Expectations and Assumptions: Examining the Influence of Staff Culture on a Novel School-Based Intervention to Enable Risky Play for Children with Disabilities

 , , , , and
, , , , and
Abstract
:1. Introduction
1.1. A Novel Intervention to Promote Risky Play for Children with Disabilities
1.2. Staff Culture: A Factor to Consider When Implementing a Novel Program
- What was the staff culture (i.e., shared beliefs, norms, values, and practices) surrounding disability, play/recess, and risk-taking that characterized each of the two schools?
- How did staff culture differentially influence how staff engaged with the intervention and, subsequently, the quantitative outcomes?
2. Methods
2.1. Case Selection
2.2. Case Descriptions
2.2.1. School A
2.2.2. School B
2.3. Data Sources
2.4. Interview Participants
2.5. Data Analysis
2.5.1. Within-Case Analysis
2.5.2. Cross-Case Synthesis
2.5.3. Trustworthiness
3. Findings
3.1. School A
3.1.1. Disability Makes Our Children Different
Some of them don’t get the rules and they don’t understand the danger. A lot of the kids don’t have any understanding of the danger I feel, some do, but I think a lot of them are just trying to get through the day. (Teacher A1)
Because it’s really tricky for our kids, like they’re overcoming all of their issues to be able to just play with us. To overcome all of their issues and then have to overcome all the other kids with autism’s issues, makes an interaction between two of our kids really quite difficult. (Teacher A4)
3.1.2. The Playground Is a Pedagogical Place
If I knew that Jack has a turn-taking outcome, I’d be like, “oh, Jack, let’s go on the trampoline, oh, it’s blah-blah-blah’s turn, okay, that means we have to wait”. And you’d try and facilitate those interactions that are working towards their goals, instead of just letting them work it out for themselves. (OT A1)
3.1.3. Keeping Control over Risk and Challenge
Although it might not be risk as such, you know, I step back a lot and let the kids try and problem solve, especially things I know they can figure out, well, they can eventually figure out, that’s not going to get them too upset. (Teacher A3)
