
WhatsApp in Clinical Practice—The Challenges of Record Keeping and Storage. A Scoping Review


Abstract
:1. Introduction
2. Methods
3. Results
3.1. Group A. Prescribed Action—Electronic
3.2. Group B. Prescribed Action—Paper Based
3.3. Group C. Prescribed Action—Uncertain Electronic or Paper Based
3.4. Group D. Inaction—ePHI Remains on Mobile Phones
3.5. Group E. Uncertain
4. Discussion
4.1. Retention of Original Messaging
4.2. Long-Term Storage
4.3. Encryption
4.4. Extra-Jurisdictional Record Keeping and Storage
4.5. Consent
4.6. Anonymisation
5. Summary
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CSF-HCP | Cellphone Stewardship Framework for Health Care Providers |
| ePHI | electronic Protected Health Information |
| EHR | Electronic Health Record |
| EMR | Electronic Medical Record |
| EPR | Electronic Patient Record |
| GDPR | General Data Protection Regulation |
| HIPAA | Health Insurance Portability and Accountability Act |
| POPI | Protection of Personal Information Act |
| WMA | World Medical Association |
Appendix A

{kind=link}
{kind=link}
| Paper | Country | Specialty | Overview of Included Studies | Evidence of Records/Storage |
|---|---|---|---|---|
| Group A. Prescribed Action—Electronic | ||||
| den Hollander and Mars. [21] 2017 | South Africa | Burn care. | Referring doctors were required to telephone the burns specialist, answer a referral questionnaire about the case and send photographs of the burn wounds before a decision was made on acceptance of the referral or providing ongoing management advice. The photographs were taken and sent by smartphone using MMS or WhatsApp. The completed questionnaire, with photographs, were entered into a database which was reviewed for the study. | Evidence of record keeping and storage. Reported transfer of data from mobile phones to electronic versions of patient notes or departmental records. Transfer was done manually to a password protected database. Retrospective study from a database where messages and photos were deleted from the consultant’s phone. |
| Joshi et al. [22] 2018 | India | Neurosurgical referral service. | Examined the use of WhatsApp for a neurosurgical referral service. Use of WhatsApp was extended from a purely intra-departmental informal communication to a formal tertiary referral service for Neurosurgical referrals. The pros and cons of deploying such a system were discussed and important concerns highlighted. | Evidence of both record keeping and storage. Reported the transfer of data from mobile phones to electronic versions of patient notes or departmental records. Transfer was done manually to a departmental secure computer. Messages remained on the phone and apparently ‘backed up’, with no explanation of how and no mention of subsequent deletion of messages. A retrospective study where information was accessed from WhatsApp messages stored on the users’ mobile phones. |
| Group B. Prescribed Action—Paper Based | ||||
| Johnston et al. [27] 2015 | UK | Communication in emergency surgical teams. | Evaluated implementation of a WhatsApp messaging service within emergency surgical teams. A prospective mixed-methods study. All emergency surgery team members used WhatsApp for communication for 19 weeks. Examined response times, communication types, and safety events. | Reported on both record keeping and storage. Temporarily stored messages on the phone for 1 week. Downloaded and kept a hard copy record but did not explain how? Benefits were a record of communication for training purposes. |
| Nardo et al. [28] 2016 | Italy | Patient surgical management. | Examined use of WhatsApp between two distant elective surgery teams to verify if WhatsApp improved patient care, while preserving their privacy and enhanced learning. | Reported on both record keeping and storage. Temporarily stored messages on the phone for 1 week before deleting messages off mobile phones. Downloaded and kept a hard copy record, but did not describe how? Applied the same protocol as Johnston et al. |
