1. Introduction
Human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS) has become one of the most severe public health issues since the first cases of AIDS were identified in 1981 [
1]. At the end of 2019, approximately 38.0 million (31.6 million–44.5 million) people are living with HIV [
2]. Due to gaps in HIV services, about 32.7 million (24.8 million–42.2 million) people have died from AIDS-related illnesses [
2]. Ensuring healthy lives and promoting well-being for all ages were addressed by the United Nations as one of 17 Sustainable Development Goals in the 2030 Agenda [
3]. Currently, the research on AIDS is mostly focused on epidemiology, and comparative analysis between different social characteristics and geographical populations has been done by epidemiologists [
4]. Since the generation, transmission, and distribution of AIDS are closely related to geospatial information [
5], tabular records could lose critical information for vaccination tracking and surveillance due to the neglect of the spatial and geographic attributes related to AIDS cases.
As a branch of epidemiology, spatial epidemiology has developed rapidly in recent years. With spatial statistical methods, spatial epidemiology improves the understanding of disease from qualitative level to quantitative level, by analyzing geographically indexed health data related to demography, environment, behavior, socio-economy, genetics, etc. [
6,
7]. Supported by geographic information science (GIS) and spatial analysis technology, spatial epidemiology describes and analyzes the spatial distribution characteristics and development pattern of epidemiological health events. With a vivid summary and precise pattern of areas at apparently high risk [
8], the related disease maps can be used for various descriptive purposes, including aid policy formation and resource allocation [
6,
9].
Spatial analysis has become increasingly common in HIV/AIDS-related research, specifically for the geographic distribution assessment [
10]. For instance, Bautista et al. [
11] analyzed the spatial distribution of HIV infection among U.S. civilian applicants for US military service from 1985 to 2003, and found the difference in HIV spatial aggregation between white people and African Americans. Focusing on HIV infection rate in rural areas of South Africa, Tanser et al. provided clear empirical evidence for the localized clustering of HIV infection [
12]. The study detected considerable geographical variation in local HIV prevalence within relatively homogenous population, i.e., population do not have much geographical socioeconomic variation. In a recent study of the prevalence of HIV in sub-Saharan Africa, Dwyer-Lindgren et al. [
13] revealed considerable within-country variation and local differences in the change direction and rate in HIV prevalence from 2000 to 2017, which brought attention to the subnational variation in HIV prevalence and the related fine-scale estimation and interventions. In China, trend surface analysis and spatial autocorrelation analysis on AIDS have been conducted for a single province or city, including Yunnan [
14] and Lanzhou [
15]. However, most publications have merely addressed characteristics of the HIV infection at the regional level.
For truly controlling HIV and directly reducing the number of new infections, an understanding of the spatial distribution needs to be combined with an investigation of potential influencing factors. Smith et al. [
16] found that education level is an important factor in AIDS risk in rural Uganda. Liu et al. [
17] studied the spatial distribution and influencing factors of HIV-infected people in Henan Province, and found that economic level and medical level will have a certain impact on the incidence of AIDS. Most recently, Yang and Li [
18] found that the economy, medical treatment, and transportation (i.e., population flow) have an impact on the AIDS incidence in China. Conventional statistics (e.g., ordinary least squares (OLS)) are the primary tools to examine the impacts of underlying factors. However, the prominent limitation of conventional statistics in geoscience is the incapability in capturing the spatial non-stationarity, i.e., spatially varying relationships between dependent and independent variables [
19,
20]. Moreover, OLS has been shown to be of limited utility when spatial data are coupled with highly correlated independent variables [
21,
22,
23]. An alternative to conventional statistics is Geographically Weighted Regression (GWR).
The discipline of the spatial and temporal analysis of the AIDS incidence and its influencing factors are not uniform. So far, the research mainly focuses on the analysis of AIDS spatial distribution, especially in South Africa [
9,
12,
13,
24,
25], At present, the related research on AIDS in China mainly focuses on the analysis of epidemiological characteristics [
26], prevention and control [
27,
28], the epidemic situation of the specific population [
29,
30], etiology and sociology [
18,
31], however, there are few studies on the spatial-temporal change analysis and influencing factors analysis. The long time series study on AIDS incidence, the future trend, and factors affecting AIDS spread in China have not yet explored.
To fill the gap, this study collected the AIDS incidence data on Chinese mainland from 2005 to 2017 to study the spatial distribution characteristics and influencing factors of the AIDS epidemic, so as to provide a theoretical basis for policymakers to customize scientific prevention and control policies. The study focused on AIDS incidence, i.e., the body’s immune system is badly damaged because of the HIV virus. The paper is organized as follows. After the description of the research data and sources,
Section 2 presents the mean research methods, including AIDS intensity level mapping (
Section 2.1), Markov chain matrix analysis (
Section 2.2), Spatial clustering character (
Section 2.3), and GWR analysis (
Section 2.4). The related results are followed in
Section 3.
Section 4 discusses key issues of the AIDS intensity on the Chinese mainland, and the findings based on the analytical method are also summarized. Finally, short conclusions are provided in
Section 5.
