
Effect of Public Empathy with Infection-Control Guidelines on Infection-Prevention Attitudes and Behaviors: Based on the Case of COVID-19




Abstract
:1. Introduction
2. Literature Review and Hypothesis Development
2.1. Types of COVID-19 Damage
2.2. Factors Influencing COVID-19 Infection-Prevention Behaviors
2.2.1. Perceived Susceptibility, Perceived Severity, and Behaviors
2.2.2. Perceived Susceptibility, Perceived Severity, and Attitudes
2.2.3. Attitude and Behavior
2.3. Social Empathy
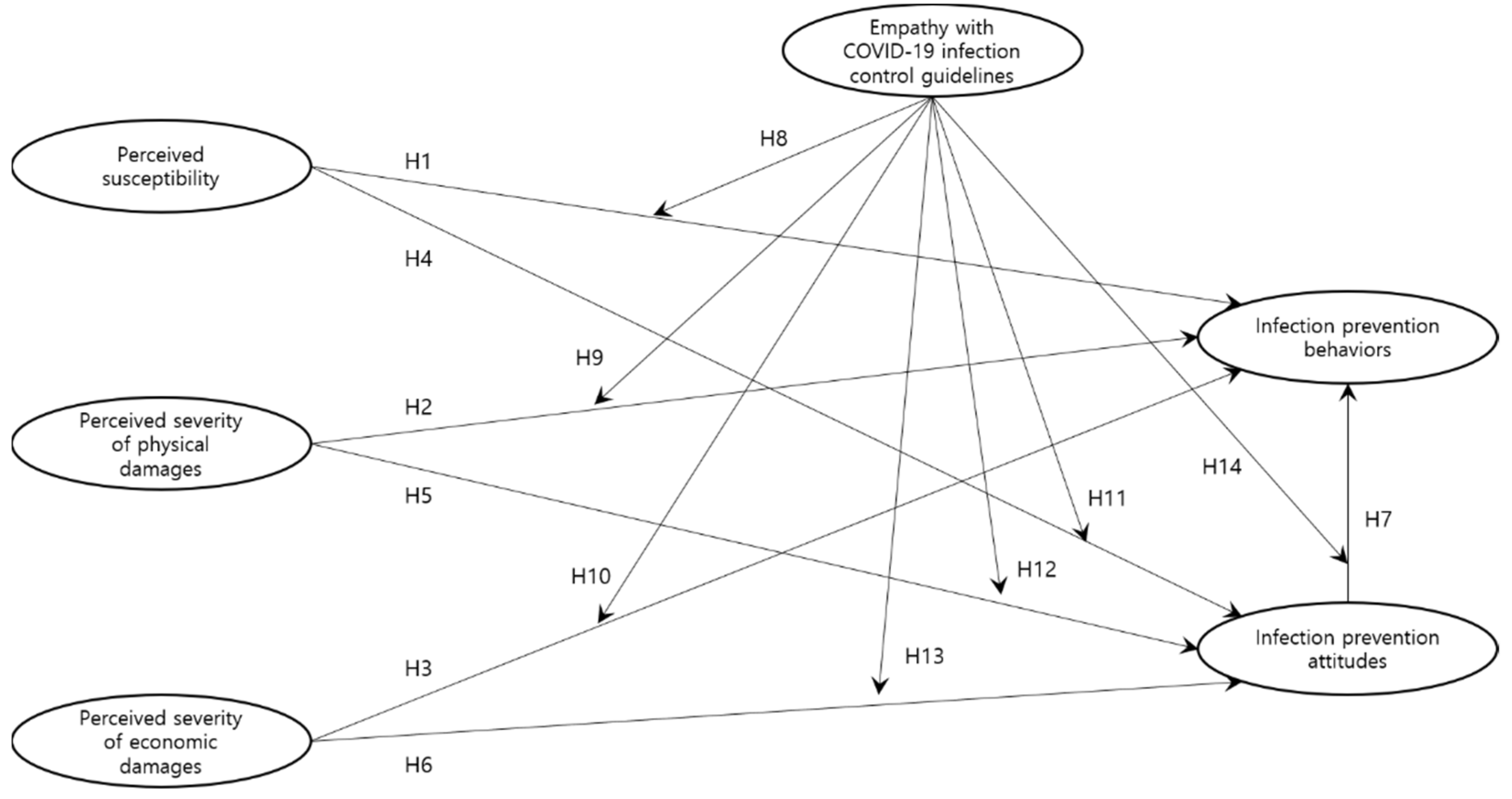
2.4. Conceptual Model
3. Materials and Methods
3.1. Data Collection
3.2. Measures
3.2.1. Perceived Susceptibility
3.2.2. Perceived Severity
3.2.3. COVID-19 Infection-Prevention Attitudes
3.2.4. COVID-19 Infection-Prevention Behaviors
3.2.5. Empathy with COVID-19 Infection-Control Guidelines
3.2.6. Statistical Analysis
4. Results
4.1. Sample
4.2. Measurement Model
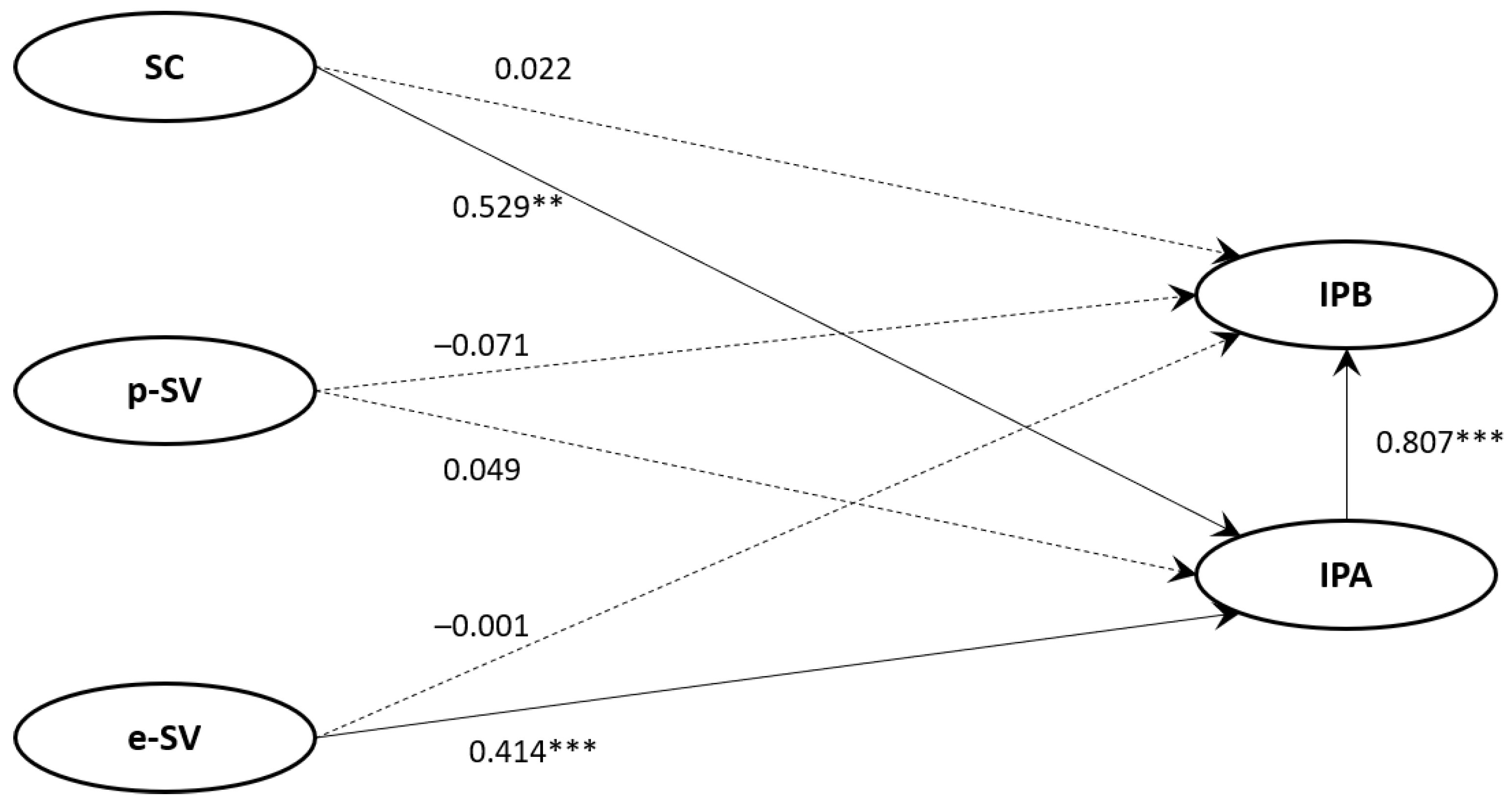
4.3. Structural Model 1
4.4. Groups Categorized by the Public’s Empathy with COVID-19 Infection-Control Guidelines
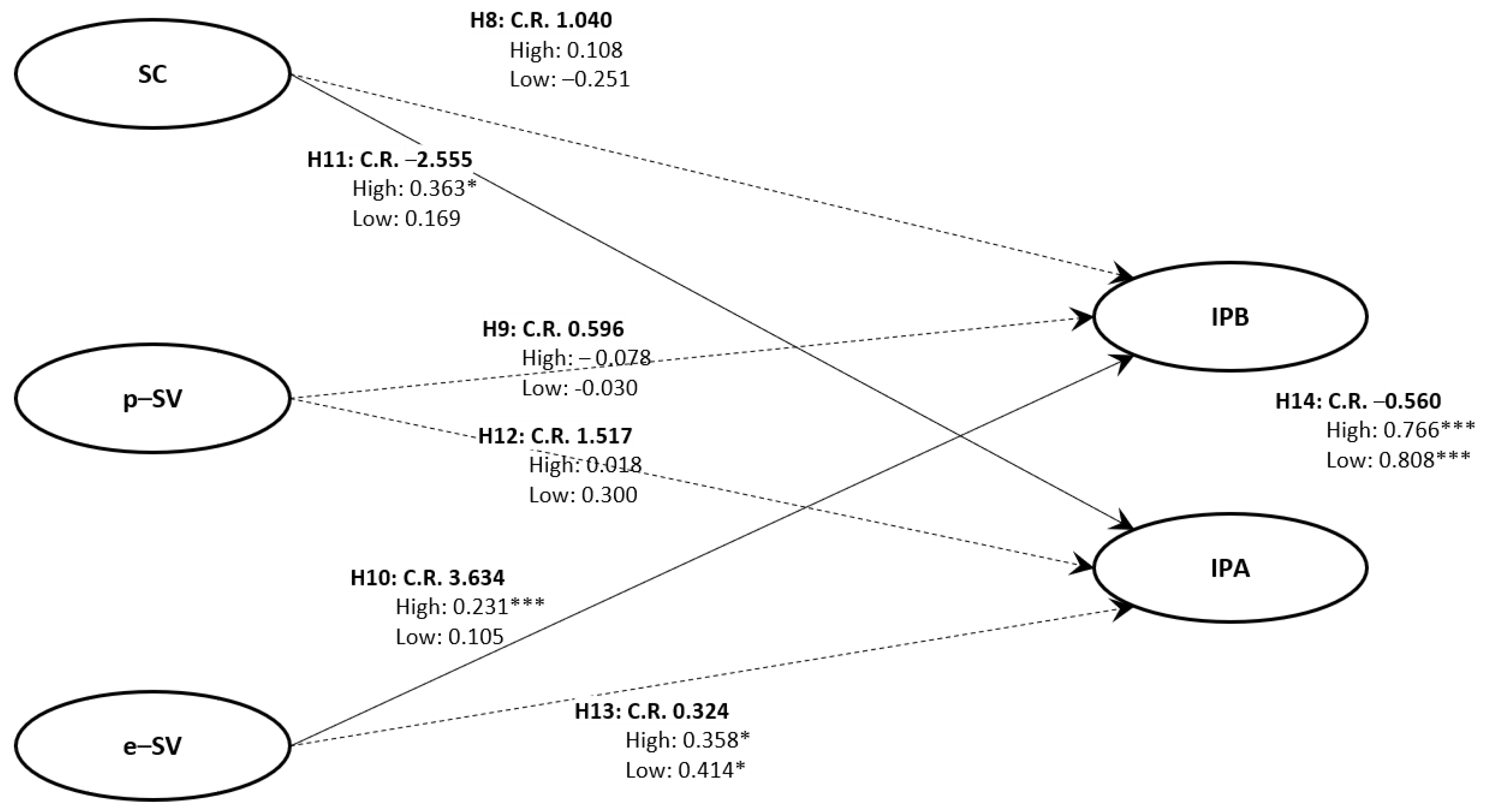
4.5. Structural Model 2
5. Discussion
6. Conclusions
7. Strengths and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A New Coronavirus Associated with Human Respiratory Disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A Pneumonia Outbreak Associated with a New Coronavirus of Probable Bat Origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johns Hopkins CSSE. COVID-19 Dashboard by the Center for System Science and Engineering (CSSE) at Johns Hopkins University (JHU), Coronavirus COVID-19. nCoV. 2019. Available online: Arcgis.com (accessed on 1 September 2021).
- National Institute for Health and Care Excellence(NICE); Scottish Intercollegiate Guidelines Network(SIGN); Royal College of General Practitioners(RCGP). COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19; NICE, SIGN, and RCGP; 2021. Available online: https://www.nice.org.uk/guidance/ng188 (accessed on 18 December 2021).
