
Mirror Therapy and Action Observation Therapy to Increase the Affected Upper Limb Functionality in Children with Hemiplegia: A Randomized Controlled Trial Protocol

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
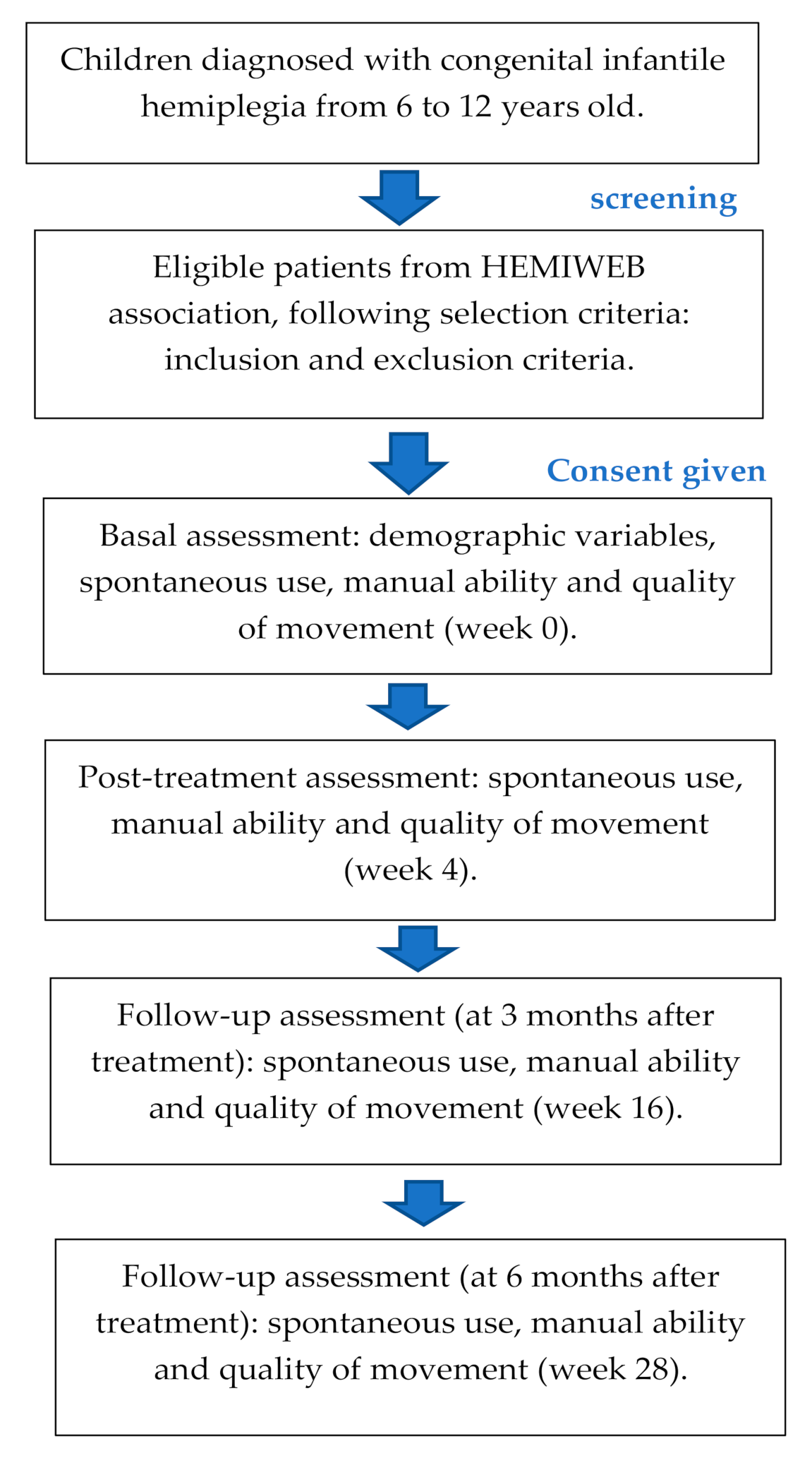
2.1. Study Design
2.2. Sample Size
2.3. Participants
- Congenital infantile hemiplegia.
- Aged between 6 and 12 years.
- Lack of use of the affected upper limb.
- Level I–III of the Manual Ability Classification System (MACS). Level I: handles objects easily and successfully; level II: handles most objects but with reduced quality and/or speed of achievement and level III: handles objects with difficulty; needs help to prepare and/or modify activities [32].