3. Results
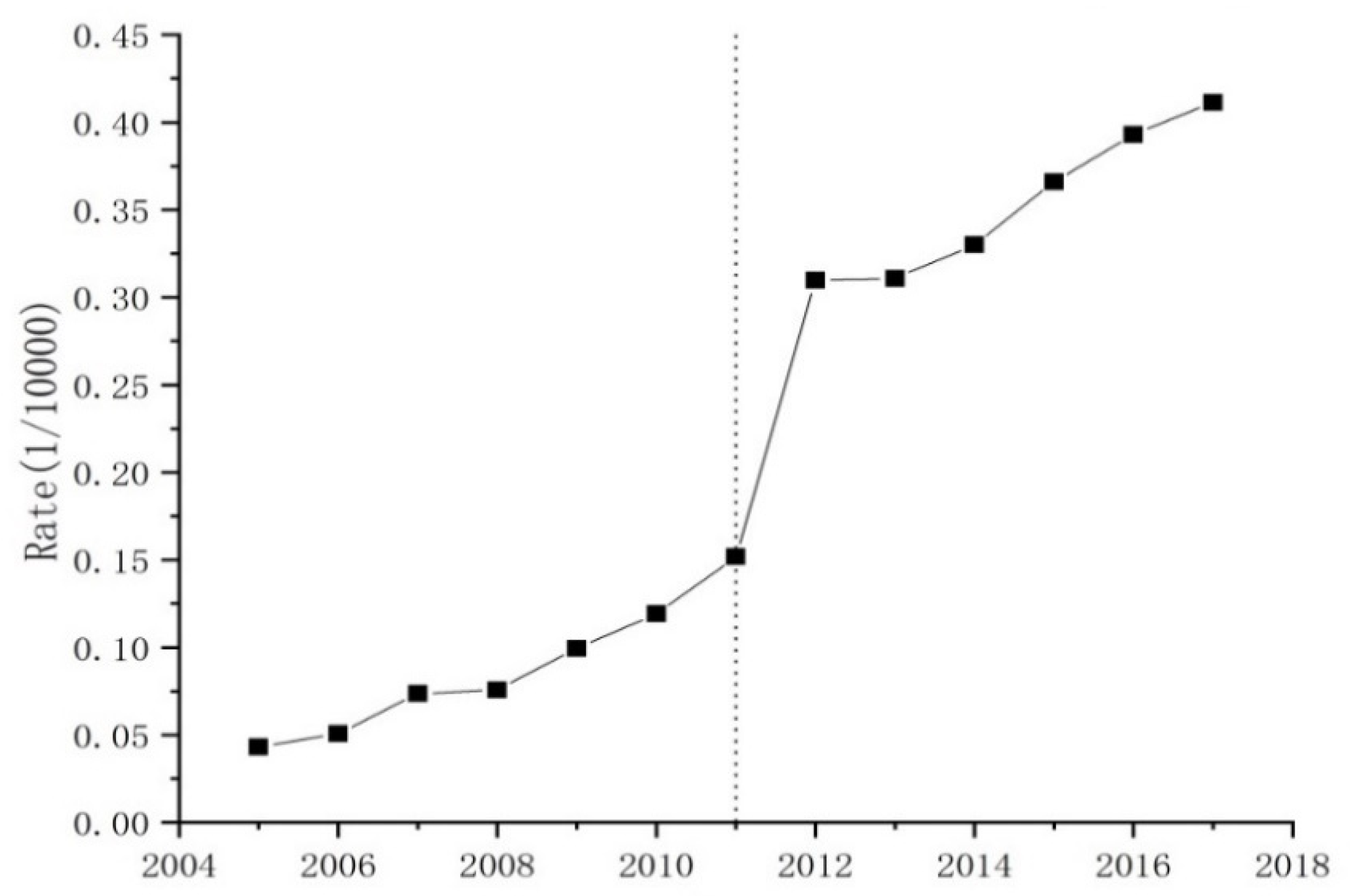
The overall change trend AIDS incidence rate at the national level for the mainland of China from 2005 to 2017 can be divided into four stages (
Figure 1). The first stage (2005–2008) witnessed a stable growth, with an average AIDS incidence rate of 0.06 per ten thousand persons (0.06/10000). In comparison, the AIDS incidence rate showed a slight increasingly tendency in the second stage (2008–2011), with an average AIDS incidence rate of 0.11 per ten thousand persons (0.11/10000). During the third stage (2011–2014), the AIDS incidence rate exhibited a remarkable fluctuating growth, with an annual growth of 105% from 2011 to 2012 as well as a steady stable growth, with an annual growth of 7.67% from 2012 to 2014. After 2014, the AIDS incidence rate indicated a stable growth again, with an average AIDS incidence rate of 0.38 per ten thousand persons (0.38/10000) and annual growth rate of 11.5%.
3.1. Spatiotemporal Variation of AIDS Intensity
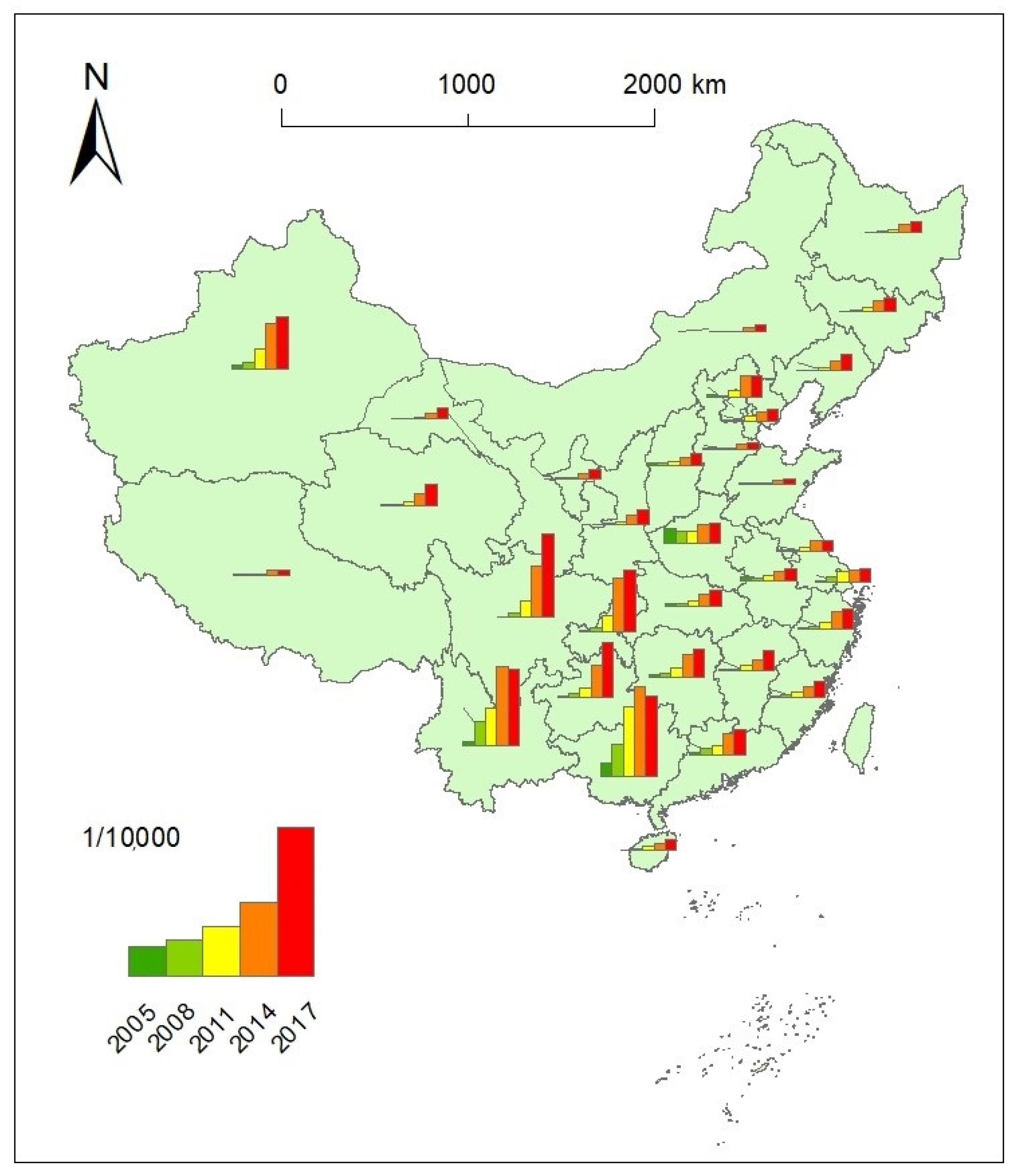
The spatial distribution of AIDS incidence rates at the provincial scale was first visualized intuitively in ArcGIS10.2 software (ERSI, Redlands, USA,
Figure 2 and
Figure 3). The AIDS incidence rate had been increasing for most of the provincial units on the Chinese mainland (
Figure 2). Apparently, the differences in AIDS incidence rates were very high during the entire study period, with high incidence rates in southwestern China, including Yunnan, Guangxi, Guizhou, Sichuan and Chongqing, and Xinjiang in northeastern China. Meanwhile, there were considerable differences among these provincial administrative units in the AIDS incidence rate from 2014 to 2017, and the AIDS incidence rate showed a decreasing tendency for Guangxi and Yunnan. In contrast, the AIDS incidence rates were relatively low, with a generally stable increase during the study period in central and eastern China during the study periods.
