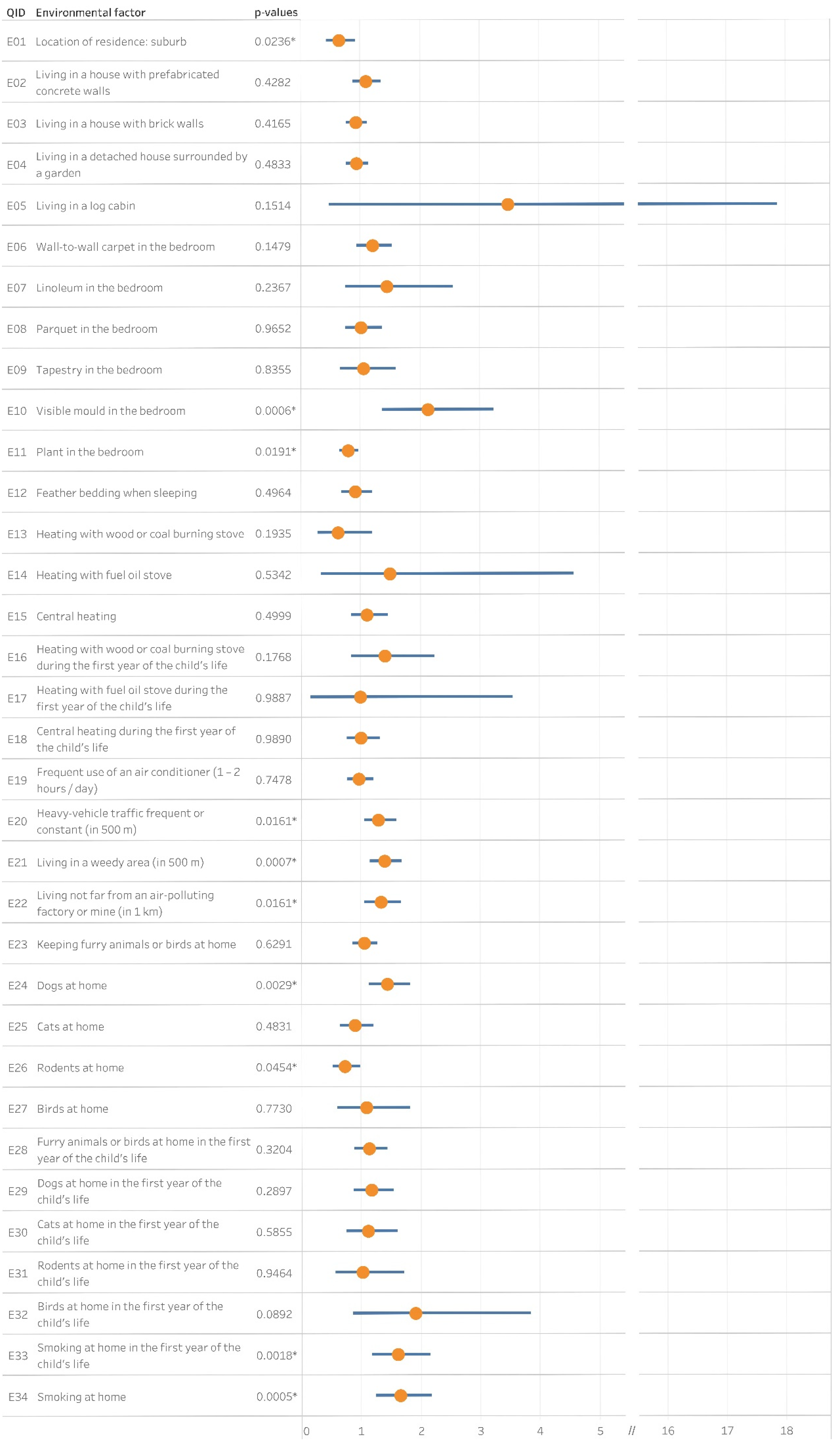
3.4. Environmental Risk Factors
3.5. Lifestyle Factors
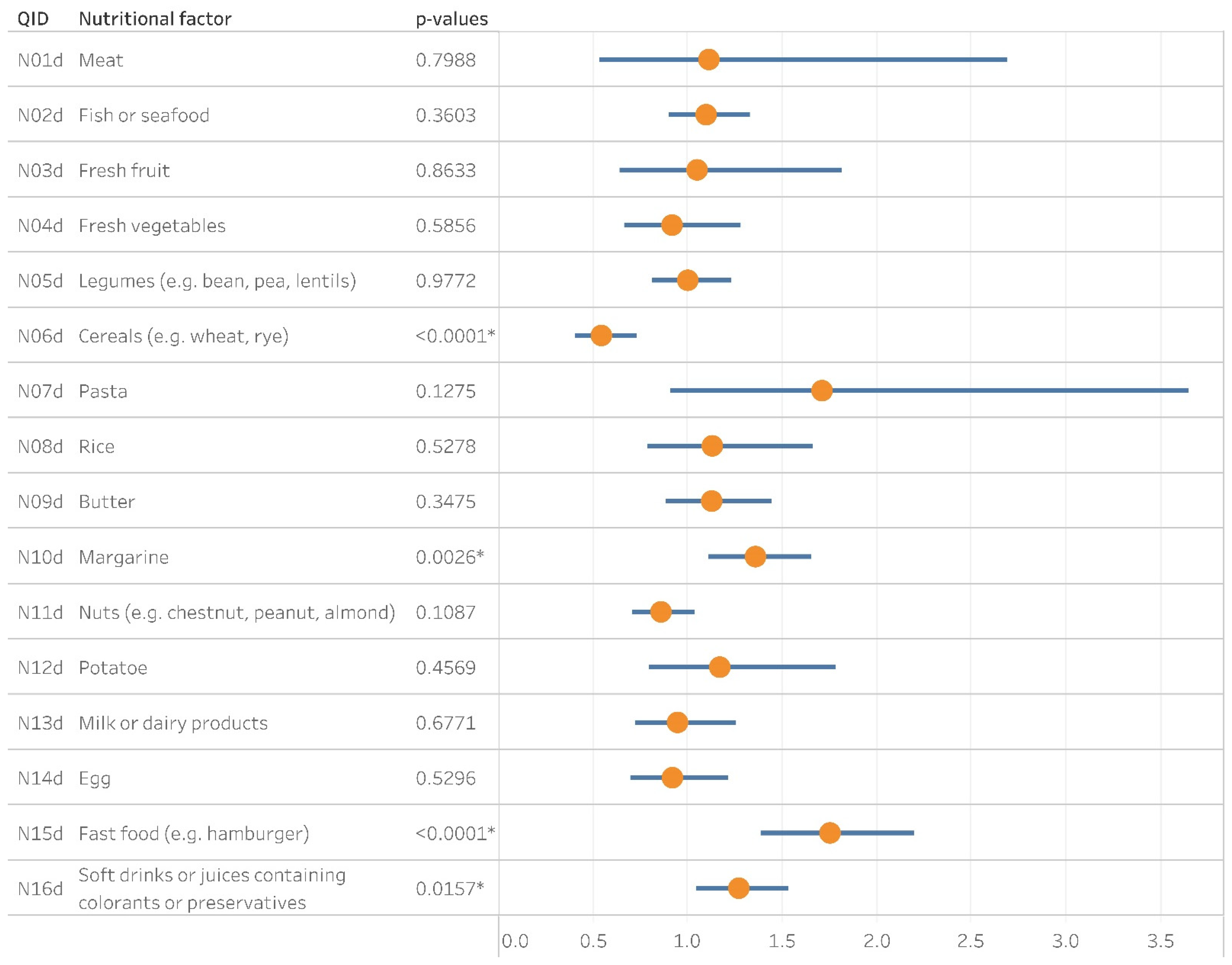
3.6. Nutritional Factors
4. Discussion
5. Limitations and Strengths
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention; The Global Initiative for Asthma (GINA): Fontana, WI, USA, 2021. [Google Scholar]
- The Global Initiative for Asthma (GINA). The Global Asthma Report 2018; The Global Initiative for Asthma (GINA): Fontana, WI, USA, 2018. [Google Scholar]
- Ellwood, P.; Asher, M.I.; Beasley, R.; Clayton, T.O.; Stewart, A.W.; ISAAC Steering Committee; ISAAC Phase Three Study Group. ISAAC Phase Three Manual; ISAAC International Data Centre: Auckland, New Zealand, 2000; p. 94. [Google Scholar]
- Mallol, J.; Crane, J.; von Mutius, E.; Odhiambo, J.; Keil, U.; Stewart, A.; Group, I.P.T.S. The International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three: A global synthesis. Allergol Immunopathol. 2013, 41, 73–85. [Google Scholar] [CrossRef] [Green Version]
- Ágfalvi, R.; Blatniczky, L.; Darvay, S.; Joubert, K. 3sz Módszertani Levél—Útmutató és Táblázatok a Gyermekkori Tápláltság Megítéléséhez [3rd Metholdological Letter—Guideline and Tables for the Evaluation of Childhood Nutrition]; Magyar Védőnők Egyesülete (MAVE): Budapest, Hungary, 2004. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing, R-3.6.2. for Windows; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- ISAAC Phase Three Study Group. ISAAC Phase Three Data. Available online: http://isaac.auckland.ac.nz/phases/phasethree/results/results.php (accessed on 4 January 2020).