- Iacobucci, G. Long COVID: Damage to Multiple Organs Presents in Young, Low Risk Patients. BMJ 2020, 371. [Google Scholar] [CrossRef]
- Mossa-Basha, M.; Medverd, J.; Linnau, K.F.; Lynch, J.B.; Wener, M.H.; Kicska, G.; Staiger, T.; Sahani, D.V. Policies and Guidelines for COVID-19 Preparedness: Experiences from the University of Washington. Radiology 2020, 296, E26–E31. [Google Scholar] [CrossRef] [PubMed]
- Carlucci, L.; D’Ambrosio, I.; Balsamo, M. Demographic and Attitudinal Factors of Adherence to Quarantine Guidelines During COVID-19: The Italian Model. Front. Psychol. 2020, 11, 559288. [Google Scholar] [CrossRef]
- Park, C.L.; Russell, B.S.; Fendrich, M.; Finkelstein-Fox, L.; Hutchison, M.; Becker, J. Americans’ COVID-19 Stress, Coping, and Adherence to CDC Guidelines. J. Gen. Intern. Med. 2020, 35, 2296–2303. [Google Scholar] [CrossRef]
- Wolff, W.; Martarelli, C.S.; Schüler, J.; Bieleke, M. High Boredom Proneness and Low Trait Self-Control Impair Adherence to Social Distancing Guidelines During the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 5420. [Google Scholar] [CrossRef]
- Mehanna, A.; Elhadi, Y.A.M.; Lucero-Prisno, D.E. Public Adherence to Precautionary Measures and Preventive Guidelines Against COVID-19 in Sudan: An Application of the Health Belief Model. medRxiv 2021. [Google Scholar] [CrossRef]
- Alsahafi, A.J.; Cheng, A.C. Knowledge, Attitudes and Behaviours of Healthcare Workers in the Kingdom of Saudi Arabia to MERS Coronavirus and Other Emerging Infectious Diseases. Int. J. Environ. Res. Public Health 2016, 13, 1214. [Google Scholar] [CrossRef] [Green Version]
- Asaad, A.; El-Sokkary, R.; Alzamanan, M.; El-Shafei, M. Knowledge and Attitudes towards Middle East Respiratory Sydrome-Coronavirus (MERS-CoV) among Health Care Workers in South-Western Saudi Arabia. East. Mediterr. Health J. 2020, 26, 435–442. [Google Scholar] [CrossRef]
- Alanzi, M.E.; Albalawi, M.A.H.; Kabrah, S.; Aljehani, Y.T.; Okashah, A.M.; Aljohani, Z.D.E.; El Sayed, S. Knowledge, Attitudes, and Practices (KAPs) of Healthcare Workers towards MERS-CoV Infection at PHCs in Madinah, KSA during Hajj 1440, 2019. Am. J. Microbiol. Res. 2019, 7, 122–129. [Google Scholar]