| Siegal et al. [29] 2016 | Israel | Otolaryngology. | Experience and practices governing the usage of WhatsApp for mobile health purposes in a national cohort of practicing otolaryngologists. | Reported on both record keeping and storage by ‘downloading’ of a hard copy/script for record keeping before deleting data from ‘participant devices’ after a defined period but the method was not described. |
| Group C. Prescribed Action—Uncertain electronic or paper based | ||||
| Wani et al. [31] 2013 | Saudi Arabia | Plastic and reconstructive surgery. | An assessment of the efficacy of smartphone and its WhatsApp application as a communication method amongst the staff of plastic and reconstructive surgery section at tertiary care health facility. WhatsApp was used for various aspects of patient management. | Reported keeping records, but it was not clear from descriptions if this was done electronically or was paper based. The chat conversations were photographed as screenshots for saving in the medical record, but it was not clear if and how the screenshots were stored, but it seems unlikely they were printed as it was reported that WhatsApp conversations could not be printed. |
| Ellanti et al. [32] 2017 | UK | Orthopaedic Surgery. | Analysis of WhatsApp communication between non-consultant members of an orthopaedic team over a six-month period. A specific “orthopaedic group” was created on WhatsApp, which included all the non-consultant orthopaedic team. | Reported only on record keeping. Reported deleting messages off mobile phones after a 6 month period and although no mention was made of formal storage or record keeping this was inferred from the descriptions in the paper. |
| Martinez et al. [35] 2018 | South Africa | Paediatric burn care. | Reviewed use of WhatsApp to facilitate paediatric burn injury consultations to a regional burn centre. A retrospective review of all WhatsApp consultations over an 18 month period. Assessed the impact in terms of reductions in admissions and clinic visits, a cost analysis plus analysis of feedback from those health practitioners regularly using the service. | Evidence of storage only. Reported keeping records, but it was not clear if it was done electronically or was paper based. Reported deleting messages off mobile phones. The importance of record keeping, and storage was noted, but no details were provided on how this was done. |
| Neogi et al. [24] 2020 | India | Interinstitutional patient transfer. | Use of WhatsApp to facilitate transfer of paediatric patients, including neonates, from paediatric department of one hospital (which does not have paediatric surgical support) to a tertiary care hospital. The WhatsApp group included the consultants and residents of the concerned department from both the hospitals. Patient details, investigations were initially uploaded on the group. The case was assessed on the messenger and the transfer coordinated. | Reported on both record keeping and storage but it was not clear if this was done electronically or was paper based. Kept an analogue or digital record, and then periodically deleted messages off mobile phones or gained consent and archived. |
| Group D. Inaction—ePHI remains on mobile phones | ||||
| Gulacti et al. [33] 2016 | Turkey | Communication between consulting and emergency physicians. | Evaluated WhatsApp messenger usage for communication between consulting and emergency physicians. A retrospective, observational study conducted in the emergency department of a tertiary care university hospital. | Reported only on record keeping and that information stored on the users’ mobile phone constituted a medical record. Retrospective study of WhatsApp messages stored on the phone with no mention of subsequent deletion of messages. |
| Sidhoum et al. [34] 2016 | France | Surgical team communication. | Experiences and results over nearly three years of the use of WhatsApp in the plastic surgery team in CHU Amiens. Transmitted patient information included text, photos, and video, with the patient’s agreement to share with other team members. | Reported only on record keeping where information stored on the users’ mobile phone constituted a medical record. Retrospective study of messages stored on the phone with no mention of subsequent deletion of messages. |