- Level I–III in the Gross Motor Function Classification System (GMFCS). Level I: can walk indoors and outdoors and climb stairs without using hands for support, can perform usual activities such as running and jumping and has decreased speed, balance and coordination; level II: can climb stairs with a railing, has difficulty with uneven surfaces, inclined or in crowds of people and has only minimal ability to run or jump and level III: walks with assistive mobility devices indoors and outdoors on level surfaces, may be able to climb stairs using a railing and may propel a manual wheelchair and need assistance for long distances or uneven surfaces [33].
- Disease not associated with congenital hemiplegia.
- Low cognitive level compatible with attending a special education school.
- Presence of contractures in the affected upper limb affecting the functional movement.
- Surgery in the six months previously to the treatment.
- Botulinum toxin in the two months previously to or during the intervention.
- Pharmacologically uncontrolled epilepsy.
2.4. Procedures and Interventions
2.5. Outcome Measures
2.5.1. Spontaneous Use
2.5.2. Manual Ability
2.5.3. Surface Electromyography (EMG) of Extensors and Flexors Muscles of the Wrist
2.5.4. Grasp Strength
2.6. Data Analysis
2.7. Ethical Aspects
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Monge Pereira, E.; Molina Rueda, F.; Alguacil Diego, I.M.; de la Cuerda, R.C.; de Mauro, A.; Miangolarra Page, J.C. Empleo de sistemas de realidad virtual como método de propiocepción en parálisis cerebral: Guía de práctica clínica. Neurologia 2014, 29, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Sgandurra, G.; Ferrari, A.; Cossu, G.; Guzzetta, A.; Biagi, L.; Tosetti, M.; Fogassi, L.; Cioni, G. Upper limb children action-observation training (UP-CAT): A randomised controlled trial in Hemiplegic Cerebral Palsy. BMC Neurol. 2011, 11, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riddell, M.; Kuo, H.C.; Zewdie, E.; Kirton, A. Mirror movements in children with unilateral cerebral palsy due to perinatal stroke: Clinical correlates of plasticity reorganization. Dev. Med. Child Neurol. 2019, 61, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Vosberg, D.E.; Beaulé, V.; Torres-Berrío, A.; Cooke, D.; Chalupa, A.; Jaworska, N.; Cox, S.M.L.; Larcher, K.; Zhang, Y.; Allard, D.; et al. Neural function in DCC mutation carriers with and without mirror movements. Ann. Neurol. 2019, 85, 433–442. [Google Scholar] [CrossRef] [Green Version]
- Ejaz, N.; Xu, J.; Branscheidt, M.; Hertler, B.; Schambra, H.; Widmer, M.; Faria, A.V.; Harran, M.D.; Cortes, J.C.; Kim, N.; et al. Evidence for a subcortical origin of mirror movements after stroke: A longitudinal study. Brain 2018, 141, 837–847. [Google Scholar] [CrossRef]
- Eliasson, A.C.; Forssberg, H.; Hung, Y.C.; Gordon, A.M. Development of hand function and precision grip control in individuals with cerebral palsy: A 13-year follow-up study. Pediatrics 2006, 118, e1226–e1236. [Google Scholar] [CrossRef]
- Boyd, R.; Sakzewski, L.; Ziviani, J.; Abbott, D.F.; Badawy, R.; Gilmore, R.; Provan, K.; Tournier, J.D.; Macdonell, R.A.; Jackson, G.D. INCITE: A randomised trial comparing constraint induced movement therapy and bimanual training in children with congenital hemiplegia. BMC Neurol. 2010, 10, 4. [Google Scholar] [CrossRef]
- Palomo-Carrión, R.; Romero-Galisteo, R.-P.; Pinero-Pinto, E.; López-Muñoz, P.; Romay-Barrero, H.; José, F.-M. Application of Low-Intensity Modified Constraint-Induced Movement Therapy to Improve the Affected Upper Limb Functionality in Infantile Hemiplegia with Moderate Manual Ability: Case Series. Children 2020, 7, 127. [Google Scholar] [CrossRef]
- Palomo-Carrión, R.; Pinero-Pinto, E.; Ando-LaFuente, S.; Ferri-Morales, A.; Bravo-Esteban, E.; Romay-Barrero, H. Unimanual Intensive Therapy with or without Unaffected Hand Containment in Children with Hemiplegia. A Randomized Controlled Pilot Study. J. Clin. Med. 2020, 9, 2992. [Google Scholar] [CrossRef]