- Chang, S.J.; Park, J. Knowledge, Attitudes and Compliance Regarding Infection Preventive Behaviors for MERS Among Staff in Long-Term Care Hospitals. J. Korea Acad.-Ind. Coop. Soc. 2018, 19, 334–344. [Google Scholar]
- Albarrak, A.I.; Mohammed, R.; Al Elayan, A.; Al Fawaz, F.; Al Masry, M.; Al Shammari, M.; Miaygil, S.B. Middle East Respiratory Syndrome (MERS): Comparing the Knowledge, Attitude and Practices of Different Health Care Workers. J. Infect Public Health 2021, 14, 89–96. [Google Scholar] [CrossRef]
- Aldrees, T.; Al Ghobain, M.; Alenezi, A.; Alqaryan, S.; Aldabeeb, D.; Alotaibi, N.; Alharethy, S. Medical Residents’ Attitudes and Emotions Related to Middle East Respiratory Syndrome in Saudi Arabia: A Cross-Sectional Study. Saudi Med. J. 2017, 38, 942. [Google Scholar] [CrossRef]
- Papagiannis, D.; Malli, F.; Raptis, D.G.; Papathanasiou, I.V.; Fradelos, E.C.; Daniil, Z.; Gourgoulianis, K.I. Assessment of Knowledge, Attitudes, and Practices owards New Coronavirus (SARS-Cov-2) of Health Care Professionals in Greece before the Outbreak Period. Int. J. Environ. Res. Public Health 2020, 17, 4925. [Google Scholar] [CrossRef]
- Di Gennaro, F.; Murri, R.; Segala, F.V.; Cerruti, L.; Abdulle, A.; Saracino, A.; Fantoni, M. Attitudes Towards Anti-SARS-CoV2 Vaccination Among Healthcare Workers: Results from a National Survey in Italy. Viruses 2021, 13, 371. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.F.; Olowokure, B.; Kaydos-Daniels, S.C.; Chang, H.J.; Barwick, R.S.; Lee, M.L.; Team, T.S.I.F. Severe Acute Respiratory Syndrome (SARS): Knowledge, Attitudes, Practices and Sources of Information Among Physicians Answering a SARS Fever Hotline Service. Public Health 2006, 120, 15–19. [Google Scholar] [CrossRef]
- Riccò, M.; Ferraro, P.; Gualerzi, G.; Ranzieri, S.; Bragazzi, N.L.; Balzarini, F.; Signorelli, C. Point-of-Care Diagnostic of SARS-Cov-2: Knowledge, Attitudes, and Perceptions (KAP) of Medical Workforce in Italy. Acta Bio Medica Atenei Parmensis 2020, 91, 57. [Google Scholar]