| Ganasegeran et al. [5] 2017 | Malaysia | Use in clinical practice. | A preliminary study. Aim was to investigate perceived benefits, if any, of WhatsApp use across general medical and emergency teams during clinical practice. | Reported on both record keeping and storage and that information stored on the users’ mobile phone constituted a medical record. Benefits of this were a record of communication for audit purposes. Mentioned concerns of messages stored on users’ phones. |
| Mars and Scott. [23] 2017 | South Africa | Dermatology and burn management. | Describes two ‘‘spontaneous’’ WhatsApp-based telemedicine services in dermatology and burn management. For dermatology, doctors at rural referring hospitals take photographs of skin lesions and send them to dermatologists together with a brief text message history. For the burns service, admissions now require completion of a preadmission questionnaire and submission of photographs of the burn sent by WhatsApp, with the decision transmitted by text message. | Reported on both record keeping and storage. In the dermatology service, some messages were stored on the consultant’s phone, no central depository. In the burns service: some messages deleted from the phones. |
| Pandian et al. [25] 2014 | India | Maxillofacial surgery. | Description of a protocol using WhatsApp for communication between postgraduate trainees and senior maxillofacial surgeons. Electronic transmission of clinical images for remote consultation was done using WhatsApp in the maxillofacial unit. | Reported on both record keeping and storage. Messages stored on the phone as a digital record for future reference such that “lost X-rays are a thing of the past”. |
| Group E. Uncertain | ||||
| Williams and Kovarik. [30] 2018 | Botswana | Dermatology care. | The use of WhatsApp for dermatology care and a description as to how this application can be easily adapted and integrated into clinical practice in resource-limited settings to improve patient outcomes. | Mentioned but did not report evidence of record keeping or storage of WhatsApp message content. A reported drawback was the inability to save data centrally or integrate WhatsApp consultations into a patient’s medical record. |
| Dungarwalla et al. [26] 2019 | UK | Oral and maxillofacial surgery. | Investigation of the use of WhatsApp among oral and maxillofacial surgery junior trainees at a level one trauma centre in London. Additionally included a review of existing studies. | Mentioned but did not report evidence of record keeping or storage. A retrospective study where information was accessed from WhatsApp messages stored on the users’ mobile phones with no mention of subsequent deletion of messages. Stated that “records constitute a pillar of good clinical practice and governance”, but reported difficulties with transferring consults to patient records when using the departmental mobile phone. |
| SECTION | ITEM | PRISMA-ScR CHECKLIST ITEM | REPORTED ON PAGE |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a scoping review. | WhatsApp in Clinical Practice—The Challenges of Record Keeping and Storage. A Scoping Review |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. | P2. |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | P3-5 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | P5 |
| METHODS | |||
| Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a Web address); and if available, provide registration information, including the registration number. | No review protocol |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | P5–6 |
| Information sources * | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed. | P5 |
| Search | 8 | Present the full electronic search strategy for at least 1 database, including any limits used, such that it could be repeated. | P6 |
| Selection of sources of evidence † | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. | P6 |