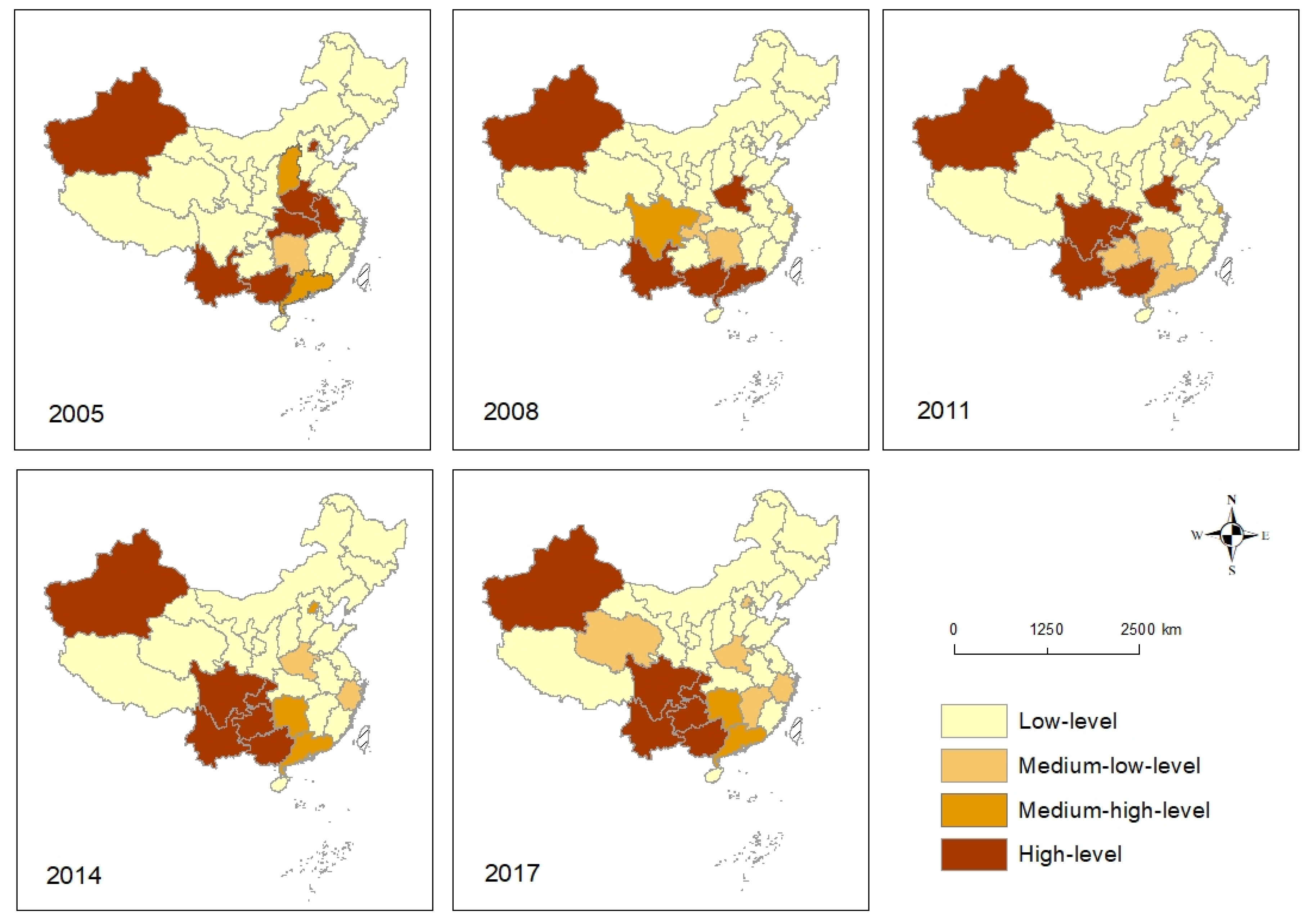
The AIDS intensity levels for the individual provincial administrative unit for the above time points were further calculated (
Table A2 in the
Appendix A). The AIDS intensity level charts in 2005, 2008, 2011, 2014, and 2017 showed the difference in the spatial distribution and temporal variation (
Figure 3). Different from other periods, the high AIDS intensity levels were relatively scattered in space in 2005. Yunnan, Guangxi, Beijing, Xinjiang, and three adjacent provinces in central China showed high AIDS intensity levels in 2005. From 2008 to 2017, the high incidence areas gradually monopolized in the southwestern region, and the spatial agglomeration was enhanced. The spatial pattern of AIDS intensity levels changed greatly from 2005 to 2008. The AIDS high-value zone expanded to Sichuan and Chongqing and the pattern of AIDS low-level intensity areas remained relatively stable from 2008 to 2011. There is a note that the AIDS intensity level changed from high (code 1) to the middle and low level (code 3) for Henan from 2011 to 2014. The spatial pattern of AIDS high-level intensity areas remained relatively stable from 2014 to 2017.
Spatial Markov matrixes were calculated for the respective four stages to compare the AIDS intensity level evolution character classified above (
Table 3). Notably, smooth transition probabilities of low-low (
) and high-high (
) AIDS intensity levels were above 0.86, and the highest was 1 for the four stages, which were far higher than the average level of other transition probability. It is also noted that the transition probabilities between adjacent levels were much greater than that between cross levels, indicating that the temporal evolution of AIDS intensity are gradual rather than jumping. The transition probabilities related to medium-high levels and medium-low levels transiting to other levels were relatively unstable, ranging from 0.17 to 1.