Kids who climb all the time and I see from assessing them that they’ve got really great gross motor skills, I’d be more likely to step back and let them climb to the top of the tree, than I would a kid who trips over all the time and spends most of their time on the floor or falling over or has less skills. (Teacher A1)
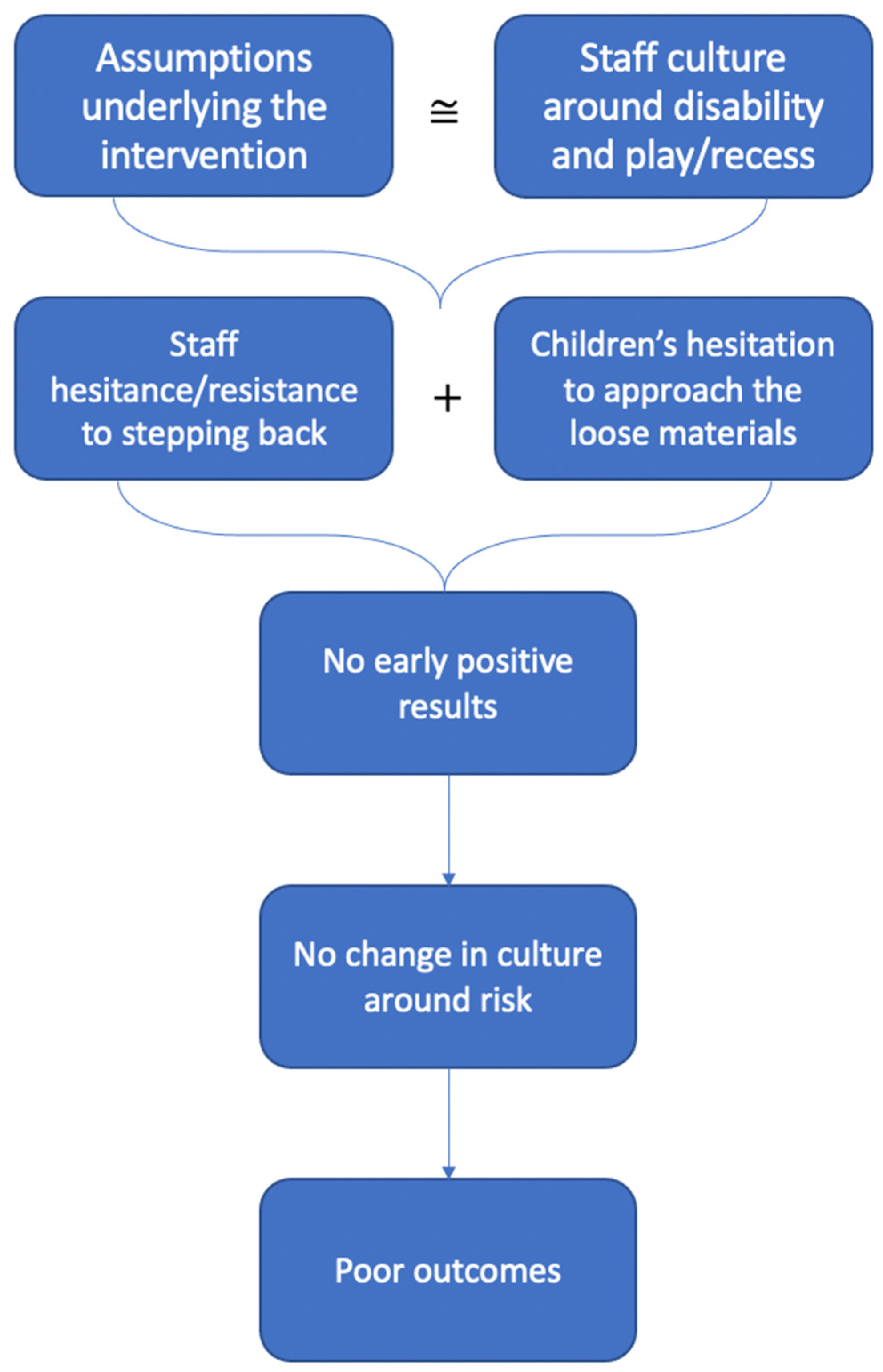
3.1.4. Theoretical Proposition: What Happened at School A?
We always try and engage with the kids in the playground, and we didn’t stop trying to engage with the kids in the playground in the other areas, it was just in that area that was like the dead spot where you don’t engage with the kids. (Teacher A1)
I think the big thing that came up for me was in the playground we’ve been told and taught to play with the kids and interact with the kids, but we were told not to encourage them to play with the playground stuff. But somehow within that message, it kind of became if they’re playing with the playground stuff, walk away. So, I didn’t always do that, like I was sometimes playing with them when they started playing with it. But I think because they are so used to taking their lead by us, it ended up… didn’t get used that much. (Teacher A4)
I just think, like, because these kids find it hard to play, a lot of them, I think perhaps if it had been presented a bit better, like if some materials had been put into the sandpit, if some had been put into the ball pit, if they’d sort of been spread out a bit. And maybe if the staff had been allowed to model, like, different things you could with it as well, I wonder if it would have got them playing a bit more. (OT A1)
And so I really don’t think, upon reflection, we do give them enough of a chance to initiate the play because we’re always trying to get so much out of them, which is probably why they didn’t get as involved as what we would have thought they would. (Teacher A2)
3.2. School B
3.2.1. High Expectations for Children with Disabilities
I don’t think I think of them any differently. They play the same games that other kids play, and they do the same thing that other kids, so not really. No. I let them do their own thing and if they look like they’re going to, you know, get injured or hurt someone, of course I’ll step in, but I don’t think I... No, I let them do their thing. Why not? We’re all entitled to it. (MS Teacher B4)