| Data charting process ‡ | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. | P6 |
| Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | P6 |
| Critical appraisal of individual sources of evidence § | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used and how this information was used in any data synthesis (if appropriate). | Not done |
| Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | P6 |
| RESULTS | |||
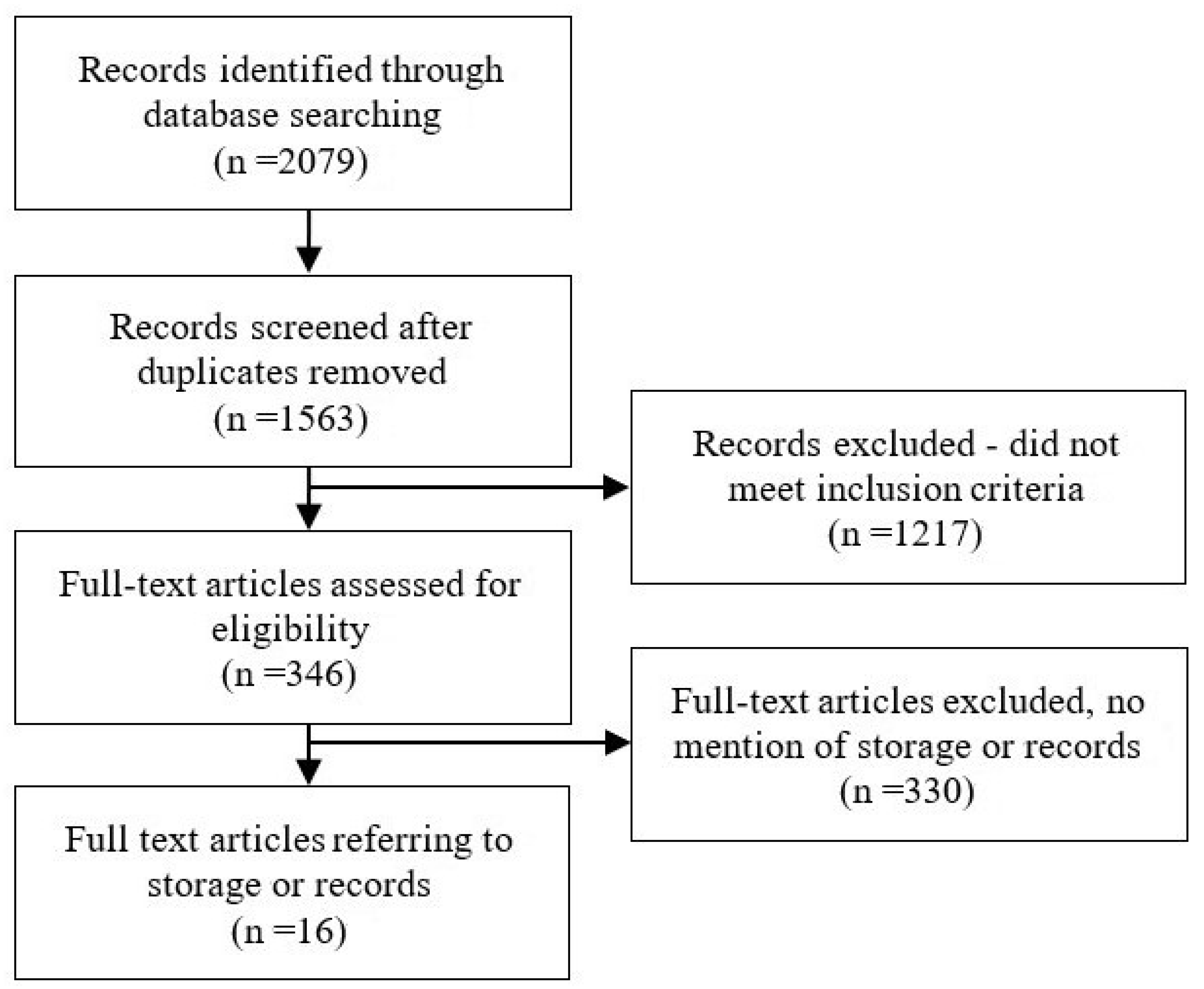
| Selection of sources of evidence | 14 | Give numbers of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram. | P7 |
| Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted and provide the citations. | P6 |
| Critical appraisal within sources of evidence | 16 | If done, present data on critical appraisal of included sources of evidence (see item 12). | Not done |
| Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | P6 |
| Synthesis of results | 18 | Summarize and/or present the charting results as they relate to the review questions and objectives. | P7–9 |
| DISCUSSION | |||
| Summary of evidence | 19 | Summarize the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups. | P9–15 |
| Limitations | 20 | Discuss the limitations of the scoping review process. | P16 |
| Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | P16–18 |
| FUNDING | |||
| Funding | 22 | Describe sources of funding for the included sources of evidence, as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review. | P19 |
References
- Nikolic, A.; Wickramasinghe, N.; Claydon-Platt, D.; Balakrishnan, V.; Smart, P. The Use of Communication Apps by Medical Staff in the Australian Health Care System: Survey Study on Prevalence and Use. JMIR Med. Inform. 2018, 6, e9. [Google Scholar] [CrossRef]
- El Hadidy, T.S.; Alshafei, A.E.; Mortell, A.E.; Doherty, E.M. Smartphones in clinical practice: Doctors’ experience at two Dublin paediatric teaching hospitals. Ir. J. Med. Sci. 2018, 187, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Marin-Gomez, F.X.; Garcia Cuyas, F.; Reig-Bolano, R.; Mendioroz, J.; Roura-Poch, P.; Pico-Nicolau, M.; Vidal-Alaball, J. Social Networking App Use Among Primary Health Care Professionals: Web-Based Cross-Sectional Survey. JMIR Mhealth Uhealth 2018, 6, e11147. [Google Scholar] [CrossRef]
- Mars, M.; Scott, R.E. WhatsApp in Clinical Practice: A Literature Review. Stud. Health Technol. Inform. 2016, 231, 82–90. [Google Scholar] [PubMed]
- Ganasegeran, K.; Renganathan, P.; Rashid, A.; Al-Dubai, S.A. The m-Health revolution: Exploring perceived benefits of WhatsApp use in clinical practice. Int. J. Med Inform. 2017, 97, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Francis, Z.; Saleem, K.; Sambujana, S.; Molise, K.; Molise, B.; Pearce, N.; Joubert, G. Usage of smart devices amongst medical practitioners in Universitas Academic Hospital. S. Afr. Fam. Pract. 2020, 62, e1–e7. [Google Scholar] [CrossRef]
- Nascimento, I.; Oliveira, J.A.Q.; Wolff, I.S.; Ribeiro, L.D.; Silva, M.; Cardoso, C.S.; Mars, M.; Ribeiro, A.L.; Marcolino, M.S. Use of smartphone-based instant messaging services in medical practice: A cross-sectional study. Sao Paulo Med. J. 2020, 138, 86–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mobasheri, M.H.; King, D.; Johnston, M.; Gautama, S.; Purkayastha, S.; Darzi, A. The ownership and clinical use of smartphones by doctors and nurses in the UK: A multicentre survey study. BMJ Innov. 2015, 1, 174–181. [Google Scholar] [CrossRef]
- Mars, M.; Morris, C.; Scott, R.E. WhatsApp guidelines—What guidelines? A literature review. J. Telemed. Telecare 2019, 25, 524–529. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. ARCHIVED: WMA Statement on Accountability, Responsibilities and Ethical Guidelines in the Practice of Telemedicine. Adopted by the 51st World Medical Assembly Tel Aviv, Israel, October 1999, and Rescinded at the WMA General Assembly, Pilanesberg, South Africa, 2006. Available online: https://www.wma.net/policies-post/wma-statement-on-accountability-responsibilities-and-ethical-guidelines-in-the-practice-of-telemedicine/ (accessed on 31 May 2021).