- Kim, M.J. The Convergence Study of Nursing Students’ Knowledge, Attitudes and Preventive Behaviors Against MERS in South Korea. J. Korea Converg. Soc. 2017, 8, 149–157. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.L.; Yoo, Y.G. Correlation between Knowledge, Attitudes and Preventive Behaviors Regarding the MERS of a Student in the Department of Emergency Medical Technology. J. Korea Acad.-Ind. Coop. Soc. 2020, 21, 401–408. [Google Scholar]
- Lee, S.-E.; Lee, N.; Yoo, S.; Park, D.-H.; Jeon, K.; Hwang, T.-Y.; Lee, J.H. A Survey on the Public Perceptions of Disaster-Related Mental Health Service. J. Korean Neuropsychiatr. Assoc. 2021, 60, 53–60. [Google Scholar] [CrossRef]
- Lee, D.Y.; Na, J.H.; Sim, M.Y. Psychological Reactions and Physical Trauma by Types of Disasters: View from Man-Made Disaster. J. Korean Neuropsychiatr. Assoc. 2015, 54, 261–268. [Google Scholar] [CrossRef]
- Lee, J.; Kim, D. Variation of Vulnerability and Post-Traumatic Stress Disorder of Residents Due to Oil Spill Accident of Hebei Spirit: Analysis of Panel Data After the Accident in Sep 2008 and Oct 2010; The Korean Association for Environmental Sociology. Korea J. Encironmental Sociol. 2011, 15, 269–298. [Google Scholar]
- World Health Organization. What Are the Symptoms of COVID-19? World Health Organization Newsroom. 2021. Available online: https://www.who.int/news-room/q-a-detail/coronovirus-disease-covid-19 (accessed on 27 August 2021).
- Lopez, A.; Caffò, A.O.; Tinella, L.; Masi, M.N.D.; Bosco, A. Variations in Mindfulness Associated with the COVID-19 Outbreak: Differential Effects on Cognitive Failures, Intrusive Thoughts and Rumination. Health Well-Being 2021, 13, 761–780. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Situation by Region, Country, Territory and Area, WHO Coronavirus (COVID-19) Dashboard. 2021. Available online: https://covid19.who.int/table (accessed on 27 August 2021).