3.2.2. Inconsistent Beliefs about Recess and Play
They, they’re learning how to, um, create friendships and learning how to maintain friendships. They’re learning how to play safely, um, abiding by their own rules of the games that they’re playing. Um, they’re learning to be you know, good sportsmen. (MS Teacher B2)
One of my things, you know, I will get out there sometimes and play captain ball or tunnel ball or some of, you know, the catching games with my class and if other kids want to join in, fine you know, so be it, but my point as well is, our kids who haven’t got those skills, need to get those skills before they go and put themselves in a situation, where they ask other kids, “Can I play?” (SLSO B1)
3.2.3. Preventing Risk before It Happens
We’re just ensuring that, um, there’s no hot spots happening and, um, the teachers that are, that are on duty are, you know, walking where they need to walk and stopping those little hot spots from you know, becoming enraged fires. (MS Teacher B2)
Traditionally the students have been quite compliant. Um, they’ve done what they’ve been told to do, kind of, but not so good at thinking for themselves and working things out. They’re very sort of rule-based and so they haven’t really worked things out for themselves. (Principal B1)
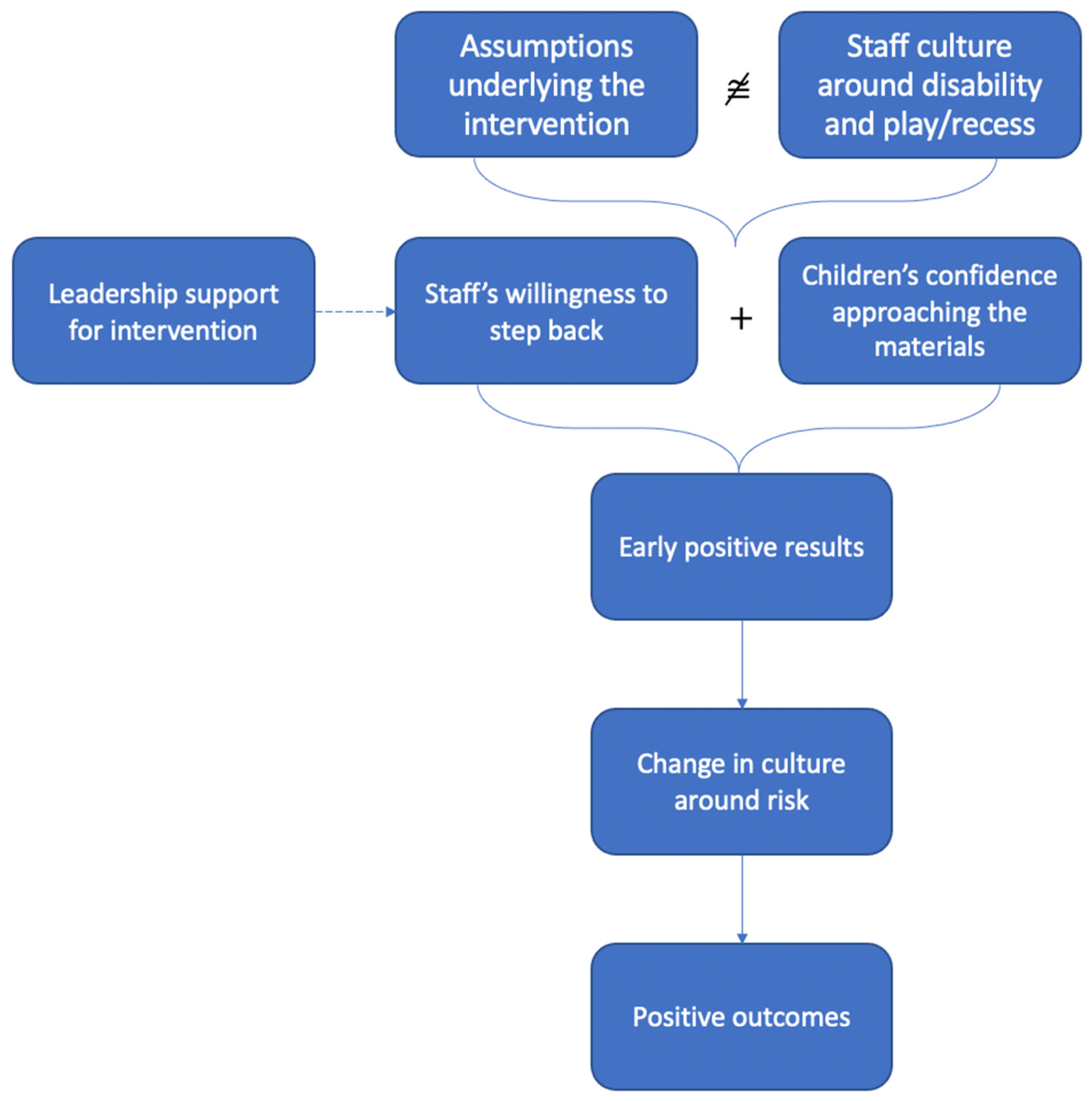
3.2.4. Theoretical Proposition: What Happened at School B?
I stepped away and I’m like, “You know what I’m gonna- I’m gonna wait until I actually- I genuinely think something’s there”. So, I’d wait over there and have my heart palpitating going, “Oh my gosh. Oh my gosh”. (laughs) But um, yeah, until like I actually took that step back, I’d be- like, you know, it took me a while to realize oh, that’s how they play. (MS Teacher B1)
More than excitement, the absolute passion and glee that a large majority of the children attacked the, um, equipment, was phenomenal. They just saw it and couldn’t wait to get a piece of it. And, so, um, they, they were passionate. They were desperate. They were like, um, addicts I think, you know, just returning to their source of, um, uh, addiction, after a long break.