- Bjerg, A.; Sandstrom, T.; Lundback, B.; Ronmark, E. Time trends in asthma and wheeze in Swedish children 1996–2006: Prevalence and risk factors by sex. Allergy 2010, 65, 48–55. [Google Scholar] [CrossRef]
- Aberle, N.; Kljaic Bukvic, B.; Blekic, M.; Vuckovic, M.; Bardak, D.; Gudelj, A.; Cancarevic, G.; Franic, M. Allergic Diseases and Atopy among Schoolchildren in Eastern Croatia. Acta Clin. Croat. 2018, 57, 82–90. [Google Scholar] [CrossRef]
- Horak, E.; Morass, B.; Ulmer, H.; Genuneit, J.; Braun-Fahrlander, C.; von Mutius, E.; Group, G.S. Prevalence of wheezing and atopic diseases in Austrian schoolchildren in conjunction with urban, rural or farm residence. Wien. Klin. Wochenschr. 2014, 126, 532–536. [Google Scholar] [CrossRef]
- Lu, Y.; Lin, S.; Lawrence, W.R.; Lin, Z.; Gurzau, E.; Csobod, E.; Neamtiu, I.A. Evidence from SINPHONIE project: Impact of home environmental exposures on respiratory health among school-age children in Romania. Sci. Total Environ. 2018, 621, 75–84. [Google Scholar] [CrossRef]
- Zhuge, Y.; Qian, H.; Zheng, X.; Huang, C.; Zhang, Y.; Li, B.; Zhao, Z.; Deng, Q.; Yang, X.; Sun, Y.; et al. Effects of parental smoking and indoor tobacco smoke exposure on respiratory outcomes in children. Sci. Rep. 2020, 10, 4311. [Google Scholar] [CrossRef] [Green Version]
- Rennie, D.C.; Karunanayake, C.P.; Lawson, J.A.; Kirychuk, S.; McMullin, K.; Abonyi, S.; Seeseequasis, J.; MacDonald, J.; Dosman, J.A.; Pahwa, P. Domestic Risk Factors for Atopic and non-Atopic Asthma in First Nations Children Living in Saskatchewan, Canada. Children 2020, 7, 38. [Google Scholar] [CrossRef]
- Sharpe, R.A.; Thornton, C.R.; Tyrrell, J.; Nikolaou, V.; Osborne, N.J. Variable risk of atopic disease due to indoor fungal exposure in NHANES 2005–2006. Clin. Exp. Allergy 2015, 45, 1566–1578. [Google Scholar] [CrossRef]
- Zhang, Z.; Reponen, T.; Hershey, G.K. Fungal Exposure and Asthma: IgE and Non-IgE-Mediated Mechanisms. Curr. Allergy Asthma Rep. 2016, 16, 86. [Google Scholar] [CrossRef]
- Caillaud, D.; Leynaert, B.; Keirsbulck, M.; Nadif, R. Indoor mould exposure, asthma and rhinitis: Findings from systematic reviews and recent longitudinal studies. Eur. Respir. Rev. 2018, 27, 1701037. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Liu, Q.; Chen, Y.; Yang, B.; Huang, X.; Li, Y.; Zhang, J.J. Effects of indoor environment and lifestyle on respiratory health of children in Chongqing, China. J. Thorac. Dis. 2020, 12, 6327–6341. [Google Scholar] [CrossRef]
- Fagbule, D.; Ekanem, E.E. Some environmental risk factors for childhood asthma: A case-control study. Ann. Trop. Paediatr. 1994, 14, 15–19. [Google Scholar] [CrossRef]
- Fretzayas, A.; Kotzia, D.; Moustaki, M. Controversial role of pets in the development of atopy in children. World J. Pediatr. 2013, 9, 112–119. [Google Scholar] [CrossRef]
- Poowuttikul, P.; Saini, S.; Seth, D. Inner-City Asthma in Children. Clin. Rev. Allergy Immunol. 2019, 56, 248–268. [Google Scholar] [CrossRef]
- Lodrup Carlsen, K.C.; Roll, S.; Carlsen, K.H.; Mowinckel, P.; Wijga, A.H.; Brunekreef, B.; Torrent, M.; Roberts, G.; Arshad, S.H.; Kull, I.; et al. Does pet ownership in infancy lead to asthma or allergy at school age? Pooled analysis of individual participant data from 11 European birth cohorts. PLoS ONE 2012, 7, e43214. [Google Scholar] [CrossRef] [Green Version]