- World Medical Association. WMA Statement on the Ethics of Telemedicine. 58th WMA General Assembly, Copenhagen, Denmark. 2007 Oct., as Amended by the 69th WMA General Assembly, Reykjavik, Iceland. Available online: https://www.wma.net/policies-post/wma-statement-on-the-ethics-of-telemedicine/ (accessed on 31 May 2021).
- O’Flaherty, K. All the Data WhatsApp and Instagram Send to Facebook 24 July 2021. Available online: https://www.wired.co.uk/article/whatsapp-instagram-facebook-data (accessed on 31 August 2021).
- Compliancy Group. Is WhatsApp HIPAA Compliant? Available online: https://compliancy-group.com/is-whatsapp-hipaa-compliant/ (accessed on 31 May 2021).
- UNCTAD. Data Protection and Privacy Legislation Worldwide. Available online: https://unctad.org/page/data-protection-and-privacy-legislation-worldwide (accessed on 31 May 2021).
- GDPR.eu. What is GDPR, the EU’s New Data Protection Law? Available online: https://gdpr.eu/what-is-gdpr/ (accessed on 31 May 2021).
- Carvalho, G.P.; Pedrini, T.F. Direito à privacidade na lei geral de proteção de dados pessoais. Rev. Da ESMESC. 2019, 26, 363–382. [Google Scholar] [CrossRef]
- HHS.Gov. Summary of the HIPAA Privacy Rule. Available online: https://www.hhs.gov/hipaa/for-professionals/privacy/laws-regulations/index.html (accessed on 31 May 2021).
- South African Government. Protection of Personal Information Act 4 of 2013. Available online: https://www.gov.za/documents/protection-personal-information-act# (accessed on 31 May 2021).
- Scott, R.E.; Morris, C.; Mars, M. Development of a “Cellphone Stewardship Framework”: Legal, Regulatory, and Ethical Issues. Telemed. e-Health 2021, 27, 316–322. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMAScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- den Hollander, D.; Mars, M. Smart phones make smart referrals: The use of mobile phone technology in burn care—A retrospective case series. Burns 2017, 43, 190–194. [Google Scholar] [CrossRef]
- Joshi, S.S.; Murali-Krishnan, S.; Patankar, P.; Choudhari, K.A. Neurosurgical referral service using smartphone client WhatsApp: Preliminary study at a tertiary referral neurosurgical unit. Br. J. Neurosurg. 2018, 32, 553–557. [Google Scholar] [CrossRef]
- Mars, M.; Scott, R.E. Being Spontaneous: The Future of Telehealth Implementation? Telemed. e-Health 2017, 23, 766–772. [Google Scholar] [CrossRef]
- Neogi, S.; Panda, S.S. Using Whatsapp to Facilitate Inter-institutional Patient Transfer. Indian Pediatr. 2020, 57, 1084–1085. [Google Scholar] [CrossRef]
- Senthoor Pandian, S.; Srinivasan, P.; Mohan, S. The maxillofacial surgeon’s march towards a smarter future-smartphones. J. Maxillofac. Oral Surg. 2014, 13, 355–358. [Google Scholar] [CrossRef] [Green Version]
- Dungarwalla, M.; Chapireau, D.; Bentley, R. Use of WhatsApp in an oral and maxillofacial surgery department at a major trauma centre and its role during major incidents: Our experience. Br. J. Oral. Maxillofac. Surg. 2019, 57, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Johnston, M.J.; King, D.; Arora, S.; Behar, N.; Athanasiou, T.; Sevdalis, N.; Darzi, A. Smartphones let surgeons know WhatsApp: An analysis of communication in emergency surgical teams. Am. J. Surg. 2015, 209, 45–51. [Google Scholar] [CrossRef]