So, what the playground project did for that, that- say that child with autism who, who plays by himself, is he had to play with others. And then those who were continually- they’re those who continually look for external sources of play, they then had to go up there and do imaginative stuff, because there aren’t- it was, it was junk, right?
4. Discussion
4.1. Differing Expectations: Influences of Culture around Disability on the Intervention
4.2. What’s the Point of Play? Influences of Culture around Play/Recess on the Intervention
4.3. Disability and Play: Intertwined Influences on the Intervention
4.4. What about Risk?
4.5. Limitations
5. Conclusions
What Could We Have Done Differently?
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sandseter, E.B. Characteristics of risky play. J. Adventure Educ. Outdoor Learn. 2009, 9, 3–21. [Google Scholar] [CrossRef]
- Kleppe, R.; Melhuish, E.; Sandseter, E.B.H. Identifying and characterizing risky play in the age one-to-three years. Eur. Early Child. Educ. Res. J. 2017, 15, 1–16. [Google Scholar] [CrossRef]
- Sandseter, E.B.; Little, H.; Wyver, S. Do theory and pedagogy have an impact on provisions for outdoor learning? A comparison of approaches in Australia and Norway. J. Adventure Educ. Outdoor Learn. 2012, 12, 167–182. [Google Scholar] [CrossRef]
- Van Rooijen, M.; Newstead, S. Influencing factors on professional attitudes towards risk-taking in children’s play: A narrative review. Early Child. Dev. Care 2016, 187, 946–957. [Google Scholar] [CrossRef]
- Wyver, S.; Tranter, P.; Naughton, G.; Little, H.; Sandseter, E.B.H.; Bundy, A. Ten ways to restrict children’s freedom to play: The problem of surplus safety. Contemp. Issues Early Child. 2010, 11, 263–277. [Google Scholar] [CrossRef] [Green Version]
- Bundy, A.C.; Wyver, S.; Beetham, K.S.; Ragen, J.; Naughton, G.; Tranter, P.; Norman, R.; Villeneuve, M.; Spencer, G.; Honey, A.; et al. The Sydney playground project-levelling the playing field: A cluster trial of a primary school-based intervention aiming to promote manageable risk-taking in children with disability. BMC Public Health 2015, 15, 1125. [Google Scholar] [CrossRef] [Green Version]
- Adams, R.C.; Levy, S.E. Shared decision-making and children with disabilities: Pathways to consensus. Pediatrics 2017, 139, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Brussoni, M.; Gibbons, R.; Gray, C.; Ishikawa, T.; Sandseter, E.B.; Bienenstock, A.; Tremblay, M.S. What is the relationship between risky outdoor play and health in children? A systematic review. Int. J. Environ. Res. Public Health 2015, 12, 6423–6454. [Google Scholar] [CrossRef]
- Engelen, L.; Bundy, A.C.; Naughton, G.; Simpson, J.M.; Bauman, A.; Ragen, J.; Baur, L.; Wyver, S.; Tranter, P.; Niehues, A.; et al. Increasing physical activity in young primary school children—it’s child’s play: A cluster randomised controlled trial. Prev. Med. 2013, 56, 319–325. [Google Scholar] [CrossRef]
- Kahathuduwa, C.N.; West, B.D.; Blume, J.; Dharavath, N.; Moustaid-Moussa, N.; Mastergeorge, A. The risk of overweight and obesity in children with autism spectrum disorders: A systematic review and meta-analysis. Obes. Rev. 2019, 20, 1667–1679. [Google Scholar] [CrossRef]
- Maiano, C.; Hue, O.; Morin, A.J.; Moullec, G. Prevalence of overweight and obesity among children and adolescence with intellectual disabilities: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 599–611. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, A.D.; Smith, P.K. Physical activity play: The nature and function of a neglected aspect of play. Child Dev. 1998, 69, 577–598. [Google Scholar] [PubMed]
- American Psychiatric Association. DSM-5 Task Force. In Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; p. xliv. 947p. [Google Scholar]
- Grady-Dominguez, P.; Bundy, A.; Ragen, J.; Wyver, S.; Villeneuve, M.; Naughton, G.; Tranter, P.; Eakman, A.; Hepburn, S.; Beetham, K. An observation-based instrument to measure what children with disabilities do on the playground: A Rasch analysis. Int. J. Play 2019, 8, 79–93. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioural Science, 2nd ed.; Lawrence Erlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- Zeitlin, S. Coping Inventory: A Measure of Adaptive Behavior; Scholastic Testing Service: Bensenville, IL, USA, 1985. [Google Scholar]