- Collin, S.M.; Granell, R.; Westgarth, C.; Murray, J.; Paul, E.; Sterne, J.A.; John Henderson, A. Pet ownership is associated with increased risk of non-atopic asthma and reduced risk of atopy in childhood: Findings from a UK birth cohort. Clin. Exp. Allergy 2015, 45, 200–210. [Google Scholar] [CrossRef] [Green Version]
- Oluwole, O.; Arinola, G.O.; Huo, D.; Olopade, C.O. Household biomass fuel use, asthma symptoms severity, and asthma underdiagnosis in rural schoolchildren in Nigeria: A cross-sectional observational study. BMC Pulm. Med. 2017, 17, 3. [Google Scholar] [CrossRef] [Green Version]
- Erwin, E.A.; Custis, N.; Ronmark, E.; Wickens, K.; Sporik, R.; Woodfolk, J.A.; Platts-Mills, T.A. Asthma and indoor air: Contrasts in the dose response to cat and dust-mite. Indoor Air 2005, 15 (Suppl. 10), 33–39. [Google Scholar] [CrossRef]
- Takkouche, B.; Gonzalez-Barcala, F.J.; Etminan, M.; Fitzgerald, M. Exposure to furry pets and the risk of asthma and allergic rhinitis: A meta-analysis. Allergy 2008, 63, 857–864. [Google Scholar] [CrossRef]
- Bowatte, G.; Lodge, C.; Lowe, A.J.; Erbas, B.; Perret, J.; Abramson, M.J.; Matheson, M.; Dharmage, S.C. The influence of childhood traffic-related air pollution exposure on asthma, allergy and sensitization: A systematic review and a meta-analysis of birth cohort studies. Allergy 2015, 70, 245–256. [Google Scholar] [CrossRef]
- Gentile, D.A.; Morphew, T.; Elliott, J.; Presto, A.A.; Skoner, D.P. Asthma prevalence and control among schoolchildren residing near outdoor air pollution sites. J. Asthma 2020, 1–11. [Google Scholar] [CrossRef]
- Khreis, H.; Nieuwenhuijsen, M.J. Traffic-Related Air Pollution and Childhood Asthma: Recent Advances and Remaining Gaps in the Exposure Assessment Methods. Int. J. Environ. Res. Public Health 2017, 14, 312. [Google Scholar] [CrossRef] [Green Version]
- Khreis, H.; Kelly, C.; Tate, J.; Parslow, R.; Lucas, K.; Nieuwenhuijsen, M. Exposure to traffic-related air pollution and risk of development of childhood asthma: A systematic review and meta-analysis. Environ. Int. 2017, 100, 1–31. [Google Scholar] [CrossRef] [Green Version]
- Sultesz, M.; Horvath, A.; Molnar, D.; Katona, G.; Mezei, G.; Hirschberg, A.; Galffy, G. Prevalence of allergic rhinitis, related comorbidities and risk factors in schoolchildren. Allergy Asthma Clin. Immunol. 2020, 16, 98. [Google Scholar] [CrossRef]
- Voros, K.; Bobvos, J.; Varro, J.M.; Malnasi, T.; Koi, T.; Magyar, D.; Rudnai, P.; Paldy, A. Impacts of long-term ragweed pollen load and other potential risk factors on ragweed pollen allergy among schoolchildren in Hungary. Ann. Agric. Environ. Med. 2018, 25, 307–313. [Google Scholar] [CrossRef]
- Ogershok, P.R.; Warner, D.J.; Hogan, M.B.; Wilson, N.W. Prevalence of pollen sensitization in younger children who have asthma. Allergy Asthma Proc. 2007, 28, 654–658. [Google Scholar] [CrossRef]
- Mitchell, E.A.; Beasley, R.; Bjorksten, B.; Crane, J.; Garcia-Marcos, L.; Keil, U.; Group, I.P.T.S. The association between BMI, vigorous physical activity and television viewing and the risk of symptoms of asthma, rhinoconjunctivitis and eczema in children and adolescents: ISAAC Phase Three. Clin. Exp. Allergy 2013, 43, 73–84. [Google Scholar] [CrossRef]