- Bank of Korea. Effect of COVID–19 on Household Income Inequality; BOK Issue Note; Bank of Korea: Seoul, Korea, 2021; Volume 9. [Google Scholar]
- Jang, Y. Finding the Balance Between COVID-19 Risk and Social Damages. Welf. Trends. 2021, 272, 5–13. [Google Scholar]
- Kim, J.; Kim, J. The Analysis of Correlation Between COVID-19 and Seoul Small Business Commercial Districts. J. Korea Inst. Inf. Commun. Eng. 2021, 25, 384–388. [Google Scholar]
- Becker, M.H. The Health Belief Model and Sick Role Behavior. Health Educ. Monogr. 1974, 2, 409–419. [Google Scholar] [CrossRef]
- Becker, M.H.; Maiman, L.A. Sociobehavioral Determinants of Compliance with Health and Medical Care Recommendations. Med. Care. 1975, 13, 10–24. [Google Scholar] [CrossRef]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. The Health Belief Model and HIV Risk Behavior Change, Preventing AIDS; Springer Book Archive: Berlin/Heidelberg, Germany, 1994. [Google Scholar]
- Rosenstock, I.M. Historical Origin of the Health Belief Model. In The Health Belief Model and Personal Health Behavior; Thorofare, B.M.H., Ed.; Charles B. Slack, Incorp: Medina, NJ, USA, 1974; pp. 1–8. [Google Scholar]
- Becker, M.H.; Maiman, L.A. Strategies for Enhancing Patient Compliance. J. Community Health 1980, 6, 113–135. [Google Scholar] [CrossRef]
- Ajzen, I.; Fishbein, M. Understanding Attitudes and Predicting Social Behavior; Prentice Hall: Englewood Cliffs, NJ, USA, 1980. [Google Scholar]
- Rogers, R.W. A Protection Motivation Theory of Fear Appeals and Attitude Change. J. Psychol. 1975, 91, 93–114. [Google Scholar] [CrossRef]
- Rogers, R.W. Cognitive and Psychological Processes in Fear Appeals and Attitude Change: A Revised Theory of Protection Motivation. In Social Psychophysiology: A Sourcebook; Cacioppo, J.T., Petty, R.E., Eds.; Guilford Press: New York, NY, USA, 1983; pp. 153–176. [Google Scholar]
- Witte, K. Putting the Fear Back into Fear Appeals: The Extended Parallel Process Model. Commun. Monogr. 1992, 59, 329–349. [Google Scholar] [CrossRef]
- Witte, K. Fear Control and Danger Control: A Test of the Extended Parallel Process Model (EPPM). Commun. Monogr. 1994, 61, 113–134. [Google Scholar] [CrossRef]
- Rimal, R.N.; Real, K. Understanding the Influence of Perceived Norms on Behaviors. Commun. Theor. 2003, 13, 184–203. [Google Scholar] [CrossRef]
- Rimal, R.N.; Juon, H. Use of the Risk Perception Attitude Framework for Promoting Breast Cancer Prevention. J. Appl. Soc. Psychol. 2010, 40, 287–310. [Google Scholar] [CrossRef]
- Iachini, T.; Frassinetti, F.; Ruotolo, F.; Sbordone, F.L.; Ferrara, A.; Arioli, M.; Pazzaglia, F.; Bosco, A.; Candini, M.; Lopez, A.; et al. Social Distance during the COVID-19 Pandemic Effects Perceived Rather Than Actual Risk. Int. J. Environ. Res. Public Health 2021, 18, 5504. [Google Scholar] [CrossRef]
- Kim, S.; Kim, S. Analysis of the Impact of Health Beliefs and Resource Factors on Preventive Behaviors Against the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8666. [Google Scholar] [CrossRef]
- Liau, A.; Zimet, G.D. Undergraduates’ Perception of HIV Immunization: Attitudes and Behaviours as Determining Factors. Int. J. STD AIDS. 2000, 11, 445–450. [Google Scholar] [CrossRef]
- Xu, H.; Gan, Y.; Zheng, D.; Wu, B.; Zhu, X.; Xu, C.; Liu, C.; Tao, Z.; Hu, Y.; Chen, M.; et al. Relationship between COVID-19 Infection and Risk Perception, Knowledge, Attitude, and Four Nonpharmaceutical Interventions During the Late Period of the COVID-19 Epidemic in China: Online Cross-Sectional Survey of 8158 Adults. J. Med. Internet Res. 2020, 22, e21372. [Google Scholar] [CrossRef]
- Jo, S.E.; Shin, H.C.; Yoo, S.; Roh, H. The Study of Factors Affecting Tuberculosis Preventive Behavior Intentions: An Extension of HBM with Mediating Effects of Self-Efficacy and Fear. Korean Acad. Soc. Public Relat. 2012, 16, 148–177. [Google Scholar] [CrossRef]
- Bin, S.O. Structural Relationships of Knowledge, Perception, Attitude and Preventive Behavior for Communicable Diseases. J. Health Inform. Stat. 2012, 37, 57–71. [Google Scholar]
- Ji, Y.; Moon, Y.M. Factors Affecting Potential Disaster Damage and Perceptible Stress Influencing Evacuation Behavior. J. Soc. Disaster Inf. 2020, 16, 594–601. [Google Scholar]
- Floyd, D.L.; Prentice-Dunn, S.; Rogers, R.W. A Meta-Analysis of Research on Protection Motivation Theory. J. Appl. Soc. Psychol. 2000, 30, 407–429. [Google Scholar] [CrossRef]
- Witte, K.; Allen, M. A Meta-Analysis of Fear Appeals: Implications for Effective Public Health Campaigns. Health Educ. Behav. 2000, 27, 591–615. [Google Scholar] [CrossRef]
- Brug, J.; Aro, A.R.; Richardus, J.H. Risk Perceptions and Behaviour: Towards Pandemic Control of Emerging Infectious Diseases: International Research on Risk Perception in the Control of Emerging Infectious Diseases. Int. J. Behav. Med. 2009, 16, 3–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajzen, I. From Intentions to Actions: A Theory of Planned Behavior. In Action Control; Kuhl, J., Berlin, B.J., Eds.; Springer: Berlin/Heidelberg, Germany, 1985; pp. 11–39. [Google Scholar]