- Skard, G.; Bundy, A.C. Test of Playfulness; Mosby: St. Louis, MO, USA, 2008. [Google Scholar] [CrossRef]
- Domitrovich, C.E.; Bradshaw, C.P.; Poduska, J.M.; Hoagwood, K.; Buckley, J.A.; Olin, S.; Romanelli, L.H.; Leaf, P.J.; Greenberg, M.T.; Ialongo, N.S. Maximizing the implementation quality of evidence-based preventive interventions in schools: A conceptual framework. Adv. Sch. Ment. Health Promot. 2008, 1, 6–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teasley, M.L. Organizational Culture and Schools: A Call for Leadership and Collaboration. Child. Sch. 2017, 39, 3–6. [Google Scholar] [CrossRef]
- McIsaac, J.L.D.; Spencer, R.; Chiasson, K.; Kontak, J.; Kirk, S.F.L. Factors Influencing the Implementation of Nutrition Policies in Schools: A Scoping Review; SAGE Publications Inc.: Thousand Oaks, CA, USA, 2019; Volume 46, pp. 224–250. [Google Scholar]
- Jordan, A.; Glenn, C.; McGhie-Richmond, D. The Supporting Effective Teaching (SET) project: The relationship of inclusive teaching practices to teachers’ beliefs about disability and ability, and about their roles as teachers. Teach. Teach. Educ. 2010, 26, 259–266. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Disability, Aging and Carers; ABS: Sydney, Australia, 2019.
- Sutton-Smith, B. The Ambiguity of Play; Harvard University Press: Boston, MA, USA, 1997. [Google Scholar]
- Peterson, S.S.; Riehl, D. Rhetorics of Play in Kindergarten Programs in an Era of Accountability. Brock Educ. J. 2016, 25, 2016. [Google Scholar] [CrossRef]
- Sandseter, E.B.H.; Sando, O.J. “We don’t allow children to climb trees”: How a focus on safety affects Norwegian children’s play in early-childhood education and care settings. Am. J. Play 2016, 8, 178–200. [Google Scholar]
- Yin, R.K. Case Study Research and Applications: Design and Methods, 6th ed.; SAGE: New York, NY, USA, 2018. [Google Scholar]
- Braun, V.; Clarke, V. Thematic Analysis; American Psychological Association: Washington, DC, USA, 2012; pp. 57–71. [Google Scholar] [CrossRef]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; SAGE: Newbury Park, CA, USA, 1985. [Google Scholar]
- Murray, C.; Pianta, R.C. The importance of teacher-student relationships for adolescents with high incidence disabilities. Theory Pract. 2007, 46, 105–112. [Google Scholar] [CrossRef]
- Doren, B.; Gau, J.M.; Lindstrom, L.E. The relationship between parent expectations and postschool outcomes of adolescents with disabilities. Except. Child. 2012, 79, 7–23. [Google Scholar] [CrossRef] [Green Version]
- Martinez, D.C.; Conroy, J.W.; Cerreto, M.C. Parent Involvement in the Transition Process of Children with Intellectual Disabilities: The Influence of Inclusion on Parent Desires and Expectations for Postsecondary Education. J. Policy Pract. Intellect. Disabil. 2012, 9, 279–288. [Google Scholar] [CrossRef]
- Jarrold, C. A review of research into pretend play in autism. Autism 2003, 7, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Jordan, R. Social play and autistic spectrum disorders: A perspective on theory, implications and educational approaches. Autism 2003, 7, 347–360. [Google Scholar] [CrossRef] [PubMed]
- Jahr, E.; Eldevik, S.; Eikeseth, S. Teaching children with autism to initiate and sustain cooperative play. Res. Dev. Disabil. 2000, 21, 151–169. [Google Scholar] [CrossRef]
- Charlop, M.H.; Lang, R.; Rispoli, M. Lights, Camera, Action! Teaching Play and Social Skills to Children with Autism Spectrum Disorder through Video Modeling; Springer: Berlin/Heidelberg, Germany, 2018; pp. 71–94. [Google Scholar] [CrossRef]
- MacCormack, J. Different, not less: The problem with defining “normal” social play of children with autism spectrum disorder. Antistasis 2020, 10. Available online: https://journals.lib.unb.ca/index.php/antistasis/article/view/31285 (accessed on 21 January 2021).