- Pandyan, A.D.; Gregoric, M.; Barnes, M.P.; Wood, D.; Van Wijck, F.; Burridge, J.; Hermens, H.; Johnson, G.R. Spasticity: Clinical perceptions, neurological realities and meaningful measurement. Disabil. Rehabil. 2005, 27, 2–6. [Google Scholar] [CrossRef]
- Nielsen, J.B.; Crone, C.; Hultborn, H. The spinal pathophysiology of spasticity—From a basic science point of view. Acta Physiol. 2007, 189, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Bleyenheuft, Y.; Gordon, A.M. Precision grip control, sensory impairments and their interactions in children with hemiplegic cerebral palsy: A systematic review. Res. Dev. Disabil. 2013, 34, 3014–3028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarcher, A.; Raison, M.; Ballaz, L.; Lemay, M.; Leboeuf, F.; Trudel, K.; Mathieu, P.A. Impact of muscle activation on ranges of motion during active elbow movement in children with spastic hemiplegic cerebral palsy. Clin. Biomech. 2015, 30, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Mai, J.; He, L.; Yan, X.; Chen, Y. Surface electromyography of wrist flexors and extensors in children with hemiplegic cerebral palsy. PM R 2015, 7, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Houwink, A.; Aarts, P.B.; Geurts, A.C.; Steenbergen, B. A neurocognitive perspective on developmental disregard in children with hemiplegic cerebral palsy. Res. Dev. Disabil. 2011, 32, 2157–2163. [Google Scholar] [CrossRef]
- Taub, E.; Wolf, S.L. Constraint-induced (CI) movement techniques to facilitate upper extremity use in sotrke patients. Top. Stroke Rehabil. 1997, 2, 28–61. [Google Scholar]
- Sunderland, A.; Tuke, A. Neuroplasticity, learning and recovery after stroke: A critical evaluation of constraintinduced therapy. Neuropsychol. Rehabil. 2005, 15, 81–96. [Google Scholar] [CrossRef]
- Chung, C.Y.; Chen, C.L.; Wong, A.M. Pharmacotherapy of spasticity in children with cerebral palsy. J. Formos. Med. Assoc. 2011, 110, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Pollock, A.; Farmer, S.E.; Brady, M.C.; Langhorne, P.; Mead, G.E.; Mehrholz, J.; van Wijck, F. Interventions for improving upper limb function after stroke. Cochrane Database Syst. Rev. 2014, 11, CD010820. [Google Scholar] [CrossRef]
- Ramachandran, V.S.; Rogers-Ramachandran, D.; Cobb, S. Touching the phantom limb. Nature 1995, 377, 489–490. [Google Scholar] [CrossRef]
- Deconinck, F.J.; Smorenburg, A.R.; Benham, A.; Ledebt, A.; Feltham, M.G.; Savelsbergh, G.J. Reflections on mirror therapy: A systematic review of the effect of mirror visual feedback on the brain. Neurorehabilit. Neural Repair 2015, 29, 349–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- French, B.; Thomas, L.H.; Coupe, J.; McMahon, N.E.; Connell, L.; Harrison, J.; Sutton, C.J.; Tishkovskaya, S.; Watkins, C.L. Repetitive task training for improving functional ability after stroke. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruchez, R.; Jequier Gygax, M.; Roches, S.; Fluss, J.; Jacquier, D.; Ballabeni, P.; Grunt, S.; Newman, C.J. Mirror therapy in children with hemiparesis: A randomized observer-blinded trial. Dev. Med. Child Neurol. 2016, 58, 970–978. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.M.; Barber, P.A.; Coxon, J.P.; Fleming, M.K.; Byblow, W.D. Priming the motor system enhances the effects of upper limb therapy in chronic stroke. Brain 2008, 131, 1381–1390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeves-Lite, A.; Zuil-Escobar, J.C.; Martínez-Cepa, C.; Romay-Barrero, H.; Ferri-Morales, A.; Palomo-Carrión, R. Conventional and Virtual Reality Mirror Therapies in Upper Obstetric Brachial Palsy: A Randomized Pilot Study. J. Clin. Med. 2020, 9, 3021. [Google Scholar] [CrossRef]
- Feltham, M.G.; Ledebt, A.; Deconinck, F.J.; Savelsbergh, G.J. Mirror visual feedback induces lower neuromuscular activity in children with spastic hemiparetic cerebral palsy. Res. Dev. Disabil. 2010, 31, 1525–1535. [Google Scholar] [CrossRef]
- Ramachandran, V.S.; Altschuler, E.L. The use of visual feedback, in particular mirror visual feedback, in restoring brain function. Brain 2009, 132, 1693–1710. [Google Scholar] [CrossRef] [Green Version]