In terms of the AIDS intensity evolution characteristics between different stages, the overall downward transition probabilities between 2005 and 2008 were higher than the upward transition probabilities, indicating that the AIDS intensity level gradually decreased; the upward transfer probabilities between 2008 and 2011 were greater than the downward transfer probabilities, indicating that AIDS risk had been gradually increasing. In the next two stages, the upward transition probabilities had been decreasing from 0.3 to 0.03 and the downward transition probabilities had been decreasing from 0.4 to 0.01, indicating that AIDS risk had been gradually decreasing.
3.2. Spatial Agglomeration Characteristic of AIDS
Table A3 in
Appendix A provides the Global Moran’s I index statistical result for the AIDS incidence rates. In the year 2005, 2006, and 2007, the returned
p-value is not statistically significant, and the global spatial autocorrelation characteristics of the AIDS incidence rates was not detected. Started from 2009,
p values were all <0.05 (passed through the 95% confidence test) and z scores are positive (>1.65, the threshold set by the null hypothesis being rejected), indicating that the AIDS incidence rates had become spatially clustered. Especially, between 2011 and 2017, the global Moran’s I index raised rapidly from −0.114 to 0.312, indicating a growing spatial clustering tendency of the AIDS incidence rate for the enter study area.
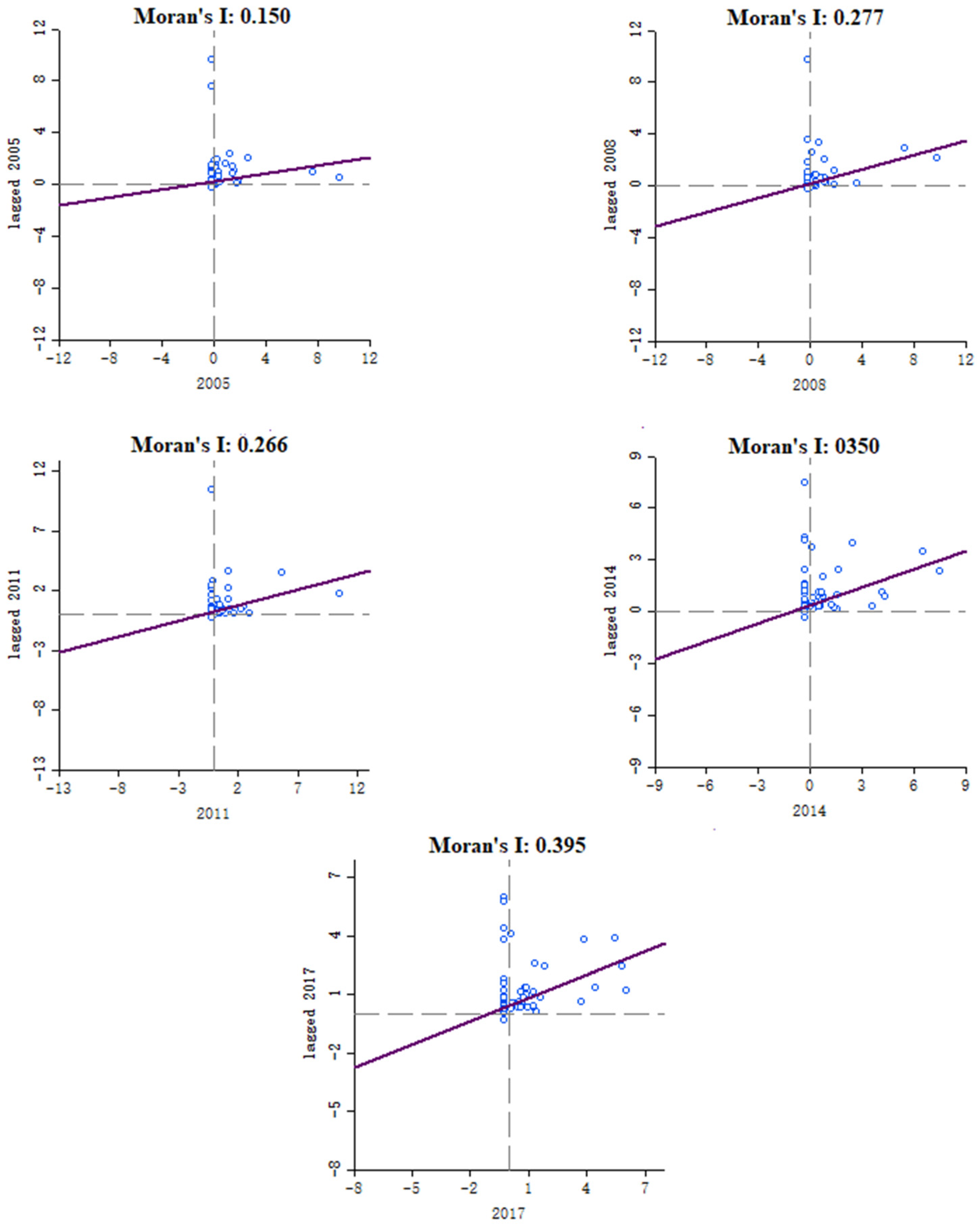