- Quintal, V.A.; Lee, J.A.; Soutar, G.N. Risk, Uncertainty and the Theory of Planned Behavior: A Tourism Example. Tour. Manag. 2010, 31, 797–805. [Google Scholar] [CrossRef]
- Burns, W.J.; Slovic, P. Risk Perception and Behaviors: Anticipating and Responding to Crises. Risk Anal. 2012, 32, 579–582. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.Y.; Chang, P. The Effect of Coronavirus Disease-19 (COVID-19) Risk Perception on Behavioural Intention towards ‘Untact’ Tourism in South Korea During the First Wave of the Pandemic (March 2020). Curr. Issues Tour. 2021, 24, 1017–1035. [Google Scholar] [CrossRef]
- Yang, M. Knowledge, Attitude, Perception, and Performance About Tuberculosis Infection Control Among Nurses in Departments at High Risk of Tuberculosis in General Hospitals. Master’s Thesis, Yonsei University, Seoul, Korea, 2014. [Google Scholar]
- Kim, S.S. A Study on Consumer’s Attitude for Food Safety and Purchase of Environment Friendly Agricultural Products. J. Fam. Better Life 2007, 25, 15–32. [Google Scholar]
- Ajzen, I. The Theory of Planned Behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Williams, R.M. Change and Stability in Value and Value Systems: A Sociological Perspective, Understanding Human Values: Individual and Societal; Free Press: New York, NY, USA, 1979. [Google Scholar]
- Fishbein, M.; Ajzen, I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research; Addison-Wesley: Reading, MA, USA, 1975. [Google Scholar]
- Ajzen, I. Attitudes, Personality, and Behavior; Dorsey: Chicago, IL, USA, 1988. [Google Scholar]
- Jo, S.E.; Yoo, S. A Study on the Effects of Risk Perception Attitudes and Subjective Norm on the Preventive Behaviors of Cervical Cancer-Testing RPA Framework on Korean College Women. J. Public Relat. Res. 2011, 15, 58–98. [Google Scholar] [CrossRef]
- Kang, J.S.; Yang, I. Influencing Factors of Tuberculosis Preventive Behavioral Intention. Korean Soc. Living Environ. Syst. 2014, 21, 444–452. [Google Scholar] [CrossRef]
- Kumar, R.; Singh, V.; Mohanty, A.; Bahurupi, Y.; Gupta, P.K. Corona Health-Care Warriors in India: Knowledge, Attitude, and Practices during COVID-19 Outbreak. J. Educ. Health Promot. 2021, 10, 44. [Google Scholar] [CrossRef]
- Chan, E.Y.Y.; Huang, Z.; Lo, E.S.K.; Hung, K.K.C.; Wong, E.L.Y.; Wong, S.Y.S. Sociodemographic Predictors of Health Risk Perception, Attitude and Behavior Practices Associated with Health-Emergency Disaster Risk Management for Biological Hazards: The Case of COVID-19 Pandemic in Hong Kong, SAR China. Int. J. Environ. Res. Public Health 2020, 17, 3869. [Google Scholar] [CrossRef]
- Erfani, A.; Shahriarirad, R.; Ranjbar, K.; Mirahmadizadeh, A.; Moghadami, M. Knowledge, Attitude, and Practice Toward the Novel Coronavirus Outbreak: A Population-Based Survey in Iran. Bull. World Health Organ. 2020, 30. [Google Scholar] [CrossRef]
- Puspitasari, I.M.; Yusuf, L.; Sinuraya, R.K.; Abdulah, R.; Koyama, H. Knowledge, Attitude, and Practice During the COVID-19 Pandemic: A Review. J. Multidiscip. Healthc. 2020, 13, 727–733. [Google Scholar] [CrossRef]
- Im, T.; Jung, H.-J.; Kang, E.-Y. The Effects of Policy Understanding on the Perception of Policy Performance by the General Public. Korean Gov. Rev. 2012, 19, 1–29. [Google Scholar]
- Lee, K.; Mok, J. The Determinant Analysis on the Public Acceptance of the Korean Nuclear Power Policy. J. Gov. Stud. 2016, 11, 55–84. [Google Scholar] [CrossRef]
- Kang, Y.J.; Kim, J.Y.; Park, J.H.; Lee, Y.H.; Chung, I.K. The State of Scientific Citizenship in Korea: Centered on the Analysis of the Citizens Perception Survey on the Science and Technology. Korean Assoc. Sci. Technol. Stud. 2015, 15, 3–43. [Google Scholar]
- Putnam, R.D. The Prosperous Community. Am. Prospect. 1993, 4, 1–11. [Google Scholar]
- Putnam, R.D. Bowling Alone: America’s Declining Social Capital. J. Democr. 1995, 6, 65–78. [Google Scholar] [CrossRef] [Green Version]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; Van Der Bles, A.M.V.D.; Spiegelhalter, D.; Van Der Linden, S. Risk Perceptions of COVID-19 Around the World. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Park, C.C.; Cho, H.; Lee, D.G.; Jeon, H. Latent profile Analysis on Korean Nurses: Emotional Labour Strategies and Well-Being. J. Adv. Nurs. 2021, 1–10. [Google Scholar] [CrossRef]
- Jong, J.; Halberstadt, J.; Bluemke, M.; Kavanagh, C.; Jackson, C. Death Anxiety, Exposure to Death, Mortuary Preferences, and Religiosity in Five Countries. Sci. Data 2019, 6, 1–5. [Google Scholar] [CrossRef]
- Rezaei, M.; Kim, D.; Alizadeh, A.; Rokni, L. Evaluating the Mental-Health Positive Impacts of Agritourism; A Case Study from South Korea. Sustainability 2021, 13, 8712. [Google Scholar] [CrossRef]
- Yıldırım, M.; Güler, A. Factor Analysis of the COVID-19 Perceived Risk Scale: A Preliminary Study. Death Stud. 2020, 1–8. [Google Scholar] [CrossRef]
- Central Disaster Management Headquarters; Central Disease Control Headquarters. Knowing the Coronavirus Infection. Available online: http://ncov.mohw.go.kr/ (accessed on 6 September 2021).