- Glazebrook, C.; McPherson, A.C.; Macdonald, I.A.; Swift, J.A.; Ramsay, C.; Newbould, R.; Smyth, A. Asthma as a barrier to children’s physical activity: Implications for body mass index and mental health. Pediatrics 2006, 118, 2443–2449. [Google Scholar] [CrossRef]
- Lang, D.M.; Butz, A.M.; Duggan, A.K.; Serwint, J.R. Physical activity in urban school-aged children with asthma. Pediatrics 2004, 113, e341–e346. [Google Scholar] [CrossRef] [Green Version]
- Pike, K.C.; Griffiths, L.J.; Dezateux, C.; Pearce, A. Physical activity among children with asthma: Cross-sectional analysis in the UK millennium cohort. Pediatr. Pulmonol. 2019, 54, 962–969. [Google Scholar] [CrossRef] [Green Version]
- Eijkemans, M.; Mommers, M.; de Vries, S.I.; van Buuren, S.; Stafleu, A.; Bakker, I.; Thijs, C. Asthmatic symptoms, physical activity, and overweight in young children: A cohort study. Pediatrics 2008, 121, e666–e672. [Google Scholar] [CrossRef]
- Eijkemans, M.; Mommers, M.; Draaisma, J.M.; Thijs, C.; Prins, M.H. Physical activity and asthma: A systematic review and meta-analysis. PLoS ONE 2012, 7, e50775. [Google Scholar] [CrossRef] [Green Version]
- Castro-Rodriguez, J.A.; Garcia-Marcos, L.; Alfonseda Rojas, J.D.; Valverde-Molina, J.; Sanchez-Solis, M. Mediterranean diet as a protective factor for wheezing in preschool children. J. Pediatr. 2008, 152, 823–828.e2. [Google Scholar] [CrossRef]
- Arvaniti, F.; Priftis, K.N.; Papadimitriou, A.; Papadopoulos, M.; Roma, E.; Kapsokefalou, M.; Anthracopoulos, M.B.; Panagiotakos, D.B. Adherence to the Mediterranean type of diet is associated with lower prevalence of asthma symptoms, among 10-12 years old children: The PANACEA study. Pediatr. Allergy Immunol. 2011, 22, 283–289. [Google Scholar] [CrossRef]
- Alwarith, J.; Kahleova, H.; Crosby, L.; Brooks, A.; Brandon, L.; Levin, S.M.; Barnard, N.D. The role of nutrition in asthma prevention and treatment. Nutr. Rev. 2020, 78, 928–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.H.; Ellwood, P.E.; Asher, M.I. Diet and asthma: Looking back, moving forward. Respir Res 2009, 10, 49. [Google Scholar] [CrossRef] [Green Version]
- Chatzi, L.; Apostolaki, G.; Bibakis, I.; Skypala, I.; Bibaki-Liakou, V.; Tzanakis, N.; Kogevinas, M.; Cullinan, P. Protective effect of fruits, vegetables and the Mediterranean diet on asthma and allergies among children in Crete. Thorax 2007, 62, 677–683. [Google Scholar] [CrossRef] [Green Version]
- Asher, M.I.; Garcia-Marcos, L.; Pearce, N.E.; Strachan, D.P. Trends in worldwide asthma prevalence. Eur. Respir. J. 2020, 56. [Google Scholar] [CrossRef]
- Black, P.N.; Sharpe, S. Dietary fat and asthma: Is there a connection? Eur. Respir. J. 1997, 10, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Ellwood, P.; Asher, M.I.; Bjorksten, B.; Burr, M.; Pearce, N.; Robertson, C.F. Diet and asthma, allergic rhinoconjunctivitis and atopic eczema symptom prevalence: An ecological analysis of the International Study of Asthma and Allergies in Childhood (ISAAC) data. ISAAC Phase One Study Group. Eur. Respir. J. 2001, 17, 436–443. [Google Scholar] [CrossRef] [Green Version]