- Nardo, B.; Cannistra, M.; Diaco, V.; Naso, A.; Novello, M.; Zullo, A.; Ruggiero, M.; Grande, R.; Sacco, R. Optimizing Patient Surgical Management Using WhatsApp Application in the Italian Healthcare System. Telemed. e-Health 2016, 22, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Siegal, G.; Dagan, E.; Wolf, M.; Duvdevani, S.; Alon, E.E. Medical Information Exchange: Pattern of Global Mobile Messenger Usage among Otolaryngologists. Otolaryngol. Head Neck Surg. 2016, 155, 753–757. [Google Scholar] [CrossRef]
- Williams, V.; Kovarik, C. WhatsApp: An Innovative Tool for Dermatology Care in Limited Resource Settings. Telemed. e-Health 2018, 24, 464–468. [Google Scholar] [CrossRef]
- Wani, S.A.; Rabah, S.M.; Alfadil, S.; Dewanjee, N.; Najmi, Y. Efficacy of communication amongst staff members at plastic and reconstructive surgery section using smartphone and mobile WhatsApp. Indian J. Plast. Surg. 2013, 46, 502–505. [Google Scholar] [CrossRef]
- Ellanti, P.; Moriarty, A.; Coughlan, F.; McCarthy, T. The Use of WhatsApp Smartphone Messaging Improves Communication Efficiency within an Orthopaedic Surgery Team. Cureus 2017, 9, e1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gulacti, U.; Lok, U.; Hatipoglu, S.; Polat, H. An Analysis of WhatsApp Usage for Communication between Consulting and Emergency Physicians. J. Med Syst. 2016, 40, 130. [Google Scholar] [CrossRef] [PubMed]
- Sidhoum, N.; Dast, S.; Abdulshakoor, A.; Assaf, N.; Herlin, C.; Sinna, R. WhatsApp: Improvement tool for surgical team communication. J. Plast. Reconstr. Aesthetic Surg. 2016, 69, 1562–1563. [Google Scholar] [CrossRef] [PubMed]
- Martinez, R.; Rogers, A.D.; Numanoglu, A.; Rode, H. The value of WhatsApp communication in paediatric burn care. Burns 2018, 44, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Chandawarkar, R.; Nadkarni, P. Safe clinical photography: Best practice guidelines for risk management and mitigation. Arch. Plast. Surg. 2021, 48, 295–304. [Google Scholar] [CrossRef]
- Chan, N.; Charette, J.; Dumestre, D.O.; Fraulin, F.O. Should ‘smart phones’ be used for patient photography? Plast. Surg. 2016, 24, 32–34. [Google Scholar] [CrossRef]
- Spence, D. Bad Medicine: What’s up with WhatsApp? Br. J. Gen. Pract. 2018, 68, 190. [Google Scholar] [CrossRef]
- De Benedictis, A.; Lettieri, E.; Masella, C.; Gastaldi, L.; Macchini, G.; Santu, C.; Tartaglini, D. WhatsApp in hospital? An empirical investigation of individual and organizational determinants to use. PLoS ONE 2019, 14, e0209873. [Google Scholar] [CrossRef]
- WhatsApp. WhatsApp Encryption Overview Technical White Paper Version 3 Updated October 22, 2020. Available online: https://scontent.whatsapp.net/v/t39.8562-34/217392192_617386875906350_2307693746154839727_n.pdf/WhatsApp_Security_Whitepaper_V4_Preview.pdf? (accessed on 31 May 2021).