- Buccino, G.; Arisi, D.; Gough, P.; Aprile, D.; Ferri, C.; Serotti, L.; Tiberti, A.; Fazzi, E. Improving upper limb motor functions through action observation treatment: Pilot study in children with cerebral palsy. Dev. Med. Child Neurol. 2012, 54, 822–828. [Google Scholar] [CrossRef]
- Smith, T.B.; Oliver, M.N.; Innocenti, M.S. Parenting stress in families of children with disabilities. Am. J. Orthopsychiatry 2001, 71, 257–261. [Google Scholar] [CrossRef]
- McConachie, H.; Colver, A.F.; Forsyth, R.J.; Jarvis, S.N.; Parkinson, K.N. Participation of disabled children: How should it be characterised and measured? Disabil. Rehabil. 2006, 28, 1157–1164. [Google Scholar] [CrossRef]
- Raina, P.; O’Donnell, M.; Rosenbaum, P.; Brehaut, J.; Walter, S.D.; Russell, D.; Swinton, M.; Zhu, B.; Wood, E. The health and well-being of caregivers of children with cerebral palsy. Pediatrics 2005, 115, e626–e636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eliasson, A.C.; Krumlinde-Sundholm, L.; Rösblad, B.; Beckung, E.; Arner, M.; Ohrvall, A.M.; Rosenbaum, P. The Manual Ability Classification System (MACS) for children with cerebral palsy: Scale development and evidence of validity and reliability. Dev. Med. Child Neurol. 2006, 48, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Hadders-Algra, M.; Boxum, A.G.; Hielkema, T.; Hamer, E.G. Effect of early intervention in infants at very high risk of cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2017, 59, 246–258. [Google Scholar] [CrossRef] [PubMed]
- Sgandurra, G.; Ferrari, A.; Cossu, G.; Guzzetta, A.; Fogassi, L.; Cioni, G. Randomized trial of observation and execution of upper extremity actions versus action alone in children with unilateral cerebral palsy. Neurorehabil. Neural Repair 2013, 27, 808–815. [Google Scholar] [CrossRef] [Green Version]
- Beani, E.; Menici, V.; Ferrari, A.; Cioni, G.; Sgandurra, G. Feasibility of a Home-Based Action Observation Training for Children With Unilateral Cerebral Palsy: An Explorative Study. Front Neurol. 2020, 11, 16. [Google Scholar] [CrossRef] [Green Version]
- Gygax, M.J.; Schneider, P.; Newman, C.J. Mirror therapy in children with hemiplegia: A pilot study. Dev. Med. Child Neurol. 2011, 53, 473–476. [Google Scholar] [CrossRef]
- Holmefur, M.M.; Krumlinde-Sundholm, L. Psychometric properties of a revised version of the Assisting Hand Assessment (Kids-AHA 5.0). Dev. Med. Child Neurol. 2016, 58, 618–624. [Google Scholar] [CrossRef]
- Krumlinde-Sundholm, L.; Eliasson, A.C. Development of the Assisting Hand Assessment: A Rasch-built measure intended for children with unilateral upper limb impairments. Scand. J. Occup. Ther. 2003, 10, 16–26. [Google Scholar] [CrossRef]
- Holmefur, M.; Aarts, P.; Hoare, B.; Krumlinde-Sundholm, L. Test-retest and alternate forms reliability of the assisting hand assessment. J. Rehabil. Med. 2009, 41, 886–891. [Google Scholar] [CrossRef] [Green Version]
- Krumlinde-Sundholm, L.; Holmefur, M.; Kottorp, A.; Eliasson, A.C. The assisting hand assessment: Current evidence of validity, reliability, and responsiveness to change. Dev. Med. Child Neurol. 2007, 49, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Jebsen, R.H.; Taylor, N.; Trieschmann, R.B.; Trotter, M.J.; Howard, L.A. An objective and standardized test of hand function. Arch. Phys. Med. Rehabil. 1969, 50, 311–319. [Google Scholar] [PubMed]
- Taylor, N.; Sand, P.L.; Jebsen, R.H. Evaluation of hand function in children. Arch. Phys. Med. Rehabil. 1973, 54, 129–135. [Google Scholar]
- Schmidt-Rohlfing, B.; Bergamo, F.; Williams, S.; Erli, H.J.; Rau, G.; Niethard, F.U.; Disselhorst-Klug, C. Interpretation of surface EMGs in children with cerebral palsy: An initial study using a fuzzy expert system. J. Orthop. Res. 2006, 24, 438–447. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; He, L.; Mai, J.; Yan, X.; Chen, Y. Muscle recruitment and coordination following constraing-induced movement therapy with electrical stimulation on children with hemiplegic cerebral palsy: A randomized controlled trial. PLoS ONE 2015, 10, e0138608. [Google Scholar]
- Dekkers, K.; Smeets, R.; Janssen-Potten, Y.; Gordon, A.M.; Speth, L.A.; Rameckers, E.A. Psychometric evaluation of 2 new upper extremity funciontal strength tests in children with cerebral palsy. Phys. Ther. 2019, 99, 1107–1115. [Google Scholar]