- Bast, L.S.; Due, P.; Ersbøll, A.K.; Damsgaard, M.T.; Andersen, A. Association of School Characteristics and Implementation in the X:IT Study-A School-Randomized Smoking Prevention Program. J. Sch. Health 2017, 87, 329–337. [Google Scholar] [CrossRef]
- Little, H.; Sandseter, E.B.H.; Wyver, S. Early Childhood Teachers’ Beliefs about Children’s Risky Play in Australia and Norway. Contemp. Issues Early Child. 2012, 13, 300–316. [Google Scholar] [CrossRef]
- Parsons, J.; Beauchamp, L. Leadership in effective elementary schools: A synthesis of five case studies. US-China Educ. Rev. 2012, 8, 697–711. [Google Scholar]
- Wolfberg, P.; Bottema-Beutel, K.; Dewitt, M. Including Children with Autism in Social and Imaginary Play with Typical Peers. Am. J. Play 2012, 5, 55–80. [Google Scholar]
- Skaines, N.; Rodger, S.; Bundy, A. Playfulness in Children with Autistic Disorder and their Typically Developing Peers. Br. J. Occup. Ther. 2006, 69, 505–512. [Google Scholar] [CrossRef]
- Stanley, G.C.; Konstantareas, M.M. Symbolic play in children with autism spectrum disorder. J. Autism Dev. Disord. 2007, 37, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for implementation research: Conceptual distinctions, measurement challenges, and research agenda. Adm. Policy Ment. Health Ment. Health Serv. Res. 2011, 38, 65–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcome | Unit of Analysis | Data Collection | Analysis |
|---|---|---|---|
| Sophistication of Play Activities | Playground session |
|
|
| Play Engagement | Playground session |
|
|
| Coping Ability | Individual child | Staff member familiar with target children completed Coping Inventory [16] during control and post-intervention. |
|
| Pseudonym | Role | |
|---|---|---|
| School A | OT A1 | Occupational therapist |
| Teacher A1 | Classroom teacher | |
| Teacher A2 | Classroom teacher | |
| Teacher A3 | Classroom teacher | |
| Teacher A4 | Classroom teacher | |
| School B | Principal B1 | Principal |
| Deputy Principal B1 | Deputy Principal | |
| SU Teacher B1 | Support Unit Teacher | |
| SU Teacher B2 | Support Unit Teacher | |
| SLSO B1 | Student Learning Support Officer (working directly with students from the support unit) | |
| MS Teacher B1 | English as an Additional Language Teacher | |
| MS Teacher B2 | Mainstream Teacher | |
| MS Teacher B3 | Mainstream Teacher | |
| MS Teacher B4 | Mainstream Teacher |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grady-Dominguez, P.; Ragen, J.; Sterman, J.; Spencer, G.; Tranter, P.; Villeneuve, M.; Bundy, A. Expectations and Assumptions: Examining the Influence of Staff Culture on a Novel School-Based Intervention to Enable Risky Play for Children with Disabilities. Int. J. Environ. Res. Public Health 2021, 18, 1008. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031008
Grady-Dominguez P, Ragen J, Sterman J, Spencer G, Tranter P, Villeneuve M, Bundy A. Expectations and Assumptions: Examining the Influence of Staff Culture on a Novel School-Based Intervention to Enable Risky Play for Children with Disabilities. International Journal of Environmental Research and Public Health. 2021; 18(3):1008. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031008
Chicago/Turabian StyleGrady-Dominguez, Patricia, Jo Ragen, Julia Sterman, Grace Spencer, Paul Tranter, Michelle Villeneuve, and Anita Bundy. 2021. "Expectations and Assumptions: Examining the Influence of Staff Culture on a Novel School-Based Intervention to Enable Risky Play for Children with Disabilities" International Journal of Environmental Research and Public Health 18, no. 3: 1008. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031008