To further measure the spatial correlation and difference of AIDS incidence rates for each provincial unit and surrounding units, we used the GeoDa software to calculate Moran’s I scatter plots diagrams for five representative time points, as mentioned in
Section 3.3.
Figure 4 shows that there had been an increasing tendency for Moran’s I of AIDS incidence (0.15, 0.277, 0.266, 0.35, and 0.395) for the five-time points. It is also noted that the scatter points of the five nodes are basically concentrated in the first quadrant, namely H-H aggregation, indicating that there was an obvious spatial aggregation phenomenon in the AIDS high incidence areas.
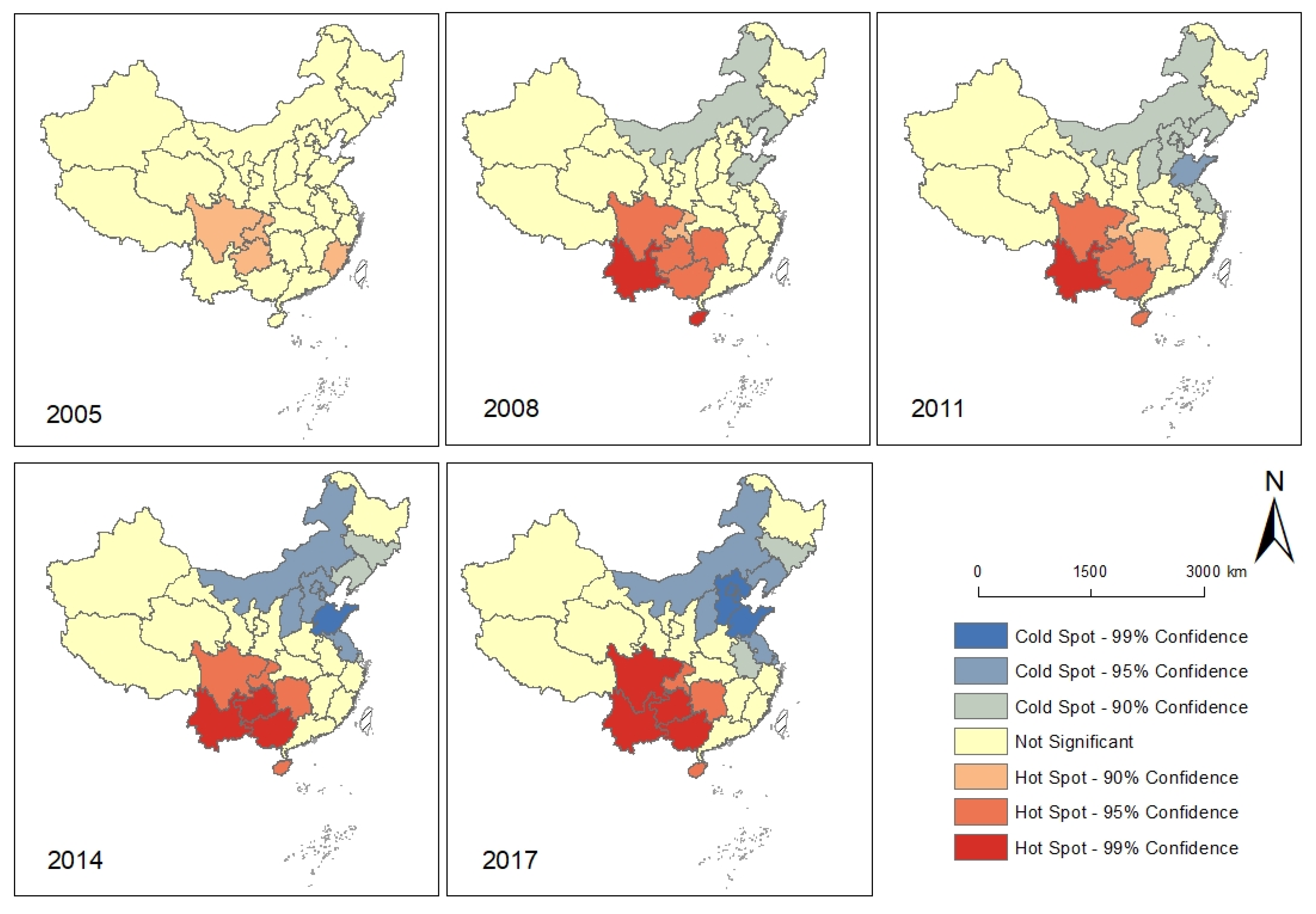
The Getis-Ord Gi * statistics results at the provincial level were interpreted in the ArcGIS environment. Similar to the interpretation of the Global Moran’s I statistics, the resultant Z score, and
p-value for each unit determined the high or low values. Based on that, the spatial patterns of the Hot-Cold Spots were illustrated in
Figure 5. The spatial agglomeration of hot-cold spots had been gradually enhanced, which was consistent with the global Moran’s index results above. In 2008 and 2011, the Hot Spots of AIDS incidence rates were mainly located at Yunnan, Guangxi, Guizhou, Chongqing, and Sichuan, which were also the Hot Spots in the following two notes with a higher statistical confidence level. Increasingly, starting from 2011, Shandong became the cold spots of AIDS incidence rates with a higher statistical confidence level compared to the sounding provinces, and this cold spot had been expanding continuously with a strong spatial aggregation characteristic. In 2017, the cold spot areas with a 99% confidence level were Shandong, Hebei, Beijing, and Tianjin, and the cold spots also extended to Inner Mongolia, Liaoning, Shaanxi, and Jiangsu with 95% confidence level.