- Lee, M.; You, M. Psychological and Behavioral Responses in South Korea during the Early Stages of Coronavirus Disease 2019 (COVID-19). Int. J. Environ. Res. Public Health 2020, 17, 2977. [Google Scholar] [CrossRef]
- Galea, S.; Merchant, R.M.; Lurie, N. The Mental Health Consequences of COVID-19 and Physical Distancing: The Need for Prevention and Early Intervention. JAMA Intern. Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [Green Version]
- Smith, G.D.; Ng, F.; Ho Cheung Li, W.H.C. COVID-19: Emerging Compassion, Courage and Resilience in the Face of Misinformation and Adversity. J. Clin. Nurs. 2020, 29, 1425–1428. [Google Scholar] [CrossRef] [Green Version]
- Song, E.; Yoo, H.J. Impact of Social Support and Social Trust on Public Viral Risk Response: A COVID-19 Survey Study. Int. J. Environ. Res. Public Health 2020, 17, 6589. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.J.; Song, E. Effects of Personal Hygiene Habits on Self-Efficacy for Preventing Infection, Infection-Preventing Hygiene Behaviors, and Product-Purchasing Behaviors. Sustainability 2021, 13, 9483. [Google Scholar] [CrossRef]
- Joreskog, K.G.; Sorbom, D. LISREL 8: Structural Equation Modelling with the SIMPLIS Command Language; Scientific Publishing Software International: Chicago, IL, USA, 1996. [Google Scholar]
- Byrne, B.M. Structural Equation Modelling with AMOS: Basic Concepts, Applications and Programming; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2001. [Google Scholar]
- Tobbin, P. Adoption of Mobile Money Transfer Technology: Structural Equation Modeling Approach. Eur. J. Bus. Manag. 2011, 3, 59–77. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating Structural Equation Models with Unobservable Variables and Measurement Error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Nunnally, J.C. Psychometric Theory; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Chen, J.; Lan, Y.C.; Chang, Y.W.; Chang, P.Y. Exploring Doctors’ Willingness to Provide Online Counseling Services: The Roles of Motivations and Costs. Int. J. Environ. Res. Public Health 2019, 17, 110. [Google Scholar] [CrossRef] [Green Version]
- Woo, J.P. Professor Woo Jong Pil’s Concept of Structure Equation Model; Hanahara Publishing, Co.: Seoul, Korea, 2013. [Google Scholar]
- Dong-A Ilbo. Medical Tourism Stopped Due to COVID-19 Now Led by Seongnam and Pushed by Companies. Available online: https://www.donga.com/news/article/all/20210909/109179057/1 (accessed on 10 September 2021).
- Incheon Ilbo. Calls for Stricter Infection Control Protocol Against Smoking in Buildings. 2021. Available online: http://www.incheonilbo.com/news/articleView.html?idxno=1108441 (accessed on 10 September 2021).
- Newsis. No Violation yet for Gathering Limit of 6 People in Seoul. 2021. Available online: https://newsis.com/view/?id=NISX20210907_0001574819&cID=10201&pID=10200 (accessed on 10 September 2021).
- Albassam, A.A.; Iqbal, M.Z.; Al-Saikhan, F.I.; Khan, S.U.D.; Iqbal, M.S. Attitude of Future Healthcare Professionals towards Ebola Virus Disease. Med. Sci. 2020, 24, 3901–3910. [Google Scholar]
- Etokidem, A.J.; Ago, B.U.; Mgbekem, M.; Etim, A.; Usoroh, E.; Isika, A. Ebola Virus Disease: Assessment of Knowledge, Attitude and Practice of Nursing Students of a Nigerian University. Afr. Health Sci. 2018, 18, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Narasimhulu, D.M.; Edwards, V.; Chazotte, C.; Bhatt, D.; Weedon, J.; Minkoff, H. Healthcare Workers’ Attitudes toward Patients with Ebola Virus Disease in the United States. In Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2018; Volume 3, pp. 1–7. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Construct 1: Perceived susceptibility (SC) SC 1: I think it might be possible that I get infected with COVID-19. SC 2: I think it might be possible that my family members get infected with COVID-19. |
| Construct 2: Perceived severity of physical damage (p-SV) p-SV 1: I think the spread of COVID-19 increases the extent of physical damage. p-SV 2: I think the development of COVID-19 increases the extent of physical damage. |
| Construct 3: Perceived severity of economic damage (e-SV) e-SV 1: I think COVID-19 has a negative impact on my local economy. e-SV 2: I think COVID-19 has a negative impact on other local economies. |
| Construct 4: COVID-19 infection-prevention attitude (IPA) IPA 1: I think I should follow infection-control guidelines despite inconveniences. IPA 2: I think I should follow infection-control guidelines despite personal costs. IPA 3: I think I should follow infection-control guidelines with a sense of social responsibility. |