- Nagel, G.; Linseisen, J. Dietary intake of fatty acids, antioxidants and selected food groups and asthma in adults. Eur. J. Clin. Nutr. 2005, 59, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Sausenthaler, S.; Kompauer, I.; Borte, M.; Herbarth, O.; Schaaf, B.; Berg, A.; Zutavern, A.; Heinrich, J.; Group, L.S. Margarine and butter consumption, eczema and allergic sensitization in children. The LISA birth cohort study. Pediatr. Allergy Immunol. 2006, 17, 85–93. [Google Scholar] [CrossRef]
- Bolte, G.; Frye, C.; Hoelscher, B.; Meyer, I.; Wjst, M.; Heinrich, J. Margarine consumption and allergy in children. Am. J. Respir. Crit. Care Med. 2001, 163, 277–279. [Google Scholar] [CrossRef]
- Poole, J.A.; Barriga, K.; Leung, D.Y.; Hoffman, M.; Eisenbarth, G.S.; Rewers, M.; Norris, J.M. Timing of initial exposure to cereal grains and the risk of wheat allergy. Pediatrics 2006, 117, 2175–2182. [Google Scholar] [CrossRef] [Green Version]
- Rastogi, D.; Canfield, S.M.; Andrade, A.; Isasi, C.R.; Hall, C.B.; Rubinstein, A.; Arens, R. Obesity-associated asthma in children: A distinct entity. Chest 2012, 141, 895–905. [Google Scholar] [CrossRef] [Green Version]
- Rastogi, D.; Holguin, F. Metabolic Dysregulation, Systemic Inflammation, and Pediatric Obesity-related Asthma. Ann. Am. Thorac. Soc. 2017, 14, S363–S367. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Has Your Child Ever Had Wheezing or Whistling in the Chest at Any Time in the Past? | ||
|---|---|---|
| Yes | 834 | 21.7% |
| No | 3002 | 78.3% |
| Has Your Child Had Wheezing or Whistling in the Chest in the Past 12 Months? | ||
| Yes | 356 | 9.3% |
| No | 3480 | 90.7% |
| How Many Attacks of Wheezing Has Your Child Had in the Past 12 Months? | ||
| none | 3598 | 93.8% |
| 1–3 | 183 | 4.8% |
| 4–12 | 42 | 1.1% |
| ≥ 12 | 13 | 0.3% |
| In the Past 12 Months, How Often, on Average, Has Your Child’s Sleep Been Disturbed Due to Wheezing? | ||
| Never woken with wheezing | 3588 | 93.5% |
| Less than one night per week | 162 | 4.2% |
| One or more nights per week | 86 | 2.3% |
| In the Past 12 Months, Has Wheezing Ever Been Severe Enough to Limit Your Child’s Speech to Only One or Two Words at a Time between Breaths? | ||
| Yes | 41 | 1.1% |
| No | 3795 | 98.9% |
| Has Your Child Ever Had Asthma? | ||
| Yes | 290 | 7.6% |
| No | 3546 | 92.4% |
| In the Past 12 Months, Has Your Child’s Chest Sounded Wheezy during or after Exercise? (Physical Education, Running, Walking on Stairs) | ||
| Yes | 227 | 5.9% |
| No | 3609 | 94.1% |
| In the Past 12 Months, Has Your Child Had a Dry Cough at Night Apart from a Cough Associated with a Cold or Chest Infection? | ||
| Yes | 422 | 11% |
| No | 3414 | 89% |
| Has Your Child Had Asthma Diagnosed by a Physician? | ||
| Yes | 248 | 6.5% |
| No | 3588 | 93.5% |
| Type of Asthma | Frequency | Percentage | |
|---|---|---|---|
| Current wheezing (CW) | No | 3480 | 90.7% |
| Yes | 356 | 9.3% | |
| Total | 3836 | 100% | |
| Physician-diagnosed asthma (PDA) | No | 3588 | 93.5% |
| Yes | 248 | 6.5% | |
| Total | 3836 | 100% | |
| Cumulative asthma (CA) | No | 3552 | 87.4% |
| Yes | 484 | 12.6% | |
| Total | 3836 | 100% |
| Severity Indicator | n in CA | % in CA | |
|---|---|---|---|
| In the past 12 months, how often, on average, has your child’s sleep been disturbed due to wheezing? | Never woken with wheezing | 292 | 60.33% |
| Less than one night per week | 119 | 24.59% | |
| One or more nights per week | 73 | 15.01% | |