3.3. Spatial Pattern of Influencing Factors of AIDS Incidence
For the variables in four groups (i.e., economy, traffic and transportation, medical treatment and education), a comprehensive variable was extracted as the influencing factor of each group of potential explanatory variables. The eigenvalues were 3.79, 1.76, 4.52 and 2.73 respectively, and coefficients were 2.00, 1.46, 2.24 and 1.73 respectively (
Table A4 and
Table A5 in
Appendix A). Taking the AIDS incidence rate in 2017 as the dependent variable, the GWR analysis was conducted on the variables of economy, transportation, medical care, and education level. The distribution of the variables and the homogeneity issue were checked and verified before the regression. The fixed spatial core was selected as Kernel type, and the corrected Akaike Information Criterion (AICc) was selected as the Bandwidth method. The AICc difference of GWR (i.e., 31.2) is much lower than that of the global model (i.e., 33.7), which indicates that GWR provides a better fit to the observed data.
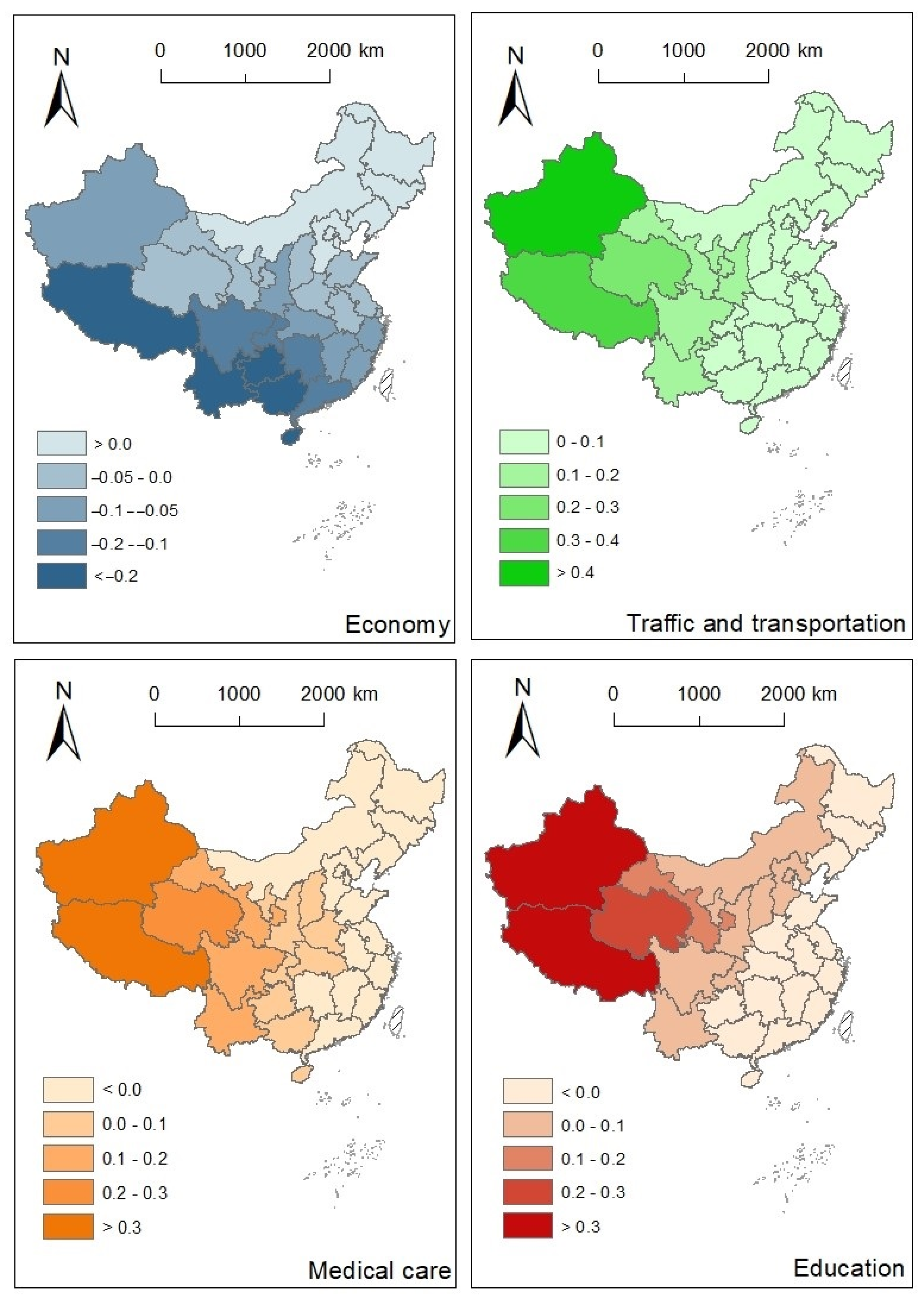
Figure 6 and
Figure A1 in the appendix showed the overall spatial variation of the GWR coefficients and their standard errors, respectively. For the sake of comparability and interpretation, the influencing variables for each observation were normalized to [0, 1].