- Watson, L.; Pathiraja, F.; Depala, A.; O’Brien, B.; Beyzade, S. Ensuring safe communication in health care: A response to Johnston et al on their paper “Smartphones let surgeons know WhatsApp: An analysis of communication in emergency surgical teams”. Am. J. Surg. 2016, 211, 302–303. [Google Scholar] [CrossRef] [PubMed]
- Drake, T.M.; Claireaux, H.A.; Khatri, C.; Chapman, S.J. WhatsApp with patient data transmitted via instant messaging? Am. J. Surg. 2016, 211, 300–301. [Google Scholar] [CrossRef]
- Schaller, K. Editorial re: WhatsAPP in neurosurgery: The best practice is in our hands. Acta Neurochir. 2016, 158, 2175. [Google Scholar] [CrossRef] [PubMed]
- Deen, S.R.; Withers, A.; Hellerstein, D.J. Mental health practitioners’ use and attitudes regarding the Internet and social media. J. Psychiatr. Pract. 2013, 19, 454–463. [Google Scholar] [CrossRef]
- Thomas, K. Wanted: A WhatsApp alternative for clinicians. BMJ 2018, 360, k622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masoni, M.; Guelfi, M.R. WhatsApp and other messaging apps in medicine: Opportunities and risks. Intern. Emerg. Med. 2020, 15, 171–173. [Google Scholar] [CrossRef] [PubMed]
- Dhawan, B. Germany has banned WhatsApp’s Controversial ‘Take It or Leave It’ Privacy Policy That Comes into Effect on May 15, Will India Be Next? 14 May 2021. Available online: https://www.financialexpress.com/industry/technology/germany-has-banned-whatsapps-controversial-take-it-or-leave-it-privacy-policy-that-comes-into-effect-on-may-15-will-india-be-next/2251975/ (accessed on 30 June 2021).
- Morris, C.; Scott, R.; Mars, M. Is Consent Not a Consideration for Instant Messaging. In Telehealth Innovations in Remote Healthcare Services Delivery; IOS Press: Amsterdam, The Netherlands, 2021; pp. 88–95. [Google Scholar]
- O’Sullivan, D.M.; O’Sullivan, E.; O’Connor, M.; Lyons, D.; McManus, J. WhatsApp Doc? BMJ Innov. 2017, 3, 238–239. [Google Scholar] [CrossRef]
- Carmona, S.; Alayed, N.; Al-Ibrahim, A.; D’Souza, R. Realizing the potential of real-time clinical collaboration in maternal-fetal and obstetric medicine through WhatsApp. Obstet. Med. 2018, 11, 83–89. [Google Scholar] [CrossRef]
- NHSX England. Using Mobile Messaging 19 May 2021. Available online: https://www.nhsx.nhs.uk/information-governance/guidance/use-mobile-messaging-software-health-and-care-settings/ (accessed on 23 November 2021).
- GDPR. General Data Protection Regulation GDPR May 25 2018 Sections 9.2 h and 9.3. Available online: https://gdpr.eu/ (accessed on 31 May 2021).


| Database | Search Strings | Resources |
|---|---|---|
| PubMed | “WhatsApp” [All fields] a | 601 |
| Scopus | (ALL (“WhatsApp”) AND ALL (“telemedicine” OR “telehealth” OR “ehealth” OR “e-health” OR “mhealth” OR “m-health”)) | 741 |
| Science Direct | ((“WhatsApp”) AND (“telemedicine” OR “telehealth” OR “ehealth” OR “e-health” OR “mhealth” OR “m-health”)) All fields | 282 |
| Ebsco Host | ((“WhatsApp”) AND (“telemedicine” OR “telehealth” OR “ehealth” OR “e-health” OR “mhealth” OR “m-health”)) All text | 503 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morris, C.; Scott, R.E.; Mars, M. WhatsApp in Clinical Practice—The Challenges of Record Keeping and Storage. A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 13426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413426
Morris C, Scott RE, Mars M. WhatsApp in Clinical Practice—The Challenges of Record Keeping and Storage. A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(24):13426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413426
Chicago/Turabian StyleMorris, Christopher, Richard E. Scott, and Maurice Mars. 2021. "WhatsApp in Clinical Practice—The Challenges of Record Keeping and Storage. A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 24: 13426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413426