| In the past 12 months, has wheezing ever been severe enough to limit your child’s speech to only one or two words at a time between breaths? | Yes | 37 | 7.64% |
| No | 447 | 92.36% | |
| In the past 12 months, has your child’s chest sounded wheezy during or after exercise? (physical education, running, walking on stairs) | Yes | 149 | 30.79% |
| No | 335 | 69.21% |
| QID | Atopic Condition: Has Your Child Ever Had…? | n (%) in CA | p-Values | OR | CI | |
|---|---|---|---|---|---|---|
| A1 | any allergic diseases | Yes (n = 1206) | 331 (27.45) | <0.0001 | 6.12 | 4.99–7.55 |
| No (n = 2630) | 153 (5.82) | |||||
| A2 | Eczema | Yes (n = 491) | 86 (17.52) | 0.0005 | 1.57 | 1.21–2.02 |
| No (n = 3345) | 398 (11.90) | |||||
| A3 | food allergy | Yes (n = 242) | 61 (25.21) | <0.0001 | 2.53 | 1.85–3.42 |
| No (n = 3595) | 423 (11.77) | |||||
| A4 | allergic rhinitis | Yes (n = 357) | 124 (34.73) | <0.0001 | 4.61 | 3.61–5.88 |
| No (n = 3479) | 360 (10.35) | |||||
| A5 | Has your child been diagnosed with allergic rhinitis by a physician? | Yes (n = 373) | 149 (39.95) | <0.0001 | 6.21 | 4.90–7.86 |
| No (n = 3463) | 335 (9.67) |
| QID | Lifestyle Factors: Presence or Frequency of Behavioral Risk Factor during the Last 12 Months | n (%) in CA | p-Values | OR | CI | |
|---|---|---|---|---|---|---|
| L1 | Weekly frequency of sport activities? | ≥3 times (n = 1879) | 214 (11.39) | 0.0098 | 0.69 | 0.52–0.92 |
| 1–2 times (n = 1474) | 194 (13.16) | 0.1554 | 0.81 | 0.61–1.09 | ||
| Never or occasionally (n = 483) | 76 (15.73) | |||||
| L2 | Average time per week spent on watching TV and / or computer | ≥3 h (n = 1948) | 259 (13.30) | 0.0965 | 1.39 | 0.96–2.08 |
| 1–3 h (n = 1501) | 185 (12.33) | 0.2312 | 1.27 | 0.87–1.92 | ||
| <1 h (n = 322) | 32 (9.94) | |||||
| None responders (n = 65) | 8 (12.31) | |||||
| L3 | The child smokes occasionally or frequently | Yes (n = 4) | 1 (25.00) | 0.4687 | 2.31 | 0.11–18.10 |
| No (n = 3832) | 483 (12.60) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molnár, D.; Gálffy, G.; Horváth, A.; Tomisa, G.; Katona, G.; Hirschberg, A.; Mezei, G.; Sultész, M. Prevalence of Asthma and Its Associating Environmental Factors among 6–12-Year-Old Schoolchildren in a Metropolitan Environment—A Cross-Sectional, Questionnaire-Based Study. Int. J. Environ. Res. Public Health 2021, 18, 13403. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413403
Molnár D, Gálffy G, Horváth A, Tomisa G, Katona G, Hirschberg A, Mezei G, Sultész M. Prevalence of Asthma and Its Associating Environmental Factors among 6–12-Year-Old Schoolchildren in a Metropolitan Environment—A Cross-Sectional, Questionnaire-Based Study. International Journal of Environmental Research and Public Health. 2021; 18(24):13403. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413403
Chicago/Turabian StyleMolnár, Dávid, Gabriella Gálffy, Alpár Horváth, Gábor Tomisa, Gábor Katona, Andor Hirschberg, Györgyi Mezei, and Monika Sultész. 2021. "Prevalence of Asthma and Its Associating Environmental Factors among 6–12-Year-Old Schoolchildren in a Metropolitan Environment—A Cross-Sectional, Questionnaire-Based Study" International Journal of Environmental Research and Public Health 18, no. 24: 13403. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413403