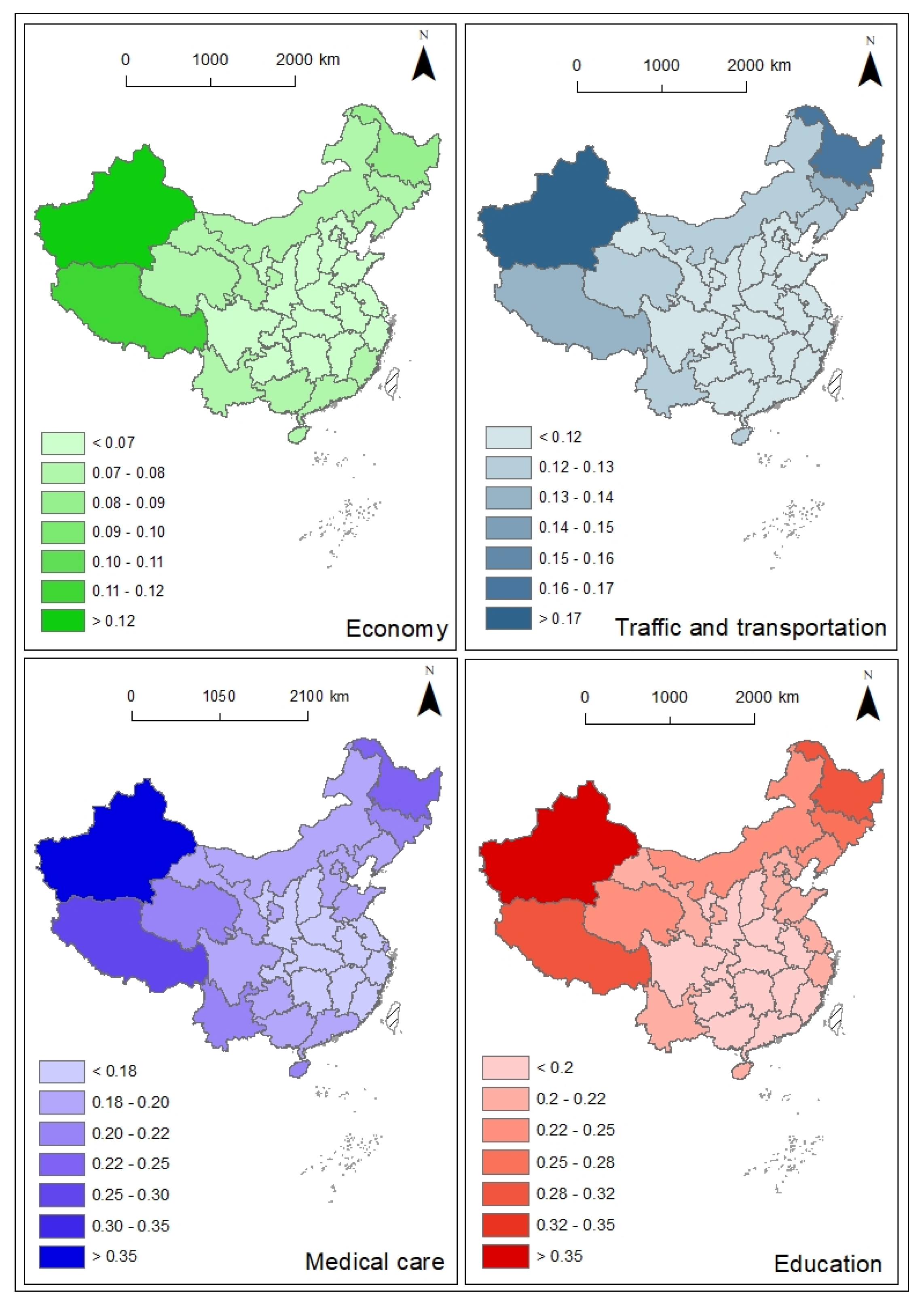
For the four variables from different perspectives of socio-economy, the standard errors of coefficients for medical care and education were much higher than those of the other factors. The ratios of the corresponding coefficient value and the standard error were higher than 2.5 for most of the observations (
Figure A1 in
Appendix B and
Figure 6), which indicated that these two variables were not significantly related to the AIDS incidence rate. Conversely, the economy had a generally negative effect on the AIDS incidence rate, based on the coefficient values and their standard error statistics. In comparison, the regression coefficients for traffic and transportation were generally positive and higher than the absolute value of the economy, that is, it had a stronger positive effect on the AIDS incidence rate.
The economy had a negative effect on the AIDS incidence rate for most of the areas in the mainland of China. Relatively absolute higher estimated coefficients were observed in western China (<−0.1) and especially southwestern China (<−0.2). It is noted that the economy level is relatively low in these regions, however, the degree of impacts was relatively large, and attention should also be paid to these areas. It indicated that a lower level of economic development would lead to a decrease in the capacity to prevent and control the AIDS epidemic. An unexpected finding of a slightly positive effect of the economy on the AIDS incidence rate was exhibited in Northeast China. Since the coefficients were near 0, and they were much lower than the coefficients in other regions, the effect of the economy on the AIDS incidence rate is hard to predict. GWR also revealed a strong spatial heterogeneity in the relationships of traffic and transportation and AIDS incidence rate. The more developed, the more the AIDS spread prevalent. The effects of traffic and transportation on the AIDS incidence rate were positive and the coefficient decreased from the west to the east, indicating that the western region is greatly influenced by the traffic and transportation development.