| Construct 5: COVID-19 infection-prevention behavior (IPB) IPB 1: I am practicing social distancing to prevent COVID-19 infection. IPB 2: I always wear a mask to prevent COVID-19 infection. IPB 3: I frequently wash my hands to prevent COVID-19 infection. |
| Construct 6: Public empathy with COVID-19 infection-control guidelines (RE) RE 1: I empathize (agree) with social distancing guidelines to prevent COVID-19 infections. RE 2: I empathize (agree) with masking guidelines to prevent COVID-19 infections. RE 3: I empathize (agree) with delaying the opening of schools to prevent COVID-19 infections. RE 4: I empathize (agree) with requiring COVID-19 tests to prevent COVID-19 infections. RE 5: I empathize (agree) with sharing information to prevent COVID-19 infections. |
| Characteristics | Frequency | Percentage | |
|---|---|---|---|
| Gender | Male | 107 | 50.7 |
| Female | 104 | 49.3 | |
| Age | 20s | 52 | 24.6 |
| 30s | 54 | 25.6 | |
| 40s | 54 | 25.6 | |
| 50s and older | 51 | 24.2 | |
| Place of residence | Seoul metropolitan area | 135 | 64.0 |
| Chungcheong and Gangwon region | 23 | 10.9 | |
| Gyeongsang region | 42 | 19.9 | |
| Jeolla region | 11 | 5.2 | |
| Educational background | High school graduation or lower | 31 | 14.7 |
| Junior college graduation | 28 | 13.3 | |
| 4-year university graduation | 127 | 60.2 | |
| Graduate school graduation | 25 | 11.8 | |
| Type of employment | Regular worker | 111 | 52.6 |
| Part-time worker | 13 | 6.2 | |
| Freelancer | 6 | 2.8 | |
| Housewife, student, and others | 81 | 38.4 | |
| Average monthly household income * | <2 million won | 22 | 10.5 |
| ≥2 million won to <3 million won | 43 | 20.4 | |
| ≥3 million won to <4 million won | 37 | 17.5 | |
| ≥4 million won to <5 million won | 39 | 18.5 | |
| ≥5 million won | 70 | 33.2 | |
| Construct | Measures | Standardized Estimate | Cronbach’s α | CR | AVE | Inter-Construct Correlations | Mean (SD) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SC | p-SV | e-SV | IPA | IPB | PE | |||||||
| Perceived susceptibility | SC1 | 0.736 | 0.942 | 0.947 | 0.900 | 0.949 | 3.730 (0.569) | |||||
| SC2 | 0.622 | |||||||||||
| Perceived severity of physical damage | p-SV1 | 0.959 | 0.856 | 0.999 | 0.998 | 0.392 | 0.999 | 2.936 (0.763) | ||||
| p-SV2 | 0.780 | |||||||||||
| Perceived severity of economic damage | e-SV1 | 0.877 | 0.778 | 0.987 | 0.975 | 0.505 | 0.046 | 0.987 | 3.780 (0.793) | |||
| e-SV2 | 0.689 | |||||||||||
| Infection-prevention attitude | IPA1 | 0.893 | 0.929 | 0.999 | 0.996 | 0.503 | 0.131 | 0.527 | 0.998 | 4.321 (0.701) | ||
| IPA2 | 0.912 | |||||||||||
| IPA3 | 0.905 | |||||||||||
| Infection-prevention behavior | IPB1 | 0.791 | 0.814 | 0.978 | 0.939 | 0.42 | 0.055 | 0.419 | 0.820 | 0.969 | 4.409 (0.594) | |
| IPB2 | 0.909 | |||||||||||
| IPB3 | 0.852 | |||||||||||
| Infection-control guidelines Public empathy | RE1 | 0.840 | 0.788 | 0.998 | 0.988 | 0.369 | 0.041 | 0.509 | 0.696 | 0.655 | 0.994 | 4.002 (0.576) |
| RE2 | 0.773 | |||||||||||
| RE3 | 0.696 | |||||||||||
| RE4 | 0.744 | |||||||||||
| RE5 | 0.612 | |||||||||||
| Construct | Mean | Standard Deviation | Empathy Group | Mean | Standard Deviation | T-Value |
|---|---|---|---|---|---|---|
| Perceived susceptibility | 3.730 | 0.569 | High | 3.781 | 0.581 | 1.961 |
| Low | 3.615 | 0.529 | ||||
| Perceived susceptibility Perceived severity of physical damage | 2.936 | 0.763 | High | 2.908 | 0.816 | −0.894 |
| Low | 3.000 | 0.631 | ||||
| Perceived severity of economic damage | 3.780 | 0.793 | High | 3.908 | 0.759 | 3.612 *** |
| Low | 3.492 | 0.798 | ||||
| Infection-prevention attitudes | 4.321 | 0.701 | High | 4.505 | 0.550 | 5.347 *** |
| Low | 3.908 | 0.822 | ||||
| Infection-prevention behaviors | 4.409 | 0.594 | High | 4.564 | 0.479 | 5.396 *** |
| Low | 4.062 | 0.679 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, E.; Lee, J.-E.; Kwon, S. Effect of Public Empathy with Infection-Control Guidelines on Infection-Prevention Attitudes and Behaviors: Based on the Case of COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 13408. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413408
Song E, Lee J-E, Kwon S. Effect of Public Empathy with Infection-Control Guidelines on Infection-Prevention Attitudes and Behaviors: Based on the Case of COVID-19. International Journal of Environmental Research and Public Health. 2021; 18(24):13408. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413408
Chicago/Turabian StyleSong, Eugene, Jae-Eun Lee, and Seola Kwon. 2021. "Effect of Public Empathy with Infection-Control Guidelines on Infection-Prevention Attitudes and Behaviors: Based on the Case of COVID-19" International Journal of Environmental Research and Public Health 18, no. 24: 13408. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413408