- Dekkers, K.; Janseen-Potten, Y.; Gordon, A.M.; Speth, L.; Smeets, R.; Rameckers, E. Reliability of máximum isometric arm, grip and pinch strength measurements in children (7–12 years) with unilateral spastic cerebral palsy. Disabil. Rehabil. 2019, 42, 1448–1453. [Google Scholar] [CrossRef]
- Bonini, L.; Rozzi, S.; Serventi, F.; Simone, L.; Ferrari, P.F.; Fogassi, L. Ventral premotor and inferior parietal cortices make distinct contribution to action organization and intention understanding. Cereb. Cortex 2010, 20, 1372–1385. [Google Scholar] [CrossRef] [Green Version]
- Fogassi, L.; Ferrari, P.F.; Gesierich, B.; Rozzi, S.; Chersi, F.; Rizzolatti, G. Parietal lobe: From action organization to intention understanding. Science 2005, 308, 662–667. [Google Scholar] [CrossRef]


{kind=link}
| Unimanual activities | Remove the lid from a container, remove marbles and place them in a glass. Pour water into a glass. Take a colored card, turn it over and place it with a similar figure to make pairs. Use a stamp, making figures in a horizontal plane, that is, on a paper on the table. Take coins from the table, put them in a slotted container. Take a sponge and dip it in finger paint, and then squeeze the foam in a horizontal plane, on the table. Lift the open lid of a tube containing colored paint and squish it to throw the paint onto a sheet of paper and spread it out. Use a toy fishing rod and catch magnetic animals or just catch magnetic animals. |
| Bimanual Activities | Chop up tissue paper. Wet a small towel and drain it. Stick cards on your sign on the table on a horizontal plane and/or on felt paper on a vertical plane. Make a large ball of clay and roll it with both hands until it is thrown at the end of the table. Open a coin box and take out 5 coins and put them back in and close the coin box. Build figures with Lego pieces. Apply glue stick on a piece of paper and throw the pieces of tissue paper cut earlier with both hands and glue them to create a picture. |
| Activities | Touch with the tips of the fingers a plasticine base for 2 min (Rest 30 s) The movement of the fingers is worked; the thumb touches each one of the fingertips for 2 min. (Rest 30 s) We work the thumb and index finger clamp with the contact of both fingers putting a resistance through a rubber between thumb and index finger for 2 min. (Rest 30 s) We will place a sponge in each of the hands to work the global grip. Squeeze and release the object and therefore also the grip strength for 2 min. (Rest 30 s) Extension movement of both wrists on a plasticine base for 2 min. (Rest 30 s) Prono-supination of the forearm, starting from a pronation position for 2 min. (Rest 30 s before starting TOA) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palomo-Carrión, R.; Zuil-Escobar, J.C.; Cabrera-Guerra, M.; Barreda-Martínez, P.; Martínez-Cepa, C.B. Mirror Therapy and Action Observation Therapy to Increase the Affected Upper Limb Functionality in Children with Hemiplegia: A Randomized Controlled Trial Protocol. Int. J. Environ. Res. Public Health 2021, 18, 1051. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031051
Palomo-Carrión R, Zuil-Escobar JC, Cabrera-Guerra M, Barreda-Martínez P, Martínez-Cepa CB. Mirror Therapy and Action Observation Therapy to Increase the Affected Upper Limb Functionality in Children with Hemiplegia: A Randomized Controlled Trial Protocol. International Journal of Environmental Research and Public Health. 2021; 18(3):1051. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031051
Chicago/Turabian StylePalomo-Carrión, Rocío, Juan Carlos Zuil-Escobar, Myriam Cabrera-Guerra, Paloma Barreda-Martínez, and Carmen Belén Martínez-Cepa. 2021. "Mirror Therapy and Action Observation Therapy to Increase the Affected Upper Limb Functionality in Children with Hemiplegia: A Randomized Controlled Trial Protocol" International Journal of Environmental Research and Public Health 18, no. 3: 1051. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031051