4. Discussion
Our results provide a comprehensive quantification of subnational AIDS epidemic trends on the Chinese mainland with geospatial analytical methods. Our study first addressed the spatial variations and time evaluations in AIDS incidence rate and intensity levels. Around the year 2004, the Chinese government and local authorities carried out a series of HIV infection checks and blood tests, to intervene in further HIV transmission through blood [
7]. Thus, the AIDS incidence rate had been relatively stable after 2008. The information on AIDS intensity levels “hot spots” of AIDS incidence rate throughout a relatively long period can be used to identify the high risks areas to target primary prevention strategies. For instance, Yunnan is located in the “Golden Triangle” region of Southeast Asia, where drug trafficking is rampant [
46]. Our finding revealed that the AIDS prevalence in this region had been dominant and become prevalent in the past decade, which is consistent with the reports that the distribution of HIV/AIDS infection in China is evolving from border regions nearby the “Golden Triangle” to inland areas [
47].
Finding on the Markov chain matrix analysis indicated that the high AIDS intensity level area and low AIDS intensity level area tend to maintain the original state in the next period. In other words, these areas had a higher probability of maintaining a high-intensity level in the next coming years and vice versa. Besides, the transfer probability between adjacent two levels is greater than that of cross-level, indicating the space-time transition and evolution had been gradual rather than jumping. Our spatial agglomeration study also demonstrated that a large proportion of AIDS patients had been concentrated in a small number of administrative units with strong spatial correlation. Our analysis highlights this favorable situation to efficiently target resources and interventions for bringing AIDS and HIV infection under control on the Chinese mainland.
Overall, the analysis of GWR revealed that the economy was most closely related to the AIDS incidence rate on the Chinese mainland. First, the economy was shown to be an essential and foremost factor that influences the AIDS incidence pattern. The regression coefficients of economic development were negative except for northeast China, which is consistent with the previous finding related to the spatial distribution of AIDS and main socio-economic driving factors in China [
48]. In southwestern China, the economic and education level are relatively low, whereas the sexual transaction and drug abuse situation are severe, thus, more attention should be paid on AIDS and its prevention strategies. In some respects, the situation in the southwestern China confirmed with previous broadly worldwide finding that poverty exacerbates the AIDS/HIV risk [
47,
49]. The difference in influencing mechanism may also dependent on the cultural backgrounds. Early marriage and childbearing can be another concern for primary AIDS prevention for areas where ethnic minorities gather with a unique culture. Minorities in concentrated communities have a relatively open and tolerant attitude towards sexual behavior and a relatively low awareness of prevention, which increases the possibility of HIV infection. Together with the finding on the spatial clustering tendency for Sichuan, Guizhou, Yunnan, and Guangxi provinces, this area is potentially in need of diagnosis and treatment services.
In terms of the traffic and transportation, the effect was more prevalent in western China than in eastern China, as evidenced by the higher estimated coefficients. The traffic and transportation in this study generally refers to population flow throughout the transportation networks. Even through the transportation by itself do not have a cause on AIDS, since the HIV transmission is different from respiratory epidemics. However, the GWR analysis indicated that the in transnational migrants accompanied by population flow due to trade cooperation and travel, and drug trafficking have a cause on AIDS. Previous study indicated that more than 60% of foreign AIDS cases travel to and from the border between Yunnan and Myanmar, which has also contributed to the spread of AIDS in the region [
50]. The frequent cross-border exchanges and interactions is also the cause of the AIDS epidemic in Xinjiang, which is adjacent to the “Golden Crescent”, a drug producing area in Central Asia [
51]. There are many drug users in this area and drug users share infected syringes. The population flow due to labor export from rural areas to cities in Sichuan, Chongqing, and Guizhou lead to dangerous sexual behaviors such as multi-sex couples and sex transactions is another susceptible factor for HIV transmission [
52]. The evolution of the AIDS incidence levels (
Figure 3) and the spatial patterns of AIDS incidence hot spots (
Figure 5) might indicate the movement of migrants and an expanded transportation network across the country.
Medical care and education level have been widely identified as important determinants of AIDS prevention at different scales [
9,
16,
36,
38]. However, our spatial regression analysis did not indicate a significant correlation at the provincial level. At the local scale, Liu et al. [
17] showed that the increase in the number of medical institutions per capita can reduce the HIV infection rate in Henan Province. The improvement of medical care and monitoring systems can enhance the surveillance capability for spatial epidemiology [
6]. A recent study of the HIV epidemic among men who have sex with men in China also showed that the number of medical institutions positively correlated with the number of reported HIV/AIDS cases depended on spatial regression at the county level [
53].
Previous studies also found that high-educated individuals should be targeted for AIDS prevention [
16] and that the individuals with a college degree or above showed a high AIDS incidence rate [
53]. Our study showed that the education effects on AIDS incidence rate varied with different regions and significant conclusions cannot be directly demonstrated. In this study, four groups of variables (i.e., economy, traffic and transportation, medical care, and education) were explored as macro comprehensive socio-economic indicators, however, the basic characteristics and information closely related to AIDS incidence may be ignored or missed. The examination of causal relationships of the related factors is needed, since the original selected variables can affect each other [
15]. Meanwhile, the overall pattern at the provincial administrative level was estimated, whereas the variations at the local level tend to be masked and the scale issue is an indispensable limitation of this study. The effects of religious beliefs, sex education at high schools can be important factors to intervene HIV transmission. The fine-scale spatiotemporal investigation of AIDS prevalence based on GIS and spatial analysis can be a fundamental method for precise AIDS interventions. Further, we just examined the historical AIDS trends at the provincial administrate level, due to the privacy protection of the AIDS incidence data at local scale. Further investigation of the traffic and transportation for targeted areas may help to figure out the spread of the AIDS in the future.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}






